

Abstract
Background
Sex differences in disruptive behavior and sensitivity to social context are documented, but the intersection between them is rarely examined empirically. This report focuses on sex differences in observed disruptive behavior across interactional contexts and diagnostic status.
Methods
Preschoolers (n = 327) were classified as non-disruptive (51%), clinically at-risk (26%), and disruptive (23%) using parent and teacher reports on developmentally-validated measures of disruptive behavior and impairment. Observed disruptive behavior was measured with the Disruptive Behavior Diagnostic Observation Schedule (DB-DOS), a developmentally-sensitive observational paradigm characterizing variation in preschoolers’ disruptive behavior across two interactional contexts (parent and examiner).
Results
Repeated measures analyses of variance revealed a three-way interaction of child sex-by-diagnostic status-by-interactional context (F = 9.81, p < .001). Disruptive boys were the only subgroup whose behavior was not sensitive to interactional context: they displayed comparable levels of disruptive behavior with parents and examiners. In contrast, disruptive girls demonstrated the strongest context effect of any group. Specifically, with the examiner, disruptive girls’ behavior was comparable to non-disruptive boys (though still more elevated than non-disruptive girls). However, in interactions with their mothers, disruptive girls displayed the highest rates of disruptive behavior of any subgroup in any context, although the difference between disruptive boys and disruptive girls in this context was not statistically significant.
Conclusions
Findings suggest the importance of sex-specific conceptualizations of disruptive behavior in young children that take patterns across social contexts into account.
Keywords: Disruptive Behavior, Sex Differences, Preschool Psychopathology
As gender research pioneer Eleanor Maccoby reminds us, “social behavior…is never a function of the individual alone…. There are certain important ways in which gender is implicated in social behavior – ways that may be obscured or missed altogether when behavior is summed across all categories of social partners” (Maccoby, 1990, p. 513). Like gender,1 disruptive behavior is social in nature, occurring in a relational context; emotion and behavior regulation are learned through interactions with the social environment (Calkins & Keane, 2009). This report examines sex differences in observed disruptive behavior across interactional contexts and diagnostic status.
Normative Sex Differences in Disruptive Behavior & Social Competence
Sex differences in normative misbehavior emerge as early as 17 months of age, with boys showing more aggression than girls (Baillargeon, et al., 2007; Carter, Briggs-Gowan, Jones, & Little, 2003). This pattern continues into preschool and throughout development (Else-Quest, Hyde, Goldsmith, & Van Hulle, 2006; Keenan & Shaw, 1997). Early sex differences also emerge in children’s prosocial behavior and competencies. By early childhood, girls demonstrate more prosocial behavior, compliance, and empathy than boys (Carter, et al., 2003), another sex-differentiated pattern that continues across development (Else-Quest, et al., 2006; McClure, 2000; Zahn-Waxler, et al., 2008).
These normative sex differences in parent-reported behaviors have been replicated in observational paradigms, with girls demonstrating greater ability to regulate behavior across social context (Cole, Zahn-Waxler, & Smith, 1994). For example, in one study first grade girls were more likely than boys to mask disappointment when receiving a disappointing gift (Saarni, 1984), and in another older girls demonstrated less aggression than boys in the presence of adults, but similar rates out of adults’ view (Pepler & Craig, 1995).
Implications for sex-differentiated clinical patterns of disruptive behavior
These normative patterns of sex-differentiated aggression, regulation, and social competence have clinical parallels. Epidemiological studies consistently find higher rates of disruptive behavior disorders (DBDs) among boys than girls (Angold, et al., 2002; Briggs-Gowan, et al., 2003; Canino, et al., 2004; Costello, Mustillo, Erkanli, Keeler, & Angold, 2003) even in early school age (Carter, et al., 2010). We theorize that girls’ disruptive behavior may manifest differentially across interactional contexts, whereas boys’ disruptive behavior may be more pervasive across contexts.
Indeed, limited evidence suggests greater capacity for self-regulation across contexts in young disruptive girls (Cole, et al., 1994). Teacher- and clinician-reports of child behavior indicated that aggressive boys’ competence scores were expectedly lower than non-aggressive boys, whereas aggressive girls’ competence scores were unexpectedly higher than non-aggressive girls’ (Dodge, McClasky, & Feldman, 1985). In a study of children’s conflict and distress narratives from 4–5 through 7, boys with stable or escalating disruptive behavior displayed mostly angry themes, whereas girls with stable disruptive behavior demonstrated more prosocial themes than other groups (Zahn-Waxler, et al., 2008). Observationally, preschool girls but not boys at-risk for DBDs demonstrated more emotional expression variability depending on who was in the room (Cole, et al., 1994). Paralleling these findings, reporter discrepancies of Oppositional Defiant Disorder (ODD) are higher among girls, with teachers reporting fewer ODD symptoms among girls than boys, but parents reporting similar rates of ODD symptoms across sex (Munkvold, Lundervold, Lie, & Manger, 2009). Thus, risk for DBDs may interact with context and gender to lead to sex-differentiated presentation of disruptive behavior across contexts.
