

Abstract
Introduction:
Surgical extraction of impacted mandibular third molars is often associated with sequelae such as postoperative pain, facial edema, and limitation in mouth opening ability. These sequelae may result in changes in the patients’ lifestyle and quality of life (QoL).
Aim:
The aim of this study was to evaluate the effect of surgical extraction of impacted mandibular third molars on patients’ QoL in the immediate postoperative period (7 days).
Materials and Methods:
Ethical approval for this study was obtained from the Health Research and Ethics committee of the Lagos University Teaching Hospital. A total of 124 individuals with impacted mandibular third molars, who satisfied the inclusion criteria and consented to participate in this study, were included. The Oral Health Impact Profile-14 (OHIP-14) QoL questionnaire was used to assess QoL. QoL was assessed preoperatively (baseline) and on postoperative days (PODs) 1, 3, and 7. Maximal interincisal mouth opening, facial width, and pain were also reviewed at all evaluation points. Data analysis was done using the Statistical Package for Social Sciences (SPSS) for Windows (version 16.0, Chicago, IL, USA).
Results:
A total of 124 individuals were included in the final analysis. An age range of 18–51 years with a mean (±standard deviation) of 28.5 (7.4) years was observed. A male to female ratio of 1:1.5 was observed. The most frequently encountered type of impaction was the mesioangular impaction 51 (41.1%) and recurrent pericoronitis was the principal reason for extraction 53 (42.7%). The severity of the sequelae (pain, trismus, and facial edema) was maximal on the first POD. Patients’ overall QoL deteriorated sharply on the first POD and subsequently improved.
Conclusion:
Surgical extraction of mandibular third molars is associated with worsening of patients’ postoperative QoL in the immediate postoperative period. Prospective patients should be informed about this, and ways of reducing this untoward effect should be explored.
Keywords: Impacted third molar, quality of life, third molar extraction
Introduction
The term “quality of life” was initially utilized primarily in the field of oncology, however as patient management evolved, its application in other fields of healthcare has increased.[1,2] Evaluation of patients’ quality of life (QoL) following oral and maxillofacial surgeries is a relatively recent development.[1,3,4] Impacted third molar extraction is one of the most frequently performed dentoalveolar surgeries.[3,5] It is typically associated with the development of postoperative sequelae such as trismus, postoperative edema and pain.[6,7] Furthermore, complications may result from the procedure.[8,9,10] These sequelae and complications are associated with significant deterioration in patients’ QoL and attendant economic implications.[8,11]
There is paucity of data on the effect of third molar surgery on the postoperative QoL of patients in Sub-Saharan Africa.[2] Especially, data on the specific domains that are affected and the severity of such impairments is scarce.[2] Increasingly, patients wish to be duly informed of the effects of proposed surgical/medical interventions on their total well-being, which includes but is not limited to physical, psychological, and social facets.[3] This study aims to evaluate the effect of third molar surgery on the patients’ postoperative QoL.
Materials and Methods
The study was approved by the Health Ethics Research Committee of Lagos University Teaching Hospital. All individuals were healthy and classified as (American Society of Anesthesiologists Risk Classification I).[12,13] In addition, they were without any form of severe/extensive periodontal disease (American Academy of Periodontology I, II) and they were at least 18 years old. Patients with acute pericoronal infections were excluded. Furthermore, patients with systemic illnesses such as diabetes mellitus, any form of immune-compromise, bleeding diathesis, and dyspepsia were excluded from the study. A written informed consent was obtained from all participants after being duly informed about the procedure and the proposed study.
All surgeries were performed by a single surgeon on outpatient basis, under local anesthesia (2% Lignocaine with 1:100,000 Adrenaline), using the buccal guttering approach. Access was achieved through a 3-sided mucoperiosteal flap after achieving profound local anesthesia by blocking the ipsilateral inferior alveolar, the buccal and the lingual nerves [Figure 1]. Buccal guttering was performed with a fast straight surgical handpiece (80,000–150,000 revs/min) and #10 surgical round headed bur under copious irrigation with normal saline. Following successful extraction of teeth, the bone edges was filed appropriately and the surgical site irrigated copiously with normal saline. The mucoperiosteal flap was reapposed with 3/0 black silk suture.
