

Abstract
Background:
Elderly population in India is increasing fast which indicates a growing share of population with more special needs for health and support. Understanding the morbidities and health-seeking behavior of elderly is essential for strengthening geriatric health-care services delivery.
Objectives:
The objective of this study was to study the morbidity profile of elderly in urban slum areas and assess their health-seeking behavior.
Methodology:
A cross-sectional study was conducted in urban slums of Jorhat district of Assam, among 125 elderly selected by simple random sampling.
Statistical Analysis Used:
The statistical analysis was performed by Chi-square and proportions.
Results:
The most common morbidity found was arthritis (70.4%) followed by visual impairment (58%). Majority (83.7%) were seeking treatment for their health problems. Among those elderly who did not seek treatment, the most common reasons given were “lack of money” (81.2%) and “not feeling necessary to go to doctor as conditions were age related” (62.5%).
Conclusions:
More than two-third of slum-dwelling elderly in the present study were suffering from chronic morbidities; a few could not afford proper health care due to lack of money and self-medication practices were prevalent among some. This stresses the need to provide suitable health facilities and affordable health care to the elderly in slum areas to ensure their active aging. Living arrangement of the elderly was found to have significantly influenced their health-seeking behavior. Strategic implementation of policies focusing on the problems and beliefs of slum-dwelling elderly which prevent them from seeking healthcare is the need of the hour.
Keywords: Geriatric, health-seeking behavior, morbidity
Introduction
Aging is a complex process, influenced by many factors. Biologically, aging is associated with accumulation of molecular and cellular damages over prolonged periods of times which leads to a gradual decrease in physiological functions of an individual, and therefore, aggravate the risk of diseases, infirmity, and ultimately causing death. However, these changes are not linear rather they appear randomly and are unique in every individual. It might be because these changes are strongly influenced by the surrounding environment and behaviors of the individual.[1] Health-seeking behavior is one of the influencing factors.
Globally, more than 800 million people are over 60 years or more, which represent 12% of total population.[2] In India, geriatric-aged population is 8.0% which corresponds to roughly 98 million. There are more elderly in rural areas (8.1%) than in the urban areas (7.9%), except few states including Assam, where more geriatric people lives in urban areas (6.6%) than the rural and with male predominance (6.8%).[3]
Elderly population in India is projected to rise to 12.4% of population by 2026 and to become 20% by 2050.[4] Hence, this raising percentage of elderly emerging from effects of declining fertility and increasing longevity not only indicates the success of public health measures and medical advances but also indicates huge impact on socioeconomic and health structure of a developing country like India.[5] With the increased share in the geriatric age group, the increase among the oldest age of 80 years and above is also high (0.8%) who have more special needs for health and support. The old age dependency ratio (12%) is also showing an upward trend in India. With differential lifespan of men and women among the oldest geriatric age group, the sex ratio continues to rise to become as high as 136 women per 100 men by 2026. This trend poses more specific challenges relating to very old-widowed women. High levels of illiteracy, particularly among older women in rural areas, are yet another aspect of vulnerability for senior citizens in India.[6]
In India, major illnesses of elderly include communicable as well as noncommunicable diseases; hearing, visual impairment and locomotor disabilities also contribute a major chunk. The prevalence of heart diseases was found to be more among elderly people living in urban areas, they are also more prone to mental morbidities due to breakdown of social and family structures and changes associated with rapid urbanization.[7]
The health problems of elderly are often chronic and disabling requiring multiple drug treatment, physiotherapy, and long-term rehabilitation. However, dedicated geriatric health care in India is still a distant dream because of lack of specialized and trained workforce and absence of an infrastructure beyond tertiary care hospitals.[8] However, apart from health infrastructure peoples, own health-seeking behaviors influence greatly the healthy elderly and active aging. When elderly people take care of their problems at appropriate time and approach the health system, the problems can be managed properly and there are lesser chances of complications or advanced diseases. Health-seeking behaviors of elderly are influenced by a variety of factors such as socioeconomic conditions, age, social status of the person, gender, authority of the elderly within the family, financial security of elderly, their own perceived health status and illness, type of illness, and access to services.[9]
Therefore, proper understanding of the morbidity pattern among elderly and the factors influencing the health-seeking behaviors of elderly is very essential so that the emerging situation in our country can be properly addressed with strengthening of geriatric health-care services and service delivery according to the needs with mitigation of the existing lacunae. Hence, this study was proposed to be conducted in urban slum areas of North Eastern state of Assam, with the following objectives to study the morbidity profile of elderly in urban slum areas, to describe the sociodemographic characteristics of the elderly population, and to find out the health-seeking behavior of elderly population residing in the slum areas.