Despite evidence that girls and boys differ in social competence and disruptive behavior, the intersection of sex differences, disruptive psychopathology, and social context has not been adequately examined. Normative studies have addressed interactional context in sophisticated ways, but rarely consider disruptive behavior psychopathology (Pepler & Craig, 1995; Zahn-Waxler, et al., 2008). In turn, studies of psychopathology reporting sex differences rarely evaluate patterns across interactional contexts. Heeding Maccoby, we must be cautious summing across all categories of social partner. Moreover, with increasing evidence of the dimensionality of developmental psychopathology, it is important to understand the spectrum of disruptive behaviors and include children who may be clinically at-risk along with those with DBDs and those without disruptive behavior (Maser, et al., 2009; Pine, Cohen, Cohen, & Brook, 1999). In this paper, we used an observational paradigm to examine whether sex differences in disruptive behavior were moderated by diagnostic status (non-disruptive, at-risk, disruptive) and interactional context (parent, non-parental adult).
Methods
Participants
Mother-child dyads (n = 336) were recruited from Midwestern clinics at several university hospitals. To ensure variability, children were sampled along a behavioral continuum. Forty percent (n = 134) were recruited from referrals to a preschool behavior problems clinic. Children were also recruited from two pediatric clinics. Approximately half (n=102) were children whose parents or other adults had behavioral concerns about them, although they had not sought mental health services, and the remaining 100 were preschoolers without behavioral concerns. Screening was used for recruitment but was not the basis of classification in the study. Rather, parent report on an in depth clinical developmentally modified interview (KDBDS), teacher report on the ECI DSM-IV checklist and parent and teacher report on the CGAS impairment measure were used as the basis for the disruptive behavior classifications.”
Inclusion criteria were child age 3–5 years, living with biological mother, participation in preschool/day-care, and low income (within 250% of the U.S. poverty level). Children with developmental disability (e.g., autism) or serious medical condition (e.g., cancer) were excluded. Nine children were excluded in these analyses because of incomplete observational data (N = 327).
Most children were African-American and age was distributed relatively evenly across 3- to 5-years (see Table 1). Most mothers were unmarried (78%) and had completed high school (87%). Average annual income was $21,743 (SD $16,544).
Table 1.
Demographic Information by Sex and Disruptive Behavior Status.
| Boys | Girls | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| Non-disruptive | At-risk | Disruptive | Non-disruptive | At-risk | Disruptive | |
| (n = 82) | (n = 50) | (n = 53) | (n = 86) | (n = 39) | (n = 26) | |
| Race | ||||||
| Black | 66 (82%) | 43 (88%) | 40 (82%) | 71 (84%) | 37 (97%) | 16 (64%) |
| White | 6 (7%) | 3 (6%) | 4 (8%) | 6 (7%) | 1 (3%) | 3 (12%) |
| Multiracial | 4 (5%) | 0 (0%) | 2 (4%) | 4 (4.5%) | 0 (0%) | 4 (16%) |
| Other | 5 (6%) | 3 (6%) | 3 (6%) | 4 (4.5%) | 0 (0%) | 2 (8%) |
| Maternal Education | ||||||
| Less than High School | 11 (14%) | 6 (12%) | 7 (14%) | 8 (9%) | 7 (18%) | 5 (20%) |
| High School | 70 (86%) | 43 (88%) | 42 (86%) | 77 (91%) | 21 (82%) | 20 (80%) |
| Marital Status | ||||||
| Single | 59 (73%) | 38 (78%) | 43 (88%) | 63 (74%) | 32 (84%) | 20 (80%) |
| Married | 22 (27%) | 11 (22%) | 6 (12%) | 22 (26%) | 6 (16%) | 5 (20%) |
| Child Age | ||||||
| 3 years | 21 (24%) | 25 (51%) | 14 (29%) | 34 (40%) | 11 (29%) | 9 (36%) |
| 4 years | 33 (41%) | 10 (20%) | 12 (25%) | 24 (28%) | 15 (39%) | 11 (44%) |
| 5 years | 27 (33%) | 14 (29%) | 23 (47%) | 27 (32%) | 12 (32%) | 5 (20%) |
| Annual Income | ||||||
| Mean | 18,479 | 17,805 | 19,324 | 23,516 | 10,396 | 21,806 |
| SD | 16,403 | 16,770 | 12,616 | 17,378 | 16,080 | 17,500 |
|
|
||||||
Informed consent was obtained from mothers before the visit. All procedures were approved by two university institutional review boards.