Figure 1.

Raised mucoperiosteal flap
Preoperatively, the following data were recorded for each subject: Demographics (age, sex), reason for extraction, type of impaction, location of the third molar (left or right), and the degree of impaction. The type of impaction and degree of impaction were assessed with standard periapical radiographs; they were then classified in accordance with the Winter's classification and Pell and Gregory classification.
Postoperatively, all individuals were placed on Caps Ibuprofen, 400 mg 8 h for 3 days; Caps Amoxycillin, 500 mg 8 h for 5 days and Tabs Metronidazole, 400 mg 8 h for 5 days. They were all required to commence the prescribed drug regimen 30 min after the surgical extraction had been concluded.
Pain assessment
Pain assessment was done on 20 min before administration of local anesthesia; then, on PODs 1, 2, 3, 4, 5, 6, and 7. Pain was evaluated subjectively using the 100 mm visual analogue scale.
Facial width assessment
The facial width measurement was done both pre- and post-operatively (POD1, POD 3, and POD7), using a flexible tape measure in accordance with the technique described by Gabka and Matsumura [Figure 2].[14] All measurements were done three times for each dimension, and the average score was recorded in centimeters (cm).
Figure 2.
Facial width measurement
Pre- and post-operatively, all patients were assessed for facial swelling, limitation in mouth opening, and pain using the same technique. Assessment for facial swelling and limitation in mouth opening was done by the researcher (who is also the surgeon). QoL assessments were done pre- and post-operatively for all individuals.
Assessment of mouth opening
Both pre- and post-operative interincisal mouth opening measurements were obtained by the use of a monoblock basic vernier caliper [Figure 3]. The individuals were required to sit in an upright position with the orbitomeatal line parallel to the floor. The maximum unassisted midline interincisal mouth opening was measured thrice, and the average was documented in millimeters (mm).
Figure 3.

Measurement of mouth opening
Quality of life
QoL assessments were done both pre- and post-operatively using the OHIP-14 QoL questionnaire. Postoperatively, assessment of postoperative QoL was done on POD1, POD3, and POD7. Each item was given scores ranging from 1 to 4, where scores 1, 2, 3, and 4 correspond to “not at all,” “a little,” “quite a lot,” and “very much,” respectively. A maximum total score of 56 (corresponding to the most severe form of QoL impairment) and a minimum score of 14 (corresponding to “no impairment” of QoL) could be obtained. Moreover, scores 1 and 2 were classified as “not affected” while scores 3 and 4 were classified as “affected.” Therefore, individuals with a summative score of 14–28 were categorized as “not affected,” while those with summative scores of 29–56 were classified as “affected.”
Statistical analysis
Data analysis was done using the Statistical Package for Social Sciences (SPSS) for Windows (version 16.0, Chicago, IL, USA). The analysis of pain, interincisal mouth opening and facial width were done using the Student's t-test. Comparison of pre- and post-operative QoL scores categorized as “affected” or “not affected” was done with the Chi-square. The comparison of summative scores pre- and post-operatively was done using the Student's t-test. The level of statistical significance was set at (P < 0.05).
Results
A total of 124 individuals were included in the final analysis. There were 49 (39.5%) males and 75 (60.5%) females, giving a male to female ratio of 1:1.5. The mean age (±standard deviation) was 28.5 (7.4) years with a range of 18–51 years. The most frequently encountered type of impaction was the mesioangular impaction, accounting for 51 (41.1%) of all the extractions done [Figure 4]. Recurrent pericoronitis was the principal reason for extraction being the indication for extraction in 53 (42.7%) of all extractions done.
Figure 4.
