

Abstract
Purpose:
The objective of this systematic review was to compare the antero-posterior, vertical and angular changes of maxillary incisors with conventional anchorage control techniques and mini-implant based space closure methods.
Materials and Methods:
The electronic databases Pubmed, Scopus, ISI Web of knowledge, Cochrane Library and Open Grey were searched for potentially eligible studies using a set of predetermined keywords. Full texts meeting the inclusion criteria as well as their references were manually searched. The primary outcome data (linear, angular, and vertical maxillary incisor changes) and secondary outcome data (overbite changes, soft tissue changes, biomechanical factors, root resorption and treatment duration) were extracted from the selected articles and entered into spreadsheets based on the type of anchorage used. The methodological quality of each study was assessed.
Results:
Six studies met the inclusion criteria. The amount of incisor retraction was greater with buccally placed mini-implants than conventional anchorage techniques. The incisor retraction with indirect anchorage from palatal mini-implants was less when compared with buccally placed mini-implants. Incisor intrusion occurred with buccal mini-implants, whereas extrusion was seen with conventional anchorage. Limited data on the biomechanical variables or adverse effects such as root resorption were reported in these studies.
Conclusion:
More RCT’s that take in to account relevant biomechanical variables and employ three-dimensional quantification of tooth movements are required to provide information on incisor changes during space closure.
Keywords: Cone Beam CT, surgical guide, drill, planning, dental implant
Introduction
Extraction of upper and/ or lower first premolars have been traditionally employed for orthodontic camouflage of patients with bidento-alveolar protrusion and Class II Division 1 malocclusions (1, 2, 3, 4, 5, 6). Unwarranted posterior tooth movement which may result during the closure of extraction spaces in such patients are usually controlled with conventional anchorage methods like transpalatal arches (7), headgear (8), bonding second molars (9), and differential moments concept (10). However, these methods are not effective in providing absolute anchorage and 2-3 mm of mesial movement of anchor teeth have been reported (7, 11). Nevertheless, after the introduction of mini-implants it is now possible to achieve absolute anchorage (12). Numerous studies have the evaluated the anchorage loss of maxillary and/or mandibular first molars during space closure. They reported that the direct anchorage from miniimplants provide absolute anchorage when compared to conventional anchorage methods (13). Although, the anchorage control of posterior teeth is superior with mini-implants, the nature of the displacement of the maxillary incisors with both methods of space closure will be of interest for clinicians. The type and direction of the resulting tooth movement depends on the interaction between the line of force and center of resistance (Cr) of any specific tooth or group of teeth (14). Different type of tooth movements may result based on the line of force applied in both methods of space closure. Additionally other biomechanical variables such as the play between the archwire and bracket, defection of the archwire, use of power arms, may have significant effect on the ensuing tooth movement (14, 15). In a recent systematic review Li et al. (16), compared the maxillary incisor changes between mini-implant and conventional methods of space closure. However, no definite conclusions were made due to the heterogeneity among the included studies. Additionally, they failed to account for the biomechanical variables that could affect the type of tooth movement. Contemporary scientific evidence on the amount of maxillary incisor retraction that may result from mini-implant or conventional anchorage techniques could provide important clinical information, which may aid in selecting the appropriate method of anchorage control during orthodontic treatment planning. Therefore, the primary objective of this systematic review is to compare the antero-posterior, vertical and angular changes of maxillary incisors with conventional and mini-implant based space closure methods.
Materials and Methods
A protocol for conducting this systematic review was drafted with the consensus of all authors and registered with PROSPERO, the prospective register of systematic reviews (Registration no. - CRD42015019093, Center for Reviews and Dissemination, University of York (www.crd. york.ac.uk/PROSPERO/index.asp). We followed the PRISMA guidelines (17) for conducting this systematic review. The primary question addressed by this review was defined according to the (PICO format: P-participant, I-intervention, C-comparison, O-outcome).
1. Participants: Patients with Class II Division 1 malocclusion or Class I bimaxillary dento-alveolar protrusion.
2. Intervention: Space closure with mini-implant anchorage.
3. Comparison: Space closure with conventional anchorage
4. Outcome: Antero-posterior, vertical and angular changes of maxillary incisors during space closure.
Search strategy for identification of studies
In May 2015, the electronic databases Pubmed, Scopus, ISI Web of knowledge, Cochrane Library and OpenGrey (18) were searched for relevant articles. The searched strategy mentioned below was initially developed for PubMed but modified to conform to other databases:
1. TAD OR temporary anchorage device OR skeletal anchorage devices OR mini-implant OR miniscrew
2. En-masse retraction OR en masse retraction OR maxillary anterior teeth retraction OR upper anterior teeth retraction OR (“Orthodontic Space Closure”[Mesh]) OR orthodontic space closure
3. “Orthodontic Anchorage Procedures”[Mesh]) OR Orthodontic Anchorage Procedures OR conventional Anchorage Procedures
4. # 1 AND # 2 AND # 3
No restrictions were placed on the language or year of publication. Results obtained from each of the databases were then exported to the Endnote software (Thomson Reuters; Carlsbad, CA, USA) and were first screened to select the potential articles of interest. The following inclusion criteria were used:
1) Subjects with either Angle Class II Division 1 malocclusion with maxillary first premolar extraction, or Class I malocclusion with bimaxillary protrusion.
