

Abstract
Background:
Porcelain fracture is the most important problem in fixed prosthetic restorations. The replacement of fractured restoraions isn’t often prefer by patients and dentists. Intraoral repair of fractured porcelain is a big alternative for patient and dentist. For this reason, dentists try to improve different surface treatments to increase the bond strength between porcelain and repair materials such as composite resins.
Aims:
The aim of this study was to evaluate the shear bond strength (SBS) of nano-hybrid (Nh.com) and nano-ceramic composite resins (Nc.com) to this feldspathic porcelains (Vita and Ivoclar).
Settings and Design:
120 ceramic disc were fabricated from feldspathic porcelain.
Materials and Methods:
The following surface treatment was applied on the ceramic surface: 1) Hydrofluoric acid+silane, 2) Air-abrasion+silane, 3) Air-abrasion=Control group. Nh.com and Nc.com was placed on the porcelain surface. Half of the specimens were stored in 37 ± 2oC distilled water and another half were subjected to thermocycling before SBS. The samples placed in an universal testing machine and applied shear force until seperation occured.
Statistical Analysis Used:
The data were analyzed by multi-way analysis of variance (ANOVA) and Duncan test (P <0.05).
Results:
The results show that Ivoclar and Vita had almost equal fracture values. Nh.com showed high bond strength than Nc.com. In the Ivoclar porcelain, hydrofluoric acid etching had highest fracture values than other surface treatments, and in the vita porcelain air-abrasion had a little difference from hydrofluoric acid etching.
Conclusions:
Different surface treatments show different effect on SBS between feldspathic porcelain and composite resins.
Keywords: Bond strength, composite, porcelain
Introduction
Porcelain-fused-to-metal crowns have been used as predictable materials since the 1960s, owing to their mechanical strength and low cost.[1,2] Studies have shown various advantages of the ceramics, such as color stability, radiopacity, coefficient of thermal expansion similar to that of dentin, large compressive strength and high abrasive resistance, and esthetics.[3] The fracture of veneering porcelain may result from trauma, improper metal framework design, incompatibility between the thermal expansion coefficient of the porcelain and core, inadequate tooth preparation, inadequate occlusal adjustment, and intraceramic defects.[4,5] The majority (65%) of the failures have been observed in the anterior region, whereas 35% were in the posterior region. Sixty percent of the failures occurred at the labial, 27% at the buccal, 5% at the incisal, and 8% at the occlusal regions. These fractures were mainly in the maxilla (75%), predominantly at the labial surface.[1]
The immediate replacement of failed complex prostheses is often impossible though, as it requires additional time, effort, and expense. In this situation, repair is a suitable method to rehabilitate the contour and color of fractured restorations. Such repair demands durable bonding, even though it is not a permanent treatment.[6] Several resin-based materials have been used to repair porcelain restorations. It is suggested that the bond strength between these two types of materials (ceramic and resin-based material) is highly dependent on surface preparation.[3] Many studies on the efficacy of ceramic surface treatment using burs, etching with hydrofluoric acid (HF), phosphoric acid, accidulated phosphate fluoride, ammonium bifluoride, lasers (CO2, Er-YAG, ND-YAG, Er, and Cr-YSGG) and air abrasion have been published that reportedly increase the bond strength of resin material to porcelain.[7,8,9,10] The use of HF followed by silane application is the standard clinical process for increasing the bond strength when repairing the porcelain surface with composite resin; this is because of the microporosites that HF produces on the porcelain surface with selective dissolution of the glass matrix. This has been observed via scanning electron microscopy (SEM).[8,11,12]
Air abrasion is a common method of surface treatment for increasing micromechanical retention because it produces a clean and active porcelain surface. On the other hand, it does not cause acute acid burns on the patient's oral tissues. In this method, the aluminum oxide particles remove the weakened phases of ceramic and create irregularities on the surface.[13] These irregularities increase the surface area and improve the mechanical retention and bond.[14] Surface topography analysis of treated ceramic with SEM provides qualitative information in this matter because this technique enables direct observation of the surface details with a high resolution.[15]
Several researchers reported that mechanical roughening by both a diamond bur and sandblaster was effective for porcelain repair.[16,17] The best results were achieved with a bur by Leibrock et al.[4] and with air abrasion by Tulunoglu and Beydemir.[18] In many studies, however, the comparison of bonding qualities with different roughening methods was performed using different resin composite repair systems. For this reason, a comparison based on the use of the same repair system is needed to confirm the differences in roughening procedures.
