

Abstract
Background
Periostin (PN) epithelial and stromal overexpression in tumor pathology has been studied according to tumor growth, angiogenesis, invasiveness, and metastasis, but a limited number of studies address PN in thyroid tumors.
Aim
Our study aimed to analyze PN expression in different histological variants of PTC and to correlate its expression with the clinicopathological prognostic factors.
Material and Methods
PN expression has been immunohistochemically assessed in 50 cases of PTC (conventional, follicular, oncocytic, macrofollicular, and tall cell variants), in tumor epithelial cells and intratumoral stroma. The association between PN expression and clinicopathological characteristics has been evaluated.
Results
Our results show that PTC presented different patterns of PN immunoreaction, stromal PN being significantly associated with advanced tumor stage and extrathyroidal extension. No correlations were found between PN overexpression in tumor epithelial cells and clinicopathological features, except for specific histological variants, the highest risk of poor outcome being registered for the conventional subtype in comparison to the oncocytic type.
Conclusions
Our study demonstrates differences in PN expression in histological subtypes of PTC. Our results plead in favor of a dominant protumorigenic role of stromal PN, while the action of epithelial PN is less noticeable.
1. Introduction
Thyroid cancer represents less than 1% of total number of cancers, but during the last decades its incidence has been continuously growing, showing a dominant involvement of female sex and of young and medium ages [1]. Papillary thyroid carcinoma (PTC) is the most common histological type. Diagnosed in approximate 85% of cases [2], this histological type has a relatively good prognosis, distant metastases, and death being rare events.
Classically, the prognostic assessment of PTC relies, according to the WHO, on the following standard clinical and morphological factors: patients' age and sex, tumor size, histological variant, extrathyroidal extension, completeness of surgical resection, and occurrence of distant metastasis [1].
Tremendous progress has been made by genomics, transcriptomics, and proteomics in all types of cancers, including PTC, resulting in a switch over from traditional clinicopathological prognosis factors to new molecular prognosis markers.
The current trend in thyroid tumor pathology is to improve the grading framework by implementation of new molecular and genetic criteria that could explain the differences between the biological behaviors, quantified by low versus high PTC aggressiveness. Consequently, a large series of molecular markers have been investigated, but none of them has been yet validated and thus they are still considered as candidate prognosis factors. Therefore this issue is remaining a source of heated debate.
As a component of the cellular matrix, periostin (PN) has been recently included in the list of putative prognostic markers. PN is a cellular adhesion molecule, initially identified within the osteoblastic cellular line in mice [3] and named according its identification in periosteum and periodontal ligamentum [4].
PN is secreted by fibroblasts [5–7] and belongs to fasciclin-I family of proteins, functioning in cell-cell and cell-extracellular matrix (ECM) interactions. It is located in fetal and normal adult organs, such as embryonic periosteum, placenta, heart valves, thyroid, adrenal glands, lung, stomach, colon, testicle, prostate, vagina, ovary, breast, and periodontal ligamentum [8–11].
PN epithelial and stromal overexpression in tumor pathology has been studied according to tumor growth, angiogenesis, invasiveness, and metastasis [10–14]. The published data are relatively limited but nevertheless they are supporting PN involvement in tumor progression in different locations, such oral [15] and head and neck carcinomas [16, 17], breast cancer [18–23], ovarian cancer [8, 12, 24–26], prostate cancer [27–30], renal cell carcinoma [31–33], pancreatic carcinoma [34, 35], stomach [36–38], colon [39, 40] and hepatocellular carcinoma [13, 41, 42], non-small-cell lung carcinoma [43–46], malignant pleural mesothelioma [47], neuroblastoma [48], glioblastoma [49–51], and its association with aggressive phenotypes and poor prognosis [7, 10, 13, 14].
To the best of our knowledge, PN expression in thyroid tumors is scarcely reported in the mainstream publications.
Within this context, the present study aims to analyze PN expression in different histological variants of PTC and to correlate its expression with the clinicopathological prognostic factors.
2. Material and Method
2.1. Patients and Tissues
The study group is comprised of 50 patients diagnosed with PTC in “Sf. Spiridon” County Clinical Emergency Hospital and surgically treated by thyroidectomy with cervical lymph node dissection.
The clinicopathological features have been retrospectively documented from the medical files and included the following data: sex, age (<45 and ≥45 years old, resp.), tumor size, multifocality (number of foci), lymphovascular invasion, extrathyroidal extension (defined as microscopic presence of tumor cells beyond the thyroid capsule, into adipose tissue, skeletal muscle, or sizable vessels and nerves), lymph node metastasis, and tumor stages according to TNM and American Joint Committee on Cancer staging system [52].
All cases have been reassessed by two independent pathologists in order to identify the histological variant of PTC and to confirm the associated thyroid pathology.
The study has been approved by the Ethics Committee of “Grigore T. Popa” University of Medicine and Pharmacy Iasi, complying with the ethical standards of Helsinki declaration that require the patients' informed consent on the usage of their biologic material.
2.2. Immunohistochemistry
For each case, a representative paraffin-embedded block has been chosen, and 3 μm sections have been cut and have been displayed on electrostatically charged polylysine-coated slides.
Tissue samples were dewaxed in xylene and rehydrated in 3 baths of alcohol with progressive decreasing concentrations. Heat induced epitope retrieval technique was used for antigen retrieval. The slides were immersed in sodium citrate pH 6 and boiled in water bath at 98°C for 30 minutes. After cooling at room temperature and inhibition of endogenous peroxidase activity, the samples have been incubated with anti-periostin polyclonal antibody (Santa Cruz, Biotechnology Inc., Santa Cruz, USA) dilution 1 : 100, overnight at 4°C. Immunoreaction has been amplified with the suitable secondary and tertiary antibodies of the LSAB-HRP complex (Dako, Carpinteria, USA) and developed with 3,3′-diaminobenzidine tetrahydrochloride chromogen (DakoCytomation, Carpinteria, USA); the positive reaction has been considered in the presence of a brown cytoplasmic stain. Positive and negative controls have been simultaneously run.
2.3. Semiquantitative Assessment
PN expression has been separately assessed in tumor epithelial cells and in intratumoral stroma, using adapted semiquantitative scores based on literature reports [25, 53, 54]. The corresponding nontumoral thyroid tissue within each PTC specimen has been constantly evaluated. This step allowed us to establish the basal level of thyroid tissue PN immunoreaction, considering the staining of the follicular cells within these areas as absent or weak (+). We have evaluated the staining intensity in the tumor cellular component – I (0 when absent, 1 for weak (+), 2 for moderate (++), and 3 for strong (+++) intensity, resp.) and percentage of positive tumor cells – P (0 for <10%, 1 for 10–30%, 2 for 30–60%, and 3 for >60% positive cells, resp.). The final score has been obtained as a sum between I and P, with a minimum value of 0 and a maximum one of 6. We have considered the values between 0 and 3 as low score (corresponding to PN negative or weak expression) and those between 4 and 6 as high score (revealing a high PN expression). The stromal PN reaction has been quantified as 0 for no staining or less than 5% and 1 for >5% of positive intratumoral stroma, respectively.
