

Abstract
Background
Spinal pain affects approximately 45–56% of pregnant women. Kinesio taping (KT) involves application of flexible water-resistant elastic bands on the patient’s body, resulting in painless and non-invasive stimulation. The aim of the study was to determine the influence of KT on reduction of low back pain in pregnant women.
Material/Methods
Kinesio Tex Gold tapes were applied using the muscular-ligament technique and Polovis Plus textile cladding blinded the sample. The starting position for the KT and placebo with lumbar spine flexion with rotation was in the opposite direction to the application. An “I”-shaped application was used. The material included 106 women in the second and third trimesters of pregnancy, with low back pain. The Visual Analogue Scale (VAS) and the Polish version of the Roland Morris Disability Questionnaire (RMDQ-2004) were used for pain assessment. Participants were randomly divided into 2 groups. KT and placebo were used alternately in 2 groups.
Results
Mean pain intensity on the 2nd and 7th post-application days was significantly lower in the study group than in the control group. Mean scores for the RMDQ differed significantly before and after KT (p<0.0001), and after KT and placebo (p<0.0057), but there are no differences before and after placebo (p<0.67) and before KT and placebo (p<0.59).
Conclusions
Low back pain in pregnant women decreased significantly after KT when compared to placebo. The therapeutic effect appeared on day 2 and continued after removal of the tape. The few side effects did not affect the course of the study.
MeSH Keywords: Kinesiology, Applied; Low Back Pain; Pregnancy
Background
Lumbar-sacral spinal pain is a medical and socioeconomic problem affecting almost 80% of the population [1,2]. Pregnancy and puerperium predispose a woman to this pain [3]. Spinal pain in pregnant women is a common problem. Epidemiological studies show that this problem affects approximately 45–56% of pregnant women [4,5]. Usually, pain occurs between 12th and 18th week of gestation, and its incidence increases between the 24th and 30th weeks of gestation. These complaints are aggravated in multiple pregnancies as well as by each new pregnancy [6,7]. Pains are caused by changes in body posture, resulting in the displacement of the center of gravity towards the front, which intensifies lordosis of the lumbar spine, and in the muscular system weakens the abdominal muscles and buttocks and leads to flexion contracture in the hip joints. Other causes of such ailments include previous trauma and pathologies of the spine or diseases of the pelvic organs [8]. Spine pain significantly limits a wide range of activities of pregnant women. Some women during this period do not give up their professional work, and those who are proactive are more likely to cope with emotional problems as well as improve their physical performance. It is also important to start or continue physical activity during pregnancy, which significantly affects the pregnancy course, as well as the birth and the postnatal period. Mobility and exercise in pregnancy are beneficial for improving cardiovascular, musculoskeletal, and digestive capacity [9]. In terms of childbirth, physical activity is associated with faster progression and less pain and stress, and it reduces the risk of serious cranial injuries [9,10]. It is therefore very important to find and explore methods that will reduce the symptoms in pregnant women and help them return to their normal activities. Our search of the literature revealed that scientists are interested in the anatomical, physiological, and biochemical changes that occur during pregnancy, as well as the etiology of spinal pain. One way to tackle the aforementioned problems is to use a therapeutic approach that will reduce the chronic tension and pain of the lumbosacral spine - Kinesio taping [11]. Kinesio taping – also known as dynamic plastering - is a method that involves the application of a flexible water-resistant elastic band on the patient’s body, with weight and thickness similar to human skin [11]. It is the source of stimuli received by the receptors located on the skin. Kinesio taping reduces pain by activating endogenous anesthesia. It is painless and non-invasive stimulation that allows for increased muscle activity and does not impede the full range of motion [12]. Therefore, the aim of the present study was to determine the effect of Kinesio taping method on the reduction of lumbar spine pain in pregnant women.
