

Abstract
Introduction:
Health indicators of rural and urban India show a wide variation. Rural areas have received large focus in child health services, but on the flip side, urban areas have been the last to receive such attention.
Materials and Methods:
A cross-sectional study was conducted to include one randomly selected outreach session from all the 19 urban primary health centers of Vadodara city from April 2013 to May 2014. Nineteen session sites were observed for the process evaluation of three components of child health care, namely, “planning of Health and Nutrition Day,” “availability of vaccines/logistics,” and “direct observation of actual immunization process” at the site using a structured checklist.
Results:
Most of the vaccines and logistics were present at all 19 sites visited, but adverse events following immunization kit were observed at ten sites (52%) only. Open vial policy, no-touch technique, and immediate cutting of syringe with hub cutter were implemented at all sites; however, completely filled Mamta Card was observed at 9 (47%) sites only. All four key messages were given at 5 (26%) sites only.
Conclusion:
Immunization services such as proper vaccine administration with no-touch technique and open vial policy were mainly focused; however, other services such as biomedical waste management, record keeping, and delivery of all four key messages need to be strengthened during Mamta Divas. Strengthening of other child health care services such as growth monitoring, Integrated Management of Neonatal and Childhood Illnesses, and referral services is required in urban areas.
Keywords: Health and nutrition day, immunization, process evaluation, urban slums
Introduction
There have been wide rural and urban differences in India, especially when we look at various health indicators. One such remarkable difference has also been observed in infant mortality rate (IMR) which is the most commonly used indicator to assess the child health. The current IMR is 27/1000 live births in urban India while 44/1000 live births in rural India making an average of 40/1000 live births, whereas in Gujarat, it is 36/1000 live births.[1] Improving child health is one of the important goals among all the Millennium Development Goals (MDGs). The Government of Gujarat aims to achieve these MDGs first in the state of Gujarat.[2] Vaccines are considered to be one of the best weapons to combat against under-five mortality.[3] Immunization is one of the most important measures help us in achieving MDG 4 (reduce under-five mortality).[4]
Integrated Nutrition and Health Project gave the concept of Nutrition and Health Day which has been widely replicated across the nation in various forms such as Mamta Abhiyan since 2005. Mamta Abhiyan includes five components: Mamta Day (Health and Nutrition Day), Mamta mulakat (postnatal care visit), Mamta Sandarbh (referral services), Mamta Nodh (record and reports), and Mamta Taruni (adolescent health). Mamta Day is the Gujarat version of what is nationally known as Village Health and Nutrition Day.[5] During this Mamta Day, a special focus is given on the child health services and specifically immunization services in the particular area of village or city. In city areas, these services are not only provided at urban primary health centers but also through outreach sessions in the form of Mamta Day. This is usually done at an Anganwadi center located within a slum/semi-slum area of the city.
The current study is carried out with an objective to evaluate child health services focusing on immunization at outreach session sites during Health and Nutrition Day (Mamta Day) in urban slums of Vadodara city.
Materials and Methods
Vadodara is the third most populous city in Gujarat and situated in the central part of the state. The health services of Vadodara city are provided by a network of 19 urban health centers run by Vadodara Municipal Corporation which is an urban local self-governance body. Each of these centers caters to the population in their assigned geographic area. The major beneficiaries of the services provided by these centers are those people residing in slum and semi-slum areas within the jurisdiction of the respective urban health center. These urban health centers organize a Health and Nutrition Day (Mamta Day), mainly for children, mothers, and adolescents once a month in these slum and semi-slum areas at Anganwadi centers. In this cross-sectional observational study, one outreach session site from each urban health center was randomly selected from the microplan of each of the 19 urban health centers of Vadodara city to cover all the urban health centers. Thus, we had observed a total of 19 Mamta Day sessions for this study. Since the Mamta Day is held on a fixed day (commonly Wednesday), the process evaluation could be done only on the days when the session was organized. Hence, the data collection for the study was from April 2013 to May 2014.
The visits were conducted as a part of regional monitoring teamwork for monitoring the Reproductive Maternal Newborn Child Health plus Adolescent program by the faculty of Community Medicine Department of Medical College in an assigned corporation. Necessary permission was given from the state government to monitor these activities and also they had given necessary instructions to local health authorities for providing support and information.
