

Abstract
Objective
The purpose of this study was to examine, using structural equation modeling, the associations between nominated friend physical activity (PA), friend social support with individual psychological factors, and adolescent PA.
Methods
Data were obtained from EAT 2010 (Eating and Activity Among Teens), a large cross-sectional study conducted in 20 middle and high schools. The sample consisted of 1951 adolescents (mean age: 14.25 ± 1.96, 54% female, 68% ethnic minorities). PA, parent and friend socia l support (perceived social support for PA from parents and friends), and psychological measures (PA enjoyment, PA self-efficacy, and PA barriers) were assessed by self-report questionnaires. The SEM analysis consisted of 1 observed variable: friend PA, and 2 latent constructs: psychological factors, perceived social support.
Results
The model was a good fit, indicating that there were significant direct effects of both friend PA (P < .01) and psychological factors (P < .0001) on adolescent PA. In addition, psychological factors mediated the association between friend PA and adolescent PA.
Conclusion
The results of this model suggest that psychological factors and friend PA are associated with adolescent PA, and that psychological factors may play an important role. Future studies should further examine the association of both friend PA and psychological variables with adolescent PA.
Keywords: social influences
Physical activity (PA) has been shown to be associated with a variety of positive health outcomes in children and adolescents such as decreased risk of cardiovascular disease, obesity, type 2 diabetes, and improved psychological and emotional health.1–3 Despite the known benefits of PA, only 24.8% of adolescents (ages 12 to 19) meet the current recommendations of 60 minutes or more of moderate to vigorous physical activity (MVPA) on all days of the week.2 Furthermore, there is evidence that PA participation declines as children age.3 PA during adolescence is of particular importance, give that sedentary adolescents are more likely to remain sedentary and are at greater risk of becoming overweight as adults.4 Therefore, it is imperative to continue examining the multilevel influences on youth PA.
To guide the development of interventions and policies aimed at increasing PA during adolescence, it is important to identify factors associated with PA. A number of studies have assessed the correlates and/or determinants of youth PA, especially psychological5,6 and neighborhood environment factors.7 Results from these studies have reported that psychological variables such as PA enjoyment, PA self-efficacy, and barriers to PA were significantly correlated with adolescent PA.5,8,9 For example, Lubans et al10 used structural equation modeling (SEM) to determine the associations between Social Cognitive Theory (SCT)11 constructs and self-reported PA in 1518 adolescent girls, observing that self-efficacy was most strongly associated with PA behavior. Another factor that may be associated with PA in adolescents is perceived social support for PA.12 Studies have examined both friend and family support for PA, and results have shown that some studies have found a positive association,12–14 while others have not.10 Lubans et al10 found that while social support for PA was significantly associated with self-efficacy, it was not correlated with PA behavior in adolescents. The researchers speculated that the lack of significance could be attributed to not including family support for PA in their model. Similarly, Beets et al8 used SEM to examine the role of social support and self-efficacy for PA in 259 high school girls. Interestingly, in contrast to Lubans et al,10 Beets et al8 observed that peer social support, but not parental social support, was directly associated with high school girls’ PA.
While perceived social support for PA has been shown to be associated with adolescent PA in some studies,12–14 relatively little is known regarding other social influences on adolescent PA behavior such as friend PA. A study by Jago et al15 examined whether the number of friends in an adolescent’s social circle was associated with PA in a sample of 10 to 11 year old children, and found that an increase in number of friends was associated with an increase in adolescent PA. Similarly, a study by Salvy et al16 that had adolescents record their social interactions for 7 days using a 2-way pager, found that adolescents were more likely to have greater level of PA intensity when in the presence of friends than when adolescents are by themselves or with family. There is evidence that suggests friends may have a direct impact on adolescents’ attitudes and beliefs toward PA, and that adolescents are more likely to either choose friends who have similar PA behavior or alter their PA behavior in response to their friends.17,18 A longitudinal study by De la Haye et al17 examined, over the course of a school year, whether participation in PA was relevant to the formation of adolescent friendships and whether adolescents were influenced by their friends’ PA in a sample of 378 8th-grade students. The results from this study indicated that participation in PA was found to play a significant role in friendship selection, with participants preferring friends whose PA levels were similar to their own. In addition, friends appeared to influence participants’ PA over the school year, as participants’ PA levels changed to become more similar to their friends.17
The majority of studies have not measured friends’ PA directly, and out of those few studies that have,17–19 only 1 study to our knowledge17 examined adolescent psychological variables in conjunction with friends’ PA. De la Haye et al17 found that adolescent PA was associated with attitudes toward PA, however, these attitudes did not mediate the relationship between friends’ PA and adolescent PA. The current study will examine chosen psychological variables (PA enjoyment, PA self-efficacy, PA barriers) that have been consistently shown to be significantly associated with adolescent PA5,21–24 to explore if they mediate the relationship between nominated friends’ PA and adolescent PA. The current study extends previous research by utilizing an SEM approach to determine the associations between the novel assessment of nominated friend PA and individual adolescent PA, while including more robust theory-derived psychosocial measures. By better understanding the relationship among friends’ PA, adolescent psychological variables, and adolescent PA, investigators will be able to identify the factors that are the driving force of adolescent PA. It was hypothesized that friend PA would be directly associated with individual MVPA and that this relationship would mediated by individual psychological variables, which is supported by both Baker et al25 and Voorhees et al26 who found that adolescents who had physically active friends, were more likely to have better attitudes about PA and to be more active themselves. In addition, perceived social support was hypothesized to mediate the relationship between the psychological variables and adolescent MVPA, an approach similar to Beets et al8 who found that social support mediated the relationship between self-efficacy for PA and individual PA behavior.
