

Abstract
Background: Bilateral vocal fold paralysis can result in shortness of breath and severe dyspnea which can be life-threatening. Patients and Methods: Thirty-five patients with bilateral vocal fold paralysis who underwent endo-extralaryngeal laterofixation according to Lichtenberger were retrospectively analyzed regarding etiology, symptoms, treatment and complications. Results: In 27 patients, laterofixation of the vocal cord alone was performed. Eight patients underwent laterofixation and additional posterior chordectomy of the opposite vocal cord according to Dennis and Kashima. The time of intervention ranged from 1 day to 38 years after the onset of bilateral vocal cord immobility. The intraoperative course was uneventful in all patients. None of the patients had postoperative aspiration. Postoperative voice function was acceptable in all patients. Complications of suture laterofixation were laryngeal edema, formation of fibrin, and malposition of the suture. Conclusion: Laterofixation of the vocal cords according to Lichtenberger is a safe and easy method that can be used as a first-stage treatment of vocal cord paralysis.
Keywords: Laterofixation, vocal fold immobility, vocal fold paralysis, recurrent laryngeal nerve paralysis, dyspnea
Bilateral vocal fold immobility can be caused by iatrogenic injury during thyroid, neck and thoracic surgery, malignancies and their therapy, neurological disorders, infection and trauma (1-5). However, iatrogenic injury by thyroid surgery is the most common cause (6). While unilateral vocal fold paralysis typically results in hoarseness, bilateral vocal fold paralysis can result in shortness of breath and severe dyspnea which can be life-threatening. The diagnosis of bilateral vocal fold paralysis is made by laryngoscopy. There are temporary reversible and permanent methods to treat patients with bilateral vocal cord paralysis. Intubation is an emergency procedure, however, some form of treatment has to follow. For the planning of further treatment, the prognosis of nerve damage is primarily important. Even for mild lesions of the recurrent nerve after thyroid surgery, regeneration of vocal cord function may require months.
There are many surgical techniques for laryngeal airway enlargement in patients with bilateral vocal fold immobility (7,8). Reconstructive procedures should be the treatments of choice, while destructive procedures should be chosen only if the recovery of nerve function is no longer to be expected. One reversible minimally invasive method to avoid tracheotomy is endo-extralaryngeal suture laterofixation of the vocal fold according to Lichtenberger (9). By lateralization of one vocal fold, the glottis is widened and an adequate airway can be restored. In 1983, Lichtenberger described the procedure using a newly developed endo-extralaryngeal needle carrier which enables a translaryngeal needle to be introduced within the larynx. Due to the reversibility of the procedure, it can be performed without delay without the need to wait for functional recovery of the recurrent nerve. However, patients must be informed that deterioration of the voice is common after this procedure.
The aim of this study was to retrospectively analyze clinical data of patients who were treated by endo-extralaryngeal suture lateralization of the vocal folds.
Patients and Methods
The data of all patients with bilateral vocal cord paralysis who underwent suture laterofixation of one vocal cord according to Lichtenberger from 2004 to 2014 in our Department, were evaluated. The patient charts were retrospectively examined for sex, age, etiology of vocal cord paralysis, symptoms and complications.
Laryngoscopy was used to assess bilateral vocal fold immobility. Laterofixation was indicated in patients with dyspnea and bilateral vocal fold immobility, or vocal fold paralysis of one vocal fold and reduced vocal fold movement of the other side.
All procedures were performed under general anesthesia. Lateralization was performed on the less mobile vocal cord. Patients were placed supine with their neck overextended. The entire glottis was exposed with an operation laryngoscope. One end of a 2-0 Prolene thread was loaded into a curved needle which was inserted into a Lichtenberger laryngeal needle holder. The laryngeal needle holder was introduced via the laryngoscope and passed below the vocal fold and then pierced through the mucosa, cartilage, and neck skin. Then the needle was retrieved and the procedure was repeated above the vocal fold using the same thread. Afterwards, an incision of approximately 1 cm was made between the ends of the thread, the thread was knotted subcutaneously and the skin incision was closed. In most cases, two suture loops were performed, one in the posterior third of the vocal fold and the other approximately 0.5 cm ventrally.