We have covered three components for the process evaluation, namely, the planning of Mamta Day at session site, availability of vaccines/logistics/supplies at session site, and the direct observation of the entire vaccination process at the site. The structured checklist was based on the Guidelines for Immunization Services by the Government of India, Mamta Abhiyan Guidelines prepared by the state of Gujarat, as well as Village Health and Nutrition Day Guidelines by the Government of India.[5,6,7]
The process evaluation of each Health and Nutrition Day was done using the structured checklist on the day of actual session at the site. Data collection was done by a single observer to avoid interobserver bias. Adequate time was given to observe each component of child health services provided during Health and Nutrition Day. It was ensured that the data collection does not interfere with the ongoing services. The staff members briefed about the nature and purpose of the exercise beforehand, and consent was taken from the clients at the outreach session. On-site corrective measures were taken as and when required, and feedback was given to local staff, medical officer, and local health authorities for the improvement of the quality of services.
Data were entered and analyzed using Microsoft Office Excel worksheet. This being a descriptive study, it reports actual numbers and proportions in the form of percentages of the study variables. Statistical tests for significance have not been applied.
Results
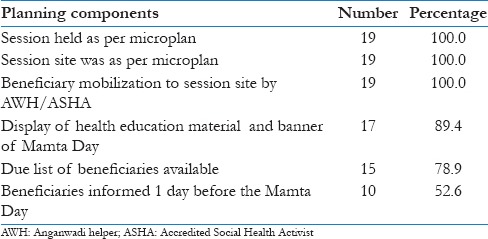
A total of 19 Health and Nutrition Day sessions at various Anganwadi centers under the urban primary health centers have been included in the study. As shown in Table 1, all 19 sessions were held as per microplan at the mentioned session sites. Beneficiaries were mobilized by the urban Accredited Social Health Activist (ASHA) or Anganwadi Helper (AWH) at all session sites visited; however, at only 10 (52.6%) sites, the beneficiaries were informed a day ahead of the session. Mamta Day banner was displayed at 17 (89.4%) out of 19 session sites visited. Only 15 sites had a list of due beneficiaries.
Table 1.
Planning of Mamta Day at session site (n=19)
We had asked about the availability of various logistics including vaccines and other essential items. Table 2 provides information regarding the availability of items related to child health component of the services. While collecting this information, it was decided that if any item is not available in sufficient quantity as per the demand or the item/instrument is not in functioning condition, then it would be considered as not available.
Table 2.
Availability of vaccines/logistics at session site (n=19)
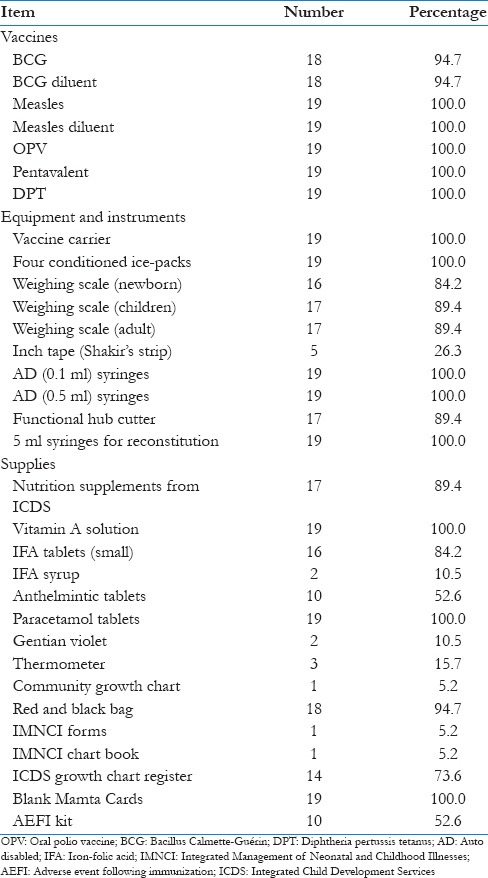
As shown in Table 2, measles, oral polio vaccine, pentavalent, and diphtheria pertussis tetanus (DPT) vaccines were available at all 19 sites whereas Bacillus Calmette–Guérin (BCG) vaccine and its diluent were not available at one site. Other essential logistics such as vaccine carrier, a weighing scale for newborns and older children, auto-disable syringe (0.1 and 0.5 ml), functional hub cutter, and 5 ml syringes for reconstitution were available at most of the session sites; however, Shakir's strip (inch tape/measuring tape) was available at five sites only. Some other supplies such as Vitamin A solution, paracetamol tablets, Blank Mamta Cards, Integrated Child Development Services growth chart registers, and red-black bag for biomedical waste were available at majority of the session sites; however, community growth chart, thermometer, Integrated Management of Neonatal and Childhood Illnesses (IMNCI) forms/chart booklets, and iron and folic acid syrup were available at one or two sites only. A kit for adverse events following immunization (AEFI) was available at 10 (52.6%) sites only.