Methods
Sample
The data from this study are from the EAT-2010 (Eating and Activity among Teens) study which was designed to examine dietary intake, physical activity, weight control behaviors, weight status, and factors associated with these outcomes in adolescents. There were a total of 2973 7th- to 12th-grade participants in the EAT-2010 study recruited from 20 public schools in Minneapolis and St. Paul MN. Six schools were traditional middle schools (6th to 8th grade), eight were traditional high schools (9th to 12th grade), 3 were K-8th grade, 1 was K-12th grade, 1 was 6th to10th grade, and 1 was 7th to 12th grade.
Due to missing data on key variables such as psychological variables, perceived social support, and nominated friends not being in the sample (18%), the current study comprised 1951 adolescents (mean age 14.25± 1.96). The sample was fairly equally divided on gender (54% girls). A majority of the sample (68%) were ethnic minorities and over half of the sample (55%) was of lower SES, defined by household income (low, middle-low, middle, middle-high, high) (Table 1). Independent sample t tests and chi-square tests examined the differences between those included in the sample (n = 1951), and the participants that were excluded (n = 629). There were no significant differences in gender or hours of MVPA per week. However, the included sample had a significantly lower BMI (P = .004), lower SES (P = .003), were significantly younger (P < .0001), and contained a higher percentage of Caucasians (P < .0001).
Table 1.
Descriptive Statistics for Sample (n = 1951)
| Variable | n (%) | Mean (SD) | Range |
|---|---|---|---|
| Male | 897 (46) | ||
| Caucasian | 627 (32) | ||
| SES (Total income) | |||
| Low (<$20,000) | 576 (29.5) | ||
| Low-middle ($20,000–34,999) | 500 (25.6) | ||
| Middle ($35,000–74,999) | 677 (34.7) | ||
| Upper-middle ($75,000–99,999) | 136 (6.9) | ||
| High ($100,000+) | 62 (3.2) | ||
| Age (yrs) | 14.3 (2.0) | 10–20 | |
| BMI (kg/m2) | 23.6 (5.7) | 13.6–55.6 | |
| MVPA (hrs/wk) | 5.9 (4.7) | 0–16 | |
| Number of nominated friends in sample | 2.08 (1.7) | 0–6 | |
Abbreviations: SES, XXX; BMI, body mass index; MVPA, moderate-to-vigorous physical activity.
