

Abstract
The rationale of diabetes related fatigue syndrome and interventions.

Frequent complaint of fatigue from people with chronic conditions is a strong predictor for functional limitations, disability, increasing mortality and other adverse outcomes. With a high prevalence of diabetes in older people worldwide, fatigue symptoms, including frailty, muscle weakness, impaired mobility, functional limitation and loss of independence, are usually complained of. Fatigue symptoms accompanied by the complications of neuromuscular dysfunction as a result of poor glycemic control, cardiovascular disease or peripheral vascular deficit are commonly shown by people with diabetes1. Evidence has shown that diabetes risk factors are related to fatigue symptoms, such as nutrition imbalance, and neuromuscular complications contributing to muscle frailty and sarcopenia1. Vitamin D deficency is common in people with diabetes, and low vitamin D status is associated with a reduced health‐related quality of life, fatigue and depressive symptoms2. Diabetes‐related fatigue can lead to frailty, including self‐reported exhaustion, low physical activity, slow walk speed, low grip strength and weight loss, which will increase the risk of falls3.
However, fatigue is a subjective symptom, lacking measurable concrete signs. Fatigue can be divided into two types. In central fatigue, an exercise‐induced increase in extracellular serotonin concentrations in several brain regions contributes to the development of fatigue during prolonged exercise. Muscle weakness and tiredness are manifested in the early stage. Peripheral fatigue consists of the inability to sustain a specified force in physical activity or loss of endurance in mental tasks, such as shifting from a sitting to a standing position, lifting a heavy bag, as well as the feeling of worthlessness or distress. The lost of muscle bulk and powerlessness can be present early for these patients3.
Diabetes‐related fatigue can result from three factors: (i) physiological factors, as a result of acute or chronic hypo‐ or hyperglycemia, the variability of blood glucose and diabetes symptom distress; (ii) psychological factors, such as depression or emotional distress related to the diagnosis or progress of diabetes, sleep disturbance and restless legs syndrome; and (iii) lifestyle factors, for example, sedentary behavior, weight control issue or obese sarcopenia3. The severity of fatigue symptoms is influenced by a variety of physical and pathological indicators. These etiologies contribute to physical limitation and loss of functional independence. The decrease of muscle strength and quality leads to muscle fatigue and a consequent reduction in work capacity2. Long‐term and chronic fatigue will cause the inability to carry out diabetes self‐care, physical disability, emotional distress and insomnia3.
Furthermore, aging can result in progressive inactivity, decreased mobility, slow gait and loss of muscle mass, especially in the lower extremities. Diabetes will accelerate the reduction of muscle mass and strength as a result of poor glycemic control, complications of neuropathy or vasculopathy, overweight/obesity, insulin resistance, inflammatory cytokines, and endocrine changes, all associated with the adverse effects on premature loss of muscle and normal function3.
The skeletal muscle is the largest insulin‐sensitive tissue in the body, so decreased muscle mass will increase the risk of insulin resistance. Furthermore, poor lifestyle, such as physical inactivity or sedentary behavior, leads to an accumulation of fat tissue in the body, especially around the abdomen. Intermuscular fat can also reduce blood flow to muscle and increase the inflammatory process for people with diabetes2.
Research in the Japanese community showed that the odds ratio for falls in the sarcopenia group was 4.42 (95% confidence interval 2.08–9.39) in men and 2.34 (95% confidence interval 1.39–3.94) in women4. Furthermore, people with diabetes had a threefold higher risk of sarcopenia (odds ratio 3.06, 95% confidence interval 1.42–6.62) than those without diabetes5. Screening for sarcopenia has been recommended by the European, International and Asian Working group on Sarcopenia6.
Though fatigue is a subjective feeling, it can be evaluated by an in‐depth interview. In addition, some tools, such as the Avlund Fatigue Scales, the 36‐item Short Form Health Survey for quality of life and sleep quality scales (such as Pittsburgh Sleeping Quality Index), have also been used to evaluate the fatigue related with sleep disturbance. The Multidimensional Fatigue Inventory has been suggested to screen fatigue status with reliable validity7. Screening the early signs of fatigue can be integrated into complications screening for diabetes mellitus annually.