The shear bond strength (SBS) test arrangement has been the most common laboratory technique for evaluating adhesives for resin-bonded ceramic restorations and ceramic repair systems. It has been shown that SBS measurements are very sensitive to the method of application of the adhesive and design of the testing arrangement.[19,20,21]
The aim of this study was to evaluate the SBS of nanohybrid (Nh.com) and nanoceramic (Nc.com) composite resins to feldspathic porcelain subjected to different surface treatments. Nh.com and Nc.com composite resins were used due to their contents and compared with each other. The null hypothesis of the present study is that Nh.com and Nc.com composite resins may show different SBS to feldspathic porcelain. Nc.com may show higher SBS than Nh.com to feldspathic porcelain because of its ceramic particle content.
Methods
The materials used in the present study are listed in Table 1. For this study, 120 samples made of feldspathic porcelain (7 mm in diameter and 3 mm in thickness) were prepared according to the manufacturer's instructions in two different products. Glaze process was not applied to the samples. Porcelain samples were embedded in a self-cure acrylic resin which was 12 mm in diameter and 6 mm in length. The surface of each specimen was polished with 300, 600, 800, 1000, and 1200 grit SiC papers to provide standardization on specimens’ surfaces. They were then ultrasonically cleaned in distilled water for 5 min. Samples were randomly divided into three groups as to surface treatments and the following surface treatments were applied to porcelain samples:
Table 1.
Materials used in the present study
Group H: HF (9.5%) + silane
Group A: Air abrasion (50 micron with Al2O3 particles) + silane
Group C: Air abrasion (50 micron with Al2O3 particles) = control group
Nh.com and Nc.com resins were placed on the ceramic specimens which were 4 mm in diameter and 2 mm thick with the help of layering methods and they were light polymerized.
After the surface treatments (air abrasion and acid etching), the surfaces of two marks of feldspathic porcelains were analyzed topographically under SEM at a magnification of ×1000 and ×2000 [Figures 1 and 2].
Figure 1.
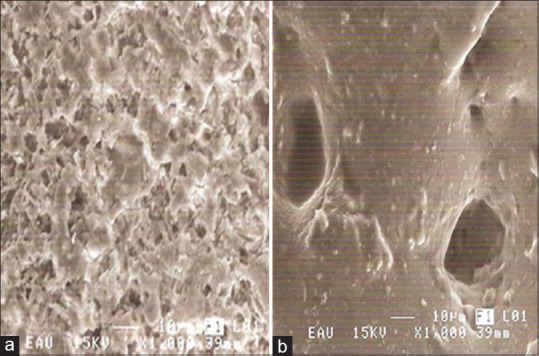
Scanning electron microscopy observation of the Ivoclar porcelain after surface treatments at ×1000 and bar marker indicating 10 μm. (a) Surface with etching hydrofluoric acid (9.5%). (b) Surface with air abraded with aluminum oxide
Figure 2.
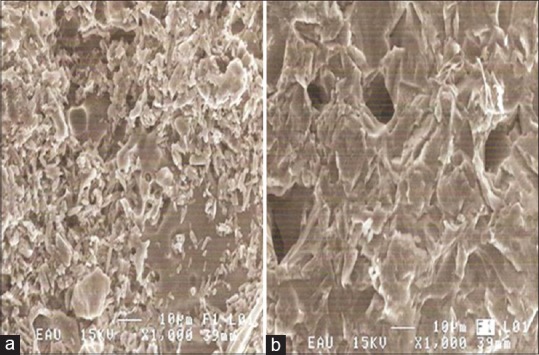
Scanning electron microscopy observation of the Vita porcelain after surface treatments at ×1000 and bar marker indicating 10 μm. (a) Surface with etching hydrofluoric acid (9.5%). (b) Surface with air abraded with aluminum oxide
After all samples were prepared, half of them were immersed in 37°C ± 2°C distilled water (D), and another half were subjected to thermocycling (T) for 5000 cycles between 5°C and 55°C. To evaluate the BS of the samples, they were respectively placed in a universal test machine (Instron, 2710-003 Model, Instron, USA) and shear force was applied until break and then separation occurred. The data were analyzed with statistical software SPSS version 17.0 (SPSS, Chicago, USA). Multiway ANOVA was performed.
After shear testing, all specimens were analyzed using an optical microscope at ×50 magnification for failure analysis. Failure types were categorized as adhesive between ceramic and Nh.com resin, ceramic and Nc.com resin; cohesive failure of the ceramic only, Nh.com resin only, Nc.com resin only; and cohesive failure of Nh.com and Nc.com resins accompanied with adhesive failure at the interface.