Trained research staff administered surveys and measured adolescents’ height and weight during physical education and science classes during the 2009–2010 academic year. All study procedures were approved by the University of Minnesota’s IRB Human Subjects Committee and by the research boards of the participating school districts. The parent/guardian of each participant provided passive consent before the student being included in the investigation (parents/guardians could contact study staff if they did not want their child to participate), and the child provided assent.20,25,27
Measures
Friend Nominations
Before data collection, rosters of all students by grade level were obtained from each school. Each participant was given a unique 4-digit identification (ID) number. Participants nominated up to 6 of their best friends (3 male friends and 3 female friends) from the school roster. PA data provided by each nominated friend was linked by ID number back to the original nominating friend, therefore allowing for the measurement of mean nominated friend PA for each participant. In the EAT-2010 cohort, participants nominated an average of 2.1 ± 1.7 friends who had provided usable data in their own surveys. A sensitivity analysis was conducted, and results indicated that using all participants with at least 1 friend provided similar results to using more stringent inclusion criteria (eg, requiring at least 2 or more nominated friends to be included).27
Godin-Shephard Physical Activity Recall
The Godin-Shephard (G-S) PA recall28 asks participants to record the number of hours in a typical week that they engaged in strenuous (“heart beats rapidly”), moderate (“not exhausting”), and mild exercise (“little effort”). The G-S recall has been previously validated in adolescent and adult populations using various criterion measures, such as the Caltrac accelerometer (r = .32 to 0.45),29 aerobic fitness (r = .38 to 0.56),30 other PA questionnaires (r = .36 to 0.61),31 and a modified version of the G-S recall has been used in previous waves of Project EAT.27 Response options were “none,” “<0.5 hours/week,” “0.5–2 hours/week,” “2.5–4 hours/week,” “4.5–6 hours/week,” and “6+ hours/week,” and were coded as 0, 0.25, 1.25, 3.25, 5.25, and 6.75 hours/week, respectively. The sum of the responses for both strenuous and moderate PA was calculated to determine hours spent in moderate to vigorous PA (MVPA) per week.
Psychological Variables
Self-efficacy for PA was self-reported by adolescents using a modification of a previously validated scale.32 This scale consisted of questions that measured children’s confidence in their ability to overcome barriers and engage in PA. The questionnaire started “I can be physically active during my free time on most days …” followed by the statements “no matter how busy my day is,” “even if it is very hot or cold outside,” and “even if I have to stay home.” Response options for this 4-point scale ranged from 1 (“Disagree a lot”) to 4 (“Agree a lot”). Internal consistency for this scale was α = 0.76.
PA enjoyment was measured using a modification of a previously validated scale33 that asked 3 questions that started “When I am active …” followed by the items “I feel bored,” “I dislike it,” and “It frustrates me.” The 4-point scale contained responses that ranged from 1 (“Agree a lot”) to 4 (“Disagree a lot”), with a higher score indicative of more enjoyment related to PA. Internal consistency for this scale was α = 0.82.
Perceived barriers to PA were measured with 4 items adapted from a validated scale by Dishman et al34 which asked “How often do these things keep you from being physically active?” Items included “The weather is bad,” “I don’t have time to do physical activity,” “It would take time away from my school work,” and “I’m embarrassed about how I look when I’m active.” The 5-point scale ranged from 1 (“very often”) to 5 (“never”), with a higher score indicative of fewer barriers. Internal consistency for this scale was α = 0.49.
Social Support (Family and Friend)
Perceived family and friend support for PA, adapted from Davison et al,35 asked the participants to record “How strongly do you agree with the following statements?” For family support, items included “My family and I do active things together” and “My family supports me in being physically active.” For friend support, items included “My friends often play sports or do something active,” “My friends think it is important to be physically active,” and “My friends and I like to do active things together.” Scales contained 4-point response options that ranged from 1 (“Disagree a lot”) to 4 (“Agree a lot”), with a higher score indicative of more social support for PA. Internal consistencies for both family and friend scales were α = 0.67.
Statistical Analysis
Descriptive statistics were performed using SAS statistical software, version 9.2. Independent sample t tests and chi-square tests were performed to examine possible differences in demographic variables between the included (n = 1951) and excluded (n = 629) participants. Given the wide age range of the sample and the possibility of differences in correlates of PA with age, t tests were conducted to examine differences in MVPA between younger (12 years and under) and older adolescents (13 to 19 years of age). If differences existed, further analyses were conducted to examine the associations with psychological factors, social support, and nominated friends’ PA.
Previous models have placed psychological variables with social support, but to further explore the social environment for PA, our approach was one that separated perceived support from the psychological variables, an approach similar to Heitzler et al36 and Beets et al.7 Friend PA was kept as a separate construct from social support because friend PA was measured directly from the nominated friends, while social support was the individual’s perception of support from family and friends.
The measurement model is represented in Figure 1. This measurement model consisted of 2 measured variables (friend PA, individual PA), and 2 latent constructs (psychological factors and perceived social support). Psychological factors consisted of PA self-efficacy, PA enjoyment, and PA barriers. Perceived social support consisted of the measured variables: friend support for PA, and family support for PA. The following covariates were also added to the model: age, gender, race, BMI, and SES.
Figure 1.