Material and Methods
The research was carried out between November 2013 and April 2016 in Lubelskie and Mazowieckie voivodships. The consent of the Bioethics Committee of the Medical University of Lublin (Opinion No. KE-0254/178/2012) was obtained prior to the study. The experimental study was randomized and single-blinded, and used a cross-over study design (Figure 1). Kinesio Tex Gold tapes (5×0.05 m Manufacturer: Kinesio Poland) were applied in the study. Polovis Plus textile cladding (5×0.05 m, Manufacturer: 3M Viscoplast S.A. Poland) was used to blind the sample. Women in the second and third trimesters of pregnancy with low back pain, who were patients of gynecological offices, and did not have any contraindications were invited to participate in the study. The inclusion criteria were: written informed consent, being pregnant in the 2nd or 3rd trimester, low back pain, no analgesic medication taken, lack of contraindications (skin lesions in sacrolumbar area), and lack of vertebral anomaly or disease. The exclusion criteria were: lack of written consent, occurrence of contraindications (listed above), vertebral anomaly, or disease prior to pregnancy. Finally, willingness to participate in the project was expressed by 106 women and the sample size was considered adequate for management by 1 co-author. Prior to the commencement of the study, written informed consent was obtained for participation in the study. Kinesio taping was applied by a co-author of the study (A.K.) who completed basic and advanced Kinesio taping courses organized by the International Kinesio Taping Association. We used muscular-ligament technique. The starting position for the Kinesio taping was the position of lumbar spine flexion with rotation in the opposite direction to the application. An “I” shaped application was used. The base was applied from the caudal side below the pain area, and the tape was directed cranially and stuck without tension (Figure 2). Identical application was made on the other side of the spine (Figure 3). Then, a transverse application with tension correction (75%) of the pain area was done (Figure 4). In addition, tape was applied to decrease lumbar spine load and support abdominal muscles (Figure 5). The placebo application was based on the Kinesio taping method (Figures 6, 7). The adhesive tape was stuck without any tension on both sides of the spine. Then, the second tape was used in a transverse way at the site where the patient indicated the pain. The application to support the abdominal muscle was then done. The Visual Analogue Scale (VAS), containing a numerical range from 0 (no pain) to 10 (strongest pain), and the Polish version of the Roland Morris Disability Questionnaire (RMDQ – 2004) were used for pain assessment. This questionnaire consisted of 24 questions and concerned problems that might occur in an individual’s daily life in relation to the painful symptoms of the spine. Women answered “yes” or “no” to each question. Answers “yes” are summed up and 1 point was awarded for each (minimum 0 point, maximum 24 points). The more points, the more the patient is disabled in the examined area. Women indicated their current pain level using the VAS before application of Kinesio taping or placebo, after returning home on the day of application, and on the 2nd and 7th day after the application. In addition, the RMDQ was filled in at the beginning of the study and 2 days after removal of the tape (on the 7th post-application day). Participants were randomly divided into 2 groups (group A – 53 women, group B – 53 women). Kinesio taping and placebo were used alternately. Group A received the Kinesio Tex Gold tape in the first stage and the placebo in the second stage. The other group (B) received the interventions in the reverse order. The wash-out period between the 2 interventions was about 3–4 weeks, and the tape was re-applied during the next visit to the office. The women in the study were asked to remove the tape on their own after 5 days. There were no dropouts.
Figure 1.
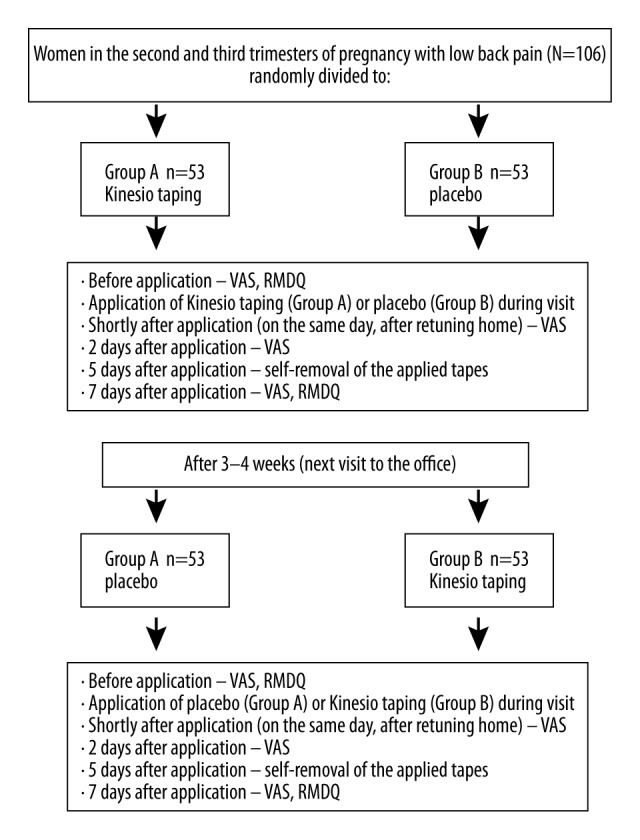
Description of study design.
Figure 2.

Application of Kinesio taping on the lumbar area.
Figure 3.

