

Abstract
Objective:
Social anxiety disorder (SAD), (also known as social phobia), is characterized by intense fear of social interaction and often associated with social avoidance and impairments. There is high risk for depression, substance use disorder, and suicide among them.
Subjects and Methods:
It is an observational, cross-sectional, single centered, questionnaire-based study assessing the frequency of SAD and depression and their possible association with quality of life among 290 consenting medical undergraduate students. Social Phobia Inventory (SPIN), Beck's Depression Inventory (BDI II), and the World Health Organization Quality of Life assessment scale (WHOQOL-BREF) were used to screen and assess severity of SAD, depression, and quality of life, respectively. The statistical analysis of proportions was done by Chi-square test, while the scores of SPIN, BDI II, and WHOQOL-BREF was compared using Mann–Whitney test or Kruskal–Wallis test followed by Dunn posttest multiple comparison, using GraphPad InStat version 3.06.
Results:
Frequency of SAD is 11.37%, and depression is 8.96%. Females are more likely to experience SAD. Participants with SAD are more likely to experience depression (P < 0.0001) and have poor quality of life (P = 0.01). Participants with depression have higher SPIN score (P < 0.0001) and poor quality of life (P < 0.0001). Females are more likely to experience social fear (P = 0.02). Participants staying away from their family are more likely to experience social anxiety in comparison to their peers (P = 0.01). Severity of depression is correlated with severity of social anxiety (Spearman r = 0.4423 [0.3416–0.5329], P < 0.0001).
Conclusion:
Participants with SAD are more likely to experience depressive symptoms and have poor quality of life and vice versa.
Keywords: Depression, quality of life, social phobia
Introduction
Anxiety disorders are the associated with excessive fear, nervousness, apprehension, and related behavioral disturbances.[1] Social anxiety disorder (SAD), (also known as social phobia), involves fear and anxiety about the social interaction and often associated with avoidant behavior.[1]
SAD is a chronic disorder significantly affecting the lifestyle of the individuals, often prevents the individual from available opportunities and makes the person disable at work and social life.[2,3,4] Children and adolescent with SAD experience significant distress and impairment in study and social relationships, while adults with SAD are more likely to experience lower education attainment, lower wages or unemployment, and poor quality of relationships with family and partner.[5,6,7,8] Persons with SAD have frequent comorbid psychiatric disorders such as depression, substance use disorders and are at increased risk of suicide.[9,10,11] As SAD have onset at early age and long duration of illness, untreated individuals are likely to suffer for a long time.[12]
In primary care setting, anxiety disorders and depression are highly prevalent and are associated with reduced level of functioning.[13] Although family physician is a first medical contact point for patients suffering from psychiatric illness,[14] mental health problems are poorly recognized and treated at primary care setting because of time constraints and limited training in identification and management of mental health issues.[15] There are studies showing evidence that timely identification and treatment of mental health problem by trained family physician at primary care setting can significantly improve mental health outcome.[16,17] As SAD have chronic course of illness, presenting with various psychiatric comorbidities such as depression, substance use disorder, and increased risk of suicide and may have various lifelong consequences in individual's social and personal life.[3,4,9,10,11] The presence of atypical depression with SAD associated with severe symptoms, suicide attempts, bipolarity, and impaired functioning in comparison to patients with nonatypical depression.[18] It is important for a primary care physician to screen the patients of SAD, associated comorbidities for better treatment and prognosis.
The prevalence of SAD varied from 2% to 16% in various studies, and SAD is much more prevalent in the general population in comparison to the primary healthcare setting.[19] The prevalence of SAD is less studied in the Eastern societies and reported very less 0.4%–0.6% in Southeast Asian countries such as Taiwan and Korea,[20] while it was 12.8% among the Indian high school adolescence.[21]
A recent Australian study found lifetime prevalence of SAD as 8.4%, and 12-month prevalence is 4.2%.[22] Although 70% of patients of SAD experienced comorbid mental health problems in their study, 20% of them reported social anxiety as their primary concern for treatment seeking, and most commonly through general practitioner.[22]
SAD is one of the most common psychiatric illnesses, which contributes significantly for functional status and quality of life. There are fewer studies in the Eastern countries assessing the frequency of SAD and its association with other psychiatric comorbidity and quality of life;[23] we have evaluated the frequency of SAD and comorbid depression, and their association with quality of life, among the undergraduate students of the medical school.