Structural Equation Model
Structural equation models (SEM) were examined using MPLUS 6 statistical software with maximum likelihood estimation. Model fit was evaluated based on the following fit indices: the model chi-square statistic, the root mean square error of approximation (RMSEA) and its 90% confidence interval, the Bentler comparative fit index (CFI), and the Tucker-Lewis Index (TLI). These indices reflect current standards and recommendations for reporting in SEM analyses.37 All indices, however, are affected by multiple design factors and the interpretation of what constitutes good fit varies across studies.37 In particular, the chi-square statistic is sensitive to sample size and often prone to type 1 error and, for this study, the chi-square results were interpreted in the context of the other model fit measures. It is generally accepted that an RMSEA less than .05 corresponds to a “good” fit and an RMSEA less than .08 corresponds to an “acceptable” fit.38 For the CFI and TLI scores, a number greater than .9 indicates a good model fit.38
Results
Structural Equation Model
Results showed good convergent validity of the factors as each indicator’s factor loading was significant (P < .0001) on its respective latent variable. All correlations among the psychosocial factors were statistically significant (P < .05), but none of the estimated correlations were excessively high (ie, ≥ 0.85). The strongest correlations were between the psychological variables and both forms of social support for adolescent PA (r = .68) and adolescent MVPA (r = .56) (Table 2).
Table 2.
Correlations Among Variables
| Variables | Friend PA | Psychological Factors | Social Support | Adolescent MVPA |
|---|---|---|---|---|
| Friend PA | 1.00 | .11* | .13* | .13* |
| Psychological Factors | .11* | 1.00 | .68* | .56* |
| Social Support | .13* | .68* | 1.00 | .40* |
| Adolescent MVPA | .13* | .56* | .40* | 1.00 |
Abbreviations: PA, physical activity; MVPA, moderate-to-vigorous physical activity.
P < .05.
Hypothesized paths and standardized parameter estimates are shown in Figure 2. The fit indices suggest that the model was a good fit (TLI = 0.90, CFI = 0.93 and RMSEA = .041, 90% confidence interval = 0.034 to 0.049). There were statistically significant direct effects between the psychological variables and MVPA (β = 0.530, P < .0001), and friend PA and MVPA (β = 0.058, P = .008). For the direct effect between psychological variables and MVPA, this standardized beta weight, for example, can be interpreted as a .53 standard deviation unit increase in the level of MVPA for a 1 standard deviation unit increase in the level of psychological variables. Friend PA was associated with the psychological variables (β = 0.125, P < .0001) and the psychological variables were associated with social support (β = 0.688, P < .0001), which suggests that these 2 mediator influence each other as well. However, social support was not directly associated with MVPA. Overall, the model accounted for approximately 23% of the variance in adolescent MVPA.
Figure 2.
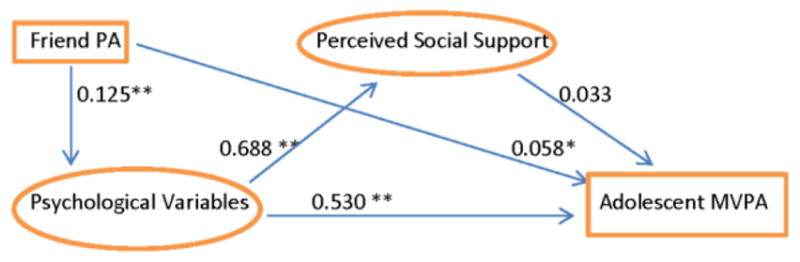
Hypothesized paths and standardized parameter estimates
*p<.01, **p<.0001
Exploratory Analyses
Regression analyses stratified by age (older and younger adolescents) indicate that psychological and social correlates associated with MVPA differed according to age. In addition to friends’ PA, number of friends was added to the model to explore if increased number of friends was associated with MVPA. For younger participants (12 and under), all of the psychological factors, decreased PA barriers (β = −.16, SE = .06, P = .005), increased PA self-efficacy (β =.27, SE = .05, P < .0001) and greater enjoyment of PA (β = .15, SE = .06, P = .008), were associated with increased levels of MVPA. For older participants (13 to 19 years), increased PA self-efficacy (β = .28, SE = .1, P = .006) and increased enjoyment of PA (β = .19, SE = .09, P = .002) were associated with increased levels of MVPA. For social support and friend PA, family support for PA (β = .16, SE = .06, P = .009) and friend PA (β = .04, SE = .02, P = .05) were associated with increased MVPA in younger adolescents, however, only friend PA (β = .1, SE = .05, P = .04) was associated with increased MVPA in older adolescents.
