

Abstract
Case summary
Cranial ventral midline hernias, most often congenital, can be associated with other congenital abnormalities, such as sternal, diaphragmatic or cardiac malformations. A 4-year-old multiparous queen with a substernal hernia was admitted for evaluation of a mammary mass. During CT examination, a bifid sternum, the abdominal hernia containing the intestines, spleen, omentum, three fetuses, a mammary mass and an incidental peritoneopericardial diaphragmatic hernia were identified. Surgery consisted of a standard ovariohysterectomy and repair of the peritoneopericardial hernia. Primary closure of the abdominal hernia was attempted but deemed impossible even after the ovariohysterectomy, splenectomy and a partial omentectomy. An external abdominal oblique muscle flap was used to close with no tension on the cranial part of the hernia. One month postoperatively, the queen had no respiratory abnormalities and the herniorrhaphy was fully healed.
Relevance and novel information
This case is the first description of a 4-year-old multiparous pregnant queen with complex congenital malformations and surgical correction of a peritoneopericardial hernia and a 6 × 8 cmsubsternal hernia with an external abdominal oblique muscle flap. Life-threatening sequelae associated with large abdominal hernias can be attributed to space-occupying effects known as loss of domain and compartment syndrome, which is why a muscle flap was used in this case. The sternal cleft was not repaired because of the size of the cleft and the age of the cat.
Introduction
Cranial ventral midline hernias are most often congenital in origin and include umbilical hernias and substernal hernias. They are classically diagnosed at a few months of age in puppies and kittens and reconstructed, if amenable, early to prevent complications, such as organ incarceration/strangulation or compartment syndrome. These hernias can be associated with other congenital abnormalities such as sternal, diaphragmatic or cardiac malformations. To our knowledge, this is the first report of surgical treatment with an external oblique abdominal muscle flap of an 6 × 8 cm congenital cranial ventral abdominal hernia in a 4-year-old multiparous pregnant queen.
Case description
A 4-year-old intact queen was admitted for evaluation of a slowly growing subcutaneous mass noticed 3 weeks earlier between the third and the fourth left mammary gland. Since birth, a substernal mass was present, which was diagnosed as a substernal hernia. Owing to the size of the defect and the absence of clinical impact, no surgical attempt was made to reconstruct the defect at that time. Despite being under oral contraception, the cat had already had three litters of two kittens with only one alive each time. The parturition went naturally each time with no evident dystocia.
At physical examination, there was a left heart murmur (grade III/VI), a sternal cleft, an 6 × 8 cm substernal ventral hernia and a 5 cm firm subcutaneous mass between the third and the fourth left mammary glands (Figure 1). The abdominal hernia was reducible. Results of complete blood count and serum biochemistry were unremarkable.
Figure 1.
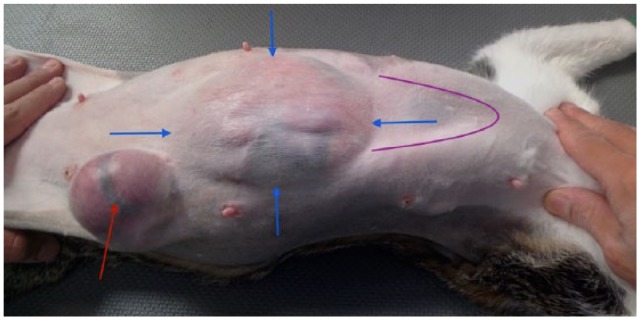
Visualisation of the abnormalities. Red arrow: 4 cm subcutaneous mass; blue arrows: delineation of the supra-umbilical abdominal hernia; violet line: delineation of the sternal cleft (head on the right)
An abdominal ultrasound was performed, which revealed a subcutaneous mass filled with an echoic content (cytologically inflammatory and haemorrhagic). This mass did not communicate with either the abdominal cavity or the hernia. During the examination, the queen was found to be pregnant with three immature fetuses. Echocardiography revealed no major abnormalities. A CT scan was performed to provide further evaluation of the congenital malformations; the sternal cleft was complete from the third to the last sternebrae (bifid sternum) (Figure 2) and hernia contents included intestines, spleen and omentum (Figure 3). The CT scan confirmed the number of fetuses (Figure 4) and the mass with no evidence of metastatic disease. A peritoneopericardial diaphragmatic hernia (PPDH) with fat content was found incidentally (Figure 5).
Figure 2.

Bifid sternum (three-dimensional reconstruction). Note the complete absence of fusion of the sternebrae from the third sternebrae until the last one
Figure 3.