Subjects and Methods
It is a single center, questionnaire-based, observational, cross-sectional study for assessing association of SAD with comorbid depression and quality of life among medical undergraduate students. The study was started after prior approval from Local Ethics Committee. Totally, 290 participants of both genders, studying undergraduate medical course, Bachelor of Medicine and Bachelor of Surgery, at Government Medical College, Bhavnagar, Gujarat, India, willing to give written informed consent, were recruited for the study, between April and June 2013. The consenting participants were instructed to fill up their demographic details, self-administered questionnaire of Social Phobia Inventory (SPIN), and World Health Organization Quality of Life assessment scale (WHOQOL-BREF) in the given performs.
SPIN is a 17-item self-rating screening instrument, to be rated in 0 (not at all) to 4 (extremity) Likert scale, assessing fear and avoidance in variety of social situations. The scale has good ability to distinguish adults with or without social phobia, and has three subscale for avoidant behavior (of talking to strangers, of speaking to people for fear of embarrassment, of going to parties, of being the center of attention, of making speeches, of being criticized, of speaking to authority), physical symptoms (blushing, sweating, palpitations, or shaking and trembling in the front of other people), and social fear (of people in authority, of parties and social events, of being criticized, of talking to strangers, of doing things when people are watching, and of being embarrassed).[24] Cutoff value of SPIN for SAD was recommended as 24, and 19 for subclinical SAD in earlier study.[25]
Beck's depression inventory (BDI II) is a self-rating questionnaire with 21 items used as screening tool as well as for assessing severity of depression.[26] The recommended cutoff value for screening of depression is 13 as the best for balance between sensitivity and specificity.[27]
WHOQOL-BREF is a 26 item self-rating instrument for assessing the quality of life in physical health, psychological, social relationship, and environmental domains.[28] Each item rated in 0–5 Likert scale. It is a validated instrument designed to assess the impact of disease on quality of life.
Qualitative data were expressed in proportions, while quantitative data were expressed in mean ± standard deviation (SD). The statistical analysis of proportions was done by Chi-square test, while the scores of SPIN, BDI II, and WHOQOL-BREF was compared using Mann–Whitney test or Kruskal–Wallis test followed by Dunn posttest multiple comparison using GraphPad InStat version 3.06 (San Diego, California, US). Correlation between BDI II score and SPIN score were analyzed by applying Pearson's coefficient. P ≤ 0.05 was considered statistically significant.
Sample size calculation:[29]
Where Z1-α/2 is standard normal variant (at 5% type I error, P < 0.05 it is 1.96 and at 1% type I error, P < 0.01 it is 2.58. In majority of studies, P < 0.05 is considered statistically significant, hence, 1.96 is used in formula.[29]
P = Expected proportion in population based on previous studies or pilot studies
d = absolute error or precision = to be decided by researcher
There are Indian studies found the prevalence of SAD as 12.8%[21] and considering precision/absolute error of 5% and type I error of 5% in above formula.

Hence, for this cross-sectional study, we have to take 172 or more samples.
Results
Consenting 290 participants were evaluated for SAD, depression, and quality of life.