Discussion
The current study examined the direct and indirect pathways of both individual and social-level associations with adolescent MVPA. The results showed an overall good fit between the proposed model and the data. Before the final model, a previous model had been tested which proposed that friends’ PA mediated the relationship between psychological variables and adolescent MVPA. However, the model fit was unacceptable (TLI < .90, CFI < .90, RMSEA > .05), and the model was greatly improved when friend PA was proposed to have direct and indirect effects on adolescent MVPA. Friend PA was directly associated with adolescent MVPA, and, in addition, the psychological variables mediated the pathway between friend PA and adolescent MVPA. Interestingly, there were no significant direct effects from social support to adolescent MVPA. Therefore, nominated friend PA and psychological factors were most strongly associated with adolescent MVPA, while perceived social support was not.
Among all variables, the psychological factors were the strongest correlates of adolescent MVPA. This finding is in agreement with Lubans et al10 who found individual psychological variables such as self-efficacy to have the strongest association with adolescent MVPA. The majority of studies have reported that psychological variables are associated with MVPA in adolescents,7,10,21,23 and adult populations.39 A new finding of this study was that these variables mediated the relationship between friend PA and adolescent MVPA.
In the current study, social support for PA was not associated with adolescent MVPA. This finding was surprising given that other studies, including the previous Project EAT cohort, have found social support for PA to be associated with adolescent MVPA.40 However, our current findings are supported by Heiztler et al34 who found that parental support was not associated with MVPA, and Lubans et al10 who reported no significant associations between peer social support and adolescent MVPA. However, our study differs from several of these studies in that we also examined hypothesized psychological variables, which appeared to be the driving force in the model. Interestingly, significant associations existed between psychological factors and social support suggesting there may be a reciprocal relationship between those variables. Evidence does suggest that increased support for PA by family in younger children, is associated with more positive feelings toward PA.33 In addition, our regression models revealed that younger participants’ MVPA was associated with family support for PA, although neither friends nor parent support for PA was associated with MVPA in older adolescents. This is partially supported by Sirard et al,20 who suggested that younger children may be more influenced by parents than older adolescents. Our overall findings are in contrast to Springer et al12 who found that both family and friend social support were significantly correlated with PA in a sample of 718 6th-grade girls. However, rather than using a composite variable for social support, Springer et al12 examined the mean values of varying types of social support (friend participation vs friend encouragement), which may account for the difference in findings. Therefore, it is possible that different aspects of social support may be more strongly associated with MVPA in adolescents.
There are several limitations of this study. First, is that the variables in this study were derived through self-report measures which are prone to recall error. Secondly, participants could only nominate friends who were attending the same school, and those friends could only be included in the data set if they, too had completed a EAT 2010 survey. Therefore, it is possible that adolescents had additional friends whose PA behavior was not examined in the study. Excluded participants had a significantly lower BMI than included participants which may have altered results. The use of self-reported PA questionnaires over objective measures is also a limitation. In addition, participants who reported no nominated friends were excluded from the study, which serves as a limitation since there is evidence that adolescents who spend more time alone have lower levels of PA.16,18 Finally, these data are cross-sectional, and therefore, temporality of relationships cannot be established. Though the results of this analysis cannot provide causality, this model does provide support for friend and individual level associations with adolescent MVPA. There are several implications based on the results of this study. It appears that PA behavior in adolescents may be more associated with the behavior of their friends rather than the combined perceived social support for PA from parents and friends. In addition, it corroborates with previous research indicating that individual beliefs about PA behavior, as the most proximal level of influence, remains a critically important correlate of adolescent MVPA. This finding is supported by several studies that have found psychological variables such as self-efficacy to be the strongest correlate of PA behavior.12,21 However, there is still a large proportion of variance in MVPA among adolescents that is not explained by the current, and previous, models. It is also likely that there are built environmental and additional social variables that are influencing these individual-level variables. Future studies should consider the association of built environment characteristics with PA (eg, street network, proximity to parks and schools) in addition to the social environment to better understand the socioenvironmental contexts that promote PA in youth.
In addition to social and physical environmental variables, obtaining qualitative data in the form of interviews or focus groups would provide deeper insight into peer influence on adolescent PA. Rich qualitative data may help to provide some additional focus to future studies. For example, results from qualitative studies may suggest that there should be a focus on types of friends (sports team friends, neighborhood friends), as well as a focus on number of friends, the emotional closeness of the friend (eg, best friends), and the position or status of the individual and those close friends within the adolescent’s social network. In addition, there were differences in the correlates associated with MVPA in older and younger participants, although friend PA remained and psychological variables appeared important for both groups. Parental support may influence younger adolescents, but this association may weaken as children age, and therefore, future qualitative and quantitative research should further explore how the social dynamic changes as children go through their adolescent years.