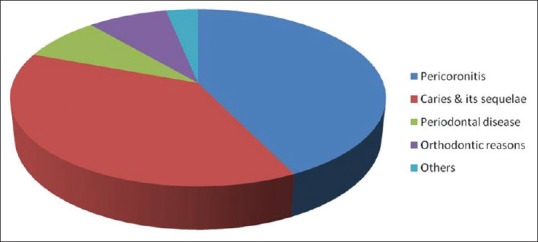
Indication for extraction
The mean preoperative pain value was lower than the mean postoperative pain values at all postoperative evaluation points except the POD7 [Figure 5]. The mean postoperative pain values were highest on the POD1; a gradual progressive reduction was noted in the pain scores until it approximated the mean preoperative score on the POD6. Notably, it was lower than the mean preoperative pain value by POD7 [Figure 5]. A comparison of the preoperative pain measurement and the postoperative pain values was statistically significant at all the postoperative evaluation days except POD6 (P < 0.05).
Figure 5.
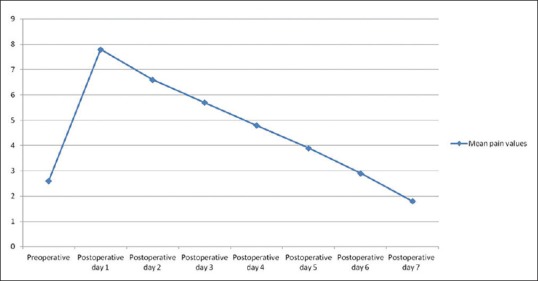
Mean preoperative and postoperative pain values
The mean preoperative interincisal mouth opening was higher than the mean postoperative interincisal mouth opening at all the postoperative evaluation points (i.e., POD1, POD3, and POD7) [Table 1]. A comparison of the mean preoperative interincisal mouth opening and the postoperative mouth opening measurements was statistically significant (P < 0.05) [Figure 6].
Table 1.
Pre- and post-operative quality of life subscales in all subjects (“percentage affected”)

Figure 6.
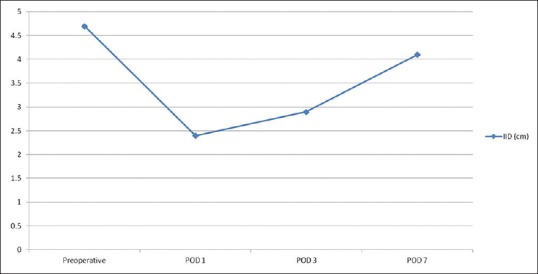
Mean preoperative and postoperative interincisal mouth opening measurements
The mean facial width was higher at all postoperative evaluation points (POD1, POD3, and POD7) than the mean preoperative values [Figure 7]. The highest postoperative values were observed on POD1, while the lowest values were recorded on POD 7. A comparison of the preoperative facial width values with the postoperative values showed a statistically significant difference at all postoperative evaluation points (P < 0.05) [Figure 7].
Figure 7.
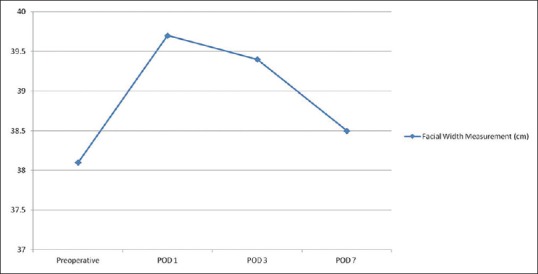
Mean preoperative and postoperative facial width measurements
Oral health-related quality of life
The mean preoperative OHIP-14 QoL score was lower than the mean postoperative scores obtained on each of the postoperative evaluation days. Notably, the mean postoperative score observed was highest on POD1, while the lowest score was recorded on POD7 [Figure 8]. A comparison of the mean preoperative score with the scores obtained on each postoperative evaluation day revealed a difference that was statistically significant for each. The “ability to chew” and the “change in diet” subscales were the principally affected subscales preoperatively [Table 1]. Conversely, the predominantly affected subscales on POD1 were the “ability to enjoy food,” “ability to chew,” and the “change in diet” subscales [Table 1]. The “change in diet” and “mouth opening ability” was the majorly affected subscales on POD3 and POD7, respectively. Notably, the percentage of individuals reporting impairment of various subscales increased drastically on POD1 and subsequently reduced through POD3 to attain the lowest levels on POD7 [Table 1]. Similarly, the mean OHIP-14 scores increased on POD1 in comparison to the preoperative values and subsequently reduced through POD3 to reach the lowest values on POD7. A significant proportion of individuals experienced social isolation, lost days at work and had difficulties engaging in their normal hobbies. The proportion of individuals who experienced these impairments was highest on POD1 and gradually declined over the postoperative period [Table 2].