Measures
Disruptive behavior
Observed disruptive behavior was assessed with the Disruptive Behavior Diagnostic Observational Schedule (DB-DOS; Wakschlag et al., 2008a). The DB-DOS includes “presses” for disruptive behavior (e.g., telling child it is time to clean up without a warning) across interactional contexts. Two contexts are with the examiner (examiner busy, examiner engaged) and one is with the parent (both engaged and busy). To ensure parallel engagement/disengagement across partners, the two examiner contexts were combined. Comparisons were made between child behavior with parent and with examiner. All examiners were women.
The DB-DOS is coded globally by context, with ordinal scales organized along a clinical continuum; (0 = normative behavior, 1 = normative misbehavior, 2 = of concern, 3 = atypical). Codes fall along two domains reflecting core features of DB: Problems in Behavioral Regulation (oppositional, resistant, and destructive behaviors) and Problems in Anger Modulation (difficulty regulating angry mood and behavior). In these analyses, observed disruptive behaviors from the two domains were combined because patterns were similar across the two domains. Only codes rated across both contexts were included. This measure has demonstrated good reliability (κ = .68) and validity (Wakschlag et al., 2008a; Wakschlag et al., 2008b).
Reported DB was assessed by parent and teacher report. Parents completed the Kiddie Disruptive Behavior Disorders Schedule (K-DBDS; Keenan et al., 2007), a semi-structured clinical interview assessing DSM-IV DBD symptoms in preschool children. The K-DBDs was developmentally enhanced with age-appropriate examples of behavior and assessing multiple components of behavior (Wakschlag, et al., 2008). The K-DBDS has demonstrated good reliability and validity (inter-rater reliability for diagnosis κ = 0.96, p < .0001). Teachers completed the Early Child Symptom Inventory (ECI; (Gadow & Sprafkin, 1997)), a DSM-based checklist. The ECI has demonstrated good reliability and validity in preschool samples, and internal consistency was good in this sample (Cronbach’s α = .80-.92). Parent and teacher reports of symptoms were significantly correlated (symptom r ranging from 0.20 to 0.31).
Impairment
Mothers and teachers completed the non-clinician version of the Children’s Global Assessment Scale (C-GAS; Setterberg, et al., 2001). Scores on the C-GAS range from 1–100, with scores ≤ 60 indicating impairment. Parent and teacher C-GAS scores were moderately correlated (r = .34).
Parenting
The Parenting Clinical Observation Schedule (PCOS; Hill, Maskowitz, Danis, & Wakschlag, 2008) was used to code behaviors during the parent context of the DB-DOS. PCOS codes are global, ordinal ratings assessing parenting behaviors along a continuum from competent to clinically concerning in three domains: Parental Responsive Involvement, Constructive Discipline, and Problematic Discipline. The PCOS has demonstrated good reliability and validity (in this sample, inter-rater reliability: mean κ = .61–.68).
Procedures
All procedures were approved by university institutional review boards and informed consent was obtained. The K-DBDS and DB-DOS were administered in laboratory visits. Teacher data was obtained via mailed questionnaires for 88% of children. Parents were compensated for participation.
Diagnostic status
Child diagnostic status was determined using parent and teacher report of child DB symptoms and impairment. An or rule of symptom endorsement and impairment by either informant (parent or teacher) was used (Munkvold, et al., 2009). For children missing teacher data (12%), status was based on parental report only. Resulting classification was: (1) 23% Disruptive: Met DSM-IV symptom criteria for ODD, CD and/or DBD-NOS by parent or teacher report and impaired (C-GAS ≤ 60 from informant endorsing symptoms); (2) 26% Clinically At-Risk: Did not meet symptom criteria but impaired OR have three or more symptoms but not impaired; and (3) 51% Non-Disruptive: Have two or fewer symptoms and not impaired. Groups did not vary significantly on child age or cognitive functioning, income, education or ethnicity. Mothers of children in the non-disruptive group were less likely to be single parents than mothers in other groups (χ2=12.55, p < .01). Girls and boys were equally likely to be classified as non-disruptive or at-risk, but boys were twice as likely to be classified as disruptive (χ2=5.87, p < .05).
Results
To examine whether observed disruptive behavior varied by child sex, diagnostic status and interactional context, a 2×3×2 repeated measures ANOVA was conducted with context as the repeated factor (parent, examiner), and sex and diagnostic status (disruptive, at-risk, non-disruptive) as fixed factors. Analyses revealed a significant main effect of context (F = 125.62, p < .001, partial η2 =.28), sex (F = 8.93, p = .003, partial η2 = .03), and diagnostic status (F = 17.82, p < .001, partial η2 = .10). However, main effects are interpreted in light of significant interactions, including a two-way context-by-sex interaction (F = 4.14, p = .04, partial η2 = .01) and a three-way interaction between sex, diagnostic status, and context (F = 9.81, p < .001, partial η2 = .06).