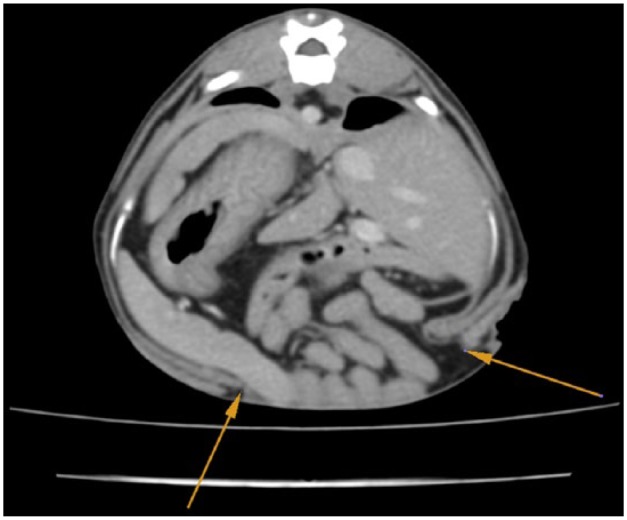
CT scan, sagittal view. Visualisation of the abdominal hernia. The two arrows indicate the borders of the hernia in a sagittal view. The spleen, intestines and some omentum are seen within the hernia
Figure 4.
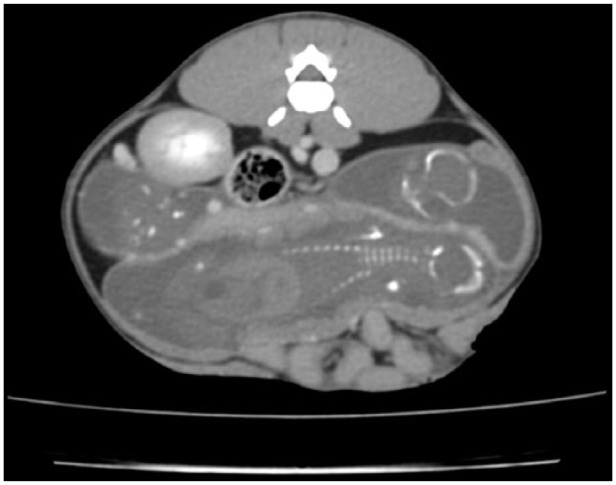
CT scan, sagittal view. Visualisation of the three fetal skeletons. The abdominal hernia is seen
Figure 5.
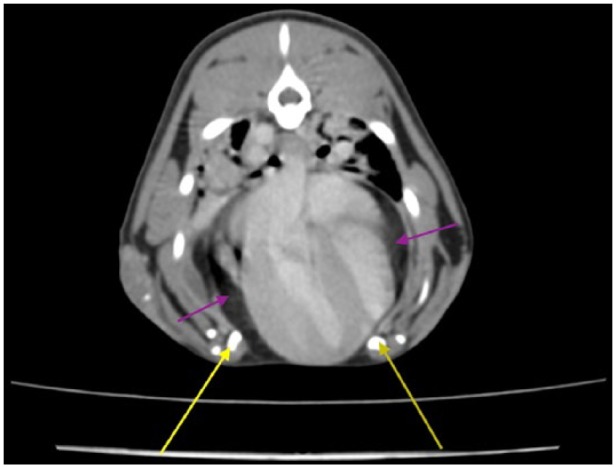
CT scan, sagittal view. The two halves of the bifid sternum are seen (yellow arrows). The peritoneopericardial hernia is seen on this view with a fat content around the heart in a distended pericardium (purple arrows)
The cat was preoxygenated with 100% O2 and induced with midazolam (Midazolam Mylan 1 mg/ml; Mylan [0.2 mg/kg IV]) and propofol (Propolipid 1%; Fresenius Kabi [1 mg/kg IV]). Anaesthesia was maintained with isoflurane (VetFlurane; Virbac) and oxygen at 100% and pain was controlled with a constant rate infusion of fentanyl (Fentanyl 50 μg/ml; Laboratoire Renaudin [2–4 μg/kg/h]). The cat was positioned in dorsal recumbency. A skin incision was started over the abdominal hernia on the midline: this permitted the opening of the hernial sac which was adherent to the skin. A midline laparotomy was performed and a standard ovariohysterectomy was performed. The PPDH was identified (Figure 6) and contained a part of the omentum. Reduction and closure of the PPDH with a continuous suture to the abdominal musculature (Biosyn, 2-0, Taper needle; Covidien) was performed without disruption of the pericardial diaphragmatic junction. Primary closure of the large abdominal wall defect due to the abdominal hernia was impossible owing to its size and chronicity (4 years’ duration). A splenectomy and a partial omentectomy were performed with a bipolar vessel sealing device (LigaSure, small jaw instrument; Covidien) in order to decrease the volume of the abdominal content. Primary closure was still not possible, particularly at the level of the retrocostal part of the defect. An external abdominal oblique muscle flap was then elevated from its vascular pedicle on the right side (Figure 7) to close the retrocostal part. The right flap was rotated 90° medially and sutured with cruciate interrupted pattern 2-0 (Biosyn, Taper needle; Covidien) on the left abdominal wall (Figure 8). Caudally, the hernia was closed primarily. The subcutaneous mass was removed with marginal margins and was followed by routine closure of subcutis and skin. A subcutaneous suction drain was placed to prevent accumulation of fluid and was left in place until discharge (3 days).