Results
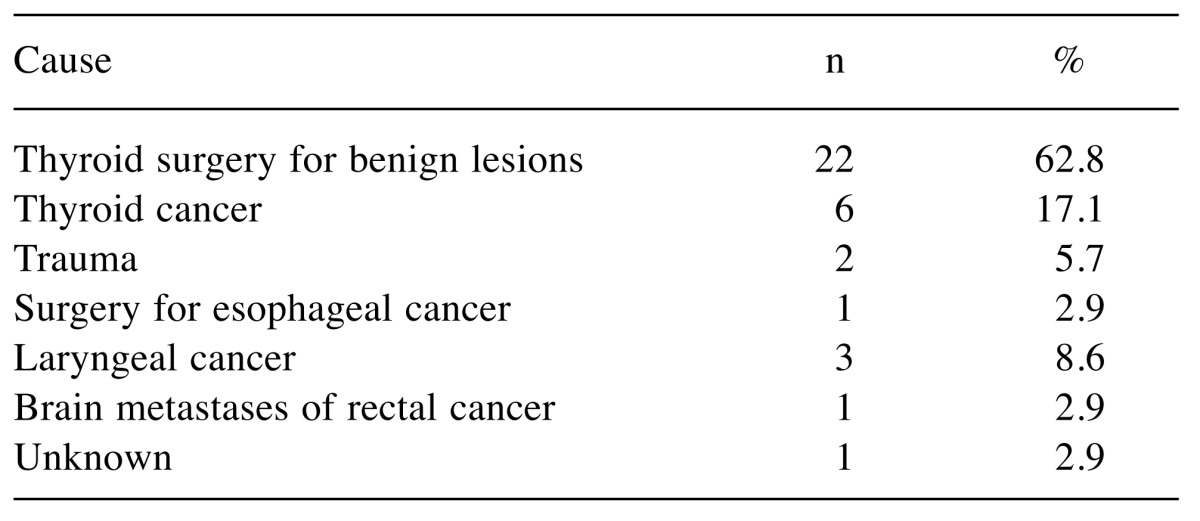
Thirty-five patients with bilateral vocal fold immobility were analyzed, 13 males and 22 females. The average age at presentation was 64.0 years (range=41-88 years). The most frequent reason for vocal fold immobility was thyroid gland surgery for benign lesions (62.8%); other causes are included in Table I. All patients presented with dyspnea. In some patients, dyspnea appeared immediately after the onset of vocal fold paralysis, in other patients it appeared months or years later; often due to infections of the upper respiratory tract leading to edema of the narrow glottic space. At presentation at our Department, three patients had tracheostomy and two patients were intubated. In two further cases, a tracheostomy and plastic tracheostomy closure had been performed before presentation at our Department.
Table I. Causes of vocal fold immobility.
In 27 patients, laterofixation of the vocal cord was solely performed. Eight patients had laterofixation and additional posterior chordectomy of the opposite vocal cord according to Dennis and Kashima (10). In all of these patients, bilateral vocal cord immobility had persisted for more than 6 years before the operation at our Department.
In 13 cases the right vocal cord was lateralized and in 22 cases the left vocal cord. The earliest intervention was performed 1 day after the onset of bilateral vocal cord immobility, the latest intervention 38 years after occurrence of bilateral vocal cord immobility due to thyroid surgery in a patient with acute respiratory failure through a respiratory infection.
The intraoperative course was uneventful in all patients. None of the patients had postoperative aspiration. Postoperative voice function was acceptable in all patients. The postoperative respiratory function was adequate for daily routine activities such as walking and climbing stairs.
The most frequent complication of suture laterofixation of the vocal cord was laryngeal edema, which appeared in six patients, on average after 2 days. Edema was treated by intravenous steroids and inhalations. In one patient, one thread had to be removed due to malposition of the thread towards the epiglottis and in one other patient a loosened thread has to be refixed. One further complication met after the operation was the formation of fibrin on the vocal fold that reduced the glottis space in three patients and made removal of fibrin under anesthesia necessary.
In three patients with malignant diseases, a tracheostomy was performed in the further course of disease due to progression of cancer which led to narrowing of the airway with severe dyspnea. In one patient, a tracheal stent was inserted due to progression of thyroid cancer into the trachea.
In three patients, after thyroid surgery for benign lesions, functional recovery of the recurrent nerve occurred and the threads were removed. In two further patients without functional recovery, a posterior chordectomy according to Dennis and Kashima (10) was performed. Three patients who presented with a tracheotomy before laterofixation were successfully decannulated and a plastic tracheotomy closure was performed.
Discussion
Thyroid surgery is the most common cause for bilateral vocal cord immobility (6). This was confirmed by the present study. When bilateral immobility of the vocal folds arises during thyroid surgery, only in rare cases is extubation impossible and therefore patients have to stay intubated or immediate tracheotomy is required. In most patients, extubation is possible and they can breathe sufficiently at rest and at low exercise. However, even in mild lesions of the recurrent nerve after thyroid surgery, regeneration of vocal cord function may require months. Whilst vocal cord function is not recovered, there is a high risk for patients that dyspnea worsens through infections of the upper respiratory tract leading to edema of the narrow glottic space. Moreover, physical exertion is usually not possible in patients with bilateral vocal fold immobility.