2.4. Statistical Analysis
Statistical analysis has been performed by GraphPad Prism software package (GraphPad Software, San Diego, CA, USA). The association between PN expression and clinicopathological characteristics has been analyzed by applying the χ2 test, whereas odds ratios (ORs) using logistic regression have been calculated to assess the correlation between PN and outcome variables for tumor aggressiveness. Statistically significant results have been considered when p < 0.05.
3. Results
3.1. Clinicopathological Characteristics
A predominant female sex was observed in our study group, 41 cases (82.0%), compared to male sex, 9 cases (18.5%). The mean age at diagnosis was 48.24 ± 14.70 years (range 19–76 years), 42.0% (21 patients) being diagnosed at young age, under 45 years. Mean tumor size was 2.18 ± 1.36 cm (range 1.1–7.5 cm). Multifocality was present in 34 cases (68%). We noted lymphovascular invasion in 14 cases (28%), extrathyroidal extension in 23 cases (46.0%), and lymph node metastasis in 7 cases (14%).
Based on TNM and AJCC criteria, the cases were staged as follows: 18 cases (36%), stage I, 6 cases (12%), stage II, 25 cases (50%), stage III, and 1 case (2%), stage IV.
Histologically, there were 10 cases (20%) diagnosed as conventional PTC and 40 cases (80%) as other variants of PTC (follicular, 21 cases (42%), oncocytic, 8 cases (16%), macrofollicular, 7 cases (14%), and tall cell, 4 cases (8%)).
3.2. PN Expression
3.2.1. Qualitative Assessment
PN immunopositivity has been noticed in both tumor cells and intratumoral stroma.
PN expression exhibited a predominantly cytoplasmic, perinuclear, finely granular pattern, in tumor cells. The distribution was predominantly homogenous, though some heterogenous areas were focally identified. The reaction intensity was predominantly moderate or strong.
The histological variants of PTC showed different patterns of PN immunoreaction. The immunoexpression was diffusely cytoplasmic, with weak apical or basal polarization, in conventional (Figure 1), follicular, and macrofollicular (Figure 2) variants. The tall cell variant was characterized by localized immunoexpression, with predominantly apical distribution, along with focal infranuclear positivity (Figure 3). The immunoreaction was predominantly negative or very weak in oncocytic variant (Figure 4).
Figure 1.
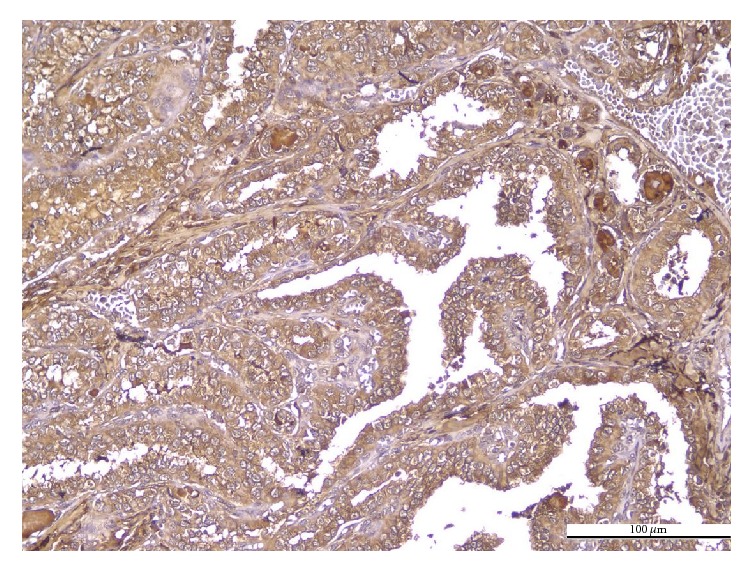
Conventional PTC. Positive PN in tumor cells: diffuse cytoplasmic positive immunoreaction of moderate intensity; negative PN in intratumoral stroma (IHC anti-PN, ×200).
Figure 2.
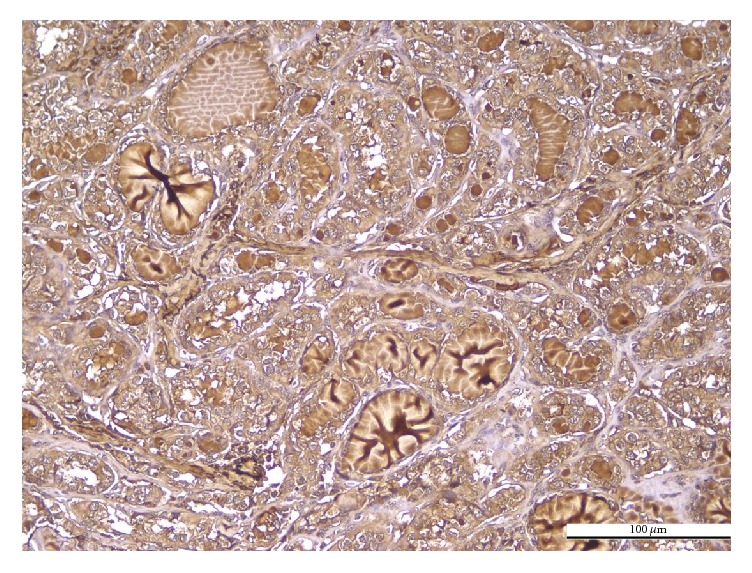
Macrofollicular PTC. Positive PN in tumor cells: diffuse cytoplasmic immunoreaction of moderate intensity; negative PN in intratumoral stroma (IHC anti-PN, ×200).
Figure 3.