Figure 6.
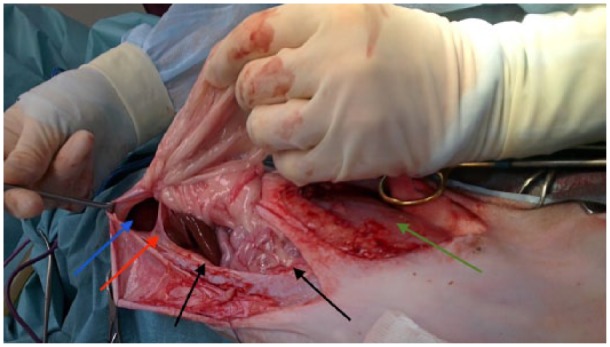
Repair of the peritoneopericardial hernia. Blue arrow: peritoneopericardial hernia with apex of the heart visible; red arrow: diaphragm; black arrow: abdominal hernia; green arrow: incision for the removal of the mammary mass (head on the left)
Figure 7.
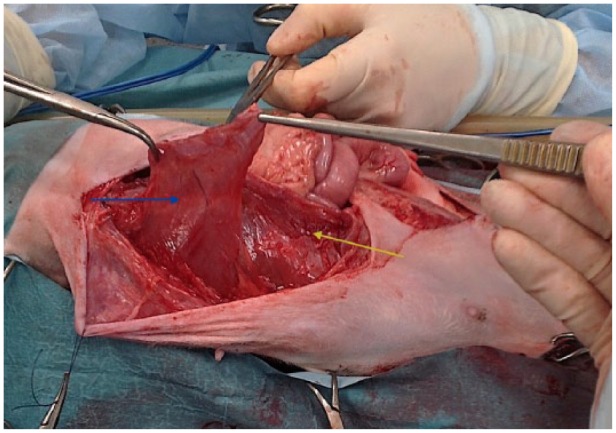
Elevation of the external abdominal oblique flap. Blue arrow: flap; yellow arrow: abdominal wall
Figure 8.
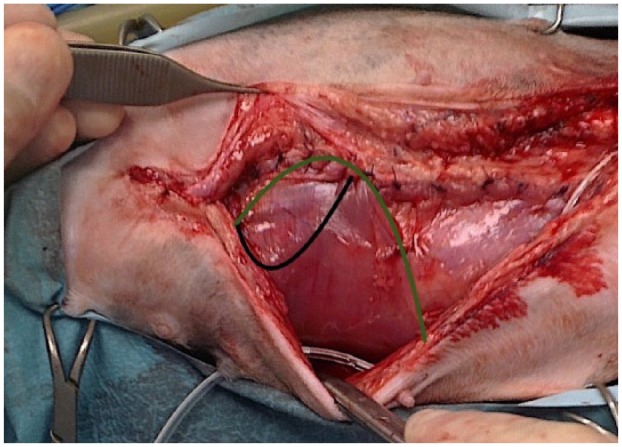
Final reconstruction of the abdominal wall. Green line: flap in place sutured to the left side of the abdominal wall and caudally to the abdominal wall itself. Black line: delineation of the retrocostal defect
The queen recovered well with no clinical abnormalities. Healing was uneventful and clinical examination was normal (except for a persistent grade III/VI heart murmur) at the 15 day follow-up. Pathological examination of the mass revealed fibroadenomatous hyperplasia. One month postoperatively, the queen was doing well, had no respiratory abnormalities and the herniorrhaphy was fully healed with no signs of recurrence. The sternal cleft was left unrepaired at that time owing to the inherent risks of such a surgery in a 4-year-old cat.