Results
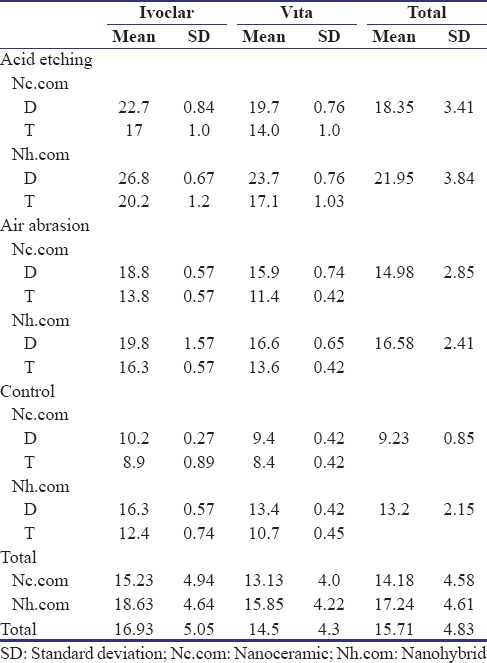
The means and standard deviations of fracture values are shown in Table 2. H-Nh.com-D group showed the highest SBS values, while C-Nh.com-T group showed the lowest SBS values in Ivoclar porcelain. In all the groups, applying Nh.com composite resin and stored in distilled water resulted in high fracture values. A-Nh.com-D group showed high fracture values while C-Nc.com-T group showed low fracture values in Vita porcelain.
Table 2.
Means and standard deviation of each group
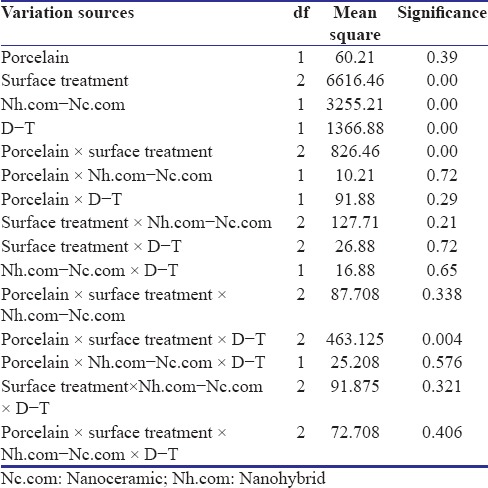
The difference between groups was evaluated by multiway analysis of variance [Table 3]. The results of ANOVA showed statistically significant differences among surface treatments, composite resins and storage conditions (P < 0.05), but there was no statistically significant differences between porcelain marks (P < 0.05). When we evaluated the results of interactions, only two-factor interactions of porcelain × surface treatment and three-factor interactions of porcelain × surface treatment × D-T were statistically significant. There was no statistically significant differences between surface treatments according to Duncan test..
Table 3.
Results of ANOVA
SBS of two different porcelains after the surface treatments are depicted in Figure 3. In the Ivoclar porcelain, the H group showed the highest SBS values than that of the A group, and in the Vita porcelain, H group and A group showed almost the same SBS values. The control groups of both porcelains showed the lowest SBS.
Figure 3.
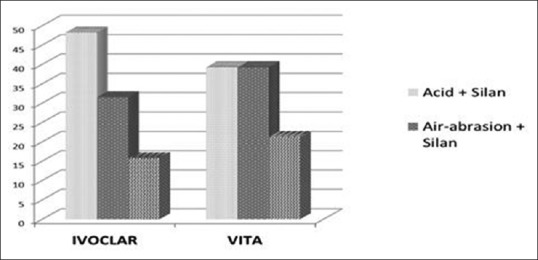
Mean bonding strength of two different porcelain surfaces according to surface treatment
SBS of Nh.com and Nc.com resins to two different porcelains is summarized in Table 4. In two porcelains, Nh.com showed the highest SBS than that of Nc.com [Figure 4].
Table 4.