2) Patients requiring extraction of all first premolars and maximum anchorage control for space closure of maxillary anterior teeth.
3) Randomized clinical trials (RCT). Studies which included patients with hereditary disorders, systemic diseases, craniofacial syndromes, or those on medications that may affect the orthodontic tooth movement, previous orthodontic treatment or orthognathic surgery were excluded.
Assessment of relevance, validity, and data extraction
Two reviewers (NJ and YSNJ) independently assessed the abstracts of studies resulting from the searches. Full texts of all studies identified in the first round were obtained and rescreened against the selection criteria. The reference lists of these articles were searched for any potentially relevant studies. The following primary and secondary outcome data were extracted from the studies that met the inclusion criteria and entered onto Excel spreadsheets based on the type of anchorage used (conventional or skeletal). The primary outcome data included: linear, angular, and vertical changes in maxillary incisor during space closure achieved with conventional and skeletal anchorage methods. The secondary outcome measures included: overbite changes, soft tissue changes (facial convexity, nasolabial angle, upper and lower lip changes), biomechanical factors (dimension of archwire used during space closure, whether power arms were used or not, type of force application), the location of miniscrew implants, root resorption of maxillary incisors and the duration of treatment.
The methodological quality of each study was assessed using the Cochrane Collaborations risk of bias tool (19). The following domains were investigated for the included RCTs: random sequence generation, allocation concealment, blinding of outcome assessor, incomplete outcome data, selective reporting and other any bias. For every RCT assessed, they were stratified as low, unclear and high risk of bias as defined in the Cochrane Handbook for Systematic Reviews of Intervention (20). The data collection and study quality assessment was performed by 2 authors (NJ and YSNJ) separately. Any disagreements between the 2 authors were resolved by consensus.
Results
A total of 280 articles were retrieved after the manual and electronic search of all databases. The QUORUM flow chart (21) (Figure 1) illustrates the process of selecting the studies based on the inclusion and exclusion criteria. After a thorough assessment, which included contacting the corresponding authors to get missing or other information pertaining to this review, only 6 randomized clinical trials (RCTs) were included in this systematic review. (Table 1) (22, 23, 24, 25, 26, 27). Among the 6 RCTs, 2 studies (23, 24) used palatal mini-implants and or onplants with indirect anchorage from transpalatal arch. Direct anchorage from mini-implants placed interdentally between maxillary first molars and second premolars were used in the other clinical trials (Table 1) (22, 25, 26, 27). The transpalatal arch, headgear, differential moments and bonding second molars were used as conventional anchorage techniques. The method of space closure employed with conventional anchorage was 2 step space closure in two studies (22, 27), enmasse retraction in 2 trials (25, 26) and not reported in the other 2 studies (Table 2) (23, 24). The dental, skeletal, and soft tissues changes obtained from these 6 RCTs are presented in Tables 3-5. Due to the heterogeneity in the selected RCTs, either due to variation in the type of archwire used for space closure, or location of mini- implants, or line of force for retraction, or time of evaluation; it was impossible to perform a meta-analysis. Instead, a narrative synthesis was performed to extract clinically relevant information.
Figure 1.
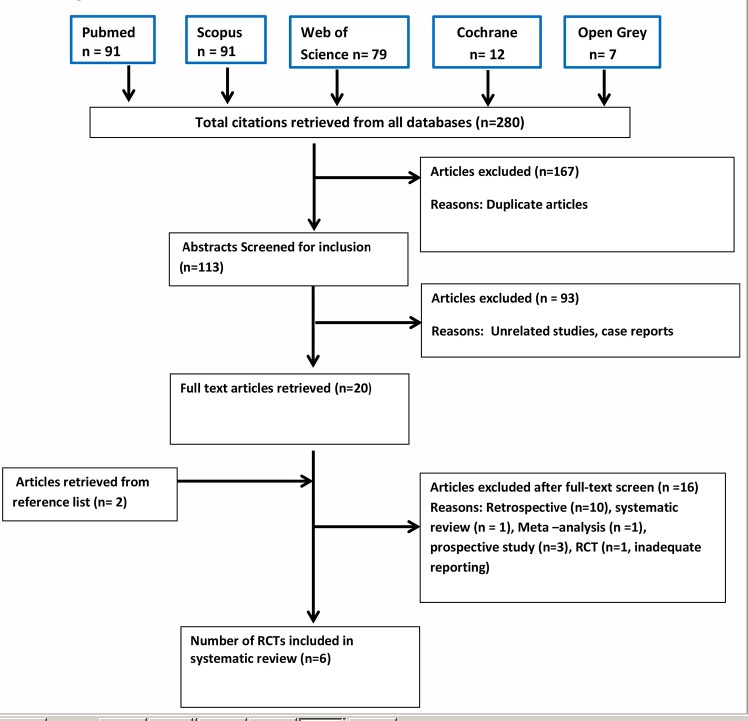
Flow chart based on PRISMA statement for article selection.
Table 1.