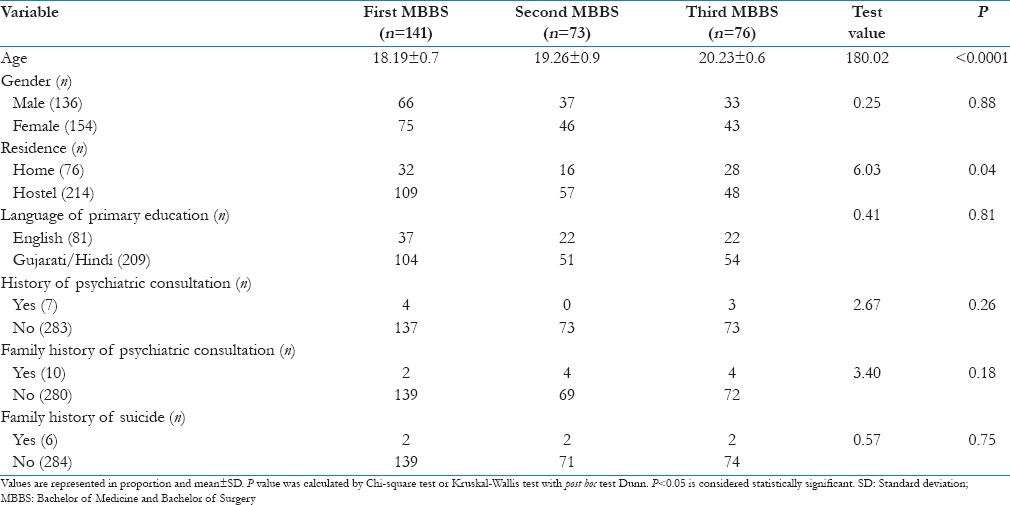
A demographic variable of the study population is shown in Table 1. The mean age of the study population is 19 ± 1.1 (mean ± SD). Among 33 participants of social phobia, there were 13 males and twenty females and only one of them had consulted psychiatrist in the past. There were 21.21% participants with SAD had depression.
Table 1.
Demographic variables of the study population, arranged as per their current academic year
As mentioned in Table 2, frequency of SAD (SPIN >24) and depression (BDI II >13) is 33 (11.37%) and 26 (8.96%), respectively. Participants with SAD are likely have higher BDI II score (10.48 ± 5.3, 6.24 ± 4.8) (P < 0.0001) and poor quality of life in social relationship domain of WHOQOL-BREF. Participants with depression are likely to have higher SPIN score in all the domains (social fear 7.73 ± 3.7, 4.34 ± 3.1; avoidant behavior 9.42 ± 3.9, 6.50 ± 4.0; physical symptoms 4.19 ± 2.3, 2.31 ± 2.1) (P < 0.0001) and poor quality of life in all the domains of WHOQOL-BREF (physical health 48.07 ± 13.9, 60.07 ± 8.6; psychological 54.00 ± 15.5, 66.77 ± 9.2; social relationship 59.29 ± 20.5, 76.76 ± 13.8; environmental 59.25 ± 11.9, 72.76 ± 12.2) (P < 0.0001). The odd ratio for depression in patients with SAD is 3.37 (95% confidence interval = 1.29–8.77, χ2 = 5.25, df = 1).
Table 2.
Association of social anxiety disorder and depression with quality of life
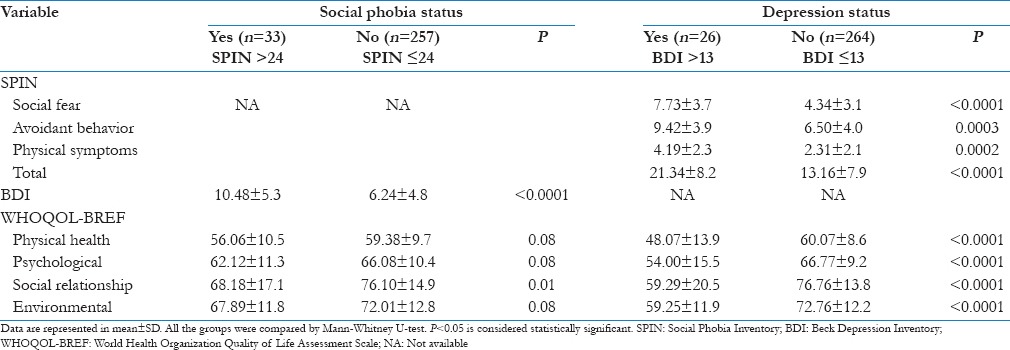
Table 3 shows that girls have more social fear in comparison to boys (4.20 ± 3.1, 5.00 ± 3.4) (P = 0.02). Participants staying at hostels and away from their family are likely to experience more social anxiety in comparison to their peers (15.52 ± 8.2, 12.14 ± 8.2) (P = 0.01). Participants who received their primary education in English medium schools are likely to experience more social anxiety in comparison to participants who received their primary education in their mother tongue (Gujarati or Hindi) (16.08 ± 7.7, 13.05 ± 8.3) (P = 0.0010).