Identical application of Kinesio taping on the other side of the spine.
Figure 4.

Transverse application of Kinesio taping.
Figure 5.

Kinesio taping applied to the abdomen to decrease lumbar spine load and support abdominal muscles.
Figure 6.

Application of placebo on the spine.
Figure 7.

Application of placebo on the abdomen.
The data were statistically analyzed using the STATISTICA StatSoft, Inc. (data analysis software system version 12) tools. Descriptive statistics tools (mean, SD) and T-Student, Tukey, and ANOVA differences were used. The significance level of p<0.05 was assumed.
Results
The Table 1 contains basic characteristics of women enrolled in the study (Table 1). Analyzing the level of pain evaluated by VAS, we found that mean pain scores on the 2nd and 7th post-application days differed significantly: the mean pain score for Kinesio taping was significantly lower in the study group than in the control group (Table 2). It was noted that only in the case of Kinesio taping, a significant reduction in pain was felt (Table 3). ANOVA showed that the mean values of the sum of the RMDQ questionnaire points in the study group differed significantly (Table 4). Additional analyzes using Tukey’s Differential Test showed that the mean scores for the RMDQ before and after Kinesio taping (p<0.0001) differed significantly, as well as between Kinesio taping and placebo (p<0.0057). There were no differences before and after placebo (p<0.67) or before Kinesio taping and placebo (p<0.59). There were no adverse reactions during the study. The only reported side effect was the itching of the area covered by the tape, which was reported in 2 women (1.9%) with Kinesio Tex Gold and in no women in the placebo group.
Table 1.
Baseline characteristics of participants (N=106).
| Characteristics | n | % | Mean ±SD |
|---|---|---|---|
| Age in years: | 29.5±4.25 | ||
| ≤25 | 15 | 14 | |
| 26–30 | 52 | 49 | |
| >30 | 39 | 37 | |
|
| |||
| Education level: | |||
| Secondary and below | 30 | 28 | |
| Tertiary and above | 76 | 72 | |
|
| |||
| Trimester of gravidity | 35.2±4.3 | ||
| 2 | 13 | 12 | week |
| 3 | 93 | 88 | |
|
| |||
| Parity: | 2.42±1.2 | ||
| 0 | 52 | 49 | (n=54) |
| 1–2 | 51 | 48 | 1.2±1.4 |
| ≥3 | 3 | 3 | (n=106) |
|
| |||
| Low back pain during previous gravidity: | |||
| Yes | 31 | 29 | |
| First gravidity | 52 | 49 | |
|
| |||
| Pre-pregnancy BMI (kg/m2) | 22.3±3.5 | ||
| <18.5 | 6 | 5.7 | |
| 18.5–24.9 | 80 | 75.5 | |
| 25.0–29.9 | 16 | 15.1 | |
| >30 | 4 | 3.8 | |
|
| |||
| Work during pregnancy – yes | 63 | 59.4 | |
|
| |||
| Type of work before pregnancy | |||
| Physical | 17 | 16 | |
| Mental | 72 | 68 | |
| Unemploiment or student | 17 | 16 | |
Table 2.
The comparison of mean VAS values of pain assessment in the study and control group.
| Pain evaluation | Method | Mean ±SD | T-Student test | |
|---|---|---|---|---|
| t | p | |||
| Before application | Kinesio taping | 4.94±1.74 | −0.82 | 0.4168 |
| Placebo | 4.96±1.73 | |||
| Shortly after application | Kinesio taping | 4.88±1.72 | −0.94 | 0.3482 |
| Placebo | 4.92±1.74 | |||
| 2 days after application | Kinesio taping | 1.13±1.47 | −17.38 | <0.0001* |
| Placebo | 4.72±1.83 | |||
| 7 days after application | Kinesio taping | 1.06±1.42 | −17.69 | <0.0001* |
| Placebo | 4.77±1.79 | |||
Table 3.
The comparison of mean VAS values of pain assessment after application of Kinesio taping and placebo.
| Method | Pain evaluation | Mean ±SD | ANOVA test | |
|---|---|---|---|---|
| F | p | |||
| Kinesio taping | Before application | 4.94±1.74 | 203.01 | <0.0001* |
| Shortly after application | 4.88±1.72 | |||
| 2 days after application | 1.13±1.47 | |||
| 7 days after application | 1.06±1.42 | |||
| Placebo | Before application | 4.96±1.73 | 0.32 | 0.8087 |
| Shortly after application | 4.92±1.74 | |||
| 2 days after application | 4.72±1.83 | |||
| 7 days after application | 4.77±1.79 | |||
Table 4.