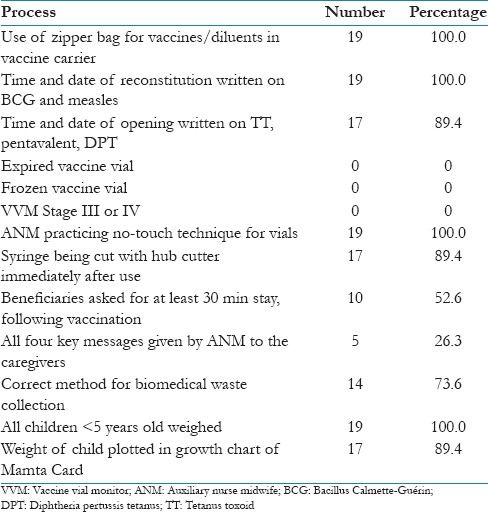
Table 3 shows the process observation of various child health services focusing on immunization. The use of zipper bags in vaccine carrier, writing of time and date of reconstitution and opening on the vaccine vials, and no-touch technique were practiced by auxiliary nurse midwife (ANM) at almost all session sites. No vial had crossed the expiry date or was frozen or in Stage III/IV in vaccine vial monitor (VVM) at any site. However, all four key messages of immunization were given to the mothers of beneficiaries at 5 (26.3%) sites only. Beneficiaries were asked to stay for 30 min after vaccination at 10 (52.6%) sites only. Although all children <5 years were weighed at all sites, it was plotted correctly in Mamta Card at 17 (89.4%) sites only.
Table 3.
Process evaluation of the immunization and other child health services (n=19)
Discussion
The Health and Nutrition Day, popularly known as Mamta Day in Gujarat, is being celebrated once a month at every Anganwadi center in urban areas which focuses on pregnant women, lactating mothers, children under 5 years, and adolescent girls as target groups. From among these target groups, the current study has focused on the process evaluation of the child health services and especially immunization at the Health and Nutrition Day sessions. The planning of Mamta Day was good with all urban primary health centers having and adhering to the microplan. Similar observation of all sessions held as per microplan was also made by Kotecha and Singh in Bhavnagar city of Gujarat.[8]
Mobilization of beneficiaries is one of the important activities, which is a reminder to the mothers of beneficiaries to take their children to the Anganwadi center for immunization. Although, at all session sites, beneficiaries were mobilized either by urban ASHA or by AWH, at only 10 (52.6%) sites, reminder was given a day ahead of Mamta Day. Contrary to this, in a study conducted by Parmar et al. in rural area of Vadodara district, the beneficiaries were informed 1 day before the Mamta Day at almost 93% session sites.[9]
Display of Mamta Day banner at the session site is necessary, so that the nearby people can come to know the exact location of the session site. Display of banner should be at such place which can be visible to all. It was displayed at 17 sites out of 19 session sites visited. It is the duty of the ANM/female health worker (FHW) to prepare the list of the beneficiaries' due for vaccination on the given day. The state of Gujarat uses the Mother and Child Tracking Software named E-Mamta (developed by National Informatics Center, New Delhi, India). This software gives a list of due beneficiaries for various services including immunization. Such due list of beneficiaries was available at 15 sites only. Whereas in a study conducted by Parmar et al., the due list of beneficiaries was available at only 1 site out of 13 sites visited by them in the rural areas of Vadodara.[9]
The different logistics and supplies pertaining to child health should be present in adequate quantity at all the session sites as per Health and Nutrition Day Guidelines. Vaccines including BCG, measles, pentavalent, and DPT were found available at almost all sites in this study. Similar finding was observed by Kotecha and Singh et al. and Shah et al. in Bhavnagar and Ahmedabad municipal corporations of Gujarat state, while in a study by Saxena et al. in Uttarakhand district, vaccines were found available at 70% sites only.[8,10,11] This difference may be due to differences in the state-level policies in the supply and distribution of vaccines to their health centers. Vaccine carrier and four conditioned ice-packs were observed at all session sites visited which was a highly appreciable finding. Similar findings were also noted by the studies conducted in urban area by Kotecha and Singh and in rural area by Parmar et al.[8,9] AEFI kit is very vital in case of any adverse event following immunization. It was not available at nearly half of the sites visited in this study which is a major concern. A study by Parmar et al. also reports that AEFI kit was not available at any of the 13 session sites visited by them.[9]