This three-way interaction between diagnostic status, child sex, and interactional context indicates that the observable disruptive behavior of girls and boys varied across interactional context depending on their diagnostic status. Further statistical decomposition was required to understand the interaction. We examined two-way interactions between: 1) diagnostic status and context within sex; and 2) context and sex within DB groups. Where these interactions were significant, pairwise contrasts were pursued (see Table 2).
Table 2.
Observed Disruptive Behavior Mean Scores (and Standard Deviations) Across Sex, Disruptive Behavior Group, and Context; see Figure 1
| Boys | Girls | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| Non-disruptive | At-risk | Disruptive | Non-disruptive | At-risk | Disruptive | |
| (n = 82) | (n = 50) | (n = 53) | (n = 86) | (n = 39) | (n = 26) | |
| Examiner | .50 (.38)1a | .57 (.43)1b | .94 (.67)1b | .35 (.28)1a | .47 (.41)1a/b | .53 (.40)1b |
| Parent | 1.01 (.56)2a | .99 (.59)2a | 1.08 (.66)1a | .65 (.49)2a | ,93 (.61)2b | 1.31 (.69) 2c |
|
|
||||||
Note. Number subscripts, which read vertically, are different when means within columns are significantly different from one another. Letter subscripts, which read horizontally, are different when means within rows are significantly different from one another. Italics are used when mean pairs are significantly different for boys and girls within the cells referencing both diagnostic status and context.
Diagnostic Status by Interactional Context Within Sex
Boys
Among boys, a repeated measures ANOVA with diagnostic status as the fixed factor and interactional context as the repeated factor was conducted. There was a main effect of context (F = 45.24, p < .001, partial η2 = .20) – boys had higher scores with parents than with examiners – and a main effect of diagnostic status (F = 6.40, p = .002, partial η2 = .07), with disruptive boys showing highest scores, followed by at-risk boys and then non-disruptive boys (ps < .05).
There was also a significant diagnostic status-by-context interaction (F = 4.51, p = .01, partial η2 = .0; see Figure 1a). As seen in Figure 1a, repeated measures ANOVAs were run across interactional contexts for disruptive; at-risk; and non-disruptive boys. For non-disruptive and at-risk boys, there was a significant main effect of context (F = 57.23, p < .001, partial η2 = .42; F = 19.04, p < .001, partial η2 = .28). Pairwise comparisons indicated that boys in the non-disruptive and at-risk groups were rated as more disruptive with parents than examiners. In contrast, disruptive boys were rated as similarly disruptive with parents and examiners (F = 1.43) (see Table 2, number subscripts).
Figure 1a.
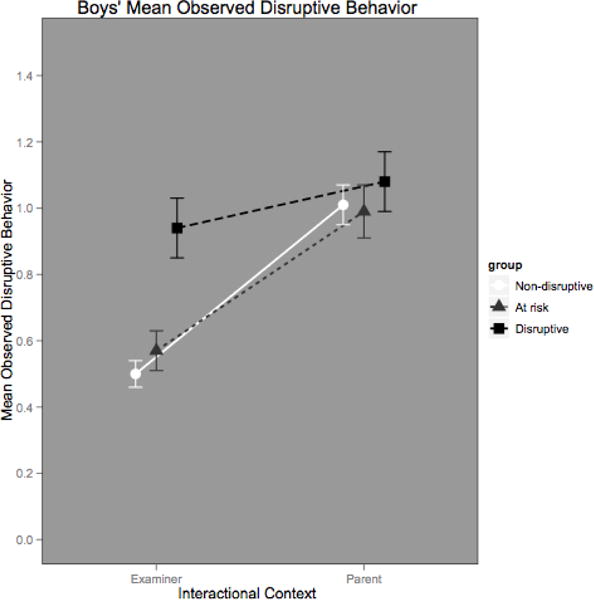
Three-Way Interaction of Sex, Diagnostic Status, and Interactional Context: Boys
Univariate ANOVAs were conducted separately for contexts with diagnostic status as the fixed factor. In the examiner context, there was a significant main effect of diagnostic status (F = 13.50, p < .001, partial η2 = .13). With examiners, disruptive boys displayed significantly higher levels of disruptive behavior than non-disruptive boys but not at-risk boys. In contrast, among boys with parents, there was no main effect of diagnostic status (F = .70; see Table 2, letter subscripts within row).
Girls
A repeated measures ANOVA with diagnostic status as the fixed factor and interactional context as the repeated factor was conducted for girls. Among girls, there was also a main effect for context (F = 90.06, p < .001, partial η2 = .38), diagnostic status (F = 14.59, p < .001, partial η2 = .17), and a diagnostic status-by-context interaction (F = 6.17, p = .003, partial η2 = .08) (See Figure 1b).
Figure 1b.