Number of the failure types after the shear test
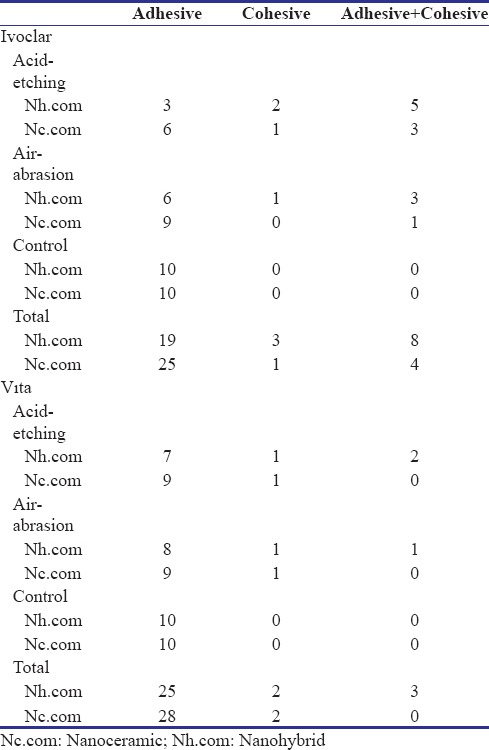
Figure 4.
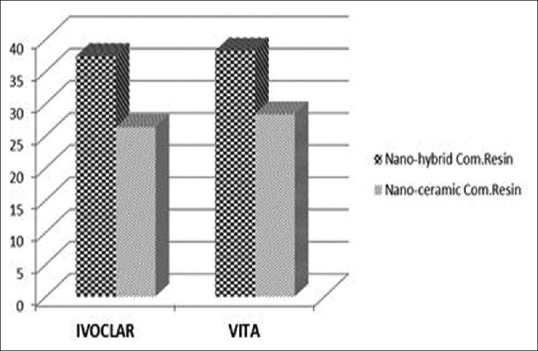
Mean bonding strength of nanohybrid composite resin and nanoceramic composite resin to two different porcelain surfaces
SBS of Nh.com and Nc.com composite resins connected with surface treatment is depicted in Figure 5. In all groups, SBS of Nh.com composite resin is more than Nc.com composite resin. The highest values are seen with acid etching + silane application and the lowest levels are seen in the control group.
Figure 5.
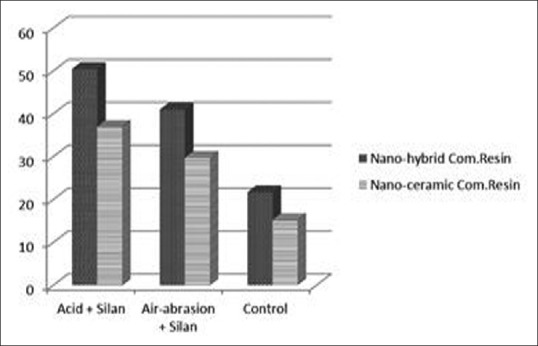
Mean bonding strength of nanohybrid composite resin and nanoceramic composite resin according to the surface treatment
If the stored conditions are taken into consideration [Figure 6], the group that has been stored in distilled water showed higher SBS than the group subjected to thermocycling. While in the group that is stored in distilled water, Vita-marked porcelain showed the higher fracture values, whereas in the group that is applied with thermocycle, Ivoclar-marked porcelain showed higher fracture values with little difference.
Figure 6.
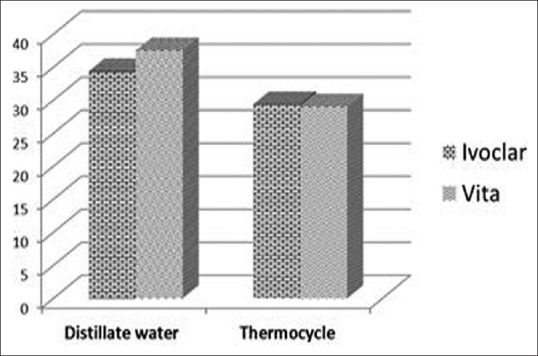
Mean bonding strength of two different porcelain surfaces according to the stored condition
The failure types of all specimens are shown in Table 4. Adhesive failure was the most commonly seen failure type in specimens.
Discussion
In the present study, we evaluated the SBS between different type composite resins and different mark feldspathic porcelain. The null hypothesis of the study was that Nh.com and Nc.com may show different SBS to feldspathic porcelain. The results of the study supported the null hypothesis. However, contrary to expectations, Nh.com composite resin showed higher SBS values than Nc.com composite resin. According to this result, we can say that ceramic particles in the composite resin have no positive effect on bonding of feldspathic porcelain.
