

Sir,
Patients with thyroid swelling can present as an anticipated difficult airway either in the form of difficult mask ventilation or intubation.[1] Careful preoperative airway evaluation in the form of clinical and radiological assessment is essential to formulate a safe anaesthetic plan.[2] We discuss here the use of dynamic airway assessment by ultrasonography (USG)[3] in deciding an acceptable and risk-free anaesthetic technique rather than static radiological airway imaging such as X-ray soft-tissue neck and non-contrast computed tomography (CT).
A 51-year-old female presented with a 10 cm × 7 cm cystic ovarian mass arising from her right ovary. There was a history of swelling in front of the neck for the past 7 years which was gradually progressing in size. She did not give any history of breathlessness or stridor at rest but complained of difficulty in breathing during activity. She had undergone left hemithyroidectomy for colloid goitre 27 years back. Clinical examination revealed that the appearance of noisy breathing when thyroid swelling was manipulated in sitting and supine position. The patient had difficulty in breathing when the thyroid swelling was palpated to evaluate its consistency but was relieved when the swelling was moved to right side. The thyroid swelling of size 8 cm × 7 cm was mobile and cervical trachea was deviated to the left side with tracheal cartilages palpable lateral to the thyroid swelling. General physical and systemic evaluation revealed no other abnormality except for the distended abdomen. Biopsy from the swelling present on the front of the neck revealed features of colloid goitre. She was posted for staging laparotomy for ovarian mass, followed by completion thyroidectomy at a later date. Airway examination revealed adequate mouth opening with modified Mallampatti class 2 with good neck extension and subluxation was 1+. Soft-tissue neck anteroposterior view in radiography [Figure 1a] showed a grossly deviated trachea towards left side with narrowing at the level of C7, 8. This was confirmed by CT of neck and thorax. The tracheal narrowing started at a distance of 2.5 cm from the vocal cord, and the narrowest diameter was noted at 5 cm from the cord. The narrowest part was located at a distance of 3 cm above the carina [Figure 1b]. Indirect laryngoscopy revealed bilateral mobile vocal cords with adequate glottis aperture. Ultrasound of the neck was performed using SEIMENS ACVSON S3000 ultrasound machine with the patient in supine position. The suprasternal acoustic window was chosen to keep the trachea and left internal carotid artery in the centre as the area of interest. Linear probe 16 MHz was chosen with a depth of 4 cm, diameter of the trachea at the level of narrowing was measured and noted as a baseline value [Figure 1c]. Then, the thyroid swelling was manually displaced to the right side of the neck keeping the linear probe over the same area as before visualising the expansion of trachea. The diameter of the trachea after manual displacement of the thyroid swelling was noted [Video 1] and the difference was found to be 3 mm expansion [Figure 1d]. In accordance with the recent S1 Guidelines on airway management by the German Society of Anaesthesiology and Intensive Care[4] we opted for combined spinal and epidural technique for total abdominal hysterectomy and the surgical procedure was successfully completed under regional anaesthesia without any active airway intervention. Nevertheless, difficult airway cart along with rigid bronchoscope was kept ready, and an ENT surgeon was alerted and was available in the operating room. The static images obtained by CT scan provide useful information about the extent, narrowing and displacement. However, the dynamic changes that can be induced in the airway while manipulating the swelling can only be evident with the use of ultrasound. We could visualise with the help of the ultrasound how the tracheal compression could be relieved by pushing the swelling to the right. This reassured us of the ability to maintain oxygenation and ventilation during surgery. Pre-operative assessment with ultrasound made in combination with X-ray and CT scan can provide useful information and help in better decision-making for airway management.
Figure 1.
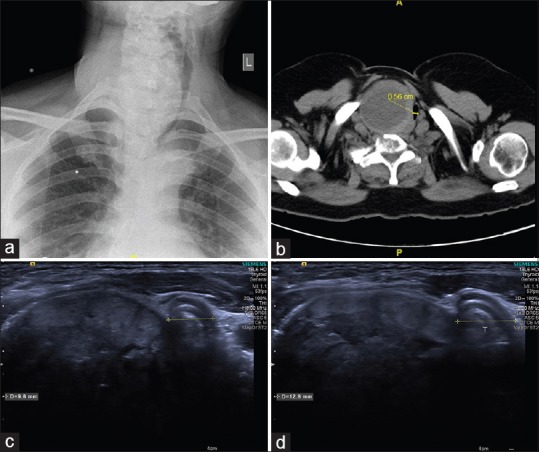
Dynamic airway evaluation
The position of the trachea in relation to the neck mass in CT scan image should be used to make a decision whether the mass should be lifted up or pushed to the side. Standard recommended technique of lifting up of the thyroid mass may not be always appropriate except if the trachea is posterior to the mass.[5] Pushing the mass to the opposite side if the trachea is displaced to the side can help to open up the compressed airway and improve airway patency as in our case. Airway ultrasound demonstrated that the narrowing of the trachea is not fixed, and the trachea can expand when the thyroid mass is pushed away. We recommend the preoperative use of neck ultrasound in combination with X-ray neck and CT scan to evaluate compression and displacement of the cervical trachea in patients with neck mass or thyroid enlargement.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video Available on: www.ijaweb.org
REFERENCES
- 1.Voyagis GS, Kyriakos KP. The effect of goiter on endotracheal intubation. Anesth Analg. 1997;84:611–2. doi: 10.1097/00000539-199703000-00027. [DOI] [PubMed] [Google Scholar]
- 2.Shaha AR, Burnett C, Alfonso A, Jaffe BM. Goiters and airway problems. Am J Surg. 1989;158:378–80. doi: 10.1016/0002-9610(89)90137-2. [DOI] [PubMed] [Google Scholar]
- 3.Parmar SB, Mehta HK, Shah NK, Parikh SN, Solanki KG. Ultrasound: A novel tool for airway imaging. J Emerg Trauma Shock. 2014;7:155–9. doi: 10.4103/0974-2700.136849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Piepho T, Cavus E, Noppens R, Byhahn C, Dörges V, Zwissler B, et al. S1 guidelines on airway management: Guideline of the German society of anesthesiology and intensive care medicine. Anaesthesist. 2015;64(Suppl 1):27–40. doi: 10.1007/s00101-015-0109-4. [DOI] [PubMed] [Google Scholar]
- 5.Memon M, Ashraf M. Antigravity lift technique is helpful in difficult intubation in patients with large goiters. Anaesth Pain Intensive Care. 2009;13:78–80. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.