Methodology
Study type, study area, and study population
A community-based cross-sectional study was conducted in the urban slum areas of Jorhat district of Assam. Jorhat is an important district in Assam and is gateway to the other North Eastern State of Nagaland. The district is situated around 300 km north of the State Capital City of Guwahati, and it is spreading over 2851 km2, with a population of 1092,256 as per the 2011 census. For our study, we randomly selected five slum areas among the total seven notified slums in the district.
Eligibility criteria
Elderly persons aged 60 years and above who were permanent residents of the area and gave informed consent to be part of our study were eligible to participate in our study.
Exclusion criteria
Those geriatric people who were not permanent residents of the area, who did not give consent to participate, and those critically ill elderly who were unable to respond to interview schedule were excluded from the study.
Sample size and sampling design
For sample size calculation, we applied the formula 4 pq/e2, where we had takenP as 47% as prevalence of morbidity among elderly.[10] Considering permissible error (e) of 19% of prevalence, the minimum sample requirement was 125. A two-stage simple random sampling design was adopted.
Out of the total 7 notified slums, 5 were selected by simple random sampling (first stage units). To get the desired sample size of 125 elderly, 25 sample units were required from every slum. Hence, a total of 25 participants (second stage units) were selected from each of the 5 slums. For every selected slum, one house was selected randomly and surveyed for elderly residents. Only one such respondent from each family was included in our study. Initiating from this house, every next nearest house was surveyed till 25 participants meeting with the eligibility criteria were obtained for the study. The study was finally conducted among 125 numbers of participants.
Ethical clearance and data collection
The study proposal was approved by the Institutional Ethics Committee. The study period was from August 2015 to January 2016. Three-month recall period from the date of interview was considered for our study.
Predesigned and pretested interview schedule was used for data collection. Data on sociodemographic factors that included age, gender, marital status, level of education, type of family, and living arrangement were collected. The schedule was pretested among thirty elderly persons who were not part of our study. Each respondent was interviewed and a thorough clinical examination was done including blood pressure measurement with sphygmomanometer. Blood glucose estimation of each respondent was done through glucometer.
Self-reported general health status of the elderly: Every respondent was asked the question, “In general, how would you rate your health today?” The responses were categorized into three groups: good (including respondent choices “very good” and “good”), moderate, and bad (including “very bad” and “bad”).[11]
Provisional diagnosis of diseases of elderly was made based on reported symptoms, clinical evaluation by investigators and available prescriptions, investigation reports with the respondents. Only chronic disease conditions were considered for our study.
Only those respondents, who were found to have any health problem, were inquired about their health-seeking behavior.
For this study, health-seeking behavior was defined as sequence of remedial actions taken by the person to rectify perceived ill-health.[12] Appropriate or desired health-seeking behaviors were defined as seeking treatment and health advice through trained doctors (both allopathic and AYUSH) from public or private health facilities (government hospital, private clinic).
Self-medication was defined for our study as the practice whereby individuals treat their ailments and conditions with medicines without consulting any health-care provider.[13]
The data were collected in our study through personal interviews by house-to-house visits after taking informed consent from the participants. The data collected were compiled, refined, and entered into Microsoft Excel software. For statistical analysis, SPSS Statistics for Windows, (Version 17.0. SPSS Inc. Chicago, US) was used.