Growth monitoring is also one of the essential components of child health services. Although weighing scale for children was present at 16 sites, inch tape/Shakir's strip which is used for measuring mid-upper arm circumference in children was present at 5 sites only. Community growth chart for explaining the mother regarding nutrition status of her child was present at one (5.2%) site only. A similar finding was observed by Saxena et al. that only site had community growth chart in the state of Uttarakhand.[11] Kotecha and Singh have observed community growth chart at almost 1/4th of the session sites visited in Bhavnagar city.[8]
Coming to the direct process observation of child health services, especially immunization, writing of date and time of opening, the vaccine vial is very vital for those vaccines where open vial policy is followed. Moreover, since BCG and measles vaccines have to be used within 4 h of its reconstitution, it is very important to mention the date and time of reconstitution on these vials as well. Apart from these cold chain indicators, VVM stage of the vaccine vial is also to be checked by the ANM/FHW before giving the vaccine to any child. Such practices of writing date and time on the vaccine vials were observed at 17 (89.4%) session sites, while for vials of BCG and measles, it was observed at all 19 (100%) session sites. A similar finding of writing date and time on all BCG and measles vials was observed by Khandhedia et al. in Rajkot district.[12] The similar practice of writing the time of reconstitution on vaccine vial was observed at 75% of urban health centers by Naik et al. in Surat city.[13] Contradictory to this, a study by Parmar et al. observed such practice of writing date and time on the vaccine vial at 60% sites only in rural Vadodara.[9] None of the session sites visited had vaccine without label/unreadable label, with expired date, in frozen state or VVM Stage III/IV. A similar finding was also noticed by Kotecha and Singh et al. and Gandhi et al. in Bhavnagar and Surat Municipal Corporation, respectively.[8,14]
ANM has to give four key messages related to vaccination to the caregivers (mothers of beneficiaries) and has to advice to stay for at least 30 min after vaccination, so as to detect and manage AEFIs at the earliest. In this study, at 10 (52.6%) session sites, ANMs were asking the mothers of the beneficiaries to stay for 30 min after vaccination, while at only 5 (26.3%) sites, all four key messages were given to the caregivers. Similar findings were observed in studies by Kotecha and Singh et al. and Parmar et al. too.[8,9] A similar finding was also observed by Rajkumari et al. in Hyderabad.[15] Such findings clearly indicate that there is a need to improve interpersonal communication skills of ANM with the caregivers.
Although all children <5 years were weighed at all sites, correct plotting of weight in Mamta Card was done at 17 (89.4%) sites only. With regard to the record keeping, filling up of relevant details in Mamta Card was adequate. All sessions had the maternal and child health services register (Register No. 4 and 5) available at session site. These registers were updated on a daily basis which was again a good practice observed. Such good practices of record keeping were also observed by Kotecha and Singh et al. in Bhavnagar, Gujarat.[8]
Limitations
The actual service delivery was observed for immunization which may have introduced participation bias as the providers' behavior may change in the presence of an observer. However, this was unavoidable. We have focused more on the immunization services in this paper, while the other services may include care of sick children and referral as well as growth monitoring.