Characteristics of the studies included in this systematic review.
| Author | Type of malocclusion | Number of participants | Age (years) | Type of Anchorage used in the control group | Mini-implant location | ||
|---|---|---|---|---|---|---|---|
| Males | Females | Total | |||||
| Al-Sibaie et al.(22) | Class II Division 1, overjet greater than 5mm | 21 | 35 | 56 | 22.34 ± 4.56 | TPA | Interdental between U6 and U5 buccally |
| Benson et al.(23) | Class II malocclusion with absolute anchorage. | NR | NR | 51 | 12-39 (Range) | HG | Mid-palatal mini-implant |
| Feldmann et al.(24) | Cases requiring 2 or 4 bicuspid extractions | 60 | 60 | 120 | 14.3 ± 1.73 | HG and TPA | Palatal mini-implant and onplant |
| Liu et al.(25) | Class I bimaxillary protrusion/ Class II Division 1 | 6 | 28 | 34 | 18-33 (range) | TPA | Interdental between U6 and U5 buccally |
| Ma et al.(26) | Class I bimaxillary protrusion | 14 | 16 | 30 | 18-22 (Range) | HG and 2nd molars included | Interdental between U6 and U5 buccally |
| Upadhyay et al.(27) | Class I bimaxillary protrusion | 0 | 36 | 36 | 17.5 ± 3.2 | TPA, HG, Bonding 7s, Differential moments | Interdental between U6 and U5 buccally |
Table 2.
Biomechanical factors.
| Author | Brackets size with prescription | Archwire | Power arms or other auxiliaries | Method of force application | Method of space closure in the conventional group | Line of force | |||
|---|---|---|---|---|---|---|---|---|---|
| Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | ||||
| Al-Sibaie et al.(22) | 0.022" slot (MBT prescription) | 0.019 x 0.025" Stainless Steel | 8 mm power arm | None | Elastic chain (150 g) | Elastic chain | 2 step | Parallel to occlusal plane | Horizontal |
| Benson et al.(23) | 0.022" slot (MBT prescription) | 0.019 x 0.025" Stainless Steel | Posted archwires | NR | NiTi coil springs (12mm) | NiTi coil springs (12mm) | NR | NR | NR |
| Feldmann et al.(24) | 0.022" slot (MBT prescription) | 0.019 x 0.025" Stainless Steel | NR | NR | Active tie backs | Active tie backs | NR | NR | NR |
| Liu et al.(25) | NR | 0.019 x 0.025" Stainless Steel | Hooks | Hooks | Elastic chain | Elastic chain | Enmasse | Upward and backward | Parallel to occlusal plane |
| Ma et al.(26) | 0.022" slot (MBT prescription) | 0.019 x 0.025" Stainless Steel | Hooks | Hooks | NiTi coil springs (100gms) | NiTi coil springs (100gms) | Enmasse | NR | Horizontal |
| Upadhyay et al.(27) | 0.022" slot (Roth prescription) | 0.017 x 0.025" Stainless Steel | Crimpable hooks | NR | NiTi coil springs (150-g) | NR | 2 step | Upward and backward | NR |
Study quality assessment
Table 6 shows the results of quality assessment of included studies. Figure 2 shows the overall risk of bias for the articles included in this systematic review. Among the 6 RCTs, 2 studies were stratified as high quality with low risk of bias (22, 23, 26 ), 2 were of medium quality with moderate risk of bias (24, 25, 27), and 2 RCTs were of poor quality with high risk of bias. In all the RCTs, the method of randomization and incomplete outcome data (attrition bias) was adequate. The allocation concealment was adequate in only 2 studies (22, 23) and Due to the type of intervention, which precluded blinding of both the operator and patients in all the included articles. However blinding of outcome assessment was possible and reported to be performed in 3 studies. (22, 23, 26) All the clinical trials reportedly had similar baseline characteristics. Reliability assessment and statistical analysis were appropriate in all studies. Sample size was estimated in 4 trials prior to collection of data (222, 23, 24, 27).Other than Ma et al. (26), the inclusion and exclusion criteria were described in the other 5 clinical trials. Lateral cephalogram were used to compare the pre and post retraction changes and the measurement methods were similar in all the clinical trials.
Table 6.
Results of the quality assessment of included articles (a: low risk of bias, b: uncertain risk of bias, b: high risk of bias).
| Quality assessment criteria | Al-Sibaie et al.(22) | Benson et al.(23) | Feldmann et al.(24) | Liu et al.(25) | Ma et al.(26) | Upadhyay et al.(27) |
|---|---|---|---|---|---|---|
| Random sequence generation (selection bias) | +a | +a | +a | +a | +a | +a |
| Allocation concealment (Selection bias) | +a | +a | ?b | ?b | ?b | ?b |
| Blinding of outcome assessment (detection bias) | +a | +a | -c | ?b | +a | ?b |
| Incomplete outcome data (attrition bias) | +a | +a | +a | +a | +a | +a |
| Selective reporting (reporting bias) | +a | +a | ?b | ?b | -c | ?b |
| Other bias | +a | +a | -c | +a | +a | +a |
Figure 2.
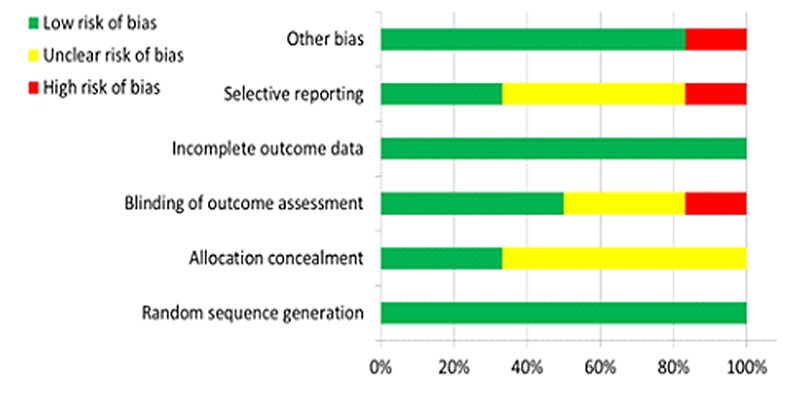
Overall risk of bias score based on Cochrane Collaborations risk of bias tool.