Results
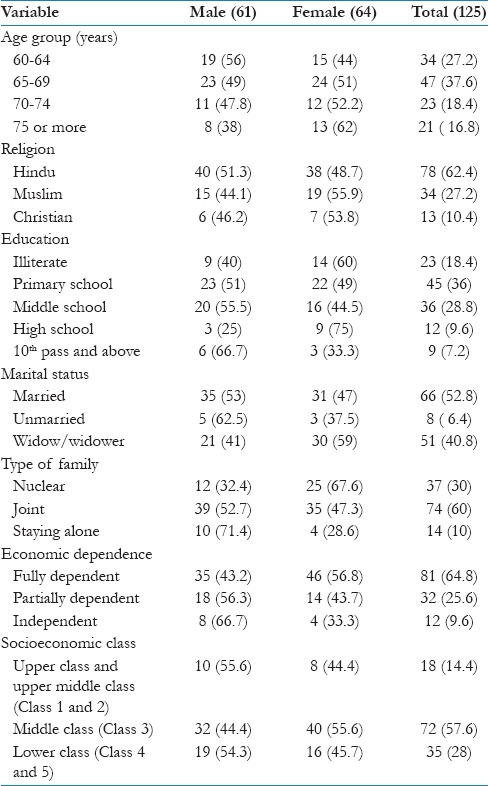
In Table 1, we analyzed the sociodemographic profile of the respondents. Out of the 125 elderly interviewed, 61 (48.8%) were male while 64 (51.2%) were female. Most of them (37.6%) were in the age group of 65–69 years and 21 (16.8%) respondents were 75 years or more. 62.4% of elderly were Hindus and 27.2% were Muslims. Most of the respondents were educated up to primary school only while 18.4% were illiterate and 7.2% had studied beyond Class 10. Illiteracy was more among elderly women (60%) than elderly men (40%). Out of 125 elderly, 66 (52.8%) were married and living with their spouses, 51 (40.8%) were living without their spouses, and 8 (6.4%) were unmarried. We found that 10% of elderly were staying alone, 60% were in joint families, and the rest 30% were in nuclear families. On analysis of financial dependence of elderly, we found that 64.8% were fully dependent on family, more females than males were dependent. 25.6% were partially dependent and 9.6% were financially independent. In our study, most elderly (57.6%) belonged to upper lower socioeconomic status according to modified BG Prasad Classification.
Table 1.
Distribution of the respondents according to their sociodemographic characteristics
In Table 2, we analyzed the morbidity profile of elderly people living in urban slum areas. Based on their history, clinical evaluation, laboratory test reports, and doctors prescriptions, we found that out of 125 elderly people, 98 (78.4%) had chronic morbidities during the study period. Many elderly were suffering from multiple morbidities at the time. Arthritis (70.4%) was found to be the most common morbidity followed by visual impairment (58%) and acid peptic diseases (56%). More women (64%) were suffering from arthritis than men. We did not consider any acute disease in our study. The study also found that 15 (0.8%) people were suffering from tuberculosis and 3 (2.4%) from cancer, and they were under treatment at that time. Most of the morbidities were found more among older men than women.
Table 2.
Distribution of elderly population according to the morbidity status (multiple responses)

We asked the respondents the question, “In general, how would you rate your health today?” The responses were analyzed and found that 25.6% reported their general health status as “good” while most elderly (56.8%) reported their health as “moderate” and 22% elderly rated their health condition as “bad” [Table 3].
Table 3.
Distribution of elderly according to their self-reported general health status

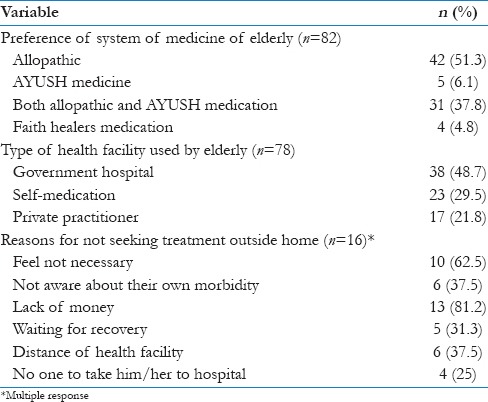
In Table 4, we analyzed the health-seeking behavior of all those elderly who reported having some morbidity or those diagnosed as having morbidity by the investigators. Among 98 elderly having some chronic morbidity, 82 (83.7%) sought health advice and treatment outside home. 51.8% preferred allopathic medicine for their illness, 37.8% used both allopathic and AYUSH medication for their problems, while 4.8% used medications bought from traditional healers. We inquired about type of health facilities used by elderly and found that 38 (48.7%) went to government health facility which include medical college and urban health center. Twenty-three (29.5%) elderly practiced self-medication and 21.8% elderly went to private practitioners for treatment. The study also found that total 16 (16.3%) individuals out of 98 elderly who had any morbidity during the study period did not seek any health advice and treatment outside home. “Lack of money” (81.2%) and “not feeling necessary to go to doctor as the conditions were age related” (62.5%) were two most common reasons for not seeking outside help for their morbidity.