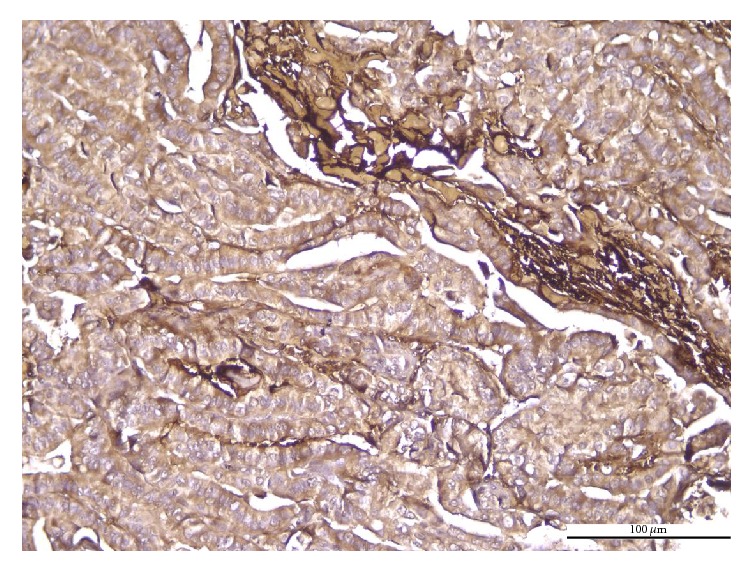
Tall cell PTC. Positive cytoplasmic PN, exhibiting focal apical and basal immunoreaction of moderate intensity; positive PN in intratumoral stroma (IHC anti-PN, ×200).
Figure 4.
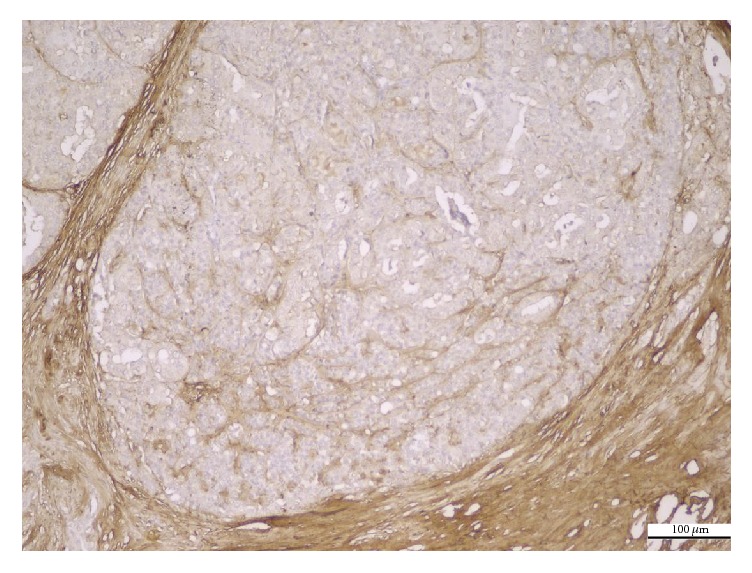
Oncocytic PTC. Negative PN expression in tumor epithelial cells and positive PN expression in tumor stroma (IHC anti-PN, ×200).
The intratumoral stromal PN expression was variable within the histological variants of PTC, from strong positivity in fibroblasts and collagen fibers up to lack of expression.
PN expression has been negative or weak, exhibiting a homogenous and diffuse cytoplasmic distribution in the follicular cells of nonneoplastic thyroid tissue.
3.2.2. Semiquantitative Assessment
Tumor cells' PN expression has been evaluated as low score in 14 cases (28.0%) and with high score in 36 cases (72.0%) (Table 1). Intratumoral stroma exhibited PN negativity or weak expression in 16 cases (32.0%), whereas the other 34 cases (68%) showed PN strong positivity (Table 2).
Table 1.
PN expression in tumor epithelial cells and clinicopathological characteristics of PTC.
| Clinicopathologic features | Case number | PN | χ 2 | OR (95% CI) |
||||
|---|---|---|---|---|---|---|---|---|
| Low score | High score | |||||||
| # | % | # | % | # | % | p value | ||
| Sex | ||||||||
| Female | 41 | 82 | 12 | 29.27 | 29 | 70.73 | p = 0.6699 | 0.69 (0.12–3.81) |
| Male | 9 | 18 | 2 | 22.22 | 7 | 77.78 | ||
|
| ||||||||
| Age | ||||||||
| <45 | 21 | 42 | 7 | 33.33 | 14 | 66.67 | p = 0.4748 | 0.63 (0.18–2.20) |
| >45 | 29 | 58 | 7 | 24.14 | 22 | 75.86 | ||
|
| ||||||||
| Tumor stage | ||||||||
| Stages I, II | 24 | 48 | 7 | 29.17 | 17 | 70.83 | p = 0.8599 | 0.89 (0.26–3.07) |
| Stages III, IV | 26 | 52 | 7 | 26.92 | 19 | 73.08 | ||
|
| ||||||||
| Histologic subtype | ||||||||
| Conventional | 10 | 20 | 0 | 0 | 10 | 100 | p = 0.0002 | 10.86 (0.55–211.91) |
| Follicular | 21 | 42 | 7 | 33.33 | 14 | 66.67 | ||
| Macrofollicular | 7 | 14 | 0 | 0 | 7 | 100 | 1.4 (0.02–78.80) |
|
| Tall cells | 4 | 8 | 0 | 0 | 4 | 100 | 1.00 (0.24–4.13) |
|
| Oncocytic | 8 | 16 | 7 | 87.5 | 1 | 12.5 | 105.00 (3.73–2948.28) |
|
|
| ||||||||
| Multifocality | ||||||||
| Yes | 34 | 68 | 10 | 29.41 | 24 | 70.59 | p = 0.7459 | 0.8 (0.20–3.08) |
| No | 16 | 32 | 4 | 25 | 12 | 75 | ||
|
| ||||||||
| Tumor size | ||||||||
| <2.18 cm | 35 | 70 | 10 | 28.57 | 25 | 71.43 | p = 0.8907 | 0.90 (0.23–3.53) |
| >2.18 cm | 15 | 30 | 4 | 26.67 | 11 | 73.33 | ||
|
| ||||||||
| Lymphovascular invasion | ||||||||
| Absent | 36 | 72 | 12 | 33.33 | 24 | 66.67 | p = 0.1780 | 0.33 (0.06–1.73) |
| Present | 14 | 28 | 2 | 14.29 | 12 | 85.71 | ||
|
| ||||||||
| Lymph node metastasis | ||||||||
| Absent | 43 | 86 | 12 | 27.91 | 31 | 72.09 | p = 0.9710 | 1.03 (0.17–6.06) |
| Present | 7 | 14 | 2 | 28.57 | 5 | 71.43 | ||
|
| ||||||||
| Extrathyroidal invasion | ||||||||
| Absent | 27 | 54 | 8 | 29.63 | 19 | 70.37 | p = 0.7810 | 0.83 (0.24–2.90) |
| Present | 23 | 46 | 6 | 26.09 | 17 | 73.91 | ||
χ 2: chi-square test; OR: odd ratio; CI: confidence interval.