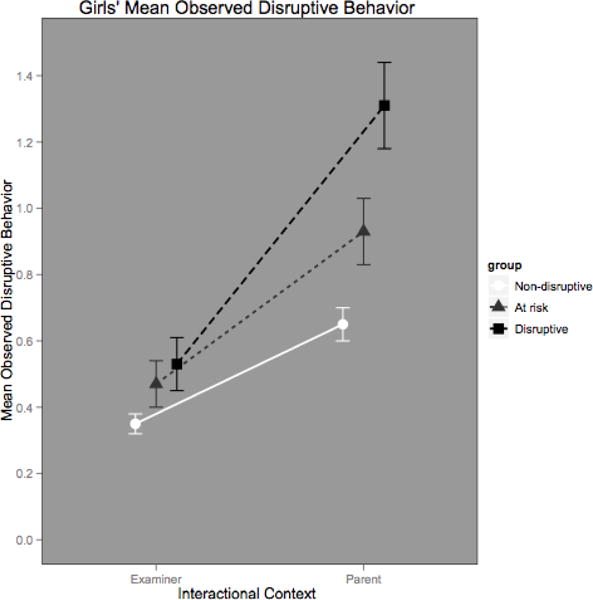
Three-Way Interaction of Child Sex, Diagnostic Status, and Interactional Context: Girls
Repeated measures ANOVAs were run across interactional context for disruptive; at-risk; and non-disruptive girls. All three DB groups evidenced a main effect of context, with girls displaying more disruptive behavior with their parents than with examiners (non-disruptive: F = 30.81, p < .001, partial η2 = .27; at-risk: F = 18.70, p < .001, partial η2 = .33; disruptive: F = 33.41, p < .001, partial η2 = .58) (see Table 2, number subscripts).
Univariate ANOVAs were conducted separately for parent and examiner contexts with diagnostic status as the fixed factor. For girls in the parent context, there was a main effect of diagnostic status (F = 14.31, p < .001, partial η2 = .16). Pairwise comparisons revealed that all three DB groups were significantly different, with at-risk girls falling between disruptive and non-disruptive girls. For girls in the examiner context, a main effect of diagnostic status was found (F = 3.78, p = .03, partial η2 = .05), with disruptive girls scoring higher than non-disruptive girls with examiners; the at-risk group was not significantly different from other groups.
Interactional Context by Sex within Diagnostic Status
Three repeated measures ANOVAs with sex as the fixed factor and interactional context as the repeated factor were run, one for each diagnostic group. Analyses revealed a significant context by sex interaction for non-disruptive (F = 5.39, p = .02, partial η2 = .03) and disruptive children (F = 10.83, p = .002, partial η2 = .13). However, there was no sex-by-context interaction or main effect of sex for at-risk children. To decompose the two-way interaction for non-disruptive and disruptive children, independent sample t-tests comparing DB ratings across sex for each interactional context were conducted. For the non-disruptive group, girls evidenced less disruptive behavior than boys in both examiner (t = 2.94, p = .004) and parent contexts (t = 4.35, p < .001). For the disruptive group, girls evidenced less disruptive behavior than boys in the examiner context (t = 2.79, p = .007), but not in the parent context (t = −1.10) (see Table 2, italics).
Post-Hoc Analyses
To ensure that variations in child behavior across interactional contexts were not merely a reflection of gendered variations in parenting, we conducted post-hoc analyses covarying PCOS observed parenting codes. Patterns of significance were similar with parenting controlled.
Discussion
The current study examined relations between child sex, diagnostic status, and interactional context to observed disruptive behavior in a sample of non-disruptive, at-risk, and disruptive preschoolers. A complex pattern of findings emerged. Preschool children’s observed disruptive behavior was moderated by both sex and diagnostic status as well as by the interactional context in which the observation occurred (examiner, parent); these patterns were not dependent on parenting.
Only disruptive boys appeared unable to regulate their behavior with a non-parental adult. Non-disruptive and at-risk boys were able to modulate their behavior with examiners but appeared indistinguishable from disruptive boys during interactions with their mothers. Indeed, disruptive boys were the only subgroup of children whose observed behavior was similar with parent and examiner. Thus, part of boys’ “disruptive” pattern appears to be the inability to modulate disruptive behavior in varying social contexts.
Girls were able to modulate their behavior with a non-parental adult, showing significantly less disruptive behavior with an examiner than with their parent. Disruptive girls demonstrated significantly more misbehavior than non-disruptive girls with an examiner, but this level of misbehavior was still less than that displayed by disruptive boys. Thus, with an examiner, disruptive girls were distinguishable within sex, but when compared to disruptive boys, they were less disruptive. Disruptive girls demonstrated significantly more disruptive behavior with their mothers; in this context, disruptive girls displayed higher rates of disruptive behavior than boys, although this difference was not statistically significant. The “disruptive” pattern for girls is context sensitive, with both disruptive and at-risk girls evidencing higher disruptive behavior with parents relative to the examiners. While the parent context was most discriminating for girls, the examiner context was most discriminating for boys.