Figure 8.
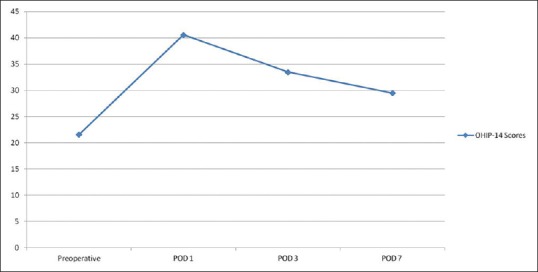
Mean preoperative and postoperative OHIP-14 scores
Table 2.
Percentage of subjects who lost days at work, experienced work isolation and/or could not continue with normal hobbies

Discussion
Increasingly, patients wish to know how a surgical procedure may impact on their wellbeing.[3] As such, it is important that patients are given evidence-based information on the likely course of their postoperative recovery. Especially in cases of prophylactic third molar extraction, patients should be provided information to enable them to juxtapose the risks of retaining impacted third molars with those of extracting them. In addition, modifications may be made to consent forms based on well-researched evidence of the expected effect on the postoperative QoL.
The OHIP-14 questionnaire was developed as an abridged version of the OHIP-49.[6] It has been shown to be reliable, valid, sensitive and precise.[15,16] A deterioration in the patients’ QoL was observed in the immediate postoperative period (the 1st week postoperatively). This observation is similar to the reports by van Wijk et al. and McGrath et al. who reported an initial sharp decline in the patients’ QoL in the immediate 3 days following surgical extraction and a gradual return to baseline at subsequent reviews.[5,11] The sharpest decline was noted on POD1 and subsequent gradual recovery was recorded over the remaining evaluation period. This correlates with the anticipated postsurgical inflammatory response, which is expected to be most severe within the first 24–72 h.[17,18] Information such as this should be made available to intending patients.
Ability to chew, ability to swallow, enjoyment of food, mouth opening ability were adversely affected in the majority of patients on POD1. This is similar to the observations made by other researchers.[5,19,20,21] This may be related to the fact that the surgical procedure involved elevation of a buccal mucoperiosteal flap, with the consequent inflammatory response from the adjacent tissues. Such inflammation may extend to involve the pterygomasseteric sling, thus culminating in limited mouth opening and/or trismus.[4,22,23] Painful mouth opening and/or trismus may affect patients chewing ability and enjoyment of food.[3,24,25] Dysphagia may be linked to the inflammatory response of the lingual and parapharyngeal tissues.[21,26,27,28] Majority of the patients 112 (90.3%) reported that the surgery necessitated a change in their diet. This may be because of the difficulty in chewing experienced by the patients. Therefore, they may have sought for alternative food items that require less or no chewing. Some authors have associated diet change with impaired of enjoyment of food, while others have associated with impaired perception of taste due to inflammatory compression of neural tissue.[4,9,20,26] Patients should be encouraged to consume foods that require little or no mastication.
Notably, changes in appearance were also reported by a significant proportion of patients. This may be related to the local inflammatory response to trauma, resulting in ipsilateral facial swelling.[2,3,5,29] Patients who are public figures or who have speaking engagements or public appearances may wish to postpone their surgeries especially when the reason for extraction is prophylactic in nature. Interestingly, a large proportion of the patients reported sleep impairment; this was most commonly reported on POD1. The reasons for sleep impairment may be due to postoperative operative site pain or even psychological reasons. Therefore, adequate analgesia and appropriate counseling should be done.
“Change in voice” and “ability to speak” were the least frequently affected subscales in this study similar to the report by McGrath et al. This may be because of the limited or nonexistent dissection on the lingual side, with resultant less inflammation on the lingual side.[4,5] Therefore, tongue movement, which is important in phonation, may be relatively undisturbed.