Table 4.
Distribution of elderly population according to their health-seeking behaviors
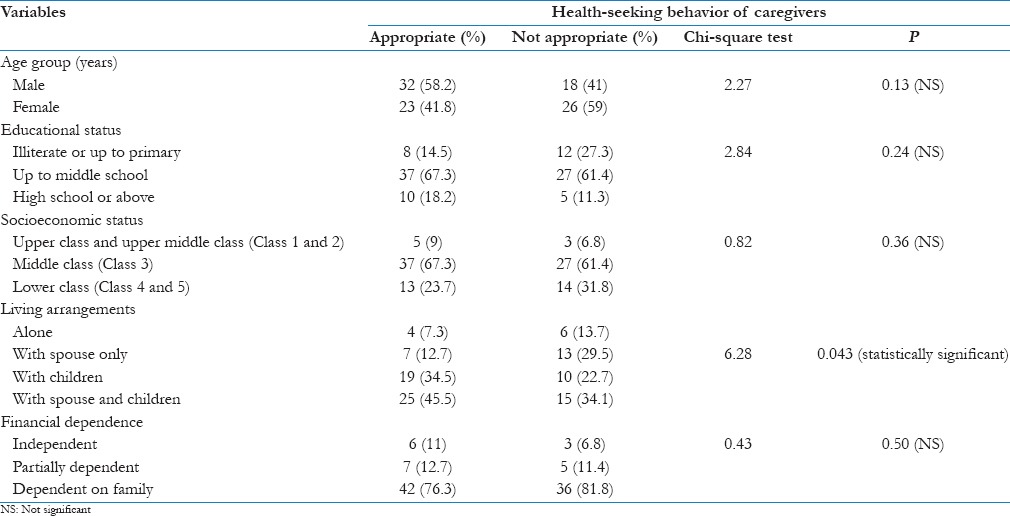
In our study, we analyzed the different factors influencing health-seeking behavior of the elderly. Health-seeking behavior of elderly was categorized as appropriate and inappropriate. It was found that out of 98 individuals having any kind of morbidity at the time of study, 55 (56.1%) elderly showed appropriate health-seeking behavior while 44 (44.9%) elderly showed inappropriate health-seeking behavior regarding their morbidities. In the Table 5, we analyzed the different factors influencing health-seeking behavior of elderly in slum areas. We found that appropriate health-seeking behavior was shown more by elderly males (58.2%) than females (41%). More illiterate and those elderly educated up to primary schools (27.3%) and those elderly belonging to lower socioeconomic status (31.8%) demonstrated inappropriate health-seeking behavior. On analysis of living arrangements of elderly and health-seeking behavior, we found that those elderly staying with their spouse and children (45.5%) have appropriate health-seeking behavior. While those elderly who stayed alone, their health-seeking behavior (13.7%) was found to be inappropriate in our study. On Chi-square analysis, we found that living arrangement has a statistically significant association with health-seeking behavior of elderly. The association between gender, educational status, socioeconomic status, financial dependence, and health-seeking behavior was found to be statistically not significant.
Table 5.