Table 2.
PN expression in intratumor stroma and clinicopathological characteristics of PTC.
| Clinicopathologic features | Case number | PN | χ 2 | OR (95% CI) |
||||
|---|---|---|---|---|---|---|---|---|
| Low score | High score | |||||||
| # | % | # | % | # | % | p value | ||
| Sex | ||||||||
| Female | 41 | 82 | 13 | 31.71 | 28 | 68.29 | p = 0.9246 | 1.07 (0.23–4.99) |
| Male | 9 | 18 | 3 | 33.33 | 6 | 66.67 | ||
|
| ||||||||
| Age | ||||||||
| <45 | 21 | 42 | 5 | 23.81 | 16 | 76.19 | p = 0.2907 | 1.05 (0.55–6.84) |
| >45 | 29 | 58 | 11 | 37.93 | 18 | 62.07 | ||
|
| ||||||||
| Tumor stage | ||||||||
| Stages I, II | 24 | 48 | 11 | 45.83 | 13 | 54.17 | p = 0.0439 | 0.28 (0.07–0.99) |
| Stages III, IV | 26 | 52 | 5 | 19.23 | 21 | 80.77 | ||
|
| ||||||||
| Histologic subtype | ||||||||
| Conventional | 10 | 20 | 5 | 50 | 5 | 50 | p = 0.7522 | 0.40 (0.08–1.90) |
| Follicular | 21 | 42 | 6 | 28.57 | 15 | 71.43 | ||
| Macrofollicular | 7 | 14 | 2 | 28.57 | 5 | 71.43 | 1.00 (0.15–6.64) |
|
| Tall cells | 4 | 8 | 1 | 25 | 3 | 75 | 3.00 (0.22–39.60) |
|
| Oncocytic | 8 | 16 | 2 | 25 | 6 | 75 | 1.20 (0.12–11.86) |
|
|
| ||||||||
| Multifocality | ||||||||
| No | 34 | 68 | 13 | 38.24 | 21 | 61.76 | p = 0.1683 | 0.37 (0.08–1.56) |
| Yes | 16 | 32 | 3 | 18.75 | 13 | 81.25 | ||
|
| ||||||||
| Tumor size | ||||||||
| <2.18 cm | 35 | 70 | 9 | 25.71 | 26 | 74.29 | p = 0.1455 | 2.52 (0.71–8.96) |
| >2.18 cm | 15 | 30 | 7 | 46.67 | 8 | 53.33 | ||
|
| ||||||||
| Lymphovascular invasion | ||||||||
| Absent | 36 | 72 | 13 | 36.11 | 23 | 63.89 | p = 0.3176 | 0.48 (0.11–2.04) |
| Present | 14 | 28 | 3 | 21.43 | 11 | 78.57 | ||
|
| ||||||||
| Lymph node metastasis | ||||||||
| Absent | 43 | 86 | 16 | 37.21 | 27 | 62.79 | p = 0.0503 | 0.11 (0.006–2.07) |
| Present | 7 | 14 | 0 | 0 | 7 | 100 | ||
|
| ||||||||
| Extrathyroidal invasion | ||||||||
| Absent | 27 | 54 | 13 | 48.15 | 14 | 51.85 | p = 0.008 | 0.16 (0.03–0.67) |
| Present | 23 | 46 | 3 | 13.04 | 20 | 86.96 | ||
χ 2: chi-square test; OR: odd ratio; CI: confidence interval.
3.2.3. Correlations with Clinicopathological Prognostic Factors
The results of the statistical analysis between PN (low versus high expression) in tumor cells and clinicopathological features are summarized in Table 1. Statistically significant differences were registered only between PN immunoreaction and histological variants (p = 0.0002). A high PN score was more frequently noted in conventional subtype than in oncocytic subtype (OD = 105, CI 3.73–2948.28, p = 0.0062).
Table 2 synthesizes the correlation between PN stromal expression (negative versus positive) and clinicopathological features. Our results show significant differences between stromal PN immunoreaction and tumor stage (early versus advanced stages) (p = 0.04) and extrathyroidal extension (p = 0.008). Moreover, a high PN score was more frequently observed in advanced tumor stage (OR 0.28, 95% CI 0.07–0.99; p = 0.0491) and in the occurrence of extrathyroidal extension (OR 0.16, CI 0.03–0.67, p = 0.0124)
We have also noted a very close value to the statistical significant p value for the lymph node metastasis.
4. Discussion
PN is encoded by a gene located on chromosome 13 (13q13.3), in humans [55]. Structurally, it is formed by one N-terminal constant domain, one cysteine-rich domain (EMILIN-like), four fasciclin-repetitive-Fas domains, and one C-terminal hydrophilic domain exhibiting a variable structure according to the isoform [3, 4, 55].
Currently, eight PN isoforms are known, only five of them being sequenced and identified in different tissues: isoform 1 or (a) in osteosarcoma, isoform 2 or (b) in human placenta, isoform 3 or (c) in ovarian carcinoma, and 2 (b), 4 (d), and 5 (e) in either normal or tumoral urinary bladder [3, 8, 56–58].
Different PN isoforms may variably influence ECM fibrillogenesis [59] but it is still unknown if their effect on ECM increases the invasiveness or metastatic potential [13, 60, 61].
During the last 15 years, several papers provided evidences that support PN involvement in different malignancies. According to these studies, stromal PN expression is a negative prognostic factor for patients' survival [13, 28, 32, 41, 42] and, in association with epithelial PN, is significantly correlated with different clinicopathological prognostic factors [11, 13, 20, 35, 44, 47, 62, 63]. PN involvement in the epithelial-mesenchymal transition (EMT) has been also a matter of research interest, due to its potential therapeutic target value [8, 13, 39, 64–66]. Therefore, PN expression was analyzed in correlation with EMT (vimentin, elastin, and collagen) and angiogenesis specific markers, demonstrating its involvement as a promoter of this process [12, 15, 39, 63, 67].
Few papers addressed PN in thyroid tumors, predominantly using techniques of molecular biology (cDNA microarrays and real-time PCR) [58, 68–70]. Eight h-periostin isoforms have been identified in both thyroid carcinoma and in corresponding nonneoplastic tissues, all of them being related to thyroid carcinogenesis, invasion, or lymph node metastasis, regardless of differences between their expression pattern [58]. A high PN gene expression is associated with aggressive and poorly differentiated PTCs [68] and is correlated with specific morphological cellular features (loss of polarization and cohesiveness) registered in the invasive front of the tumor [69]. Only one of the four studies from literature has also analyzed PN immunoexpression, within a rather limited number of cases (10 normal thyroids, 10 follicular adenomas, 10 follicular thyroid carcinomas, and 10 PTCs samples, resp.) [70]. No PN staining has been noticed in normal thyroid tissue, in follicular adenoma, and in follicular thyroid carcinoma, and only 4 cases from a total of 10 PTCs showed a diffuse cytoplasmic immunoreaction [70].