Majority of the patients lost days at work during the immediate postoperative period. This was especially marked on POD1. Inability to work during the immediate postoperative period following surgical extraction of third molars has been reported severally.[30,31] Some authors have reported an association the female sex with the inability to work.[30,31] Although more females reported lost days at work in this study, the difference when compared with values from their male counterparts was not statistically significant.
A number of patients had to temporarily disengage or reduce from their normal sport and social activities. Although this occurred in a comparatively low number of patients, it is important to inform intending patients of this possibility. It is also vital that patients are warned about the possible impairment they may experience in any of the domains/subscales.
Since most impairment in patients’ postoperative QoL may be associated with inflammatory responses, the use of anti-inflammatory drugs should be advocated for.[32,33,34] Many authors have evaluated the use of anti-inflammatory agents in third molar surgery with promising results.[4,34,35]
Postoperative values for pain, facial width, and mouth opening improved gradually relative to the values recorded on POD1, which is suggestive of the reducing intensity of the inflammatory response. Remarkably, postoperative evaluation of the patients on POD7 still gave average values for pain, facial width, mouth opening, and QoL that were worse than the average preoperative values. This trend was also recorded by other researchers.[7,36]
Conclusion
Surgical extraction of impacted mandibular third molars is associated with a significant deterioration of patients’ QoL, especially within the first 3 PODs. Prospective patients should be informed about this and ways of reducing this untoward effect should be explored.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Tschiesner UM, Rogers SN, Harreus U, Berghaus A, Cieza A. Comparison of outcome measures in head and neck cancer – Literature review 2000-2006. Head Neck. 2009;31:251–9. doi: 10.1002/hed.20960. [DOI] [PubMed] [Google Scholar]
- 2.Braimah RO, Ndukwe KC, Owotade FJ, Aregbesola SB. Oral health related quality of life (OHRQoL) following third molar surgery in sub-Saharan Africans: An observational study. Pan Afr Med J. 2016;25:97. doi: 10.11604/pamj.2016.25.97.7656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Adeyemo WL, Taiwo OA, Oderinu OH, Adeyemi MF, Ladeinde AL, Ogunlewe MO, et al. Oral health-related quality of life following non-surgical (routine) tooth extraction: A pilot study. Contemp Clin Dent. 2012;3:427–32. doi: 10.4103/0976-237X.107433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ibikunle AA, Adeyemo WL, Ladeinde AL. Oral health-related quality of life following third molar surgery with either oral administration or submucosal injection of prednisolone. Oral Maxillofac Surg. 2016;20:343–52. doi: 10.1007/s10006-016-0571-4. [DOI] [PubMed] [Google Scholar]
- 5.McGrath C, Comfort MB, Lo EC, Luo Y. Changes in life quality following third molar surgery – The immediate postoperative period. Br Dent J. 2003;194:265–8. doi: 10.1038/sj.bdj.4809930. [DOI] [PubMed] [Google Scholar]
- 6.Slade GD, Spencer AJ. Development and evaluation of the oral health impact profile. Community Dent Health. 1994;11:3–11. [PubMed] [Google Scholar]
- 7.Sancho-Puchades M, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Quality of life following third molar removal under conscious sedation. Med Oral Patol Oral Cir Bucal. 2012;17:e994–9. doi: 10.4317/medoral.17677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.White RP, Jr, Shugars DA, Shafer DM, Laskin DM, Buckley MJ, Phillips C, et al. Recovery after third molar surgery: Clinical and health-related quality of life outcomes. J Oral Maxillofac Surg. 2003;61:535–44. doi: 10.1053/joms.2003.50106. [DOI] [PubMed] [Google Scholar]