The comparison of mean values of the sum of points from the RMDQ before and after application of Kinesio taping and placebo.
| RMDQ evaluation | Mean ±SD | ANOVA test | |
|---|---|---|---|
| F | p | ||
| Before kinesio taping | 5.66±2.64 | 12.31 | <0.0001* |
| After kinesio taping | 3.67±2.40 | ||
| Before placebo | 5.20±2.21 | ||
| After placebo | 4.79±2.65 | ||
Discussion
During pregnancy, there are a number of anatomical, physiological, and biochemical changes in a woman’s body, some of which involve the skeleton. Sacro-iliac synchondrosis and pubic symphysis widen. The altered center of gravity of the pregnant woman’s body modifies the angle of the sacral position relative to the iliac bones. This results in backward bending of the upper spine, which compensates for the displacement of the body’s center of gravity due to an increase in the size of the abdomen. The fetal mass is an additional load and causes the dislocation of center of gravity. The pain may appear on one or both sides of the sacral bone and also along the paravertebral muscles. It is estimated that pain in the lumbar-sacral spine occurs in 45–56% of pregnant women. These problems can appear as early as in the 12th week of pregnancy, and their severity increases between the 24th and 30th gestational weeks [6]. Cervical or lumbosacral spinal pain is one of the most common problems that women report during pregnancy. There are many physiotherapeutic methods that help to relieve pain in the spine. However, pregnancy is a period in which careful care and attention should be exercised. Recent recommendations based on randomized controlled trials support the effectiveness of physical exercise in the treatment of chronic spinal pain. Moderate physical activity and breathing exercises, walking, and swimming are recommended for women who do not have a high-risk gestation. To reduce low back pain, massage is also used, but is only permitted before the second trimester of pregnancy [13]. The effectiveness of Kinesio taping in the treatment of osteoarthritis has been demonstrated in numerous publications. The effect of Kinesio taping on abdominal oblique muscles and symmetry of pelvic movements was investigated by Dylewski et al. [14]. Erkan et al. [15] examined the effect of dynamic taping on cervical pain. Ciosek et al. [16] conducted a study on the use of Kinesio taping in chronic pain in the lumbar-sacral spine. A similar study design was used by Castro-Sanchez et al. [17] in their study of the effects of Kinesio taping on pain relief of the lumbar spine. The influence of the Kinesio taping method on pain control was also investigated by Czyzewski et al. [18], who focused on the pain experienced after fracture of the ribs. Interesting research was also done at Hacettepe University in Ankara, Turkey in collaboration with the Shanghai Clinic. Aytar et al. [19] conducted studies on the use of Kinesio taping in anterior knee compartment pain. Researchers from Sao Paulo, Brazil by Alves de Oliveira et al. [20] investigated the use of Kinesio taping in painful shoulder syndrome. In the scientific literature, there are few reports of spinal pain control in pregnant women using Kinesio taping. In a study by Senderek et al. [11], the research material comprised 48 women between the 5th and 9th month of pregnancy. Muscular-ligament technique was used in the study to reduce spinal pain and lymphatic technique to reduce swelling of the lower limbs. When referring to the results of the above-mentioned studies, the Kinesio taping method, as in our own study, results in reduction of pain in the low back area. In the study, Senderek et al. [11] found that the therapeutic effect can be maintained for 24 h from application. The results of our own studies show that the therapeutic effect can be maintained for as long as a few days. In addition, the results of both studies indicate that the Kinesio taping tape does not cause allergic reactions and is a method acceptable to pregnant women. Sabour et al. [21] conducted a study of 30 primiparas in the third trimester of pregnancy. Women were divided into 2 groups: in the first one there were pregnant women who exercised to reduce spine pain, and in the second group they performed identical physical exercises and Kinesio taping was also applied. The VAS scale was used to assess the pain level, the Oswestry questionnaire assessed disability, and a flexible ruler was used for measuring the angle of lordosis in the sagittal plane. All measurements were performed before and after the test. The results of the study, as well as