Within this context, the present study provides new data regarding the specific PN immunoexpression in epithelial tumor cells and intratumoral stroma, in different histological subtypes of PTC.
To the best of our knowledge, this is the first report of qualitative differences in epithelial and stromal PN expression between conventional, follicular, macrofollicular, tall cell, and oncocytic subtypes. Thus, the idea that PN may be tissue-specific [11] is strengthened by supplementary evidences of its heterogeneity, reported in different histological subtypes of a specific tumor, such as clear cell, papillary, and chromophobe renal cell carcinoma types [33], and conventional and nonconventional osteosarcoma subtypes [71].
The pivotal role of PN synthesis in different malignancies is currently under scrutiny, by comparing the involvement of tumor epithelial cells with that of the tumor stromal component. As a consequence, it has been hypothesized that PN acts in a cell-type-dependent manner related to its expression in stromal versus epithelial cells, as a result of the activity of different PN terminal regions [13].
This hypothesis has been the starting point of our work which has individually quantified PN immunoexpression in tumor cells and in tumor stroma, respectively. We have additionally refined the reported scores already used for PN assessment [25, 53, 54], considering both the percentage of positive cells and the reaction intensity, using a threshold to label the investigated cases into low and high score categories. This modality of semiquantitative evaluation, based on a specific algorithm, has not been yet applied in thyroid tumor pathology.
Our study showed a heterogeneity of PN stromal immunoexpression, comparable to other malignancies reporting either PN positivity [19, 22, 23, 49, 64] or PN negativity [72]. The most papers have reported that stromal PN has a more aggressive potential than the epithelial PN. This aggressiveness can be attributed to the capacity of the PN produced by the stromal components to act not only by intracellular signaling pathways but also by its fibrillogenic potential within ECM, its C-terminal region interacting with ECM molecules [73, 74].
Our results support the dominant protumorigenic role of stromal PN, while epithelial PN action is less evident. We found that the high stromal PN expression is significantly associated with an advanced tumor stage and extrathyroidal extension. Similar results are also reported in renal cell carcinoma [31, 33], prostate [13, 27, 28], penile [75], and breast cancer [20, 23]. There are no available literature data about the stromal PN profile in thyroid tumors.
On the other hand, PN overexpression in tumor epithelial cells was correlated with specific histological PTC variants, the highest risk being registered for the conventional subtype in comparison to the oncocytic one. Our data are supplementing other results in the mainstream publications. Strictly referring to the thyroid pathology, the single published paper on PN immunoexpression in PTC [70] reports a correlation between PN overexpression and clinicopathological features (i.e., extrathyroidal invasion, distant metastasis, and higher grade staging).
Despite the small number of cases, the authors outline the correlation between PN, ETM, and an aggressive tumor behavior [70]. Moreover, they consider that PN could be a stronger negative prognostic marker than B-RAF, regardless of B-RAF mutation [70]. In other types of malignancies, comparable relationships are demonstrated in renal cell carcinoma (mainly for clear cell subtype) where a greater tumor epithelial PN expression is significantly associated with sarcomatoid differentiation, higher tumor stage, lymph node metastases, and poor overall survival [32, 33] and also in hepatocellular carcinoma, where PN correlates with microvascular invasion, multiple tumors, and advanced tumor stage [41, 42].
Taken together, our results are consistent with the complex framework of controversies regarding PN role in carcinogenesis, particularly for the thyroid location, and support the interest in understanding its relationship with different tumor behaviors. Further research is needed for the validation of PN current status as a promising biomarker.
5. Conclusions
Our study demonstrates a wide variability of PN expression in PTC, both in tumor epithelial component and in tumor stroma. High stromal rather than epithelial PN expression is associated with an aggressive tumor behavior. These results support PN involvement in tumor progression and its possible use as a prognostic marker.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- 1.LiVosi V. A., Albores-Saavedra J., Asa S. L., et al. World Health Organization Classification of Tumours. Pathology and Genetics. Tumours of Endocrine Organs. Lyon, France: IARC Press; 2004. Papillary carcinoma; pp. 57–66. [Google Scholar]
- 2.Erhamamci S., Reyhan M., Kocer N. E., Nursal G. N., Torun N., Yapar A. F. Simultaneous occurrence of medullary and differentiated thyroid carcinomas. Report of 4 cases and brief review of the literature. Hellenic Journal of Nuclear Medicine. 2014;17(2):148–152. doi: 10.1967/s002449910137. [DOI] [PubMed] [Google Scholar]
- 3.Takeshita S., Kikuno R., Tezuka K., Amann E. Osteoblast-specific factor 2: cloning of a putative bone adhesion protein with homology with the insect protein fasciclin I. Biochemical Journal. 1993;294(1):271–278. doi: 10.1042/bj2940271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Horiuchi K., Amizuka N., Takeshita S., et al. Identification and characterization of a novel protein, periostin, with restricted expression to periosteum and periodontal ligament and increased expression by transforming growth factor β. Journal of Bone and Mineral Research. 1999;14(7):1239–1249. doi: 10.1359/jbmr.1999.14.7.1239. [DOI] [PubMed] [Google Scholar]