Factors influencing health-seeking behaviors of the caregivers
Discussion
The present study conducted among elderly population living in urban slum areas of Jorhat Town of Assam found some valuable findings regarding their morbidity profile and health-seeking behavior. Out of 125 elderly respondents in our study, 48.8% were male and 51.2% were females. Most of the respondents were educated up to primary school. 10% of the total elderly were staying alone, 60% were in joint families, and rest 30% were in nuclear families. 64.8% of elderly were fully dependent on family, more females than males were dependent on others. Most of the respondents in our study (57.6%) were from low socioeconomic status. According to Government of India report 2016, nearly 104 million elderly persons (aged 60 years or above) were in India; out of them, 53 million females and 51 million males. The old age dependency ratio was 14.2% in 2011. The report also revealed that 65% of the aged persons had to depend on others for their day-to-day maintenance. The situation was worse for elderly females than the males. More than 56% of elderly lived with their spouse and 32% of aged persons live with their children while about 5% of elderly persons live alone.[3]
In the study, we found that out of 125 elderly people, 78.4% were suffering from at least a chronic morbidity at the time. Similar findings were observed in previous studies conducted among elderly population in urban slums.[14,15] This high prevalence of morbidity might be an indicator of poor general health condition of inhabitants of slums areas. Marimuthu et al. in their study attribute the poor health condition of slum-dwellers to illiteracy, poor environmental conditions, and lack of proper health facilities.[16] Slum areas are still not properly covered by government health infrastructure which might also contribute to high morbidity among elderly. Many studies conducted in Indian slums found lack of health facilities in slum areas.[17]
The study observed that arthritis (70.4%) was the most common morbidity among elderly followed by visual impairment (58%) and acid peptic diseases (56%). In the study, many elderly were found to be suffering from multiple morbidities at the same time. A study by Thakur et al. found that visual impairment was the most common morbidity among elderly with the prevalence of 83.3% and 44% respondents suffering from arthritis.[18] The most prevalent morbidities among elderly in urban slum areas observed by Thomas et al. were hypertension (46.9%) followed by arthritis (30.2%), diabetes (26.5%), respiratory problem (24.3%), and cataract (21%).[10]
Elderly men were found to be suffering from more illnesses than elderly females in our study. Although the study indicated a high prevalence of morbidity among elderly, only 22% of elderly rated their health condition as “bad,” 25.6% reported their general health status as “good,” while most elderly (56.8%) reported their health as “moderate.” The WHO Global Ageing and Adult Health Study in India also observed that among older respondents (aged 50-plus), 31% reported their health status as good while nearly half (47%) considered their health to be moderate and rest reported their health status as poor.[11] Similar results were obtained by Thomas et al. but Joshi et al. in their study in Kolkata found that more than 80% of elderly felt themselves as ill.[10,19]
In our study, 83.7% elderly sought health advice and treatment outside home for their morbidities. Most elderly (51.8%) used allopathic medication for their problems. The study also found that most elderly (48.7%) in slums preferred government health facilities and 29.5% elderly practiced self-medication. Lower socioeconomic condition of most elderly in our study might contribute to the preference of government health facilities but as government health infrastructure is not well equipped in slum areas; therefore, self-medication practices were also found to be high among the elderly. Sharma et al. in their study among elderly population in North India found that majority of the older persons preferred allopathic medicine (81.2%) followed by ayurvedic medicines (11.3%). Most of the older persons also preferred government hospital for treatment of their morbidities.[20]
It was found that 56.1% elderly showed appropriate health-seeking behavior in our study. Appropriate health-seeking behavior was found more among elderly males, those having higher educational status and elderly staying with their spouse and children. While those elderly who stayed alone, illiterate elderly, those belonging to lower socioeconomic status, their health-seeking behavior was found to be inappropriate in our study. Further, our study found only the living arrangement of elderly to be statistically associated with health-seeking behavior of elderly. Dey et al. in their article on health status of elderly in India observed that barriers, such as gender, religion, caste, socioeconomic status, social stigma, and economic dependence, hamper the access of elderly population to health-care services.[9] Gender bias in treatment-seeking behavior of elderly was also observed by Kishore et al. in their study in Uttarakhand.[21]
Conclusions
With the increase in elderly population in India, the burden of chronic morbidity, disability, and mortality is also on the rise, but still there is inadequate data on geriatric population because routine data collection in India is still not sensible to morbidity, pathological progression, and disability outcomes among elderly.[19] Therefore, community-based studies on morbidity and health-seeking behavior of elderly, especially among urban poor might be an important data source. Although our study was conducted with a small sample and only few variables were considered important findings that emerged from our study include: most elderly in slum areas were fully dependent on their families, a sizeable portion of elderly were staying alone, more than two-third of our study population were suffering from chronic morbidities at the time of the study with male predominance. Health-seeking behavior was appropriate for 56.1% of the elderly while a few could not afford proper health care due to lack of money; self-medication practices are prevalent among some elderly. This highlights the need to provide suitable health facilities and affordable health care to the elderly in slum areas to ensure their active aging. Living arrangement of elderly was found to have significantly influenced the health-seeking behavior of elderly living in slum areas of Jorhat town. There must be strategic implementation of policies focusing on the problems and beliefs of slum-dwelling elderly, which prevent them from seeking health care.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We gratefully acknowledge the participants for their cooperation in the study.