our own research, have clearly confirmed that Kinesio taping is an effective method to combat lower back pain and may provide a safe complement to other therapies. Recent research on the reduction of low back pain in pregnant women was carried out in Turkey in 2015 by Kaplan et al. [5]. Sixty-five women were included in the study. All of them were treated with paracetamol, which was not used in our study. The Kinesio taping method was additionally applied in the study group. As in the present study, the RMDQ and the VAS scale were used to evaluate the results. They showed that Kinesio taping combined with paracetamol treatment is more effective than pharmacological treatment alone. As in our own studies, it has also been demonstrated that the Kinesio taping method is effective and can therefore be used as a complementary therapy for low back pain in pregnant women. Ceren Gürşen et al. [22] examined the impact of Kinesio taping on abdominal muscle strength after caesarean section. The study involved 24 women and was conducted 4 to 6 months after delivery. All women practiced appropriate physical exercises. The Kinesio taping method was additionally used in the study group (n=12). Dynamic taping was applied twice a week for 4 weeks for straight and oblique abdominal muscles as well as for the caesarean section scar area. The RMDQ and the VAS scale were used to evaluate the method by the authors, as in our own studies. The results of the study confirmed the effectiveness of the Kinesio taping for strengthening abdominal muscles. The study was conducted on a small group, so the authors concluded that the research should be continued. In 2015, Liddle and Pennick [23] presented a meta-analysis of the different ways of preventing and treating low back pain in pregnancy. Among these methods there was Kinesio taping, but the cited authors found only 1 paper devoted to this issue, published by Kay et al. [24]. Their material consisted of 29 pregnant women who were treated with Kinesio taping and exercise, and acetaminophen in the control group. In both groups, pain and functional disability were significantly less intense with treatment, whereas in the Kinesio taping group the improvement was significantly greater than in the control group.
The method of dynamic taping is often used in a variety of conditions, but this does not translate into the number of scientific reports in this field. The number of studies on the effects of the Kinesio taping method on a variety of ailments and conditions is very limited. There are no prospective, randomized studies on large groups that would confirm or exclude the efficacy of this method. The review of the above publications provides controversies regarding the effect of Kinesio taping. Most of the cited studies and the present research confirm the beneficial effect of Kinesio taping on pain relief. On the other hand, in studies using the Kinesio taping-placebo comparison method, conflicting results were obtained. It is worth stressing that dynamic taping is a safe method. These publications confirm that the Kinesio taping relieves pain and can be used as a complementary or surrogate therapy in case of contraindications to other forms of physiotherapy. In most studies, however, long-term therapeutic effects have not been observed. The results obtained in our own studies confirm the positive effect of Kinesio taping in the treatment of low back pain in pregnant women.
Conclusions
Low back pain in pregnant women, as evaluated by VAS and RMDQ after Kinesio taping, decreased significantly compared to placebo. The therapeutic effect starts from day 2 and is maintained for 2 days after removal of the tape. Side effects were very few and did not affect the course of the study.
Footnotes
Source of support: Departmental sources
Conflicts of interest
None.
References
- 1.Palmer K, Walsh K, Bendall H. Back pain in Britain: Comparison of two prevalence surveys at an interval of 10 years. BMJ. 2000;320:1577–78. doi: 10.1136/bmj.320.7249.1577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Van Tulder M, Koes B, Bouter L. A cost-of-illness study of back pain in the Netherlands. Pain. 1995;62(2):233–40. doi: 10.1016/0304-3959(94)00272-G. [DOI] [PubMed] [Google Scholar]
- 3.Svensson H, Andersson G, Hagstad A, et al. The relationship of low-back pain to pregnancy and gynecologic factors. Spine. 1990;15:371–75. doi: 10.1097/00007632-199005000-00006. [DOI] [PubMed] [Google Scholar]