Discussion
Cranial ventral midline hernias are most often congenital and include umbilical hernias and substernal (or ventral) hernias. Congenital cranioventral abdominal hernias, incomplete caudal sternal fusion (sternal cleft) and umbilical defects with concomitant diaphragmatic hernias of various types have been observed in dogs.1 PDDHs are a common congenital anomaly in dogs and cats. Organs that frequently herniate into the pericardial sac include the liver, falciform ligament, omentum, spleen, small intestines and, rarely, stomach.1 PPDHs may occur with other congenital abnormalities, as in our case, including sternal defects, cranial midline abdominal wall hernia, umbilical hernia and cardiac defects. Sternal clefts result from a failure of midline fusion of sternal bars, which occurs progressively from cranial to caudal. A bifid sternum, such as in our case, is clinically important because it leaves the heart and great vessels unprotected. Attempts to repair the anomaly are typically performed as early as possible.2 Combinations of congenital abnormalities occur only sporadically in dogs, cats and humans.1–3
Severe, often life-threatening, sequelae associated with abdominal hernias can be attributed to space-occupying effects such as loss of domain, incarceration or obstruction, or strangulation. Loss of domain occurs when the abdominal wall has become accustomed to a relatively small intra-abdominal volume because of organ displacement outside the cavity (usually through a large defect, as in our case), particularly when the hernia becomes chronic. Manual reduction of hernia contents and primary closure of the defect is difficult or impossible in this situation. Repair of the restricted abdominal wall by forcing herniated contents back into the abdomen results in excessive tension on the repair, increasing the risk of recurrence. Even more deleterious risks include acute pulmonary complications, secondary to restriction of diaphragm function, and poor organ perfusion (abdominal compartment syndrome).1 Therefore, to restore the integrity of the abdominal wall, large defects, as in our case, or in cases of suspected loss of domain, are usually repaired either with autologous or non-autologous options.1 It is also possible to consider the removal of non-vital organs to gain some space, such as the spleen or part of the omentum. In fact, the risk of fatal and debilitating infection after splenectomy is far less common in cats and dogs than in humans.4
Using the patient’s own tissue (autologous) is preferable to the non-autologous method for most hernias. It offers the advantage of providing dynamic and vascular support (particularly in a contaminated environment or in a previously irradiated area). Non-autologous methods are often preferred for reconstruction after tumour resection and for hernia when primary closure is not possible. Indeed, non-autologous methods increase abdominal wall elastic properties, allow tension-free solution repair and reduce hernia recurrence and postoperative complications related to loss of domain. Use of mesh is usually more simple and results in less donor site morbidity. However, complications include infection, fistula formation and skin erosion, which lead to a high rate of removal in human studies.5 An autologous option was chosen in this case.
Different autologous repair methods are used, such as separation of anatomic components, abdominal wall partitioning and muscle flaps.1 Skeletal muscle can be freed and mobilised to repair defects beneath the skin of the abdomen, particularly in chronic large hernias, as in our case.6 However, muscle transposition to a defect is limited to the region of the selected muscle and the length of the vascular pedicle. Vascularised muscle flaps should be of a size and shape that will allow it to cover the defect without bulkiness or excess tension. The location of its vascular supply should be consistent and resistant to superficial trauma. The flap should be readily accessible and transposition should not result in significant loss of function. In the veterinary literature, two flaps have been described that meet these requirements for abdominal wall hernia closure: the cranial sartorius and the external abdominal oblique muscles.1,6 The latissimus dorsi is usually used to cover thoracic defects, but it can be used in selected ventral or lateral regions of the cranial abdomen.7 The cranial sartorius muscle flap covers the caudal 30% of the abdomen or about 80% of the length between the pubis and ribs on the ipsilateral side.8
The external abdominal oblique muscle consists of two components: the costal part originates segmentally from the fourth or fifth rib through the thirteenth rib, whereas the lumbar part originates in the thoracolumbar fascia along the iliocostalis muscle.9 The external abdominal oblique muscle flap, a myofascial island flap based on the lumbar component, has been described for use in abdominal wall reconstruction.10 The cranial branch of the cranial abdominal artery supplies the middle zone of the lateral abdominal wall and is accompanied by the cranial hypogastric nerve and satellite vein (Figure 9).10 This flap can be used for treatment of ventral, cranial to mid abdominal wall defects along its arc of rotation such as subcostal hernia.
Figure 9.

External abdominal oblique myofascial island flap. (a) Location of the lumbar component of the muscle. (b) Three edges of the flap are severed and reflected to show location of the neuromuscular pedicle (from Alexander et al10)
Complications of general hernia repair are of three kinds: preoperative, early postoperative and late postoperative.11 Perioperative complications are anaesthesia complications, haemorrhage, visceral injury, ‘loss of domain’ and poor tissue strength at hernia margins. Early postoperative complications include seroma, haematoma, wound dehiscence and pain; and late postoperative complications include the formation of tracts and recurrence.