References
- 1.Rodríguez-Rodero S, Fernández-Morera JL, Menéndez-Torre E, Calvanese V, Fernández AF, Fraga MF. Aging genetics and aging. Aging Dis. 2011;2:186–95. [PMC free article] [PubMed] [Google Scholar]
- 2.New York: United Nations; 2013. United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2013; pp. 9–11. [Google Scholar]
- 3.New Delhi: Central Statistics Office, Ministry of Statistics and Programme Implementation, Govt. of India; 2016. Govt. of India. Elderly in India - Profile and Programmes 2016; pp. 26–9. [Google Scholar]
- 4.Aronkar C. Aging of population in India and need for wider social security scheme. Int J Soc Sci Interdiscip Res. 2012;1:199–203. [Google Scholar]
- 5.New Delhi: Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India; 2012. Govt. of India. National Programme for the Health Care of the Elderly (NPHCE): An Approach towards Active and Healthy Ageing; pp. 2–4. [Google Scholar]
- 6.Subaiya L, Bansod DW. New Delhi: United Nations Population Fund (UNFPA); 2011. Demographics of Population Ageing in India: Trends and Differentials, BKPAI Working Paper No. 1; pp. 4–7. [Google Scholar]
- 7.Ingle GK, Nath A. Geriatric health in India: Concerns and solutions. Indian J Community Med. 2008;33:214–8. doi: 10.4103/0970-0218.43225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Evans JM, Kiran PR, Bhattacharyya OK. Activating the knowledge-to-action cycle for geriatric care in India. Health Res Policy Syst. 2011;9:42. doi: 10.1186/1478-4505-9-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dey S, Nambiar D, Lakshmi JK, Sheikh K, Reddy KS. Health of the elderly in India: Challenges of access and affordability. In: Smith JP, Majmundar M, editors. Aging in Asia: Findings from New and Emerging Data Initiatives. Washington, DC: The National Academies Press; 2012. pp. 371–83. [PubMed] [Google Scholar]
- 10.Thomas V, Lavanya KM, Muraleedhar Morbidity profile and health seeking behaviour of the elderly in urban slums of Hyderabad, Andhra Pradesh, India – A cross sectional study. Int J Curr Res Rev. 2012;4:174–80. [Google Scholar]
- 11.Geneva: World Health Organization; 2013. WHO. Study on Global Ageing and Adult Health (SAGE) Wave 1: India National Report; pp. 97–101. [Google Scholar]
- 12.MacKian S. Manchester: University of Manchester; 2003. A Review of Health Seeking Behaviour: Problems and Prospects. HSD/WP/05/03. Health Systems Development Programme; pp. 5–7. [Google Scholar]
- 13.Marak A, Borah M, Bhattacharyya H, Talukdar K. A cross-sectional study on self-medication practices among the rural population of Meghalaya. Int J Med Sci Public Health. 2016;5:1134–8. [Google Scholar]
- 14.Singh JP, Singh S, Kasturwar NB, Hassan A. Geriatric morbidity profile in an urban slum, central India. Indian J Community Health. 2013;25:164–70. [Google Scholar]
- 15.Srivastava K, Sharma P, Gupta SC, Kaushal SK, Chaturvedi M. Determinants of health of aged population: A cross-sectional study. Indian J Prev Soc Med. 2012;43:428–32. [Google Scholar]
- 16.Marimuthu P, Meitei MH, Sharma B. General morbidity prevalence in the delhi slums. Indian J Community Med. 2009;34:338–42. doi: 10.4103/0970-0218.58395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gupta I, Guin P. Health status and access to health services in Indian slums. [Last accessed on 2017 Jan 15];Health. 2015 7:245–55. Available from: http://www.dx.doi.org/10.4236/health. 2015.72029 . [Google Scholar]
- 18.Thakur R, Banerjee A, Nikumb V. Health problems among the elderly: A cross-sectional study. Ann Med Health Sci Res. 2013;3:19–25. doi: 10.4103/2141-9248.109466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Joshi K, Kumar R, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. Int J Epidemiol. 2003;32:978–87. doi: 10.1093/ije/dyg204. [DOI] [PubMed] [Google Scholar]
- 20.Sharma D, Mazta SR, Parashar A. Morbidity pattern and health-seeking behavior of aged population residing in Shimla hills of North India: A cross-sectional study. J Family Med Prim Care. 2013;2:188–93. doi: 10.4103/2249-4863.117421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kishore S, Sharma K, Singh R, Gaur BP. Chronic morbidity and health care seeking behaviour amongst elderly population in rural areas of Uttarakhand. Indian J Community Health. 2015;27:252–6. [Google Scholar]