A novel finding of the current study was that nominated friend PA was directly and indirectly associated with adolescent MVPA. Only a few studies have examined this relationship between measured friend MVPA and individual MVPA. The direct association of friend PA and adolescent PA is supported by the results of Sirard et al.,20 who found, in a sample of 2126 adolescents from the EAT 2010 study, a significant correlation between adolescents’ PA and their friends’ PA. This current study, however, also found that psychological factors (PA enjoyment, PA self-efficacy, PA barriers) mediate the relationship between adolescent MVPA and friends’ MVPA which suggests that adolescents’ attitudes toward PA may be influenced by the PA behavior of his/her friends. This finding is supported by a qualitative study conducted by Jago et al,15 with participants reporting that friends influenced their PA behavior and were a key factor influencing enjoyment (enjoyment of PA was the most important factor in maintaining activity participation). De la Haye et al17 found that adolescents’ self-reported PA tended to become more similar to that of their friends over a 1-year period, in addition to being friends with others who already had similar PA levels. These findings imply that adolescents may be influenced by their friends’ activity levels, and that a change in friends’ PA behavior may be associated with a change in the individual-level psychological variables associated with PA (eg, PA self-efficacy and enjoyment), and thus, the individual’s PA behavior. Additional longitudinal data are needed to identify the mechanisms regarding the transmission of attitudes, beliefs, and actual PA behavior within and among adolescent social networks.
In summary, nominated friend MVPA was directly associated with adolescent MVPA, but was also mediated through PA psychological constructs (PA self-efficacy, PA enjoyment, and PA barriers). Further investigation of the direct and mediating mechanisms underlying the social influences on adolescent PA is warranted, taking into account the strong association of the psychological constructs. By understanding the social influences on PA, effective PA interventions that may not only directly increase MVPA in adolescents, but also have an impact on the social network, thereby, improving how adolescents in the network think and feel about PA as well as their actual PA behavior.
Acknowledgments
The authors thank the participating schools, students, and sources of funding for the study: NIH NICHD R21 5R21HD58707-2 (principal investigator: JRS). Project EAT-2010 was funded by NIH NHLBI 1 RO1 HL084064-01A2 (principal investigator: DN-S) and NIH NICHD R21 5R21D58707-2 (principle investigator: JRS).
Contributor Information
Jeanette M. Garcia, Nutrition Dept, Harvard TH Chan School of Public Health, Boston, MA
John R. Sirard, Dept of Kinesiology, University of Massachusetts at Amherst
Ross Larsen, Youth-Nex, Curry School of Education, University of Virginia, Charlottesville, VA.
Meg Bruening, School of Nutrition and Health Promotion, Arizona State University, Tempe, AZ.
Melanie Wall, Dept of Biostatistics, Mailman School of Public Health, Columbia University, New York, New York.
Dianne Neumark-Sztainer, Division of Epidemiology and Community Health, University of Minnesota, Minneapolis, MN.
References
- 1.Sallis JF, Patterson TL, Buono MJ. Relation of cardiovascular fitness and physical activity to cardiovascular disease risk factors in children and adults. Am J Epidemiol. 1988;127(5):933–941. doi: 10.1093/oxfordjournals.aje.a114896. [DOI] [PubMed] [Google Scholar]
- 2.DHHS. 2008 physical activity guidelines for Americans. http://health.gov/paguidelines/pdf/paguide.pdf.