It was found that HF etching was the most effective treatment to roughen Ivoclar porcelain surface to create a strong bond with Nh.com composite resin, and air abrasion had a little SBS difference from HF etching in Vita porcelain. Otherwise, it was found that Nh.com composite resin showed low SBS to the porcelain surface with different surface treatments applied than that of Nc.com composite resin.
Various techniques such as acid etching, air abrasion, silanization, and application of metal primer have been introduced for the repair of fractured metal ceramic restorations. Acid etching of feldspathic porcelain creates micromechanical undercuts that have a decisive effect for better adhesion.[2,22] Many studies have reported that a combination of micromechanical roughness and silane application to the porcelain creates durable bonding.[23,24] Silane is a dual functional monomer that consists of a silanol group that reacts with the ceramic surface, and it contains a methacrylate group that co-polymerizes with the resin matrix of the composite.[2] Silane coupling agents are known to enhance the wettability of glass substrates by resin composites and are also known to increase the mechanical and chemical bonding of resin composite to ceramics.[25] The alloy primer or composite-containing diphosphate monomer (10-Methacryloyloxydecyl dihydrogen phosphate), which has a phosphate ester group to bond directly to metal oxides, has been assessed as having superior bonding durability to base metal alloy.[26]
Several authors consider etching of the ceramic surface as being critical for the SBS of a composite resin when it is used to repair fractured ceramic restorations. HFA etching is a preferred method for modifying ceramic surfaces to improve micromechanical retention between a bonding agent and a fractured ceramic restoration because it is more effective in roughening the surface than other chemical methods.[24,27] The shear SBS of a composite resin to a fractured ceramic restoration is affected by the type of composite resin.[28,29,30] The shear SBS of hybrid composite resins is generally higher than that provided by microfilled composite resins.[30]
Wolf et al.[31] show that air abrasion with 50 μm aluminum oxide is a better method for preparing the surface than bur-performed retentions. Nevertheless, singly, air abrasion is not sufficient to improve the bond of composite–porcelain interface.[32] Silanization improved repair resistance when HF was previously utilized.[33] However, there is no consensus on the best porcelain treatment method to be applied in different clinical situations.[34] Etching procedures have been used to facilitate bonding between porcelain and resin, creating a porous surface on the porcelain that leads to a retentive bond.[32]
While HF selectively dissolves the glass matrix creating micromechanical retention, silanization serves for the chemical adhesion between the organic and inorganic substances with which durable adhesion could be obtained.[2] HF is not necessary to obtain resistant adhesion between composite and porcelain if the silane agent, which reacts with OH groups on the porcelain surface, is used.[25] Silane is a functional monomer consisting of a silanol group that reacts with the ceramic surface and contains a methacrylate group that co-polymerizes with the resin matrix of the composite. Silane coupling agents are known to enhance the wettability of glass substrates by resin composites, contribute to covalent bond formation between the ceramic surface and the composite, and at the same time, increase physical, mechanical, and chemical bonding of resin composite to ceramic. Their decreased hydrolytic stability at the bonded interface has been previously reported.[35,36,37]
Silane agents appear to be the essential components for a porcelain repair procedure, by modifying its surface structure, rendering it more reactive with the composite, enabling chemical adhesion in both inorganic/porcelain and organic/composite surfaces. Theoretically, the silane bond should provide a stable repair of the fractured porcelain.[25] Lacy et al.[38] observed that, when silane was not applied, the composite BS to porcelain was relatively weak, regardless of the type of surface treatment, with the failure occurring at the interface. The values were higher with silane application after etching. Thus, the findings suggest that bonding to porcelain is mostly chemical and not mechanical.[37]
Adequate bond between ceramics and composite resins is achieved with a silane coupling agent and an adhesive. Silanes work as mediators, promoting adhesion between inorganic and organic matrices through dual reactivity.[39]
Kupiec[40] evaluated three different ceramic surface treatments: (a) aluminum oxide (Al2O3) and air abrasion (50 μm), (b) 8% HF, and (c) air abrasion and HF. The last combination recorded the most consistently effective BS. Aluminum oxide abrasion provides a clean and reactive bonding surface in porcelains.[41]
Regarding the topographic patterns produced by the treatments on the ceramic surface, the specimens etched with HF acid presented a rougher surface in the Ivoclar-marked porcelain than the Vita-marked porcelain. The specimens air abraded with Al2O3 particle presented higher retention areas in the Ivoclar-marked porcelain than that of the Vita-marked porcelain [Figures 1 and 2]. Ivoclar-marked porcelain showed the higher bonding resistance than the Vita-marked porcelain. The SEM pictures also supported this result.