Especially in patients with acute respiratory failure, prompt diagnosis followed by adequate treatment is mandatory. In acute life-threatening situations, the patient should be intubated to re-establish a patent airway. Although a tracheotomy can also be avoided by other methods such as arytenoidectomy or chordectomy, due to its reversibility, the suture laterofixation technique is of particular importance in selected patients (11). In iatrogenic injury of the recurrent nerve, a spontaneous recovery of vocal fold function can be anticipated in several patients if the recurrent nerve was not transected. Once the nerve function has been recovered, the laterofixation of the vocal fold can be reversed. However, like all operative techniques improving the airway, laterofixation may worsen glottic sphincter function and voice quality, but has a lower risk of postoperative adverse events (12). Therefore, appropriate preoperative patient selection is crucial.
Deterioration of voice is not a real complication but an expected side-effect of laterofixation. Voice impairment also occurred in all patients of this study; however, postoperative voice function was acceptable in all patients. Aspiration is described after laterofixation in some studies (13-15) but not in others (16-18) and was not experienced in the patient cohort analyzed here.
In our patient cohort, postoperative edema of the mucosa was the most common complication after laterofixation, which was also seen in other studies to a greater or lesser degree (19,20). Patients with significant edema ought to be treated with steroids intravenously and inhalations, and may be admitted to the Intensive Care Unit for surveillance. In the postoperative period, edema can make immediate re-intubation necessary. However, this was not necessary in the analyzed patient cohort.
The formation of fibrin is common after laser surgery of the larynx and occurred predominately in patients who were treated by laterofixation of one vocal fold and posterior chordectomy according to Dennis and Kashima of the other vocal fold. In these patients, airway obstruction by fibrin can lead to dyspnea, which can be resolved by removal of fibrin in most cases.
The recovery of vocal fold function can be identified by laryngoscopy even in patients with laterofixation sutures in situ. In these cases, the sutures can be cut subcutaneously and removed. In patients without recovery of vocal fold function, definitive surgery such as posterior chordectomy according to Dennis and Kashima can be performed or the sutures of laterofixation can be left (12).
There are some limitations to our study. The first and most obvious is that it consists of a relatively small number of patients. The retrospective nature of the study moreover makes accurate long-term analysis difficult.
Conclusion
Bilateral vocal fold palsy leads to reduction of the glottic space, which can lead to acute respiratory failure or to persistent dyspnea that worsens with physical exercise and infection of the neck area. Laterofixation of the vocal cords according to Lichtenberger is a safe method which can be used as a first-stage treatment of vocal cords paralysis. However, complications may occur which make a treatment with steroids or second operation necessary. In some cases, laterofixation according to Lichtenberger does not lead to adequate respiratory function and has to be completed with other surgical methods.
References
- 1.Taha H, Irfan S, Krishnamurthy M. Cisplatin induced reversible bilateral vocal cord paralysis: an undescribed complication of cisplatin. Head Neck. 1999;21:78–79. doi: 10.1002/(sici)1097-0347(199901)21:1<78::aid-hed11>3.0.co;2-7. [DOI] [PubMed] [Google Scholar]
- 2.Praveen CV, De Lord CF. Bilateral vocal fold paralysis following treatment with vincristine. J Laryngol Otol. 2006;120:423. doi: 10.1017/S0022215106001022. [DOI] [PubMed] [Google Scholar]
- 3.Reiter R, Hoffmann TK, Rotter N, Pickhard A, Scheithauer MO, Brosch S. Etiology, diagnosis, differential diagnosis and therapy of vocal fold paralysis. Laryngorhinootologie. 2014;63:161–173. doi: 10.1055/s-0033-1355373. [DOI] [PubMed] [Google Scholar]