- 4.Wu W, Meijer O, Uegaki K, et al. Pregnancy-related pelvic girdle pain (PPP). Terminology, clinical presentation, and prevalence. Eur Spine J. 2004;13:575–89. doi: 10.1007/s00586-003-0615-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kaplan S, Alpayci M, Karaman E, et al. Short-term effects of kinesio taping in women with pregnancy – related low back pain: a randomized controlled clinical trial. Med Sci Monit. 2016;22:1297–301. doi: 10.12659/MSM.898353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vermani E, Mittal R, Weeks A. Pelvic gridle pain and low back pain in pregnancy: A review. Pain Pract. 2010;10:60–71. doi: 10.1111/j.1533-2500.2009.00327.x. [DOI] [PubMed] [Google Scholar]
- 7.Wang S, De Zinno P, Fermo L, et al. Complementary and Alternative medicine for low back pain in pregnancy: a cross sectional survey. J Altern Complement Med. 2005;11(3):459–64. doi: 10.1089/acm.2005.11.459. [DOI] [PubMed] [Google Scholar]
- 8.Sneag DB, Bendo JA. Pregnancy-related low back pain. Orthopedics. 2007;30(10):839–45. doi: 10.3928/01477447-20071001-14. [DOI] [PubMed] [Google Scholar]
- 9.Rycyk M, Marczewski K. [Physical activity of pregnant women according to men]. Fizjoterapia. 2012;XIV 1(35):55–61. [in Polish. [Google Scholar]
- 10.Bell BB, Dorset, Dooley MMP. Exercise in pregnancy (RCOG Statement 4) London: Jan 1, 2006. Royal College of Obstetricians and Gynaecologists. [cited 2017 March 10] Available from: www.rcog.org.uk/womens-health/clinical-guidance/exercise-pregnancy. [Google Scholar]
- 11.Senderek T, Breitenbach S, Hałas I. [Kinesio taping – new possibilities of physiotherapy in pregnant women]. Fizjoterapia Polska. 2005;5(2):266–71. [in Polish] [Google Scholar]
- 12.Szczegielniak J, Krajczy M, Bogacz K, et al. Kinesio taping in physiotherapy after abdominal surgery. Fizjoterapia Polska. 2007;7(3):299–307. [in Polish] [Google Scholar]
- 13.Recreational exercise and pregnancy. Royal College of Obstetricians and Gynaecologists; London: Sep, 2006. [cited 2017 March 10] Available from: http://www.rcog.org.uk/globalassets/documents/patients/patient-information-leaflets/pregnancy/recreational-exercise-and-pregnancy.pdf. [Google Scholar]
- 14.Dylewski M, Sójka M, Senderek T, et al. [The influence of Kinesio taping application on oblique abdominal muscles on symmetry of pelvical movements]. Fizjoterapia Polska. 2008;3:290–98. [in Polish] [Google Scholar]
- 15.Erkan H, Harput G, Baltaci G. Additional effects of kinesiotaping to mobilization techniques in chronic mechanical neck pain. Turkish Journal of Physiotherapy and Rehabilitation. 2015;26(3):107–13. [Google Scholar]
- 16.Ciosek Ż, Kopacz Ł, Samulak Ł. [The influence of Kinesio taping on sacro-lumbar back pain]. Pomeranian Journal of Life Science. 2015;61(1):115–19. [in Polish] [PubMed] [Google Scholar]
- 17.Castro-Sanchez AM, Lara-Palomo IC, Mataran-Penarrocha G. Kinesio taping reduces disability and pain slightly in chronic non-specific low back pain: A randomized trial. J Physiother. 2012;8(5):89–95. doi: 10.1016/S1836-9553(12)70088-7. [DOI] [PubMed] [Google Scholar]
- 18.Czyżewski P, Hałas I, Kopytiuk R, et al. [Application of the Kinesio taping method in reduction of pain after costal fractures – a preliminary report]. Postępy Rehabilitacji. 2012;(4):29–35. [in Polish] [Google Scholar]
- 19.Aytar A, Ozunlu N, Surenkok S. Initial effects of kinesio taping in patients with patellofemoral pain syndrome: A randomized, double-blind study. Isokinetics and Exercise Science. 2011;(19):135–42. [Google Scholar]
- 20.Alves de Oliveira VM, Paixa Batista L, Rodarti Pitangui AC. Effectiveness of Kinesio taping in pain and scapular dyskinesis in athletes with shoulder impingement syndrome. Revista Dor Sao Paulo. 2013;14(1):27–30. [Google Scholar]
- 21.Sabbour A, Omar H. The effect of Kinesiotaping therapy augmented with pelvic tilting exercises on low back pain in primigravidas during the third trimester. Faculty of Physical Therapy, Cairo University. 2011;16(1):53–61. [Google Scholar]
- 22.Gürşen C, İnanoğlu D, Kaya S, et al. Effects of exercise and Kinesio taping on abdominal recovery in women with cesarean section: A pilot randomized controlled trial. Arch Gynecol Obstet. 2016;293(3):557–65. doi: 10.1007/s00404-015-3862-3. [DOI] [PubMed] [Google Scholar]
- 23.Liddle SD, Pennick V. Interventions for preventing and treating low-back and pelvic pain during pregnancy. Cochrane Database Syst Rev. 2015;(9):CD001139. doi: 10.1002/14651858.CD001139.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kaya E, Yosunkaya N. The effect of Kinesiotaping on low back pain during pregnancy. Turkish Journal of Physical Medicine and Rehabilitation. 2013;59(Suppl 1):248. [Google Scholar]