Disruptive boys are marked by pervasive disruption across contexts, whereas disruptive girls show most context sensitivity. Whereas boys with disruptive behavior are comparably elevated in both parent and non-parent contexts – the only subgroup to look this way – girls with disruptive behavior show the greatest decrement between parent and non-parent contexts among the six groups studied.
Interestingly, boys’ mean level of disruptive behavior was quite similar regardless of their clinical status when they were interacting with their mothers. Clinical status was only salient with the examiner. This is in contrast to a large body of work documenting that clinic-referred and non-referred children can be distinguished in observations of structured parent-child interactions (e.g., Webster-Stratton, 1985). The lack of clinical differentiation in the parent condition for boys may reflect the fact that the DB-DOS was specifically designed to increase the rates of disruptive behavior by including specific presses, thereby eliciting higher rates of disruptive behavior than standard developmental paradigms. Systematic exploration of this methodologic disparity (structured tasks/play versus presses for disruptive behavior during parent-child interactions) is needed to determine optimal observational approaches for eliciting clinically meaningful differences in disruptive behavior across contexts.
Looking along levels of clinically meaningful disruptive psychopathology, at-risk boys and girls demonstrate similar patterns and rates of DB to one another, and both show sensitivity to interactional context. Our inclusion of at-risk children as a distinct group reflects our conceptualization of disruptive behavior as along a spectrum (Cole, et al., 1994; Maser, et al., 2009).
A third pattern emerged for non-disruptive boys and girls. Consistent with the normative literature, non-disruptive boys showed more DB relative to girls across both interactional contexts, but both non-disruptive boys and girls demonstrated less disruptive behavior with non-parental adults than with parents. Thus, it is among children with the most disruptive psychopathology that sex-differentiated sensitivity to interactional context becomes most apparent.
These patterns have critical implications for the contexts of diagnostic assessment, as impaired girls may not appear disruptive to a non-parent clinician using cross-sex norms for behavior. Indeed, these data suggest that a preschool girl who behaves at levels comparable to a disruptive boy outside of the home is violating sex-based expectations even among girls with DBDs.
Evidence that preschool girls with disruptive behavior problems are more likely to be disruptive with a parent than with a non-parental adult is consistent with what we know of girls’ interpersonal aggression patterns throughout the lifespan. Girls in middle childhood more often channel aggressive in close interpersonal relationships (e.g. relational aggression; Crick & Grotpeter, 1995); adolescent girls are more likely to show physical aggression towards family members, partners, or familiar females as opposed to strangers (Heide, 2003; Robbins, Monahan, & Silver, 2003). In all of these cases, the social context of interpersonal relationships serves as a conduit for girls’ aggressive behavior (Hipwell & Loeber, 2006; Munkvold et al., 2009). Alternatively, normatively higher social competence may operate as a possible protective factor for girls, whereas for boys, lower social competence and greater disruptive behaviors may lead to more entrenched and impairing disruptive behavior over time (Carter et al., 2003).
These findings also have relevance for diagnostic categories of disruptive behavior. For DSM-5, a requirement of pervasiveness for ODD has been considered (“Oppositonal Defiant Disorder: Rationale,” 2010). However, these results suggest that a requirement of pervasiveness may obscure clinically significant patterns in young girls. This may be particularly true in preschool, where close relationships may be limited to the home environment. Establishing whether this pattern is present across age periods is an important area for future research.
Strengths and Limitations
A strength of this study is the sampling, specifically in its inclusion of a large sample of young children falling along three levels of clinical severity. This conceptualization of a clinically meaningful spectrum of disruptive behavior addresses the gap in the sex differences literature that often looks only within normative or clinical populations. This sample also included a sufficient number of girls whose disruptive behavior is clinically impairing – a population that is understudied (Pardini, Frick, & Moffitt, 2010). A further strength is the direct observation of disruptive behavior across contexts.
These findings should be interpreted in light of study limitations. The generalizability of findings is limited by our predominantly low-income, African-American sample. Replication in representative samples and across age periods is essential for generalizability.
Future research could illuminate the social-emotional, cognitive, affective, and biological processes contributing to these distinct patterns. Cognitive and affective processes that may be in operation include negotiating a conflict between strong affective responses and a social role involving caring for others (Zahn-Waxler, et al., 2008) or a developing sense of self that is interdependent (Cross & Madson, 1997; Gabriel & Garnder, 1999).