Researchers found that bond failures occurred predominantly in porcelain (cohesive).[17] In contrast to this finding, in the present study, bond failures occurred predominantly between porcelain and composite resins.
Shear strength test has been the most commonly employed test modality to study the performance of porcelain repair systems. However, it is believed that this test geometry causes high tensile surface stresses within the porcelain, close to the area of load application, initiating fracture at the porcelain surface.[42]
Conclusions
Within the limitations, these conclusions were drawn;
Different mark of feldspathic porcelain showed different SBS values
Different surface treatments showed different effects on SBS of composite resins to feldspathic porcelain
Nc.com composite resin showed lower SBS values than that of Nh.com composite resin
Ceramic particles in the composite resin have no positive effect on the bonding of feldspathic porcelain.
One limitation of the present study is that the surface treatment is not enough. New surface treatment will be applied except for conventional surface treatment. Moreover, different substructural materials will be used except porcelain.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors wish to thank Memiş Özdemir for his professional assistance with the statistical analysis. This study was orally presented at FDI 2013 Istanbul 101st Annual World Dental Congress in Turkey on August 28–31, 2013.
References
- 1.dos Santos JG, Fonseca RG, Adabo GL, dos Santos Cruz CA. Shear bond strength of metal-ceramic repair systems. J Prosthet Dent. 2006;96:165–73. doi: 10.1016/j.prosdent.2006.07.002. [DOI] [PubMed] [Google Scholar]
- 2.Ozcan M, Vallittu PK. Effect of surface conditioning methods on the bond strength of luting cement to ceramics. Dent Mater. 2003;19:725–31. doi: 10.1016/s0109-5641(03)00019-8. [DOI] [PubMed] [Google Scholar]
- 3.Pameijer CH, Louw NP, Fischer D. Repairing fractured porcelain: How surface preparation affects shear force resistance. J Am Dent Assoc. 1996;127:203–9. doi: 10.14219/jada.archive.1996.0170. [DOI] [PubMed] [Google Scholar]
- 4.Leibrock A, Degenhart M, Behr M, Rosentritt M, Handel G. In vitro study of the effect of thermo- and load-cycling on the bond strength of porcelain repair systems. J Oral Rehabil. 1999;26:130–7. doi: 10.1046/j.1365-2842.1999.00346.x. [DOI] [PubMed] [Google Scholar]
- 5.Ozcan M. Fracture reasons in ceramic-fused-to-metal restorations. J Oral Rehabil. 2003;30:265–9. doi: 10.1046/j.1365-2842.2003.01038.x. [DOI] [PubMed] [Google Scholar]
- 6.Yoo JY, Yoon HI, Park JM, Park EJ. Porcelain repair – İnfluence of different systems and surface treatments on resin bond strength. J Adv Prosthodont. 2015;7:343–8. doi: 10.4047/jap.2015.7.5.343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Eduardo Cde P, Bello-Silva MS, Moretto SG, Cesar PF, de Freitas PM. Microtensile bond strength of composite resin to glass-infiltrated alumina composite conditioned with Er, Cr: YSGG laser. Lasers Med Sci. 2012;27:7–14. doi: 10.1007/s10103-010-0822-9. [DOI] [PubMed] [Google Scholar]
- 8.Kukiattrakoon B, Thammasitboon K. Optimal acidulated phosphate fluoride gel etching time for surface treatment of feldspathic porcelain: On shear bond strength to resin composite. Eur J Dent. 2012;6:63–9. [PMC free article] [PubMed] [Google Scholar]
- 9.Blatz MB, Sadan A, Kern M. Resin-ceramic bonding: A review of the literature. J Prosthet Dent. 2003;89:268–74. doi: 10.1067/mpr.2003.50. [DOI] [PubMed] [Google Scholar]
- 10.Dilber E, Yavuz T, Kara HB, Ozturk AN. Comparison of the effects of surface treatments on roughness of two ceramic systems. Photomed Laser Surg. 2012;30:308–14. doi: 10.1089/pho.2011.3153. [DOI] [PubMed] [Google Scholar]
