

Abstract
Rationale:
Pectus excavatum (PE) in the setting of congenital heart disease is not uncommon. The surgical strategy has evolved over the last 20 years from a staged approach to simultaneous repair of both defects.
Patient concerns:
A 3-year-old boy was admitted for elective repair of PE and atrial septal defect (ASD).
Diagnoses:
Clinically, there were obvious features of PE and a grade 2 systolic murmur heard loudest at the 2nd intercostal space abutting the left sternal border. Echocardiography confirmed the presence of a secundum-type ASD. Following discussions with the family, consent was obtained and the patient underwent concomitant surgery for both defects. The ASD was first device-closed under the guidance of transesophageal echocardiography (TEE) and then a standard Nuss procedure was performed with an 8-inch bar.
Outcomes:
Postoperative echocardiography confirmed a satisfactory device closure of the ASD. The repair of PE was considered satisfactory on physical examination and with chest radiography. The postoperative course was uneventful except for atelectasis of the right upper lobe. The patient was discharged 10 days postoperatively.
Lessons:
This case suggests that in carefully selected cases with concomitant PE and ASD, a combination of Nuss procedure and TEE-guided transcatheter device closure can be safely performed with less physical and no radiation trauma and theoretically better aesthetic effects and surgical outcome.
Keywords: atrial septal defect, Nuss procedure, transesophageal echocardiography guided, transcatheter
1. Introduction
Congenital heart defect in association with pectus excavatum (PE) is not an uncommon finding. The surgical strategy for dealing with both entities have evolved over the last decades.[1,2] Conforming to the push for minimally invasive treatments, atrial septal defect (ASD) repairs have shifted to the realm of the interventional cardiologists, with percutaneous closure the modern norm. In the setting of a coexisting PE that requires surgical repair, avoidance of chest wall disruption (e.g., median sternotomy) to access the ASD is beneficial, to afford an improved outcome to repair of the PE.[3,4] Herein, we describe a case of a 3-year-old patient who underwent concomitant Nuss procedure and transcatheter ASD device closure.
2. Case presentation
A 3 years and 9 months old boy was referred to our institution with a known heart murmur and sunken chest. The child was otherwise normal, and physical examination showed concavity and flaring of the 4th to 7th ribs anteriorly with involvement of the corresponding sternal segments. On heart auscultation, there was a grade 2 systolic murmur at the 2nd intercostal space (ICS) on the left sternal border. Preoperative transthoracic echocardiogram (TTE) showed an 8 mm secundum-type ASD. Chest computed tomography revealed asymmetrical PE with a Haller index of 3.8 (Fig. 1). After family discussions, the patient proceeded with concomitant transcatheter ASD device closure and Nuss procedure.
Figure 1.
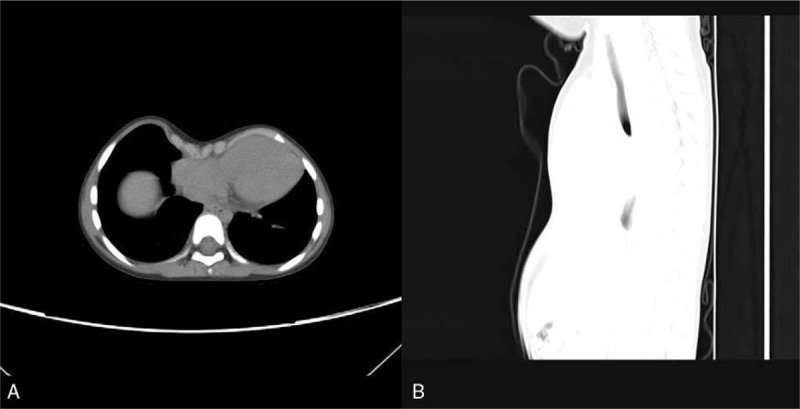
Axial view (A) and sagittal view (B) of chest CT show the severe funnel chest before surgery. CT = computed tomography
Transesophageal echocardiography (TEE) was used to guide the implantation of the closure device. Though the 16 mm sized ASD measured by TEE was somewhat different from the size obtained from TTE, an 18 mm sized symmetrical device (Shanghai Shape Memory Alloy Co., Ltd., Shanghai, People's Republic of China) was implanted uneventfully. Intraoperatively TEE showed no residual leak (Fig. 2). The patient was then positioned for the Nuss procedure. Two small skin incisions along the 6th ICS was made at the anterior axillary line bilaterally. A prebent 8 inch bar (GRIKIN Advanced Material Co., Ltd., Beijing, People's Republic of China) was inserted successfully under thoracoscopic guidance and with the aid of an introducer which traversed retrosternally. The bar was then secured to adjacent ribs using steel wires. Postoperative course was uneventful except for right upper lung atelectasis on postoperative day 1 (Fig. 3) which resolved with analgesia and aggressive chest physiotherapy. The patient was discharged on postoperative day 10.
Figure 2.