- 9.Ibikunle AA, Adeyemo WL. Oral health-related quality of life following third molar surgery with or without application of ice pack therapy. Oral Maxillofac Surg. 2016;20:239–47. doi: 10.1007/s10006-016-0558-1. [DOI] [PubMed] [Google Scholar]
- 10.Renton T, Hankins M, Sproate C, McGurk M. A randomised controlled clinical trial to compare the incidence of injury to the inferior alveolar nerve as a result of coronectomy and removal of mandibular third molars. Br J Oral Maxillofac Surg. 2005;43:7–12. doi: 10.1016/j.bjoms.2004.09.002. [DOI] [PubMed] [Google Scholar]
- 11.van Wijk A, Kieffer JM, Lindeboom JH. Effect of third molar surgery on oral health-related quality of life in the first postoperative week using Dutch version of oral health impact profile-14. J Oral Maxillofac Surg. 2009;67:1026–31. doi: 10.1016/j.joms.2008.12.041. [DOI] [PubMed] [Google Scholar]
- 12.Daabiss M. American society of anaesthesiologists physical status classification. Indian J Anaesth. 2011;55:111–5. doi: 10.4103/0019-5049.79879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Davenport DL, Bowe EA, Henderson WG, Khuri SF, Mentzer RM., Jr National surgical quality improvement program (NSQIP) risk factors can be used to validate American society of anesthesiologists physical status classification (ASA PS) levels. Ann Surg. 2006;243:636–41. doi: 10.1097/01.sla.0000216508.95556.cc. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gabka J, Matsumura T. Measuring techniques and clinical testing of an anti-inflammatory agent (tantum) Munch Med Wochenschr. 1971;113:198–203. [PubMed] [Google Scholar]
- 15.Montero-Martín J, Bravo-Pérez M, Albaladejo-Martínez A, Hernández-Martín LA, Rosel-Gallardo EM. Validation the oral health impact profile (OHIP-14sp) for adults in Spain. Med Oral Patol Oral Cir Bucal. 2009;14:E44–50. [PubMed] [Google Scholar]
- 16.Fernandes MJ, Ruta DA, Ogden GR, Pitts NB, Ogston SA. Assessing oral health-related quality of life in general dental practice in Scotland: Validation of the OHIP-14. Community Dent Oral Epidemiol. 2006;34:53–62. doi: 10.1111/j.1600-0528.2006.00254.x. [DOI] [PubMed] [Google Scholar]
- 17.Finnerty CC, Mabvuure NT, Ali A, Kozar RA, Herndon DN. The surgically induced stress response. JPEN J Parenter Enteral Nutr. 2013;37:21S–9S. doi: 10.1177/0148607113496117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sun L, Jia P, Zhang J, Zhang X, Zhang Y, Jiang H, et al. Production of inflammatory cytokines, cortisol, and aβ1-40 in elderly oral cancer patients with postoperative delirium. Neuropsychiatr Dis Treat. 2016;12:2789–95. doi: 10.2147/NDT.S113077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Slade GD, Foy SP, Shugars DA, Phillips C, White RP., Jr The impact of third molar symptoms, pain, and swelling on oral health-related quality of life. J Oral Maxillofac Surg. 2004;62:1118–24. doi: 10.1016/j.joms.2003.11.014. [DOI] [PubMed] [Google Scholar]
- 20.Savin J, Ogden GR. Third molar surgery – A preliminary report on aspects affecting quality of life in the early postoperative period. Br J Oral Maxillofac Surg. 1997;35:246–53. doi: 10.1016/s0266-4356(97)90042-5. [DOI] [PubMed] [Google Scholar]
- 21.Hassan OO. Lagos: Lagos University Teaching Hospital; 2010. The Effect of Dexamethasone Administration on the Quality of Life after Mandibular Third Molar Surgery. A Dissertation Submitted to the National Postgraduate Medical College of Nigeria (NPMCN) [Google Scholar]
- 22.Warraich R, Faisal M, Rana M, Shaheen A, Gellrich NC, Rana M, et al. Evaluation of postoperative discomfort following third molar surgery using submucosal dexamethasone - a randomized observer blind prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116:16–22. doi: 10.1016/j.oooo.2012.12.007. [DOI] [PubMed] [Google Scholar]
