

Abstract
Adolescent idiopathic scoliosis (AIS) remains the most common and potentially severe form of scoliosis during the rapid growth period. It is generally accepted that AIS is a multifactorial disease controlled by genetic, hormonal, neuromuscular, and environmental factors. Herein, we describe a case of 12-year-old scoliotic girl with a double curve of initially 26° thoracic and 23° lumbar, seeking chiropractic care. The therapy was provided three times/twice a week for 6 months. Adjustments of the spine through chiropractic, both soreness and mobility, were shown to improve. A total correction in Cobb angle of 6° (23%) in the thoracic curve and 7° (30%) in the lumbar curve was illustrated on consequent radiographs. This case highlights the advantage of chiropractic adjustment of early scoliosis primarily because the medical community does not offer any treatment for such a mild scoliosis. Further, randomized trial is warranted to support this viability for AIS.
Keywords: Adolescent idiopathic scoliosis, chiropractic, Cobb's angle, spinal curvature
Introduction
Adolescent idiopathic scoliosis (AIS) accounts for approximately 80% of cases of idiopathic scoliosis and has implications for the quality of life with limited activity, pain, and negatively impacting respiratory function and self-esteem. Treatment options depend on the severity of the scoliotic curve. In patients who are still growing with a Cobb angle <25°, observation is the mainstay of therapy.[1] A recent study has shown that chiropractic may alleviate the pain and discomfort associated with scoliosis,[2] possibly allow mobilizing regions of the spine that are incapable to achieve by other means.
Case Report
A 12-year-old Asian girl with back soreness and scoliosis for a year sought chiropractic care between July 2015 and January 2016. At the initial visit, her right shoulder was slightly higher with waistline asymmetry. There was no clinical leg-length discrepancy. Adams forward bend test showed positive. Spine radiographs exhibited a double curve pattern, with Cobb angles of 26° thoracic and 23° lumbar, respectively [Figure 1a]. To prevent the risk for curve progression in this youngster and adverse impacts upon her self-esteem, the patient was scheduled to undergo chiropractic treatment.
Figure 1.
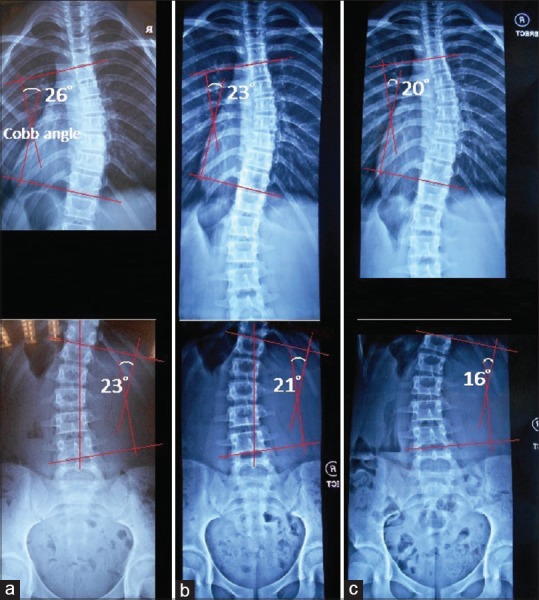
(a) Pretreatment imaging showed a double curve of initially 26° thoracic and 23° lumbar. (b) After 6 months of treatment, Cobb measure was 23° thoracic and 21° lumbar. (c) Correction of 23% (6°) in the thoracic and 30% (7°) in the lumbar curve at 9 months after chiropractic care
Chiropractic care was provided three times a week for the first 2 months, followed by twice a week for the next 4 months. The treatments first consisted of 5 min of general massage applied to the postural muscles using a G5® Machine (General Physiotherapy, Inc., St. Louis, Missouri, U.S.A) to relax muscles allowed for manual manipulation of the area. Flexion distraction was then administered while the patient lied facedown on with both ankles cuffed to the table, and the caudal section of the motorized table slowly raised and lowered to create an intermittent traction to the spine. During the flexion-distraction procedure, spinal manipulation was also employed for 10 min at each treatment. At the completion of 6-month treatment [Figure 1b] and at the 9-month follow-up [Figure 1c], patient's Cobb angles measured by consecutive radiographs were totally corrected by 6° in the thoracic curve (from 26° down to 20°) and 7° in the lumbar curve (from 23° down to 16°). The patient reported alleviated soreness, improved mobility, and more confident, visually appeared better in muscle tones and reduction in her spinal curvature.
Discussion
AIS affects adolescents between the ages of 10 and 15, predominantly in females. The mechanisms driving the initiation and propagation of the scoliotic curves are incompletely understood. Several candidate genes have been linked to AIS, but confirmation of these associations remains inconsistent and requires larger replication studies.[3] Scoliosis has been hypothesized to be the result of minor spinal injuries and uncorrected subluxations.[4] After a critical degree of curvature has developed, a vicious mechanical cycle drives the progression of scoliosis, which accelerates during periods of rapid spinal growth.[5] Although AIS affects both genders, females are eightfold more likely to progress to a stage that requires treatment. Estrogens cause the tendons, ligaments, and muscles to retain flexibility for adolescent growth spurt,[6] and curve progression is most likely during periods of large hormonal changes. Early diagnosis is the key to keeping scoliosis from development or worsening and providing the best treatment.