- 5.Norris R. A., Moreno-Rodriguez R. A., Sugi Y., et al. Periostin regulates atrioventricular valve maturation. Developmental Biology. 2008;316(2):200–213. doi: 10.1016/j.ydbio.2008.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hamilton D. W. Functional role of periostin in development and wound repair: implications for connective tissue disease. Journal of Cell Communication and Signaling. 2008;2(1-2):9–17. doi: 10.1007/s12079-008-0023-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ruan K., Bao S., Ouyang G. The multifaceted role of periostin in tumorigenesis. Cellular and Molecular Life Sciences. 2009;66(14):2219–2230. doi: 10.1007/s00018-009-0013-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gillan L., Matei D., Fishman D. A., Gerbin C. S., Karlan B. Y., Chang D. D. Periostin secreted by epithelial ovarian carcinoma is a ligand for alpha(V)beta(3) and alpha(V)beta (5) integrins and promotes cell motility. Cancer Research. 2002;62(18):5358–5364. [PubMed] [Google Scholar]
- 9.Tai I. T., Dai M., Chen L. B. Periostin induction in tumor cell line explants and inhibition of in vitro cell growth by anti-periostin antibodies. Carcinogenesis. 2005;26(5):908–915. doi: 10.1093/carcin/bgi034. [DOI] [PubMed] [Google Scholar]
- 10.Kudo Y., Siriwardena B. S. M. S., Hatano H., Ogawa I., Takata T. Periostin: Novel diagnostic and therapeutic target for cancer. Histology and Histopathology. 2007;22(10-12):1167–1174. doi: 10.14670/HH-22.1167. [DOI] [PubMed] [Google Scholar]
- 11.Nuzzo P. V., Buzzatti G., Ricci F., et al. Periostin: A novel prognostic and therapeutic target for genitourinary cancer? Clinical Genitourinary Cancer. 2014;12(5):301–311. doi: 10.1016/j.clgc.2014.02.005. [DOI] [PubMed] [Google Scholar]
- 12.Zhu M., Fejzo M. S., Anderson L., et al. Periostin promotes ovarian cancer angiogenesis and metastasis. Gynecologic Oncology. 2010;119(2):337–344. doi: 10.1016/j.ygyno.2010.07.008. [DOI] [PubMed] [Google Scholar]
- 13.Morra L., Moch H. Periostin expression and epithelial-mesenchymal transition in cancer: a review and an update. Virchows Archiv. 2011;459(5):465–475. doi: 10.1007/s00428-011-1151-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ratajczak-Wielgomas K., Dziegiel P. The role of periostin in neoplastic processes. Folia Histochemica et Cytobiologica. 2015;53(2):120–132. doi: 10.5603/FHC.a2015.0014. [DOI] [PubMed] [Google Scholar]
- 15.Siriwardena B. S. M. S., Kudo Y., Ogawa I., et al. Periostin is frequently overexpressed and enhances invasion and angiogenesis in oral cancer. British Journal of Cancer. 2006;95(10):1396–1403. doi: 10.1038/sj.bjc.6603431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chang Y., Lee T. C., Li J. C., et al. Differential expression of osteoblast-specific factor 2 and polymeric immunoglobulin receptor genes in nasopharyngeal carcinoma. Head & Neck. 2005;27(10):873–882. doi: 10.1002/hed.20253. [DOI] [PubMed] [Google Scholar]
- 17.Kudo Y., Ogawa I., Kitajima S., et al. Periostin promotes invasion and anchorage-independent growth in the metastatic process of head and neck cancer. Cancer Research. 2006;66(14):6928–6935. doi: 10.1158/0008-5472.CAN-05-4540. [DOI] [PubMed] [Google Scholar]
- 18.Shao R., Bao S., Bai X., et al. Acquired expression of periostin by human breast cancers promotes tumor angiogenesis through up-regulation of vascular endothelial growth factor receptor 2 expression. Molecular and Cellular Biology. 2004;24(9):3992–4003. doi: 10.1128/MCB.24.9.3992-4003.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Puglisi F., Puppin C., Pegolo E., et al. Expression of periostin in human breast cancer. Journal of Clinical Pathology. 2008;61(4):494–498. doi: 10.1136/jcp.2007.052506. [DOI] [PubMed] [Google Scholar]
- 20.Zhang Y., Zhang G., Li J., Tao Q., Tang W. The expression analysis of periostin in human breast cancer. Journal of Surgical Research. 2010;160(1):102–106. doi: 10.1016/j.jss.2008.12.042. [DOI] [PubMed] [Google Scholar]
- 21.Xu D., Xu H., Ren Y., et al. Cancer stem cell-related gene periostin: a novel prognostic marker for breast cancer. PLoS ONE. 2012;7(10) doi: 10.1371/journal.pone.0046670.e46670 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Contié S., Voorzanger-Rousselot N., Litvin J., Clézardin P., Garnero P. Increased expression and serum levels of the stromal cell-secreted protein periostin in breast cancer bone metastases. International Journal of Cancer. 2011;128(2):352–360. doi: 10.1002/ijc.25591. [DOI] [PubMed] [Google Scholar]
- 23.Nuzzo P. V., Rubagotti A., Zinoli L., Salvi S., Boccardo S., Boccardo F. The prognostic value of stromal and epithelial periostin expression in human breast cancer: Correlation with clinical pathological features and mortality outcome. BMC Cancer. 2016;16(1, article no. 95) doi: 10.1186/s12885-016-2139-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zhu M., Saxton R. E., Ramos L., et al. Neutralizing monoclonal antibody to periostin inhibits ovarian tumor growth and metastasis. Molecular Cancer Therapeutics. 2011;10(8):1500–1508. doi: 10.1158/1535-7163.MCT-11-0046. [DOI] [PubMed] [Google Scholar]
- 25.Choi K. U., Yun J. S., Lee I. H., et al. Lysophosphatidic acid-induced expression of periostin in stromal cells: Prognoistic relevance of periostin expression in epithelial ovarian cancer. International Journal of Cancer. 2011;128(2):332–342. doi: 10.1002/ijc.25341. [DOI] [PubMed] [Google Scholar]
- 26.Karlan B. Y., Dering J., Walsh C., et al. POSTN/TGFBI-associated stromal signature predicts poor prognosis in serous epithelial ovarian cancer. Gynecologic Oncology. 2014;132(2):334–342. doi: 10.1016/j.ygyno.2013.12.021. [DOI] [PubMed] [Google Scholar]
- 27.Tsunoda T., Furusato B., Takashima Y., et al. The increased expression of periostin during early stages of prostate cancer and advanced stages of cancer stroma. The Prostate. 2009;69(13):1398–1403. doi: 10.1002/pros.20988. [DOI] [PubMed] [Google Scholar]