Anti‐fatigue training strategies should include physical activity and nutritional management. Practice guidelines consistently recommend that people with diabetes obtain at least 150 min of moderate‐to‐vigorous aerobic exercise per week. The resistance training is beneficial and a small amount of physical activity is better than no activity; health outcomes are highly correlated with the quality and amount of physical activity the patients engage in8. It has been suggested that essential amino acids and carbohydrate mixture nutrition, and vitamin D supplements be taken after resistance exercise, but they did not further increase muscle protein synthesis during post‐exercise for fatigue recovery8.
In summary, fatigue is a common problem for people with diabetes, especially in elderly patients. Therefore, we generated the rationale and interventions for prevention of diabetes‐related fatigue in Figure 1. Early detection and management will improve the quality of life and diabetes control. Annual screening of fatigue, integrated with the screening for diabetic complications, might become a more complete program for future diabetes care.
Figure 1.
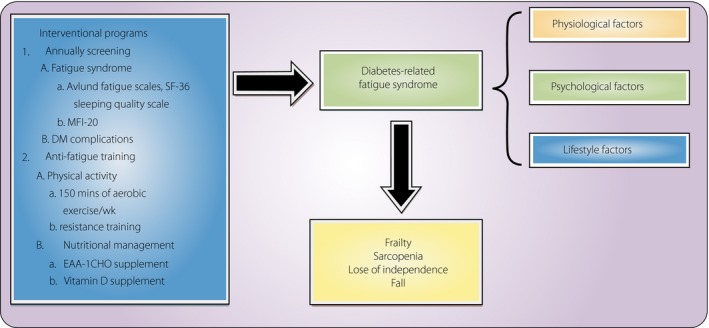
The rationale of diabetes‐related fatigue syndrome and interventions. Fatigue caused by physiological, psychological or lifestyle factors will lead to frailty, sarcopenia and falls. Annual screening and anti‐fatigue training can be introduced in the early stage. DM, diabetes mellitus; EAA‐1CHO, essential amino acids and carbohydrate; MFI‐20, Multidimensional Fatigue Inventory; SF‐36, 36‐item Short Form Health Survey.
Disclosure
The authors declare no conflict of interest.
References
- 1. Bianchi L, Volpato S. Muscle dysfunction in type 2 diabetes: a major threat to patient's mobility and independence. Acta Diabetol 2016; 53: 879–889. [DOI] [PubMed] [Google Scholar]
- 2. Ozfirat Z, Chowdhury TA. Vitamin D deficiency and type 2 diabetes. Postgrad Med J 2010; 86: 18–25. quiz 24. [DOI] [PubMed] [Google Scholar]
- 3. Cobo A, Vázquez LA, Reviriego J, et al Impact of frailty in older patients with diabetes mellitus: an overview. Endocrinol Nutr 2016; 63: 291–303. [DOI] [PubMed] [Google Scholar]
- 4. Tanimoto Y, Watanabe M, Sun W, et al Sarcopenia and falls in community‐dwelling elderly subjects in Japan: defining sarcopenia according to criteria of the European Working Group on Sarcopenia in Older People. Arch Gerontol Geriatr 2014; 59: 295–299. [DOI] [PubMed] [Google Scholar]
- 5. Kim J, Park Y. Low muscle mass is associated with metabolic syndrome in Korean adolescents: the Korea National Health and Nutrition Examination Survey 2009‐2011. Nutr Res 2016; 36: 1423–1428. [DOI] [PubMed] [Google Scholar]
- 6. Chen L, Lee W, Peng L, et al Recent advances in sarcopenia research in Asia: 2016 update from the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 2016; 17: 767. e1‐7 [DOI] [PubMed] [Google Scholar]
- 7. Avlund K. Fatigue in older adults: an early indicator of the aging process? Aging Clin Exp Res 2010; 22: 100–115. [DOI] [PubMed] [Google Scholar]
- 8. Makanae Y, Fujita S. Role of Exercise and Nutrition in the Prevention of Sarcopenia. J Nutr Sci Vitaminol (Tokyo) 2015; 61(Suppl): S125–S127. [DOI] [PubMed] [Google Scholar]