Primary outcomes
Maxillary incisor retraction: Amount of maxillary incisor retraction measured at the incisal edge ranged from 0.7 - 6.33 mm with conventional anchorage methods and 2.1 - 7.22 mm with skeletal anchorage (Table 3). Angular change of maxillary incisors: The angular change of maxillary incisors during space closure ranged from 7.12 – 16.83 degrees with conventional anchorage methods and 4.6 – 13.53 degrees with skeletal anchorage (Table 3). Vertical changes of maxillary incisors: Only 3 clinical trials (22, 25, 26) reported the vertical change of maxillary incisors. Maxillary incisor extrusion ranged from 0.92 -2.03mm with conventional anchorage, and 1.53 - 2.15mm with skeletal anchorage (Table 3). Two of these studies (25, 26) measured the vertical position of the incisors before and after completion of treatment, whereas the third study measured after the space closure (27).
Table 3.
Comparison of dental changes of maxillary central incisors and maxillary first molars.
| Author | Maxillary incisor retraction (mm) | Angular change of incisor inclination (degrees) | Vertical change of maxillary incisors (mm) | Anchorage loss of maxillary 1st molars (mm) | Vertical change of maxillary molar (mm) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mini-implant | Conventional anchorage group | Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | |
| group | ||||||||||
| Al-Sibaie et al.(22) | -5.92 | -4.79 | -5.03 | -7.94 | -1.53 | 0.92 | -0.75 | 27760 | 0.02 | 0.38 |
| Benson et al.(23) | -2.1 | -0.7 | NR | NR | NR | NR | 42856 | 3 | NR | NR |
| Feldmann et al.(24) | -3.9 (onplant) -4.7 (TAD) | -4.8 (HG) -3.3 (TPA) | -4.6 (onplant) / -5.3 (TAD) | -6.71 (HG)/ 5.7 (TPA) | NR | NR | 0.1 (onplant) /0 (TAD) | 1.2 (HG) | NR | NR |
| Liu et al.(25) | -7.03 | -4.76 | -13.53 | -12.03 | -1.91 | 42736 | -1.42 | 33239 | -0.06 | 14611 |
| Ma et al.(26) | -6.65 | -5.59 | -6.66 | -7.12 | -2.15 | 42796 | NR | NR | NR | NR |
| Upadhyay et al.(27) | -7.22 | -6.33 | -13.11 | -16.83 | NR | NR | -0.78 | 44621 | -0.22 | 0.67 |
Secondary outcomes
Anchorage loss of maxillary 1stmolars: The anchorage loss with conventional techniques ranged from 1 – 3.22mm. In contrast, a 0.75 – 1.42mm anchorage gain (i.e. distalization of maxillary 1st molar) was noted when the mini-implant was placed buccally between the maxillary 1st and 2nd premolar. However anchorage loss of 0.74 – 1.5mm was observed when the mini-implant was placed in the palatal region (Table 3). Vertical change in maxillary 1st molar: The reported maxillary 1st molar extrusion ranged from 0.38 – 1.4mm with conventional anchorage methods and intrusion ranged from -0.22 to - 0.06mm with skeletal anchorage (Table 3). A 0.02mm extrusion of the 1st molar was reported by Al-Sibae et al. (22) when using mini-implants. Soft tissue changes: The increase of the nasolabial angle during space closure was higher with skeletal anchorage (6.94 – 11.67°) compared to conventional anchorage (5 – 5.93°) (Table 4). The change in the distance from the upper lip to E line was basically similar, ranging from 2.47 – 3.38mm and 2.89 – 4.71mm in the conventional and skeletal anchorage groups respectively. The lower lips were retracted 1.47 – 3.11mm with reference to E line in the conventional group while this ranged from 2.5 – 4.78mm in the skeletal anchorage group. Finally, the angle of facial convexity showed a slight decrease of 1.17 – 1.26 degrees and 1.82 – 2.33 degrees in the conventional and skeletal anchorage groups respectively.
Table 4.
Comparison of soft tissue changes between mini-implant and conventional anchorage group.
| Study | Naso-labial angle (°) | Angle of convexity (°) | Ls to E line (mm) | Li to E line (mm) | ||||
|---|---|---|---|---|---|---|---|---|
| Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | |
| Al-Sibaie et al.(22) | -9.08 | -5.93 | NR | NR | -2.98 | -2.47 | -2.50 | -1.42 |
| Benson et al.(23) | NR | NR | NR | NR | NR | NR | NR | NR |
| Feldmann et al.(24) | NR | NR | NR | NR | NR | NR | NR | NR |
| Liu et al.(25) | -6.94 | -5.94 | -1.82 | -1.26 | -4.71 | -3.38 | NR | NR |
| Ma et al.(26) | NR | NR | NR | NR | NR | NR | NR | NR |
| Upadhyay et al.(27) | -11.67 | -5 | -2.33 | -1.17 | -2.89 | -2.56 | -4.78 | -3.11 |
Skeletal changes: The mandibular plane angle and lower anterior facial height was either maintained or slightly reduced after space closure with skeletal anchorage, whereas slight increase in this angle was seen with conventional anchorage (Table 5). The change in ANB angle was highly variable between the 2 groups, but a minor reduction was seen in both groups.