Summary and Conclusions
Taken together, these patterns suggest that disruptive girls and boys demonstrate sex-differentiated sensitivity to social context, resulting in sex-typed patterns of disruptive behavior across social context that vary across clinically meaningful distinctions of disruptive behavior. For boys, elevated and impairing disruptive behavior is associated with a pervasive display of misbehavior across interactional context; for girls, it may be associated with greater flexibility or extremes of display. These findings are consistent with a framing of both disruptive behavior and gender as socially mediated and occurring within specific relational contexts (Deaux & Major, 1987). Moreover, they contradict claims that disruptive behavior in the preschool period is largely similar across boys and girls, supporting instead the need for sex-specific theories of disruptive behavior (and perhaps interventions) throughout the lifespan that take into consideration the interactional context of behavior. For preschoolers, both gender and context appear critical to understanding the distinction between typical and atypical behavior.
Footnotes
We distinguish gender and sex: “sex” refers to biologically based categories of male and female, and “gender” to the “psychological features frequently associated with these biological states” (Deaux, 1985, p. 51).
References
- Angold A, Erkanli A, Farmer E, Fairbank J, Burns B, Keeler G, et al. Psychiatric disorder, impairment, and service use in rural African American and white youth. Archives of General Psychiatry. 2002;59:893–901. doi: 10.1001/archpsyc.59.10.893. [DOI] [PubMed] [Google Scholar]
- Baillargeon R, Zoccolillo M, Keenan K, Cote S, Perusse D, Hong-Xing W, et al. Gender differences in physical aggression: A prospective population-based survey of children before and after two years of age. Developmental Psychology. 2007;43(1):13–26. doi: 10.1037/0012-1649.43.1.13. [DOI] [PubMed] [Google Scholar]
- Briggs-Gowan M, Owens P, Schwab-Stone M, Leventhal J, Leaf P, Horwitz S. Persistence of psychiatric disorders in pediatric settings. Journal of the American Academy of Child and Adolescent Psychiatry. 2003;42(11):1360–1369. doi: 10.1097/01.CHI.0000084834.67701.8a. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Keane SP. Developmental origins of early antisocial behavior. Development and Psychopathology. 2009;21:1095–1109. doi: 10.1017/S095457940999006X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Canino G, Shrout P, Rubio-Stipec M, Bird H, Bravo M, Ramirez R, et al. The DSM-IV rates of child and adolescent disorders in Puerto Rico. The Archives of General Psychiatry. 2004;61:85–93. doi: 10.1001/archpsyc.61.1.85. [DOI] [PubMed] [Google Scholar]
- Carter A, Briggs-Gowan M, Jones S, Little T. The Infant-Toddler Social and Emotional Assessment (ITSEA): Factor structure, reliability, and validity. Journal of Abnormal Child Psychology. 2003;31(5):495–514. doi: 10.1023/a:1025449031360. [DOI] [PubMed] [Google Scholar]
- Carter A, Wagmillier R, Gray S, McCarthy K, Horwitz S, Briggs-Gowan M. Prevalence of DSM-IV disorder in a representative, healthy birth cohort at school entry: Sociodemograhic risks and social adaptation. Journal of the American Academy of Child & Adolescent Psychiatry. 2010;49(7):686–698. doi: 10.1016/j.jaac.2010.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole P, Zahn-Waxler C, Smith K. Expressive control during a disappointment: Variations related to preschoolers’ behavior problems. Developmental Psychology. 1994;30:835–846. [Google Scholar]
- Costello E, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Archives of General Psychiatry. 2003;60(8):837–844. doi: 10.1001/archpsyc.60.8.837. [DOI] [PubMed] [Google Scholar]
- Cross S, Madson L. Models of the self: Self-construals and gender. Psychological Bulletin. 1997;122(1):5–37. doi: 10.1037/0033-2909.122.1.5. [DOI] [PubMed] [Google Scholar]
- Deaux K, Major B. Putting gender into context: An interactive model of gender-related behavior. Psychological Review. 1987;94(3):369–389. [Google Scholar]
- Dodge K, McClasky C, Feldman E. Situational approach to the assessment of social competence in children. 1985;53(3):344–353. doi: 10.1037//0022-006x.53.3.344. [DOI] [PubMed] [Google Scholar]
- Else-Quest N, Hyde J, Goldsmith H, Van Hulle C. Gender differences in temperament: A meta-analysis. Psychological Bulletin. 2006;132(1):33–72. doi: 10.1037/0033-2909.132.1.33. [DOI] [PubMed] [Google Scholar]
- Gabriel S, Garnder W. Are there ‘his’ and ‘hers’ types of interdependence? The immplications of gender differences in collective versus relational interdependdence for affect, behavior, and cognition. Journal of Personality and Social Psychology. 1999;77(3):642–655. [Google Scholar]