On physical examination, the patient may exhibit asymmetry of the trunk such as uneven shoulders or hips, humpback, or listing to one side. The anteroposterior radiograph of the entire spine in standing position remains the gold standard for diagnosing and monitoring of scoliosis.[7] The degree of scoliotic curvature is evaluated by the Cobb angle, formed by perpendiculars to the lines drawn from the superior end plate of the upper end vertebra and from the inferior end plate of the lower end vertebra.[7] As a general rule, a Cobb angle of 10° is regarded as a minimum angulation to define scoliosis. The Cobb angle of more than 15° is considered as structural scoliosis.[8] A curvature of 10–15° normally does not require any treatment except for regular checkups till the patient has gone through puberty. When a change is ≥5° between consecutive X-ray examinations, it is considered as an actual progression that requires management.[1]
Current treatment options include observation, bracing, and surgery, depending on the severity of the scoliotic curve. Since some degree of scoliosis is commonly seen in the general population, observation is the mainstay of therapy in patients who are still growing with a Cobb angle <25°.[3] Between 20 and 40°, brace treatment may be warranted to keep the curve from progressing. Surgery may be required to correct the curve of more than 40°. For years it has been debated whether chiropractic can help reduce spinal curvatures. Sometime around 450 B.C., Hippocrates, the Greek physician, described varieties of curving of the spine and treated scoliosis primarily on spinal manipulation and traction.[9] In the retrospective study of 28 patients with adult scoliosis, spinal curvature and level of disability had been shown to improve at the completion of chiropractic treatment without bracing.[2] As illustrated in this case receiving 6-month chiropractic care, our patient achieved a total correction of 6° (23%) in the thoracic curving and 7° (30%) in the lumbar curving [Figure 1]. A change in Cobb angle of ≥5° is considered clinically significant.[8] Chiropractic treatment of scoliosis has classically consisted of spinal manipulation, augmented exercise, postural counseling, and heel lifts. Electrical stimulation has also been employed for a chiropractic armamentarium recently. The mechanisms underlying our observation might be related to increased spine mobility and ligamentous lengthening of the scoliotic curves.[10] However, concrete scientific data supporting the efficacy of manual therapy, i.e., osteopathic, chiropractic, and massage techniques, for AIS are still lacking.[2]
Conclusion
Early chiropractic intervention is recommended in AIS, in view of the fact that scoliosis is at an increased risk of deteriorating in growing children. While limited, chiropractic appears to play a role in the adjustment and monitoring of early stage scoliosis primarily since the medical community does not offer any treatment for a mild scoliosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kim H, Kim HS, Moon ES, Yoon CS, Chung TS, Song HT, et al. Scoliosis imaging: What radiologists should know. Radiographics. 2010;30:1823–42. doi: 10.1148/rg.307105061. [DOI] [PubMed] [Google Scholar]
- 2.Morningstar MW. Outcomes for adult scoliosis patients receiving chiropractic rehabilitation: A 24-month retrospective analysis. J Chiropr Med. 2011;10:179–84. doi: 10.1016/j.jcm.2011.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Samaan MC, Missiuna P, Peterson D, Thabane L. Understanding the role of the immune system in adolescent idiopathic scoliosis: Immunometabolic CONnections to Scoliosis (ICONS) study protocol. BMJ Open. 2016;6:e011812. doi: 10.1136/bmjopen-2016-011812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lantz CA. A review of the evolution of chiropractic concepts of subluxation. Top Clin Chiropr. 1995;2:1–10. [Google Scholar]
- 5.Cassar-Pullicino VN, Eisenstein SM. Imaging in scoliosis: What, why and how? Clin Radiol. 2002;57:543–62. doi: 10.1053/crad.2001.0909. [DOI] [PubMed] [Google Scholar]
- 6.Leboeuf D, Letellier K, Alos N, Edery P, Moldovan F. Do estrogens impact adolescent idiopathic scoliosis? Trends Endocrinol Metab. 2009;20:147–52. doi: 10.1016/j.tem.2008.12.004. [DOI] [PubMed] [Google Scholar]
- 7.Malfair D, Flemming AK, Dvorak MF, Munk PL, Vertinsky AT, Heran MK, et al. Radiographic evaluation of scoliosis: Review. AJR Am J Roentgenol. 2010;194(3 Suppl):S8–22. doi: 10.2214/AJR.07.7145. [DOI] [PubMed] [Google Scholar]
- 8.Morrissy RT, Goldsmith GS, Hall EC, Kehl D, Cowie GH. Measurement of the Cobb angle on radiographs of patients who have scoliosis. Evaluation of intrinsic error. J Bone Joint Surg Am. 1990;72:320–7. [PubMed] [Google Scholar]
- 9.Marketos SG, Skiadas P. Hippocrates. The father of spine surgery. Spine (Phila Pa 1976) 1999;24:1381–7. doi: 10.1097/00007632-199907010-00018. [DOI] [PubMed] [Google Scholar]
- 10.Villafañe JH, Silva GB, Dughera A. Manipulative and rehabilitative therapy as a treatment of idiopathic scoliosis without psychological sequelae: A case report. J Chiropr Med. 2012;11:109–14. doi: 10.1016/j.jcm.2012.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]