- 3.Fakhouri TH, Hughes JP, Burt VL, Song M, Fulton JE, Ogdon CL. Physical Activity in U.S. Youth Aged 12 – 15 Years, 2012. NCHS Data Brief, no 141. Hyattsville, MD: National Center for Health Statistics; 2014. [PubMed] [Google Scholar]
- 4.Pietilainen KH, Kaprio J, Borg P, et al. Physical inactivity and obesity: a vicious circle. Obesity (Silver Spring) 2008;16(2):409–414. doi: 10.1038/oby.2007.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Barr-Anderson DJ, Young DR, Sallis JF, et al. Structured physical activity and psychosocial correlates in middle-school girls. Prev Med. 2007;44(5):404–409. doi: 10.1016/j.ypmed.2007.02.012. [DOI] [PubMed] [Google Scholar]
- 6.Spiridon K. Psychological correlates of physical activity in children and adolescents in a cluster analytical approach. Int J Sports Sci. 2011;1(11):9–19. [Google Scholar]
- 7.Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 1993;25(1):99–108. doi: 10.1249/00005768-199301000-00014. [DOI] [PubMed] [Google Scholar]
- 8.Beets MW, Pitetti KH, Forlaw L. The role of self-efficacy and referent specific social support in promoting rural adolescent girls’ physical activity. Am J Health Behav. 2007;31(3):227–37. doi: 10.5555/ajhb.2007.31.3.227. [DOI] [PubMed] [Google Scholar]
- 9.Brodersen NH, Steptoe A, Williamson S, Wardle J. Sociodemographic, developmental, environmental, and psychological correlates of physical activity and sedentary behavior at age 11 to 12. Ann Behav Med. 2005;29(1):2–11. doi: 10.1207/s15324796abm2901_2. [DOI] [PubMed] [Google Scholar]
- 10.Lubans DR, Okely AD, Morgan PJ, Cotton W, Puglisi L, Miller J. Description and evaluation of a social cognitive model of physical activity behavior tailored for adolescent girls. Health Educ Res. 2012;27(1):115–128. doi: 10.1093/her/cyr039. [DOI] [PubMed] [Google Scholar]
- 11.Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31:143–164. doi: 10.1177/1090198104263660. [DOI] [PubMed] [Google Scholar]
- 12.Springer AE, Kelder S, Hoelscher DM. Social support, physical activity, and sedentary behavior among 6th grade girls: a cross sectional study. Int J Behav Nutr Phys Act. 2006;3:8. doi: 10.1186/1479-5868-3-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Beets MW, Cardinal BJ, Alderman BL. Parental social support and the physical activity-related behaviors of youth: a review. Health Educ Res. 2010;37:621–644. doi: 10.1177/1090198110363884. [DOI] [PubMed] [Google Scholar]
- 14.Duncan SC, Duncan TE, Strycker LA. Sources and types of social support in youth physical activity. Health Psychol. 2005;24(1):3–10. doi: 10.1037/0278-6133.24.1.3. [DOI] [PubMed] [Google Scholar]
- 15.Jago R, Brockman R, Fox KR, Cartwright K, Page AS, Thompson JL. Friendship groups and physical activity: qualitative findings on how physical activity is initiated and maintained among 10–11 year old children. Int J Behav Nutr Phys Act. 2009;6:4–12. doi: 10.1186/1479-5868-6-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Salvy S, Bowker J, Roemmich JN, et al. Peer influence on children’s physical activity: an experience sampling study. J Pediatr Psychol. 2008;33(1):39–49. doi: 10.1093/jpepsy/jsm039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.De la Haye K, Robins G, Mohr P, Wilson C. How physical activity shapes, and is shaped by, adolescent friendships. Soc Sci Med. 2011;73:719–728. doi: 10.1016/j.socscimed.2011.06.023. [DOI] [PubMed] [Google Scholar]
- 18.Salvy S, de la Haye K, Bowker JC, Hermans RCJ. Influence of peers and friends on children’s and adolescents’ eating and activity behaviors. Physiol Behav. 2012;106:369–378. doi: 10.1016/j.physbeh.2012.03.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ali MM, Amialchuk A, Heiland FW. Weight-related behavior among adolescents: the role of peer effects. PLoS One. 2011;6(6):e21179. doi: 10.1371/journal.pone.0021179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sirard JR, Bruening M, Wall MM, Eisenberg ME, Sun K, Neumark-Sztainer D. Physical activity and screen time in adolescents and their friends. Am J Prev Med. 2013;44(1):48–55. doi: 10.1016/j.amepre.2012.09.054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Craggs C, Corder K, Van Sluijis EMF, Griffin SJ. Determinants of change in physical activity in children and adolescents. Am J Prev Med. 2011;40(6):645–658. doi: 10.1016/j.amepre.2011.02.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Neumark-Sztainer D, Story M, Hannon PJ, Thorp T, Rex J. Factors associated with changes in physical activity: a cohort study of inactive adolescent girls. Arch Pediatr Adolesc Med. 2003;157(8):803–810. doi: 10.1001/archpedi.157.8.803. [DOI] [PubMed] [Google Scholar]