Table 5.
Comparison of skeletal changes between mini-implant and conventional anchorage group.
| Author | ANB (degrees) | MPA (degrees) | ANS-Me (mm) | |||
|---|---|---|---|---|---|---|
| Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | Mini-implant group | Conventional anchorage group | |
| Al-Sibaie et al.(22) | -0.62 | -0.75 | -0.41 | -1.38 | NR | NR |
| Benson et al.(23) | NR | NR | NR | NR | NR | NR |
| Feldmann et al.(24) | -0.3 (onplant)/-0.3 (mini-implant) | -0.4 (HG) /-0.5 (TPA) | -0.3 (onplant)/0 (mini-implant) | 0.1 (HG)/0.4 (TPA) | NR | NR |
| Liu et al.(25) | -1.07 | -0.09 | -1.12 | 0.78 | 0.18 | 0.48 |
| Ma et al.(26) | 0.03 | 0.38 | 0.13 | 42795 | NR | NR |
| Upadhyay et al.(27) | -0.67 | 0 | -1.11 | 0.28 | -1.44 | 0.56 |
Root resorption: None of the clinical trials reported root resorption in the maxillary incisors. Retraction time: Only two RCTs22, 26 reported the retraction time which ranged from 9.94 – 16.97 months with conventional anchorage (Table 7) and slightly shorter (8.61 - 12.9 months) with skeletal anchorage.
Table 7.
Evaluation of space closure.
| Author | Evaluation method | Time points used for the evaluation | Mean (SD) retraction time (months) | |
|---|---|---|---|---|
| Mini-implant group | Control group | |||
| Al-Sibaie et al.(22) | Lateral ceph | 1)Pretreatment | 12.9 | 16.97 |
| 2)After alignment | ||||
| 3)After achieving Class I canine relation | ||||
| Benson et al.(23) | Lateral ceph | 1)Pretreatment | NR | NR |
| 2)After achieving Class I canine relation | ||||
| Feldmann et al.(24) | Lateral ceph | 1)Pretreatment | NR | NR |
| 2)After alignment and space closure or achieving Class I canine relation | ||||
| Liu et al.(25) | Lateral ceph | 1)Pretreatment | NR | NR |
| 2)Post treatment | ||||
| Ma et al.(26) | Lateral ceph | 1)Pretreatment | NR | NR |
| 2)Post treatment | ||||
| Upadhyay et al.(27) | Lateral ceph | 1)Pretreatment | 8.61 (2.2) | 9.94 (2.44) |
| 2)After space closure | ||||
Biomechanical variables: Most of the clinical trials (22, 23, 24, 25, 26) used 0.019 x 0.025-inch stainless steel archwire during space closure. However, Upadhyay et al. (27) study used 0.017 x 0.025-in stainless steel archwire during space closure. Hooks were crimped or soldered on the archwires distal to the lateral incisors and an elastic chain or Nickel Titanium springs were used in the mini-implant group. But, Al-Sibaie et al. (22) used power arms with a length of 8mm. In the conventional group only 2 studies (25, 26) reported using hooks on the archwire during retraction. The line of retraction force in the mini-implant group had an intrusive and retractive component as reported in 2 studies and parallel to occlusal plane in Al-Sibaie study (22), whereas in the conventional group it was horizontal or parallel to occlusal plane as reported in 3 clinical trials (22, 25, 26) (Table 2). Finally, in Upadhyay et al. (27) study they used 0.022-in brackets with Roth prescription and 4 studies reported using 0.022-in MBT brackets (Table 2) (22, 23, 24, 26).
Discussion
Most of the available literature primarily focused on the loss of anchorage in relation to the maxillary 1st molar during space closure using conventional and mini-implant anchorage (12). Thus, the primary aim of this systematic review was to determine the maxillary incisor changes both in anteroposterior and vertical dimension. In addition, we wanted to evaluate the effects of the direction of the retraction force, archwire dimension and power arms on maxillary incisors during space closure. These variables can alter the resulting tooth movement and such information could influence the selection of the most appropriate method of anchorage.