- 23.UStün Y, Erdogan O, Esen E, Karsli ED. Comparison of the effects of 2 doses of methylprednisolone on pain, swelling, and trismus after third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:535–9. doi: 10.1016/S1079210403004645. [DOI] [PubMed] [Google Scholar]
- 24.Grossi GB, Maiorana C, Garramone RA, Borgonovo A, Beretta M, Farronato D, et al. Effect of submucosal injection of dexamethasone on postoperative discomfort after third molar surgery: A prospective study. J Oral Maxillofac Surg. 2007;65:2218–26. doi: 10.1016/j.joms.2006.11.036. [DOI] [PubMed] [Google Scholar]
- 25.Pandurić DG, Brozović J, Susić M, Katanec D, Bego K, Kobler P, et al. Assessing health-related quality of life outcomes after the surgical removal of a mandibular third molar. Coll Antropol. 2009;33:437–47. [PubMed] [Google Scholar]
- 26.Ogden GR, Bissias E, Ruta DA, Ogston S. Quality of life following third molar removal: A patient versus professional perspective. Br Dent J. 1998;185:407–10. doi: 10.1038/sj.bdj.4809827. [DOI] [PubMed] [Google Scholar]
- 27.Karaca I, Simşek S, Uǧar D, Bozkaya S. Review of flap design influence on the health of the periodontium after mandibular third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:18–23. doi: 10.1016/j.tripleo.2006.11.049. [DOI] [PubMed] [Google Scholar]
- 28.Kirk DG, Liston PN, Tong DC, Love RM. Influence of two different flap designs on incidence of pain, swelling, trismus, and alveolar osteitis in the week following third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:e1–6. doi: 10.1016/j.tripleo.2007.01.032. [DOI] [PubMed] [Google Scholar]
- 29.Majid OW. Submucosal dexamethasone injection improves quality of life measures after third molar surgery: A comparative study. J Oral Maxillofac Surg. 2011;69:2289–97. doi: 10.1016/j.joms.2011.01.037. [DOI] [PubMed] [Google Scholar]
- 30.Aravena PC, Delgado F, Olave H, Ulloa-Marin C, Perez-Rojas F. Chilean patients’ perception of oral health-related quality of life after third molar surgery. Patient Prefer Adherence. 2016;10:1719–25. doi: 10.2147/PPA.S106814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Deliverska EG, Petkova M. Complications after extraction of impacted third molars-literature review. J IMAB Ann Proc Sci Pap. 2016;22:1202–11. [Google Scholar]
- 32.Markiewicz MR, Brady MF, Ding EL, Dodson TB. Corticosteroids reduce postoperative morbidity after third molar surgery: A systematic review and meta-analysis. J Oral Maxillofac Surg. 2008;66:1881–94. doi: 10.1016/j.joms.2008.04.022. [DOI] [PubMed] [Google Scholar]
- 33.Tiwana PS, Foy SP, Shugars DA, Marciani RD, Conrad SM, Phillips C, et al. The impact of intravenous corticosteroids with third molar surgery in patients at high risk for delayed health-related quality of life and clinical recovery. J Oral Maxillofac Surg. 2005;63:55–62. doi: 10.1016/j.joms.2004.01.029. [DOI] [PubMed] [Google Scholar]
- 34.Majid OW, Mahmood WK. Effect of submucosal and intramuscular dexamethasone on postoperative sequelae after third molar surgery: Comparative study. Br J Oral Maxillofac Surg. 2011;49:647–52. doi: 10.1016/j.bjoms.2010.09.021. [DOI] [PubMed] [Google Scholar]
- 35.Dan AE, Thygesen TH, Pinholt EM. Corticosteroid administration in oral and orthognathic surgery: A systematic review of the literature and meta-analysis. J Oral Maxillofac Surg. 2010;68:2207–20. doi: 10.1016/j.joms.2010.04.019. [DOI] [PubMed] [Google Scholar]
- 36.Colorado-Bonnin M, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Quality of life following lower third molar removal. Int J Oral Maxillofac Surg. 2006;35:343–7. doi: 10.1016/j.ijom.2005.08.008. [DOI] [PubMed] [Google Scholar]