- 23.Strauss RS, Rodzilsky D, Burack G, Colin M. Psychosocial correlates of physical activity in healthy children. Arch Pediatr Adolesc Med. 2001;155(8):897–902. doi: 10.1001/archpedi.155.8.897. [DOI] [PubMed] [Google Scholar]
- 24.Bergh IH, Grydeland M, Bjelland M, et al. Personal and social-environmental correlates of objectively measured physical activity in Norwegian pre-adolescent children. Scand J Med Sci Sports. 2011;21:315–324. doi: 10.1111/j.1600-0838.2011.01295.x. [DOI] [PubMed] [Google Scholar]
- 25.Baker CW, Little TD, Brownell KD. Predicting adolescent eating and activity behaviors: the role of social norms and personal agency. Health Psychol. 2003;22(2):189–198. doi: 10.1037/0278-6133.22.2.189. [DOI] [PubMed] [Google Scholar]
- 26.Voorhees CC, Murray D, Welk G, et al. The role of peer social network factors and physical activity in adolescent girls. Am J Health Behav. 2005;29(2):183–190. doi: 10.5993/AJHB.29.2.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Neumark-Sztainer D, Wall M, Larson N, et al. Secular trends in weight status and weight-related attitudes and behaviors in adolescents from 1999 to 2010. Prev Med. 2012;54(1):77–81. doi: 10.1016/j.ypmed.2011.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Godin G, Shephard RL. A simple method to assess exercise behavior in the community. Can J Appl Sport Sci. 1985;10(3):141–146. [PubMed] [Google Scholar]
- 29.Miller DJ, Freedson PS, Kline GM. Comparison of activity levels using the Caltrac accelerometer and five questionnaires. Med Sci Sports Exerc. 1994;26(3):376–382. doi: 10.1249/00005768-199403000-00016. [DOI] [PubMed] [Google Scholar]
- 30.Jacobs DR, Ainsworth BE, Hartman TJ, Leon AS. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med Sci Sports Exerc. 1993;25:81–91. doi: 10.1249/00005768-199301000-00012. [DOI] [PubMed] [Google Scholar]
- 31.Sallis JF, Buono MJ, Roby J, Micale FG, Nelson JA. Seven-day recall and other physical activity self-reports in children and adolescents. Med Sci Sports Exerc. 1993;25(1):99–108. doi: 10.1249/00005768-199301000-00014. [DOI] [PubMed] [Google Scholar]
- 32.Motl RW, Dishman RK, Trost SG, et al. Factorial validity and invariance of questionnaires measuring social-cognitive determinants of physical activity among girls. Prev Med. 2000;31(5):584–594. doi: 10.1006/pmed.2000.0735. [DOI] [PubMed] [Google Scholar]
- 33.Motl RW, Dishman RK, Saunders R, Dowda M, Felton G, Pate RR. Measuring enjoyment of physical activity in adolescent girls. Am J Prev Med. 2001;21(2):110–117. doi: 10.1016/S0749-3797(01)00326-9. [DOI] [PubMed] [Google Scholar]
- 34.Dishman RK, Motl LR, Sallis JF, et al. Self-management strategies mediate self-efficacy and physical activity. Am J Prev Med. 2005;29(1):10–18. doi: 10.1016/j.amepre.2005.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Davison KK. Activity-related support from parents, peers, and siblings and adolescents’ physical activity: are there gender differences? J Phys Act Health. 2004;1:363–376. [Google Scholar]
- 36.Heitzler CD, Lytle LA, Erickson DJ, Barr-Anderson D, Sirard JR, Story M. Evaluating a model of youth physical activity. Am J Health Behav. 2010;34(5):593–606. doi: 10.5993/AJHB.34.5.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.McDonald RP, Ho MR. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7(1):64–82. doi: 10.1037/1082-989X.7.1.64. [DOI] [PubMed] [Google Scholar]
- 38.Kline RB. Principles and Practice of Structural Equation Modeling. New York: Guilford Press; 2005. [Google Scholar]
- 39.Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: review and update. Med Sci Sports Exerc. 2002;34(12):1996–2001. doi: 10.1097/00005768-200212000-00020. [DOI] [PubMed] [Google Scholar]
- 40.Bauer KW, Nelson MC, Boutelle KN, Neumark-Stzainer D. Parental influences on adolescents’ physical activity and sedentary behavior: longitudinal findings from Project EAT-II. Int J Behav Nutr Phys Act. 2008;5:12. doi: 10.1186/1479-5868-5-12. [DOI] [PMC free article] [PubMed] [Google Scholar]