Table 3.
Association of gender, residence and study medium with Social Phobia Inventory score

The correlation between SPIN and BDI II was calculated using Spearman. r = 0.4423 (0.3416–0.5329), P < 0.0001 [Figure 1].
Figure 1.
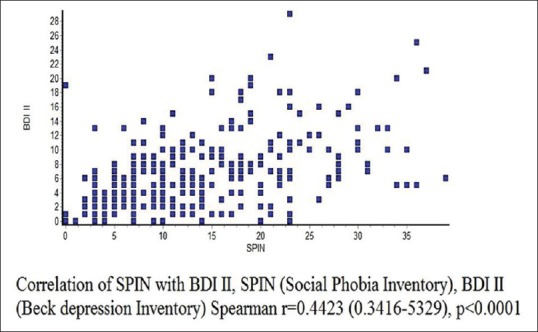
Correlation score of social phobia inventory with Beck Depression Inventory
Discussion
The main finding of our study is the frequency of SAD as 11.37%, and that of depression is 8.96%, similar finding was reported in Indian adolescence and Iranian population.[21,23] In consistent with earlier study, SAD is more frequent among women.[23] Females are more likely to experience social fears in comparison to male, while avoidant and physical symptoms were equal in both genders. This finding is in consistent with prior study that females have higher frequency of social fear than social phobia.[30]
The participants with SAD are more likely to experience depressive symptoms and have poor quality of life in social domain of WHOQOL-BREF, which include personal relationships, social support, and social relationship.[28] It was reported earlier that lifetime diagnosis of SAD is associated with dissatisfaction with person's main activity, family life, friends, leisure activities, and income.[8] It was reported in the previous study that 69% of the patients of social phobia having associated major comorbid disorders and presence of comorbidity increase the risk for suicidal attempts.[9] Although uncomplicated social phobia associated with suicidal ideation, financial dependency, distress and impairments, mental health professionals are rarely consulted for the treatment.[9] These findings are in consistent with our results.
In consistent with the previous study, social phobia increases likelihood for experiencing depressive symptoms and fear subtype of social phobia is strongly associated with depression.[8] Major depression (after adjustment with lifetime social phobia) is associated with dissatisfaction and poor quality of life.[8] Association of impairment in quality of life in depression is stronger than that with social phobia.[8]
Participants with depression are more likely experience social anxiety in all the domains including social fear, avoidant behavior and physical symptoms, and correlates severity of social anxiety with severity of depression. These findings are in consistent with earlier study.[8]
Participants staying at home with their families are less likely to experience social anxiety, especially in avoidant behavior and physical symptoms in comparisons to their peers. It is in accordance with earlier study that persons with poor social supports are more likely to experience social anxiety symptoms in comparison to persons with good social supports.[23]
In contrast to earlier study, participants who received their primary education in English medium school are more likely to experience anxiety symptoms in comparison to participants who received their primary education in their mother tongue.[31] This discrepancy in finding of our study could be because of selection of participants from the medical school instead of secondary school students. As there is growing trend to view English medium schools as superior in comparison to local language schools and persons with social phobia have lower educational attainment, selection of participants from higher meritorious institute makes the participants who received their primary education in mother tongue, having lower anxiety score have been recruited in this study.[5,31]
We recommend screening for SAD among adolescents and young adults, as it is a lifetime diagnosis, and it is associated with psychiatric illness such as depression, and their severity is correlated. Individuals with comorbid depression have poor quality of life.
Limitations
Although we have assessed the association of SAD with depression and quality of life among medical students using validated scale of assessment, our study has several limitations such as recruiting participants from single center and assessing frequency of SAD and depression by self-reported questionnaire, measurement errors, and participant bias are unavoidable, as avoidant personality disorder, other anxiety disorders and substance use disorders often coexist with SAD and may become a confounding factors in assessing SAD. Similarly, dysthymia and substance use disorders can be the confounding factors in assessing depression. Being a cross-sectional nature of study, cause-effect relationship cannot be established with this study. Further large sample-sized interview-based cohort studies are recommended for further evaluation.