Main findings
The amount of maxillary incisor retraction reported in 5 of the 6 RCTs included in the systematic review was greater with skeletal anchorage than conventional methods. Furthermore, the amount of incisor retraction with palatal mini-implants23, 24 was less when compared to buccally placed interdental mini-implants. This may result from the fact that palatal mini-implants provide indirect anchorage and this was not effective in preventing mesial movement of maxillary molars, which limited the amount of incisor retraction. In addition, one of these palatal mini-implant studies (24) included patients with crowding and those requiring moderate to maximum anchorage which may have also limited the magnitude of incisor retraction. The degree of change in the incisor angulation was greater with conventional anchorage compared to skeletal anchorage. This may result from the differences in the line of retraction force between these 2 techniques. The line of force in the conventional group was horizontal or parallel to the occlusal plane, whereas it was upward and backward when miniimplants are placed buccally. In contrast, Al-Sibae et al. (22) used 8 mm power arms to make the line of force parallel to the occlusal plane. It should be noted that the change in the incisor angulation was highest in Upadhyay et al. study (27) who used 0.017 x 0.025” stainless steel archwire for retraction, whereas other studies used 0.019 x 0.025”archwires. In Feldmann et al. study (24) (that employed palatal mini-implants or onplants), the amount of angulation change was significantly higher in the conventional group in spite of having similar line of action of force. The vertical change of incisors was only reported in 3 studies (22, 25, 26), they reported the differences between the mini-implant and conventional anchorage groups. Intrusion of maxillary incisors was observed in the mini-implant group whereas extrusion was reported with conventional retraction methods. However, in 2 studies the measurements were recorded after completion of treatment and hence the incisor movement could be altered during finishing (25, 26). The only biomechanical explanation may be attributed to the difference in line of retraction force between mini-implant and conventional group. Al- Sibaie et al. (22) used 8mm power arm and the line of force was parallel to occlusal plane in the miniimplant group. Despite using an 8mm power arm by Al-Sibaie et al. (22), significant intrusion of maxillary incisors was seen, which could be attributed to the bending moment of the power arm (15).
Direct anchorage from mini-implants provided absolute anchorage but slight distal movement of maxillary 1st molars (i.e. anchorage gain) was also reported (22, 25, 26, 27). Indirect anchorage from palatal mini-implants was not effective in providing absolute anchorage during space closure (23, 24). Also, with conventional anchorage methods, significant mesial movement of maxillary molars was reported. Additionally, when 0.017 x 0.025” archwire was used, greater anchorage loss was observed (27) when compared to clinical trials that used 0.019 x 0.025-in archwire (22, 25, 26). In the vertical dimension, the position of the maxillary 1st molars was maintained in the mini-implant group and slight extrusion was seen in conventional anchorage group (22, 25, 27). Most of the clinical trials reported slight decrease in the mandibular plane angle in the mini-implant group when compared to the conventional anchorage group (22, 25, 26, 27). Similarly, a slight decrease in the lower anterior facial height was reported in the mini-implant group in some studies (25, 27). Since the vertical control of molars was superior in the mini-implant group, it may be safe to recommend mini-implants for space closure in maximum anchorage subjects with hyperdivergent growth pattern.
The impact of facial soft tissue changes between the mini-implant and conventional anchorage was assessed among the 6 RCTS. Three trials (22, 25, 27) reported the changes in nasolabial angle and antero-posterior position of lips and 2 RCTs (25, 27) reported the changes in the angle of facial convexity. The amount of nasolabial angle change was not significant in one clinical trial (26) between the two groups. However greater change in the nasolabial angle was observed in the mini-implant group in the other 2 studies (22, 27). These changes were pronounced when 0.017 x 0.025” archwire was used for space closure ( 27).The reduction in the angle of facial convexity was too small between the two groups and may not be clinically significant ( 25, 27). The upper lip was retracted in both groups but these differences were not significant (22, 25, 27). However, two clinical trials (22, 27) reported that the lower lip retracted more with reference to E line in the mini-implant group.
Confounding factors
Several other confounding factors may have influenced the differences in the incisor retraction reported by the included studies. In 4 clinical trials (22, 23, 24, 27), incisor retraction was estimated immediately after space closure; while this was measured at the completion of orthodontic treatment in the remaining 2 studies (25, 26). Likewise, the use of reverse curve of Spee archwire and intermaxillary elastics by Benson et al. (23) during space closure in few subjects may have further confounded their results. Li et al. (16) performed a meta-analysis of Bensons (23) and Feldmann study (24) for incisor retraction, ignoring this factor. Incorporation of reverse curve of Spee in the archwire may affect the type of tooth movement in comparison with subjects and other clinical trials without the curve of Spee. The quality and quantity of incisor movement differed when two archwire of different dimension were used. The amount of retraction and angular change of incisors were greater in the study (27) that used 0.017 x 0.025”archwire during space closure in comparison to the other 5 RCTs (22, 23, 24, 25, 26) that employed 0.019 x 0.025”stainless steel archwire. The linear displacement of maxillary incisors was slightly less when a 0.019 x 0.025” archwire was used in all the studies except in Liu et al. article (25). However, in the Liu et al. (25) study, the amount of incisor movement was measured after orthodontic treatment and the incisor position could have been altered during the finishing stage. In the Al-Sibaie et al. (22) study, a 8 mm power arm was used during space closure in the mini-implant group, and as a result the type of incisor movement was different from the other clinical trials. Although the linear displacement was comparable with other articles, the angular displacement was much less, approximating translation.
The archwire bracket play is an important variable that can significantly affect the quality and quantity of tooth movement (15). Since the bracket play is greater when an archwire with smaller dimension is used, one can expect greater angular changes and more retraction. Another important observation was the greater angular change of incisors in the conventional anchorage group, which could be attributed to the difference in line of force between the 2 groups. The line of force had an intrusive and retractive component in mini-implant group, whereas in the conventional group it was parallel to the occlusal plane. The maxillary incisor position was better controlled in the mini-implant group due to the intrusive component of the retractive force. As expected, greater tipping of the incisors was seen in conventional anchorage group, especially with a 0.017 x 0.025-in archwire (22) which may require additional root torqueing during finishing.