- 11.Yavuz T, Dilber E, Kara HB, Tuncdemir AR, Ozturk AN. Effects of different surface treatments on shear bond strength in two different ceramic systems. Lasers Med Sci. 2013;28:1233–9. doi: 10.1007/s10103-012-1201-5. [DOI] [PubMed] [Google Scholar]
- 12.Fabianelli A, Pollington S, Papacchini F, Goracci C, Cantoro A, Ferrari M, et al. The effect of different surface treatments on bond strength between leucite reinforced feldspathic ceramic and composite resin. J Dent. 2010;38:39–43. doi: 10.1016/j.jdent.2009.08.010. [DOI] [PubMed] [Google Scholar]
- 13.Ozcan M. Evaluation of alternative intra-oral repair techniques for fractured ceramic-fused-to-metal restorations. J Oral Rehabil. 2003;30:194–203. doi: 10.1046/j.1365-2842.2003.01037.x. [DOI] [PubMed] [Google Scholar]
- 14.Bottino MC, Ozcan M, Coelho PG, Valandro LF, Bressiani JC, Bressiani AH, et al. Micro-morphological changes prior to adhesive bonding: High-alumina and glassy-matrix ceramics. Braz Oral Res. 2008;22:158–63. doi: 10.1590/s1806-83242008000200011. [DOI] [PubMed] [Google Scholar]
- 15.Kara HB, Dilber E, Koc O, Ozturk AN, Bulbul M. Effect of different surface treatments on roughness of IPS empress 2 ceramic. Lasers Med Sci. 2012;27:267–72. doi: 10.1007/s10103-010-0860-3. [DOI] [PubMed] [Google Scholar]
- 16.Wolf DM, Powers JM, O’Keefe KL. Bond strength of composite to porcelain treated with new porcelain repair agents. Dent Mater. 1992;8:158–61. doi: 10.1016/0109-5641(92)90074-m. [DOI] [PubMed] [Google Scholar]
- 17.Suliman AH, Swift EJ, Jr, Perdigao J. Effects of surface treatment and bonding agents on bond strength of composite resin to porcelain. J Prosthet Dent. 1993;70:118–20. doi: 10.1016/0022-3913(93)90004-8. [DOI] [PubMed] [Google Scholar]
- 18.Tulunoglu IF, Beydemir B. Resin shear bond strength to porcelain and a base metal alloy using two polymerization schemes. J Prosthet Dent. 2000;83:181–6. doi: 10.1016/s0022-3913(00)80010-4. [DOI] [PubMed] [Google Scholar]
- 19.Anusavice KJ, Dehoff PH, Fairhurst CW. Comparative evaluation of ceramic-metal bond tests using finite element stress analysis. J Dent Res. 1980;59:608–13. doi: 10.1177/00220345800590030901. [DOI] [PubMed] [Google Scholar]
- 20.Van Noort R, Noroozi S, Howard IC, Cardew G. A critique of bond strength measurements. J Dent. 1989;17:61–7. doi: 10.1016/0300-5712(89)90131-0. [DOI] [PubMed] [Google Scholar]
- 21.Van Noort R, Cardew GE, Howard IC, Noroozi S. The effect of local interfacial geometry on the measurement of the tensile bond strength to dentin. J Dent Res. 1991;70:889–93. doi: 10.1177/00220345910700050501. [DOI] [PubMed] [Google Scholar]
- 22.Borges GA, Sophr AM, de Goes MF, Sobrinho LC, Chan DC. Effect of etching and airborne particle abrasion on the microstructure of different dental ceramics. J Prosthet Dent. 2003;89:479–88. doi: 10.1016/s0022-3913(02)52704-9. [DOI] [PubMed] [Google Scholar]
- 23.Panah FG, Rezai SM, Ahmadian L. The influence of ceramic surface treatments on the micro-shear bond strength of composite resin to IPS Empress 2. J Prosthodont. 2008;17:409–14. doi: 10.1111/j.1532-849X.2007.00296.x. [DOI] [PubMed] [Google Scholar]
- 24.Chen JH, Matsumura H, Atsuta M. Effect of etchant, etching period, and silane priming on bond strength to porcelain of composite resin. Oper Dent. 1998;23:250–7. [PubMed] [Google Scholar]
- 25.Shahverdi S, Canay S, Sahin E, Bilge A. Effects of different surface treatment methods on the bond strength of composite resin to porcelain. J Oral Rehabil. 1998;25:699–705. doi: 10.1046/j.1365-2842.1998.00299.x. [DOI] [PubMed] [Google Scholar]