The mammary mass was a benign lesion possibly due to long-term administration of synthetic progestins as oral contraception.12 The concurrent gestation with progesterone administration may have increased its risk of formation.12
Finally, the sternal cleft was not repaired during the same surgery because of the size of the cleft and the age of the cat. In humans, the hypoplastic nature of the sternal bars, the width of the cleft or advanced age of the patient sometimes preclude primary repair,13 and prosthetic materials are used to bridge the gap.14 The queen in this case is adult and the thorax is inevitably much less flexible. Primary closure of the sternum, such as described in the study of Schwarzkopf et al (2-month-old kitten), would be difficult to impossible, particularly primarily in such a case.3 Cardiovascular and pulmonary consequences would be expected. As the queen is 4 years old and has been asymptomatic to date, it was decided to choose a conservative approach.
Conclusions
This case is the first description of a 4-year-old multiparous pregnant queen with a sternal cleft and surgical correction of a PPDH and a 6 × 9 cm substernal hernia, and mammary mass removal. Despite the removal of the three fetuses, the spleen and part of the omentum, surgical correction of the abdominal hernia necessitated an external oblique abdominal muscle flap and was uneventful. Because of the age of the queen and the size of the sternal cleft, a conservative approach was elected.
Footnotes
Conflict of interest: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Accepted: 18 November 2017
References
- 1. Smeak DD. Abdominal wall reconstruction and hernias. In: Tobias KM, Johnston SA. (eds). Veterinary surgery: small animal. St Louis, MO: Saunders Elsevier, 2012, pp 1353–1379. [Google Scholar]
- 2. Benlloch-Gonzalez M, Poncet C. Sternal cleft associated with Cantrell’s pentalogy in a German shepherd dog. J Am Anim Hosp Assoc 2015; 51: 279–284. [DOI] [PubMed] [Google Scholar]
- 3. Schwarzkopf I, Bavegems VC, Vandekerckhove PM, et al. Surgical repair of a congenital sternal cleft in a cat. Vet Surg 2014; 43: 623–629. [DOI] [PubMed] [Google Scholar]
- 4. Pachter HL, Guth AA, Hofstetter SR. Changing patterns in the management of splenic trauma: the impact of nonoperative management. Ann Surg 1998; 227: 708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Grevious MA, Cohen M, Jean-Pierre F, et al. The use of prosthetics in abdominal wall reconstruction. Clin Plast Surg 2006; 33: 181. [DOI] [PubMed] [Google Scholar]
- 6. Feng YC, Chen KS, Chang SC. Reconstruction with latissimus dorsi, external abdominal oblique and cranial sartorius muscle flaps for a large defect of abdominal wall in a dog after surgical removal of infiltrative lipoma. J Vet Med Sci 2016; 78: 1717–1721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Pavletic MM. Introduction to myocutaneous and muscle flaps. Vet Clin North Am Small Anim Pract 1990; 20: 127–146. [DOI] [PubMed] [Google Scholar]
- 8. Sylvestre AM, Weinstein MJ, Popovitch CA, et al. The sartorius muscle flap in the cat: an anatomic study and two case reports. J Am Anim Hosp Assoc 1997; 33: 91–96. [DOI] [PubMed] [Google Scholar]
- 9. Howard EE, Alexander de L. The skeletal and muscular systems. In: Howard EE, Alexander de L. (eds). Guide to the dissection of the dog. 7th ed. Philadelphia, PA: Saunders, 2010, pp 6–92. [Google Scholar]
- 10. Alexander LG, Pavletic MM, Engler SJ. Abdominal wall reconstruction with a vascular external abdominal oblique myofascial flap. Vet Surg 1991; 20: 379–384. [DOI] [PubMed] [Google Scholar]
- 11. Smeak DD. Management and prevention of surgical complications associated with small animal abdominal herniorraphy: gastrointestinal surgical complications. Probl Vet Med 1989; 1: 254. [PubMed] [Google Scholar]
- 12. Van Nimwegen S, Kirpensteijn J. Specific disorders. In: Tobias KM, Johnston SA. (eds). Veterinary surgery: small animal. St Louis, MO: Saunders Elsevier, 2012, pp 1325–1326. [Google Scholar]
- 13. Snyder BJ, Robbins RC, Ramos D. Primary repair of complete sternal cleft with pectoralis major muscle flaps. Ann Thorac Surg 1996; 61: 983–984. [DOI] [PubMed] [Google Scholar]
- 14. Abel RM, Robinson M, Gibbons P, et al. Cleft sternum: case report and literature review. Pediatr Pumonol 2004; 37: 375– 377. [DOI] [PubMed] [Google Scholar]