- 28.Tischler V., Fritzsche F. R., Wild P. J., et al. Periostin is up-regulated in high grade and high stage prostate cancer. BMC Cancer. 2010;10, article no. 273 doi: 10.1186/1471-2407-10-273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sun C., Zhao X., Xu K., et al. Periostin: A promising target of therapeutical intervention for prostate cancer. Journal of Translational Medicine. 2011;9(1, article no. 99) doi: 10.1186/1479-5876-9-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Nuzzo P. V., Rubagotti A., Zinoli L., et al. Prognostic value of stromal and epithelial periostin expression in human prostate cancer: correlation with clinical pathological features and the risk of biochemical relapse or death. BMC Cancer. 2012;12, article 625 doi: 10.1186/1471-2407-12-625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Castronovo V., Waltregny D., Kischel P., et al. A chemical proteomics approach for the identification of accessible antigens expressed in human kidney cancer. Molecular & Cellular Proteomics. 2006;5(11):2083–2091. doi: 10.1074/mcp.M600164-MCP200. [DOI] [PubMed] [Google Scholar]
- 32.Dahinden C., Ingold B., Wild P., et al. Mining tissue microarray data to uncover combinations of biomarker expression patterns that improve intermediate staging and grading of clear cell renal cell cancer. Clinical Cancer Research. 2010;16(1):88–98. doi: 10.1158/1078-0432.CCR-09-0260. [DOI] [PubMed] [Google Scholar]
- 33.Morra L., Rechsteiner M., Casagrande S., et al. Relevance of periostin splice variants in renal cell carcinoma. The American Journal of Pathology. 2011;179(3):1513–1521. doi: 10.1016/j.ajpath.2011.05.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Baril P., Gangeswaran R., Mahon P. C., et al. Periostin promotes invasiveness and resistance of pancreatic cancer cells to hypoxia-induced cell death: role of the β4 integrin and the PI3k pathway. Oncogene. 2007;26(14):2082–2094. doi: 10.1038/sj.onc.1210009. [DOI] [PubMed] [Google Scholar]
- 35.Ben Q.-W., Jin X.-L., Jun L., Cai X., Yuan F., Yuan Y.-Z. Periostin, a matrix specific protein, is associated with proliferation and invasion of pancreatic cancer. Oncology Reports. 2011;25(3):709–716. doi: 10.3892/or.2011.1140. [DOI] [PubMed] [Google Scholar]
- 36.Li J.-S., Sun G.-W., Wei X.-Y., Tang W.-H. Expression of periostin and its clinicopathological relevance in gastric cancer. World Journal of Gastroenterology. 2007;13(39):5261–5266. doi: 10.3748/wjg.v13.i39.5261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kikuchi Y., Kunita A., Iwata C., et al. The niche component periostin is produced by cancer-associated fibroblasts, supporting growth of gastric cancer through ERK activation. The American Journal of Pathology. 2014;184(3):859–870. doi: 10.1016/j.ajpath.2013.11.012. [DOI] [PubMed] [Google Scholar]
- 38.Lv H., Liu R., Fu J., et al. Epithelial cell-derived periostin functions as a tumor suppressor in gastric cancer through stabilizing p53 and E-cadherin proteins via the Rb/E2F1/p14ARF/Mdm2 signaling pathway. Cell Cycle. 2014;13(18):2962–2974. doi: 10.4161/15384101.2014.947203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bao S., Ouyang G., Bai X., et al. Periostin potently promotes metastatic growth of colon cancer by augmenting cell survival via the Akt/PKB pathway. Cancer Cell. 2004;5(4):329–339. doi: 10.1016/S1535-6108(04)00081-9. [DOI] [PubMed] [Google Scholar]
- 40.Xiao Z.-M., Wang X.-Y., Wang A.-M. Periostin induces chemoresistance in colon cancer cells through activation of the PI3K/Akt/survivin pathway. Biotechnology and Applied Biochemistry. 2015;62(3):401–406. doi: 10.1002/bab.1193. [DOI] [PubMed] [Google Scholar]
- 41.Riener M.-O., Fritzsche F. R., Soll C., et al. Expression of the extracellular matrix protein periostin in liver tumours and bile duct carcinomas. Histopathology. 2010;56(5):600–606. doi: 10.1111/j.1365-2559.2010.03527.x. [DOI] [PubMed] [Google Scholar]
- 42.Jang S. Y., Park S. Y., Lee H. W., et al. The combination of periostin overexpression and microvascular invasion is related to a poor prognosis for hepatocellular carcinoma. Gut and Liver. 2016;10(6):948–954. doi: 10.5009/gnl15481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sasaki H., Auclair D., Fukai I., et al. Serum level of the periostin, a homologue of an insect cell adhesion molecule, as a prognostic marker in nonsmall cell lung carcinomas. Cancer. 2001;92(4):843–848. doi: 10.1002/1097-0142(20010815)92:4<843::AID-CNCR1391>3.0.CO;2-P. doi: 10.1002/1097-0142(20010815)92:4<843::AID-CNCR1391>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- 44.Soltermann A., Tischler V., Arbogast S., et al. Prognostic significance of epithelial-mesenchymal and mesenchymal-epithelial transition protein expression in non-small cell lung cancer. Clinical Cancer Research. 2008;14(22):7430–7437. doi: 10.1158/1078-0432.ccr-08-0935. [DOI] [PubMed] [Google Scholar]
- 45.Morra L., Rechsteiner M., Casagrande S., et al. Characterization of periostin isoform pattern in non-small cell lung cancer. Lung Cancer. 2012;76(2):183–190. doi: 10.1016/j.lungcan.2011.10.013. [DOI] [PubMed] [Google Scholar]
- 46.Hong L.-Z., Wei X.-W., Chen J.-F., Shi Y. Overexpression of periostin predicts poor prognosis in non-small cell lung cancer. Oncology Letters. 2013;6(6):1595–1603. doi: 10.3892/ol.2013.1590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Schramm A., Opitz I., Thies S., et al. Prognostic significance of epithelial-mesenchymal transition in malignant pleural mesothelioma. European Journal of Cardio-Thoracic Surgery. 2010;37(3):566–572. doi: 10.1016/j.ejcts.2009.08.027. [DOI] [PubMed] [Google Scholar]
- 48.Sasaki H., Sato Y., Kondo S., et al. Expression of the periostin mRNA level in neuroblastoma. Journal of Pediatric Surgery. 2002;37(9):1293–1297. doi: 10.1053/jpsu.2002.34985. [DOI] [PubMed] [Google Scholar]
- 49.Tian B., Zhang Y., Zhang J. Periostin is a new potential prognostic biomarker for glioma. Tumor Biology. 2014;35(6):5877–5883. doi: 10.1007/s13277-014-1778-3. [DOI] [PubMed] [Google Scholar]
- 50.Zhou W., Ke S. Q., Huang Z., et al. Periostin secreted by glioblastoma stem cells recruits M2 tumour-associated macrophages and promotes malignant growth. Nature Cell Biology. 2015;17(2):170–182. doi: 10.1038/ncb3090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Mikheev A. M., Mikheeva S. A., Trister A. D., et al. Periostin is a novel therapeutic target that predicts and regulates glioma malignancy. Neuro-Oncology. 2015;17(3):372–382. doi: 10.1093/neuonc/nou161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Greene F. L., Page D. L., Fleming I. D., et al., editors. AJCC Cancer Staging Handbook. 6th. New York, NY, USA: Springer; 2002. [Google Scholar]