Implications for clinical practice
Extrapolating the findings of this systematic review into the clinical setting is somewhat difficult due to the lack of homogeneity in the published RCTs. However, based on the findings from the included RCTs, the following observations can be made; The amount of incisor retraction (overjet reduction) was greater with a 0.017 x 0.025” archwire when compared with a 0.019 x 0.025” archwire. Intrusion and retraction of maxillary incisors was possible with TADS placed buccally between the maxillary 1st molar and premolar. The tipping of maxillary incisors can be controlled by using a 0.019 x 0.025” archwire for space closure or by incorporating a power arm whose length approximates the center of resistance of the anterior segment and/ or having a line of retractive force with an intrusive and retractive component. The use of buccally placed mini-implant for space closure can be recommended in patients with deep bites requiring maximum anchorage as intrusion and retraction of the maxillary incisors is observed. On the contrary, overbite increase was documented with traditional methods of space closure.
Suggestions for future research
Although six RCTs were included in this review, the amount of anteroposterior, angular and vertical changes of maxillary incisors was different due to heterogeneity either in study methodology or type of intervention. We couldn’t find answers to some of the questions regarding when to use a particular archwire dimension or power arm, the length of power arm, the line of retraction force during space closure. This information is important to the clinician for selecting either appropriate anchorage method during space closure or select correct biomechanical variables that can predictably achieve treatment objectives. However, further research is necessary to evaluate the quality of maxillary incisor movement considering the biomechanical variables which can give valuable information.
The loss of anchorage in all RCT’s included for this systematic review has been performed using lateral cephalograms. However, lateral cephalograms have several inherent limitations as it is a 2-D representation of a 3-D object. Superimposition of contralateral molars on a cephalogram may induce measurement errors when assessing anchorage loss. Utilization of novel 3-D imaging techniques such as intra-oral scanners or digital model scanners could be a possible solution to minimize such errors. It has been shown that such 3-D scans taken at 2 time points can be superimposed with reasonable accuracy using the palatal rugae (28). The amount of tooth movement of all teeth on all 3 planes can be evaluated after such superimpositions.
Conclusion
The amount of incisor retraction was greater with buccally placed mini-implants when compared to conventional anchorage techniques. However, the incisor retraction was less with indirect anchorage from palatal mini-implants when compared with buccally placed mini-implants. Vertically, maxillary incisor intrusion was seen in the buccal miniimplant group, whereas extrusion was seen with conventional anchorage. More RCT’s that take in to account relevant biomechanical variables and employ three-dimensional quantification of tooth movements are required to provide accurate information on incisor movements during space closure.
Footnotes
Source of funding: None declared.
Conflict of interest: None declared.
References
- 1.Bills DA, Handelman CS, BeGole EA. Bimaxillary dentoalveolar protrusion: traits and orthodontic correction. Angle Orthod. 2005. May;75(3):333–9. [DOI] [PubMed] [Google Scholar]
- 2.Bishara SE, Cummins DM, Jakobsen JR, Zaher AR. Dentofacial and soft tissue changes in Class II, division 1 cases treated with and without extractions. Am J Orthod Dentofacial Orthop. 1995. January;107(1):28–37. 10.1016/S0889-5406(95)70154-0 [DOI] [PubMed] [Google Scholar]
- 3.Guo Y, Han X, Xu H, Ai D, Zeng H, Bai D. Morphological characteristics influencing the orthodontic extraction strategies for Angle’s class II division 1 malocclusions. Prog Orthod. 2014. July;15(1):44. 10.1186/s40510-014-0044-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Janson G, Brambilla AC, Henriques JF, de Freitas MR, Neves LS. Class II treatment success rate in 2- and 4-premolar extraction protocols. Am J Orthod Dentofacial Orthop. 2004. April;125(4):472–9. 10.1016/j.ajodo.2003.04.013 [DOI] [PubMed] [Google Scholar]
- 5.Markic G, Katsaros C, Pandis N, Eliades T. Temporary anchorage device usage: a survey among Swiss orthodontists. Prog Orthod. 2014. April;15(1):29. 10.1186/s40510-014-0029-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tan TJ. Profile changes following orthodontic correction of bimaxillary protrusion with a preadjusted edgewise appliance. Int J Adult Orthodon Orthognath Surg. 1996;11(3):239–51. [PubMed] [Google Scholar]
- 7.Zablocki HL, McNamara JA Jr, Franchi L, Baccetti T. Effect of the transpalatal arch during extraction treatment. Am J Orthod Dentofacial Orthop. 2008. June;133(6):852–60. 10.1016/j.ajodo.2006.07.031 [DOI] [PubMed] [Google Scholar]