- 26.Yanagida H, Tanoue N, Ide T, Matsumura H. Evaluation of two dual-functional primers and a tribochemical surface modification system applied to the bonding of an indirect composite resin to metals. Odontology. 2009;97:103–8. doi: 10.1007/s10266-009-0103-x. [DOI] [PubMed] [Google Scholar]
- 27.Kato H, Matsumura H, Ide T, Atsuta M. Improved bonding of adhesive resin to sintered porcelain with the combination of acid etching and a two-liquid silane conditioner. J Oral Rehabil. 2001;28:102–8. doi: 10.1046/j.1365-2842.2001.00627.x. [DOI] [PubMed] [Google Scholar]
- 28.Matsumura H, Kawahara M, Tanaka T, Atsuta M. A new porcelain repair system with a silane coupler, ferric chloride, and adhesive opaque resin. J Dent Res. 1989;68:813–8. doi: 10.1177/00220345890680051201. [DOI] [PubMed] [Google Scholar]
- 29.Coornaert J, Adriaens P, De Boever J. Long-term clinical study of porcelain-fused-to-gold restorations. J Prosthet Dent. 1984;51:338–42. doi: 10.1016/0022-3913(84)90217-8. [DOI] [PubMed] [Google Scholar]
- 30.Gregory WA, Hagen CA, Powers JM. Composite resin repair of porcelain using different bonding materials. Oper Dent. 1988;13:114–8. [PubMed] [Google Scholar]
- 31.Wolf DM, Powers JM, O’Keefe KL. Bond strength of composite to etched and sandblasted porcelain. Am J Dent. 1993;6:155–8. [PubMed] [Google Scholar]
- 32.Kelsey WP, 3rd, Latta MA, Stanislav CM, Shaddy RS. Comparison of composite resin-to-porcelain bond strength with three adhesives. Gen Dent. 2000;48:418–21. [PubMed] [Google Scholar]
- 33.Swift EJ, Jr, Cloe BC, Boyer DB. Effect of a silane coupling agent on composite repair strengths. Am J Dent. 1994;7:200–2. [PubMed] [Google Scholar]
- 34.Kussano CM, Bonfante G, Batista JG, Pinto JH. Evaluation of shear bond strength of composite to porcelain according to surface treatment. Braz Dent J. 2003;14:132–5. doi: 10.1590/s0103-64402003000200011. [DOI] [PubMed] [Google Scholar]
- 35.Ozcan M, Valandro LF, Amaral R, Leite F, Bottino MA. Bond strength durability of a resin composite on a reinforced ceramic using various repair systems. Dent Mater. 2009;25:1477–83. doi: 10.1016/j.dental.2009.06.020. [DOI] [PubMed] [Google Scholar]
- 36.Matinlinna JP, Lassila LV, Ozcan M, Yli-Urpo A, Vallittu PK. An introduction to silanes and their clinical applications in dentistry. Int J Prosthodont. 2004;17:155–64. [PubMed] [Google Scholar]
- 37.Berry T, Barghi N, Chung K. Effect of water storage on the silanization in porcelain repair strength. J Oral Rehabil. 1999;26:459–63. doi: 10.1046/j.1365-2842.1999.00396.x. [DOI] [PubMed] [Google Scholar]
- 38.Lacy AM, LaLuz J, Watanabe LG, Dellinges M. Effect of porcelain surface treatment on the bond to composite. J Prosthet Dent. 1988;60:288–91. doi: 10.1016/0022-3913(88)90270-3. [DOI] [PubMed] [Google Scholar]
- 39.Matinlinna JP, Vallittu PK. Bonding of resin composites to etchable ceramic surfaces-an insight review of the chemical aspects on surface conditioning. J Oral Rehabil. 2007;34:622–30. doi: 10.1111/j.1365-2842.2005.01569.x. [DOI] [PubMed] [Google Scholar]
- 40.Kupiec KA, Wuertz KM, Barkmeier WW, Wilwerding TM. Evaluation of porcelain surface treatments and agents for composite-to-porcelain repair. J Prosthet Dent. 1996;76:119–24. doi: 10.1016/s0022-3913(96)90294-2. [DOI] [PubMed] [Google Scholar]
- 41.de Melo RM, Valandro LF, Bottino MA. Microtensile bond strength of a repair composite to leucite-reinforced feldspathic ceramic. Braz Dent J. 2007;18:314–9. doi: 10.1590/s0103-64402007000400008. [DOI] [PubMed] [Google Scholar]
- 42.Della Bona A, van Noort R. Shear vs. Tensile bond strength of resin composite bonded to ceramic. J Dent Res. 1995;74:1591–6. doi: 10.1177/00220345950740091401. [DOI] [PubMed] [Google Scholar]