Conclusion
Planning of the immunization services at the Village Health and Nutrition Day was largely satisfactory. With regard to the availability of supplies, although majority of the essential items were found to be available, focus needs to be given to AEFI kit, thermometer, measuring tape/Shakir's strip, and community growth chart since they were not available at many sites. With regard to the immunization, although the injection technique was good, the biomedical waste management and communication with the client need to be strengthened. Furthermore, the focus should be given to the IMNCI and growth monitoring services.
Financial support and sponsorship
We would like to acknowledge the Ministry of Health and Family Welfare, Government of Gujarat, for financial support to carry out RMNCH + A activities.
Conflicts of interest
There are no conflicts of interest.
References
- 1.SRS Statistical Reports 2014. Sample Registration System, Office of Registrar General; New Delhi, India. [Last accessed on 2016 Feb 08];2014 49 Available from: http://www.censusindia.gov.in/vital_statistics/SRS_Statistical_Report.html . [Google Scholar]
- 2.New Delhi: SEAR, WHO; 2009. WHO. High-Level Consultation to Accelerate Progress towards Achieving Maternal and Child Health Millennium Development Goals (MDGs 4 and 5) in South-East Asia. [Google Scholar]
- 3.Stanley A, Plotkin W, Paul A. Vaccines. 5th ed. Philadelphia, USA: Saunders; 2008. [Google Scholar]
- 4.3rd ed. Geneva: World Health Organization; 2009. World Health Organization. State of the World's Vaccines and Immunization. [Google Scholar]
- 5.Government of Gujarat. MAMTA Abhiyan Guidelines. Gandhinagar: Ministry of Health and Family Welfare, Government of Gujarat. 2006 [Google Scholar]
- 6.New Delhi: Ministry of Health & Family Welfare, Government of India; 2006. Government of India. Immunization Handbook for Health Workers. [Google Scholar]
- 7.New Delhi: Ministry of Health and Family Welfare, Government of India; February; 2007. [Last accessed on 2016 Sept 12]. Government of India. Monthly Village Health and Nutrition Day – Guidelines for AWWs/ASHAs/ANMs/PRIs. Available from: http://www.nrhm.gov.in/images/pdf/communitisation/vhnd/vhnd_guidelines.pdf . [Google Scholar]
- 8.Kotecha I, Singh MP. Process evaluation of health and nutrition day (Mamta Day) in Urban Slum Areas of Bhavnagar Municipal Corporation. Natl J Integr Res Med. 2012;3:111–4. [Google Scholar]
- 9.Parmar A, Parmar N, Pandya C, Mazumdar VS. Process evaluation of routine immunization (RI) and growth monitoring services during Mamta Day (Village Health and Nutrition Day) in Sinor block of Vadodara District, Gujarat, India. Natl J Community Med. 2014;5:378–82. [Google Scholar]
- 10.Shah J, Agarwal M, Patel J, Trivedi A. Quality assessment of immunization services: A cross sectional study at UHCs of Ahmedabad Municipal Corporation. International J Health Sci Res. 2015;5:21–5. [Google Scholar]
- 11.Saxena V, Kumar P, Kumari R, Nath B, Pal R. Availability of village health and nutrition day services in Uttarakhand, India. J Family Med Prim Care. 2015;4:251–6. doi: 10.4103/2249-4863.154667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Khandhedia SA, Ninama RD, Kadri AM. Quality assessment of immunization services at village health and nutrition day (VHND) in the rural areas of Rajkot district, Gujarat, India. Int J Interdiscip Multidiscip Stud. 2015;2:15–9. [Google Scholar]
- 13.Naik AK, Rupani MP, Bansal RK. Evaluation of vaccine cold chain in urban health centers of municipal corporation of Surat city, Western India. Int J Prev Med. 2013;4:1395–401. [PMC free article] [PubMed] [Google Scholar]
- 14.Gandhi SJ, Dabhi M, Chauhan N, Kantharia S. Assessment of maternal and child health services during Mamta Days in urban areas of Surat city. Int J Med Sci Public Health. 2016;5:1199–203. [Google Scholar]
- 15.Rajkumari HK, Hira P, Rithuma O, Murthy GV, Ajitha K, Suresh M. Evaluating the fixed nutrition and health day (FNHD) program in the rural area of Shamirpet, Ranga Reddy District and the urban area of Dabeerpura, Hyderabad District. Natl J Res Community Med. 2012;1:101–5. [Google Scholar]