Conclusion
The frequency of SAD is 11.37%. Participants with SAD are more likely to experience depression and poor quality of life and vice versa. Participants with poor social supports have more social anxiety symptoms.
As SAD is very prevalent in general population usually starts during adolescence age and it significantly affects educational attainment, poor wages, poor family relationship, increase risk of depressive disorder, and significantly impairs quality of life of individuals. High suspicion for screening of SAD and timely intervention by pharmacotherapy or psychotherapy may be helpful for long-term well-being of an individual.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.5th ed. Washington, DC: American Psychiatric Press; 2013. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. [Google Scholar]
- 2.Wittchen HU, Fehm L. Epidemiology, patterns of comorbidity, and associated disabilities of social phobia. Psychiatr Clin North Am. 2001;24:617–41. doi: 10.1016/s0193-953x(05)70254-9. [DOI] [PubMed] [Google Scholar]
- 3.Wittchen HU, Fuetsch M, Sonntag H, Müller N, Liebowitz M. Disability and quality of life in pure and comorbid social phobia. Findings from a controlled study. Eur Psychiatry. 2000;15:46–58. doi: 10.1016/s0924-9338(00)00211-x. [DOI] [PubMed] [Google Scholar]
- 4.La Greca AM, Lopez N. Social anxiety among adolescents: Linkages with peer relations and friendships. J Abnorm Child Psychol. 1998;26:83–94. doi: 10.1023/a:1022684520514. [DOI] [PubMed] [Google Scholar]
- 5.Van Ameringen M, Mancini C, Farvolden P. The impact of anxiety disorders on educational achievement. J Anxiety Disord. 2003;17:561–71. doi: 10.1016/s0887-6185(02)00228-1. [DOI] [PubMed] [Google Scholar]
- 6.Katzelnick DJ, Kobak KA, DeLeire T, Henk HJ, Greist JH, Davidson JR, et al. Impact of generalized social anxiety disorder in managed care. Am J Psychiatry. 2001;158:1999–2007. doi: 10.1176/appi.ajp.158.12.1999. [DOI] [PubMed] [Google Scholar]
- 7.Moitra E, Beard C, Weisberg RB, Keller MB. Occupational impairment and Social Anxiety Disorder in a sample of primary care patients. J Affect Disord. 2011;130:209–12. doi: 10.1016/j.jad.2010.09.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stein MB, Kean YM. Disability and quality of life in social phobia: Epidemiologic findings. Am J Psychiatry. 2000;157:1606–13. doi: 10.1176/appi.ajp.157.10.1606. [DOI] [PubMed] [Google Scholar]
- 9.Schneier FR, Johnson J, Hornig CD, Liebowitz MR, Weissman MM. Social phobia. Comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282–8. doi: 10.1001/archpsyc.1992.01820040034004. [DOI] [PubMed] [Google Scholar]
- 10.Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:617–27. doi: 10.1001/archpsyc.62.6.617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cougle JR, Keough ME, Riccardi CJ, Sachs-Ericsson N. Anxiety disorders and suicidality in the National Comorbidity Survey-Replication. J Psychiatr Res. 2009;43:825–9. doi: 10.1016/j.jpsychires.2008.12.004. [DOI] [PubMed] [Google Scholar]
- 12.Olfson M, Guardino M, Struening E, Schneier FR, Hellman F, Klein DF. Barriers to the treatment of social anxiety. Am J Psychiatry. 2000;157:521–7. doi: 10.1176/appi.ajp.157.4.521. [DOI] [PubMed] [Google Scholar]
- 13.Ansseau M, Dierick M, Buntinkx F, Cnockaert P, De Smedt J, Van Den Haute M, et al. High prevalence of mental disorders in primary care. J Affect Disord. 2004;78:49–55. doi: 10.1016/s0165-0327(02)00219-7. [DOI] [PubMed] [Google Scholar]
- 14.King M, Nazareth I, Levy G, Walker C, Morris R, Weich S, et al. Prevalence of common mental disorders in general practice attendees across Europe. Br J Psychiatry. 2008;192:362–7. doi: 10.1192/bjp.bp.107.039966. [DOI] [PubMed] [Google Scholar]