- 53.Jia W., Wang W., Ji C.-S., et al. Coexpression of periostin and EGFR in patients with esophageal squamous cell carcinoma and their prognostic significance. OncoTargets and Therapy. 2016;9:5133–5142. doi: 10.2147/OTT.S111132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Sung P.-L., Jan Y.-H., Lin S.-C., et al. Periostin in tumor microenvironment is associated with poor prognosis and platinum resistance in epithelial ovarian carcinoma. Oncotarget . 2016;7(4):4036–4047. doi: 10.18632/oncotarget.6700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Litvin J., Selim A.-H., Montgomery M. O., et al. Expression and function of periostin-isoforms in bone. Journal of Cellular Biochemistry. 2004;92(5):1044–1061. doi: 10.1002/jcb.20115. [DOI] [PubMed] [Google Scholar]
- 56.Litvin J., Zhu S., Norris R., Markwald R. Periostin family of proteins: Therapeutic targets for heart disease. Anatomical Record - Part A Discoveries in Molecular, Cellular, and Evolutionary Biology. 2005;287(2):1205–1212. doi: 10.1002/ar.a.20237. [DOI] [PubMed] [Google Scholar]
- 57.Kim C. J., Isono T., Tambe Y., et al. Role of alternative splicing of periostin in human bladder carcinogenesis. International Journal of Oncology. 2008;32(1):161–169. [PubMed] [Google Scholar]
- 58.Bai Y., Nakamura M., Zhou G., et al. Novel isoforms of periostin expressed in the human thyroid. Japanese Clinical Medicine. 2010;1:13–20. doi: 10.4137/JCM.S5899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Hoersch S., Andrade-Navarro M. A. Periostin shows increased evolutionary plasticity in its alternatively spliced region. BMC Evolutionary Biology. 2010;10(1, article no. 30) doi: 10.1186/1471-2148-10-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Kudo A. Periostin in fibrillogenesis for tissue regeneration: Periostin actions inside and outside the cell. Cellular and Molecular Life Sciences. 2011;68(19):3201–3207. doi: 10.1007/s00018-011-0784-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Conway S. J., Izuhara K., Kudo Y., et al. The role of periostin in tissue remodeling across health and disease. Cellular and Molecular Life Sciences. 2014;71(7):1279–1288. doi: 10.1007/s00018-013-1494-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Utispan K., Sonongbua J., Thuwajit P., et al. Periostin activates integrin α5β1 through a PI3K/AKT-dependent, pathway in invasion of cholangiocarcinoma. International Journal of Oncology. 2012;41(3):1110–1118. doi: 10.3892/ijo.2012.1530. [DOI] [PubMed] [Google Scholar]
- 63.Lv Y., Wang W., Jia W., et al. High-level expression of periostin is closely related to metastatic potential and poor prognosis of hepatocellular carcinoma. Medical Oncology. 2013;30(1):1–9. doi: 10.1007/s12032-012-0385-7. [DOI] [PubMed] [Google Scholar]
- 64.Li P., Oparil S., Feng W., Chen Y.-F. Hypoxia-responsive growth factors upregulate periostin and osteopontin expression via distinct signaling pathways in rat pulmonary arterial smooth muscle cells. Journal of Applied Physiology. 2004;97(4):1550–1558. doi: 10.1152/japplphysiol.01311.2003. [DOI] [PubMed] [Google Scholar]
- 65.Yan W., Shao R. Transduction of a mesenchyme-specific gene periostin into 293T cells induces cell invasive activity through epithelial-mesenchymal transformation. The Journal of Biological Chemistry. 2006;281(28):19700–19708. doi: 10.1074/jbc.m601856200. [DOI] [PubMed] [Google Scholar]
- 66.Kim C. J., Sakamoto K., Tambe Y., Inoue H. Opposite regulation of epithelial-to-mesenchymal transition and cell invasiveness by periostin between prostate and bladder cancer cells. International Journal of Oncology. 2011;38(6):1759–1766. doi: 10.3892/ijo.2011.997. [DOI] [PubMed] [Google Scholar]
- 67.Kudo Y., Iizuka S., Yoshida M., et al. Periostin directly and indirectly promotes tumor lymphangiogenesis of head and neck cancer. PLoS ONE. 2012;7(8) doi: 10.1371/journal.pone.0044488.e44488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Fluge Ø., Bruland O., Akslen L. A., Lillehaug J. R., Varhaug J. E. Gene expression in poorly differentiated papillary thyroid carcinomas. Thyroid. 2006;16(2):161–175. doi: 10.1089/thy.2006.16.161. [DOI] [PubMed] [Google Scholar]
- 69.Bai Y., Kakudo K., Nakamura M., et al. Loss of cellular polarity/cohesiveness in the invasive front of papillary thyroid carcinoma and periostin expression. Cancer Letters. 2009;281(2):188–195. doi: 10.1016/j.canlet.2009.02.043. [DOI] [PubMed] [Google Scholar]
- 70.Puppin C., Fabbro D., Dima M., et al. High periostin expression correlates with aggressiveness in papillary thyroid carcinomas. Journal of Endocrinology. 2008;197(2):401–408. doi: 10.1677/JOE-07-0618. [DOI] [PubMed] [Google Scholar]
- 71.Hu F., Wang W., Zhou H.-C., Shang X.-F. High expression of periostin is dramatically associated with metastatic potential and poor prognosis of patients with osteosarcoma. World Journal of Surgical Oncology. 2014;12(1, article no. 287) doi: 10.1186/1477-7819-12-287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Fukushima N., Kikuchi Y., Nishiyama T., Kudo A., Fukayama M. Periostin deposition in the stroma of invasive and intraductal neoplasms of the pancreas. Modern Pathology. 2008;21(8):1044–1053. doi: 10.1038/modpathol.2008.77. [DOI] [PubMed] [Google Scholar]
- 73.Morris R. A., Damon B., Mironov V., et al. Periostin regulates collagen fibrillogenesis and the biomechanical properties of connective tissues. Journal of Cellular Biochemistry. 2007;101(3):695–711. doi: 10.1002/jcb.21224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Takayama G., Arima K., Kanaji T., et al. Periostin: A novel component of subepithelial fibrosis of bronchial asthma downstream of IL-4 and IL-13 signals. The Journal of Allergy and Clinical Immunology. 2006;118(1):98–104. doi: 10.1016/j.jaci.2006.02.046. [DOI] [PubMed] [Google Scholar]
- 75.Gunia S., Jain A., Koch S., et al. Periostin expression correlates with pT-stage, grading and tumour size, and independently predicts cancer-specific survival in surgically treated penile squamous cell carcinomas. Journal of Clinical Pathology. 2013;66(4):297–301. doi: 10.1136/jclinpath-2012-201262. [DOI] [PubMed] [Google Scholar]