- 8.Thiruvenkatachari B, Ammayappan P, Kandaswamy R. Comparison of rate of canine retraction with conventional molar anchorage and titanium implant anchorage. Am J Orthod Dentofacial Orthop. 2008. July;134(1):30–5. 10.1016/j.ajodo.2006.05.044 [DOI] [PubMed] [Google Scholar]
- 9.Geron S, Shpack N, Kandos S, Davidovitch M, Vardimon AD. Anchorage loss—a multifactorial response. Angle Orthod. 2003. December;73(6):730–7. [DOI] [PubMed] [Google Scholar]
- 10.Davoody AR, Posada L, Utreja A, Janakiraman N, Neace WP, Uribe F et al. A prospective comparative study between differential moments and miniscrews in anchorage control. Eur J Orthod. 2013. October;35(5):568–76. 10.1093/ejo/cjs046 [DOI] [PubMed] [Google Scholar]
- 11.Feldmann I, Bondemark L. Orthodontic anchorage: a systematic review. Angle Orthod. 2006. May;76(3):493–501. [DOI] [PubMed] [Google Scholar]
- 12.Jambi S, Walsh T, Sandler J, et al. Reinforcement of anchorage during orthodontic brace treatment with implants or other surgical methods. status and date: New search for studies and content updated (conclusions changed), published in 2014(8). [DOI] [PMC free article] [PubMed]
- 13.Yao CC, Lai EH, Chang JZ, Chen I, Chen YJ. Comparison of treatment outcomes between skeletal anchorage and extraoral anchorage in adults with maxillary dentoalveolar protrusion. Am J Orthod Dentofacial Orthop. 2008. November;134(5):615–24. 10.1016/j.ajodo.2006.12.022 [DOI] [PubMed] [Google Scholar]
- 14.Tominaga JY, Chiang PC, Ozaki H, Tanaka M, Koga Y, Bourauel C et al. Effect of play between bracket and archwire on anterior tooth movement in sliding mechanics: A three-dimensional finite element study. J Dent Biomech. 2012;3(0):1758736012461269. 10.1177/1758736012461269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tominaga JY, Tanaka M, Koga Y, Gonzales C, Kobayashi M, Yoshida N. Optimal loading conditions for controlled movement of anterior teeth in sliding mechanics. Angle Orthod. 2009. November;79(6):1102–7. 10.2319/111608-587R.1 [DOI] [PubMed] [Google Scholar]
- 16.Li F, Hu HK, Chen JW, Liu ZP, Li GF, He SS et al. Comparison of anchorage capacity between implant and headgear during anterior segment retraction. Angle Orthod. 2011. September;81(5):915–22. 10.2319/101410-603.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Prisma Statement [Internet]. Houston: PRISMA; 2017. [cited 2017 Dec 2]. Available from: http://www.prisma-statement.org/. [Google Scholar]
- 18. Opengrey [Internet]. Version 1.0 France: INIST-CNRS; 2000 - . [cited 2017 Dec 2]. Available from: http://www.opengrey.eu/. [Google Scholar]
- 19.Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD et al. ; Cochrane Bias Methods Group; Cochrane Statistical Methods Group . The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011. October;343 oct18 2:d5928. 10.1136/bmj.d5928 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0 [Internet]. [London]: The Cochrane Collaboration; 2017. December [revised 2011 Mar; cited 2017 Dec 2]. [about 200 p.] Available from: http://training.cochrane.org/handbook. [Google Scholar]
- 21.Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet. 1999. November;354(9193):1896–900. 10.1016/S0140-6736(99)04149-5 [DOI] [PubMed] [Google Scholar]
- 22.Al-Sibaie S, Hajeer MY. Assessment of changes following en-masse retraction with mini-implants anchorage compared to two-step retraction with conventional anchorage in patients with class II division 1 malocclusion: a randomized controlled trial. Eur J Orthod. 2014. June;36(3):275–83. 10.1093/ejo/cjt046 [DOI] [PubMed] [Google Scholar]
- 23.Benson PE, Tinsley D, O’Dwyer JJ, Majumdar A, Doyle P, Sandler PJ. Midpalatal implants vs headgear for orthodontic anchorage—a randomized clinical trial: cephalometric results. Am J Orthod Dentofacial Orthop. 2007. November;132(5):606–15. 10.1016/j.ajodo.2006.01.040 [DOI] [PubMed] [Google Scholar]
- 24.Feldmann I, Bondemark L. Anchorage capacity of osseointegrated and conventional anchorage systems: A randomized controlled trial. Am J Orthod Dentofacial Orthop 2008;133(3):339 e319-328. 10.1016/j.ajodo.2007.08.014 [DOI] [PubMed]
- 25.Liu YH, Ding WH, Liu J, Li Q. Comparison of the differences in cephalometric parameters after active orthodontic treatment applying mini-screw implants or transpalatal arches in adult patients with bialveolar dental protrusion. J Oral Rehabil. 2009. September;36(9):687–95. 10.1111/j.1365-2842.2009.01976.x [DOI] [PubMed] [Google Scholar]
- 26.Ma J, Wang L, Zhang W, Chen W, Zhao C, Smales RJ. Comparative evaluation of micro-implant and headgear anchorage used with a pre-adjusted appliance system. Eur J Orthod. 2008. June;30(3):283–7. 10.1093/ejo/cjm128 [DOI] [PubMed] [Google Scholar]
- 27.Upadhyay M, Yadav S, Nagaraj K, Patil S. Treatment effects of mini-implants for en-masse retraction of anterior teeth in bialveolar dental protrusion patients: A randomized controlled trial. Am J Orthod Dentofacial Orthop 2008;134(1):18-29 e11. 10.1016/j.ajodo.2007.03.025 [DOI] [PubMed]
- 28.Thiruvenkatachari B, Al-Abdallah M, Akram NC, Sandler J, O’Brien K. Measuring 3-dimensional tooth movement with a 3-dimensional surface laser scanner. Am J Orthod Dentofacial Orthop. 2009. April;135(4):480–5. 10.1016/j.ajodo.2007.03.040 [DOI] [PubMed] [Google Scholar]