- 4.Crawley BK, Sulica L. Vocal fold paralysis as a delayed consequence of neck and chest radiotherapy. Otolaryngol Head Neck Surg. 2015;153:239–243. doi: 10.1177/0194599815583476. [DOI] [PubMed] [Google Scholar]
- 5.Holinger LD, Holinger PC, Holinger PH. Etiology of bilateral abductor vocal cord paralysis: a review of 389 cases. Ann Otol Rhinol Laryngol. 1976;85:428–436. doi: 10.1177/000348947608500402. [DOI] [PubMed] [Google Scholar]
- 6.Rosenthal LH, Benninger MS, Deeb RH. Vocal fold immobility: a longitudinal analysis of etiology over 20 years. Laryngoscope. 2007;117:1864–1870. doi: 10.1097/MLG.0b013e3180de4d49. [DOI] [PubMed] [Google Scholar]
- 7.Sapundzhiev N, Lichtenberger G, Eckel HE, Friedrich G, Zenev I, Toohill RJ, Werner JA. Surgery of adult bilateral vocal fold paralysis in adduction: history and trends. Eur Arch Otorhinolaryngol. 2008;265:1501–1514. doi: 10.1007/s00405-008-0665-1. [DOI] [PubMed] [Google Scholar]
- 8.Lichtenberger G. Comparison of endoscopic glottis-dilating operations. Eur Arch Otorhinolaryngol. 2003;260:57–61. doi: 10.1007/s00405-002-0505-7. [DOI] [PubMed] [Google Scholar]
- 9.Lichtenberger G. Endo-extralaryngeal needle carrier instrument. Laryngoscope. 1983;93:1348–1350. doi: 10.1002/lary.1983.93.10.1348. [DOI] [PubMed] [Google Scholar]
- 10.Dennis DP, Kashima H. Carbon dioxide laser posterior cordectomy for treatment of bilateral vocal cord paralysis. Ann Otol Rhinol Laryngol. 1989;98:930–934. doi: 10.1177/000348948909801203. [DOI] [PubMed] [Google Scholar]
- 11.Damrose EJ. Suture laterofixation of the vocal fold for bilateral vocal fold immobility. Curr Opin Otolaryngol Head Neck Surg. 2011;19:416–421. doi: 10.1097/MOO.0b013e32834c7d15. [DOI] [PubMed] [Google Scholar]
- 12.Nawka T, Sittel C, Gugatschka M, Arens C, Lang-Roth R, Wittekindt C, Hagen R, Muller AH, Volk GF, Guntinas-Lichius O. Permanent transoral surgery of bilateral vocal fold paralysis: A prospective multi-center trial. Laryngoscope. 2015;125:1401–1408. doi: 10.1002/lary.25137. [DOI] [PubMed] [Google Scholar]
- 13.Rovo L, Jori J, Brzozka M, Czigner J. Airway complication after thyroid surgery: minimally invasive management of bilateral recurrent nerve injury. Laryngoscope. 2000;110:140–144. doi: 10.1097/00005537-200001000-00025. [DOI] [PubMed] [Google Scholar]
- 14.Rovo L, Jori J, Ivan L, Brzozka M, Czigner J. ‘Early’ vocal cord laterofixation for the treatment of bilateral vocal cord immobility. Eur Arch Otorhinolaryngol. 2001;258:509–513. doi: 10.1007/s004050100378. [DOI] [PubMed] [Google Scholar]
- 15.Motoyoshi K, Yumoto E, Hyodo M, Kadota Y, Hinohira Y. Laterofixation of the vocal cord by Ejnell’s operation for bilateral vocal cord paralysis. Nihon Jibiinkoka Gakkai Kaiho. 1998;101:1057–1061. doi: 10.3950/jibiinkoka.101.9_1057. [DOI] [PubMed] [Google Scholar]
- 16.Geterud A, Ejnell H, Stenborg R, Bake B. Long-term results with a simple surgical treatment of bilateral vocal cord paralysis. Laryngoscope. 1990;100:1005–1008. doi: 10.1288/00005537-199009000-00016. [DOI] [PubMed] [Google Scholar]
- 17.Ejnell H, Mansson I, Hallen O, Bake B, Stenborg R, Lindstrom J. A simple operation for bilateral vocal cord paralysis. Laryngoscope. 1984;94:954–958. doi: 10.1288/00005537-198407000-00018. [DOI] [PubMed] [Google Scholar]
- 18.Hyodo M, Nishikubo K, Motoyoshi K. Laterofixation of the vocal fold using an endo-extralaryngeal needle carrier for bilateral vocal fold paralysis. Auris Nasus Larynx. 2009;36:181–186. doi: 10.1016/j.anl.2008.04.002. [DOI] [PubMed] [Google Scholar]
- 19.Jovic RM, Mitrovic S, Janjevic D, Dragicevic D, Canji K. Difficulties and complications of using endo-extralaryngeal laterofixation of vocal cords in bilateral recurrent laryngeal nerve palsy. Med Pregl. 2008;61(Suppl 2):51–56. [PubMed] [Google Scholar]
- 20.Korkmaz MH, Bayir O, Cadalli Tatar E, Saylam G, Ocal B, Keseroglu K, Ozdek A. Glottic airway gain after ‘suture arytenoid laterofixation’ in bilateral vocal cord paralysis. Acta Otolaryngol. 2015;135:931–936. doi: 10.3109/00016489.2015.1042554. [DOI] [PubMed] [Google Scholar]