- 15.Ostergaard SD, Foldager L. The association between physical illness and major depressive episode in general practice. Acta Psychiatr Scand. 2011;123:290–6. doi: 10.1111/j.1600-0447.2010.01668.x. [DOI] [PubMed] [Google Scholar]
- 16.Bunevicius A, Peceliuniene J, Mickuviene N, Valius L, Bunevicius R. Screening for depression and anxiety disorders in primary care patients. Depress Anxiety. 2007;24:455–60. doi: 10.1002/da.20274. [DOI] [PubMed] [Google Scholar]
- 17.Simon GE, Von Korff M, Lin E. Clinical and functional outcomes of depression treatment in patients with and without chronic medical illness. Psychol Med. 2005;35:271–9. doi: 10.1017/s0033291704003071. [DOI] [PubMed] [Google Scholar]
- 18.Koyuncu A, Ertekin E, Ertekin BA, Binbay Z, Yüksel C, Deveci E, et al. Relationship between atypical depression and social anxiety disorder. Psychiatry Res. 2015;30(225):79–84. doi: 10.1016/j.psychres.2014.10.014. [DOI] [PubMed] [Google Scholar]
- 19.Martin P. The epidemiology of anxiety disorders: A review. Dialogues Clin Neurosci. 2003;5:281–98. doi: 10.31887/DCNS.2003.5.3/pmartin. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chavira DA, Stein MB. Phenomenology of social phobia. In: Stein DJ, Hollander E, editors. Textbook of Anxiety Disorders. Washington, DC: The American Psychiatric Publishing; 2002. pp. 289–300. [Google Scholar]
- 21.Mehtalia K, Vankar GK. Social anxiety in adolescents. Indian J Psychiatry. 2004;46:221–7. [PMC free article] [PubMed] [Google Scholar]
- 22.Crome E, Grove R, Baillie AJ, Sunderland M, Teesson M, Slade T. DSM-IV and DSM-5 social anxiety disorder in the Australian community. Aust N Z J Psychiatry. 2015;49:227–35. doi: 10.1177/0004867414546699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Talepasand S, Nokani M. Social phobia symptoms: Prevalence and sociodemographic correlates. Arch Iran Med. 2010;13:522–7. [PubMed] [Google Scholar]
- 24.Connor KM, Davidson JR, Churchill LE, Sherwood A, Foa E, Weisler RH. Psychometric properties of the social phobia inventory (SPIN). New self-rating scale. Br J Psychiatry. 2000;176:379–86. doi: 10.1192/bjp.176.4.379. [DOI] [PubMed] [Google Scholar]
- 25.Ranta K, Kaltiala-Heino R, Rantanen P, Tuomisto MT, Marttunen M. Screening social phobia in adolescents from general population: The validity of the social phobia inventory (SPIN) against a clinical interview. Eur Psychiatry. 2007;22:244–51. doi: 10.1016/j.eurpsy.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 26.Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–71. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- 27.Lasa L, Ayuso-Mateos JL, Vázquez-Barquero JL, Díez-Manrique FJ, Dowrick CF. The use of the beck depression inventory to screen for depression in the general population: A preliminary analysis. J Affect Disord. 2000;57:261–5. doi: 10.1016/s0165-0327(99)00088-9. [DOI] [PubMed] [Google Scholar]
- 28.Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. 1998;28:551–8. doi: 10.1017/s0033291798006667. [DOI] [PubMed] [Google Scholar]
- 29.Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35:121–6. doi: 10.4103/0253-7176.116232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Essau CA, Conradt J, Petermann F. Frequency and comorbidity of social phobia and social fears in adolescents. Behav Res Ther. 1999;37:831–43. doi: 10.1016/s0005-7967(98)00179-x. [DOI] [PubMed] [Google Scholar]
- 31.Deb S, Chatterjee P, Walsh KM. Anxiety among high school students in India: Comparisons across gender, school type, social strata, and perceptions of quality time with parents. Aust J Educ Dev Psychol. 2010;10:18–31. [Google Scholar]