- Gadow K, Sprafkin J. Early Child Inventory: Norms Manual. Stony Brook, NY: Checkmate Plus; 1997. [Google Scholar]
- Heide K. Youth homicide: A review of the literature and a blueprint for action. International Journal of Offender Therapy and Comparative Criminology. 2003;47(6):6–36. doi: 10.1177/0306624X02239272. [DOI] [PubMed] [Google Scholar]
- Hipwell A, Loeber R. Do we know which interventions are effective for disruptive and delinquent girls? Clinical Child and Family Psychology Review. 2006;9(3/4):221–255. doi: 10.1007/s10567-006-0012-2. [DOI] [PubMed] [Google Scholar]
- Hill C, Maskowitz K, Danis B, Wakschlag LS. Validation of a clinically sensitive observational coding system for parenting behaviors: The Parenting Clinical Observation Schedule. Parenting: Science & Practice. 2008;8:153–185. doi: 10.1080/15295190802045469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keenan K, Shaw D. Developmental and social influences on young girls’ early problem behavior. Psychological Bulletin. 1997;121(1):95–113. doi: 10.1037/0033-2909.121.1.95. [DOI] [PubMed] [Google Scholar]
- Maccoby E. Gender and relationships: A developmental account. American Psychologist. 1990;45(4):513–520. doi: 10.1037//0003-066x.45.4.513. [DOI] [PubMed] [Google Scholar]
- Maser J, Norman S, Zisook S, Erverall L, Stein M, Schettler P, et al. Psychiatric nosology is ready for a paradigm shift in DSM V. Clinical Psychology: Science and Practice. 2009;16:24–40. [Google Scholar]
- McClure E. A meta-analytic review of sex differences in facial expression processing and their development in infants, children, and adolescents. Psychological Bulletin. 2000;126(3):424–453. doi: 10.1037/0033-2909.126.3.424. [DOI] [PubMed] [Google Scholar]
- Munkvold L, Lundervold A, Lie S, Manger T. Should there be separate parent and teacher-based categories of ODD? Evidence from a general population. Journal of Child Psychology and Psychiatry. 2009;50(10):1264–1272. doi: 10.1111/j.1469-7610.2009.02091.x. [DOI] [PubMed] [Google Scholar]
- Oppositonal Defiant Disorder: Rationale. 2010 2010, from http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=106#.
- Pardini D, Frick P, Moffitt T. Building an evidence base for DSM-5 conceptualizations of oppositional defiant disorder and conduct disorder: Introduction to special section. Journal of Abnormal Psychology. 2010;119(4):683–688. doi: 10.1037/a0021441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pepler D, Craig W. A peek behind the fence: Naturalistic observations of aggressive children with remote audiovisual recording. Developmental Psychology. 1995;31(4):548–553. [Google Scholar]
- Pine D, Cohen E, Cohen P, Brook J. Adolescent depressive symptoms as predictors of adult depression: Moodiness or mood disorder? American Journal of Psychiatry. 1999;156:133–135. doi: 10.1176/ajp.156.1.133. [DOI] [PubMed] [Google Scholar]
- Robbins P, Monahan J, Silver E. Mental disorder, violence, and gender. Law and Human Behavior. 2003;27(6):561–571. doi: 10.1023/b:lahu.0000004886.13268.f2. [DOI] [PubMed] [Google Scholar]
- Saarni C. An observational study of children’s attempts to monitor their expressive behavior. Child Development. 1984;55:1504–1513. [Google Scholar]
- Setterberg S, Bird H, Gould M, Saffer D, Fisher P. Parent and intervewer versions of the Children’s Global Assessment Scale. New York: Columbia University; 2001. [Google Scholar]
- Wakschlag L, Hill C, Carter A, Danis B, Egger H, Keenan K, et al. Observational assessment of preschool disruptive behavior, part 1: Reliability of the Disruptive Behavior Diagnostic Observation Schedule (DB-DOS) Journal of the American Academy of Child & Adolescent Psychiatry. 2008a;47(6):622–631. doi: 10.1097/CHI.0b013e31816c5bdb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wakschlag L, Briggs-Gowan M, Hill C, Danis B, Leventhal B, Keenan K, et al. Observational assessment of the preschool disruptive behavior, part II: Validity of the Disruptive Behavior Diagnostic Observation Schedule (DB-DOS) Journal of the American Academy of Child & Adolescent Psychiatry. 2008b;47(6):632–641. doi: 10.1097/CHI.0b013e31816c5c10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webster-Stratton C. Mother perceptions and mother-child interactions: Comparisons of a clinic-referred and a nonclinic group. Journal of Clinical Child Psychology. 1985;14(4):334–339. [Google Scholar]
- Zahn-Waxler C, Park J, Usher B, Belouad F, Cole P, Gruber R. Young children’s representations of conflict and distress: A longitudinal study of boys and girls with disruptive behavior problems. Development and Psychopathology. 2008;20:99–119. doi: 10.1017/S0954579408000059. [DOI] [PubMed] [Google Scholar]