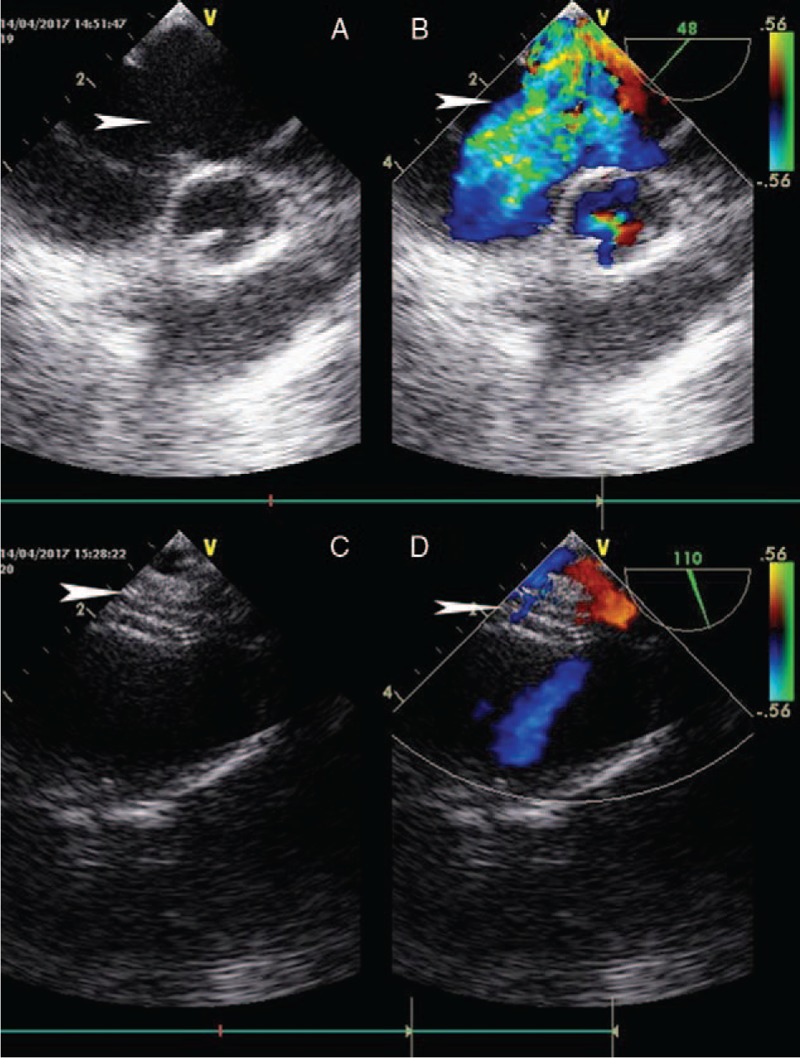
Predeployment 2D echocardiogram (A) and Doppler (B) and Postdeployment 2D echocardiogram(C) and Doppler (D) of TEE (white arrow heads). 2D = two-dimensional; TEE = transesophageal echocardiography.
Figure 3.
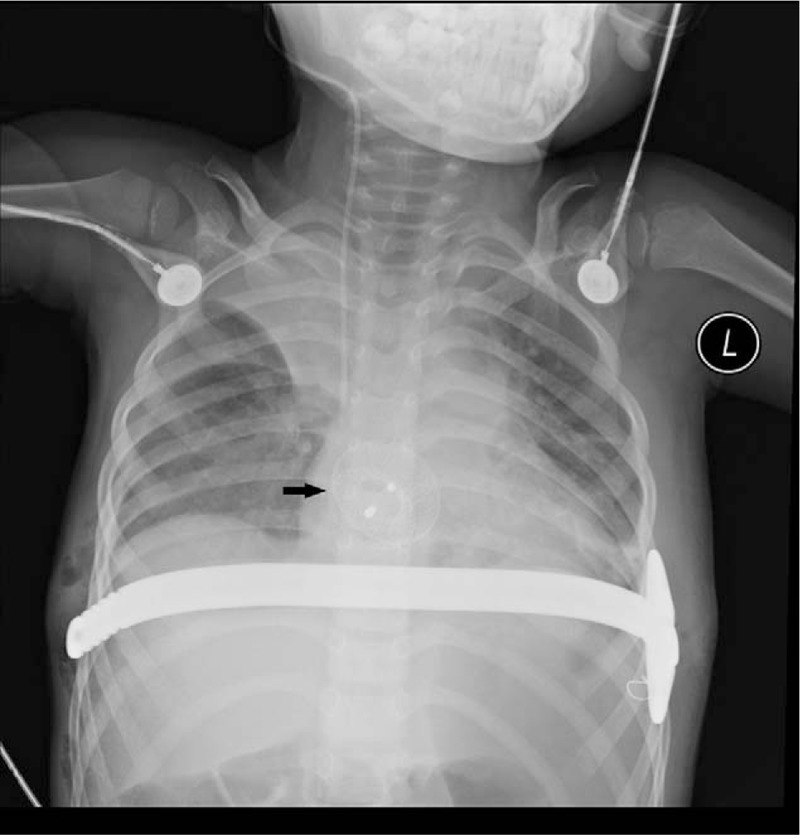
Bedside postoperative day 1 chest X-ray shows right upper lung atelectasis and proper position of the ASD device (black arrow) and Nuss bar. ASD = atrial septal defect.
3. Discussion
The surgical management of concomitant ASD and PE has evolved over the last 20 years from staged operations[1] to concomitant operation in a single anaesthesia.[2] This short period of time has witnessed significant advances in technique and materials. For PE, the Ravitch procedure was once the gold standard but gradually superseded by the Nuss procedure following its introduction in 1998.[5]
Similarly, the evolution of transcatheter-based techniques avoids the morbidity associated with open surgery and enables management of concomitant diseases in a hybrid manner, minimizing incision size and in some cases, avoiding the use of cardiopulmonary bypass.[6] Moreover, echocardiography-guided transcatheter techniques avoid radiation hazard, especially, in children.[7]
To our best knowledge, this is the first case to report concomitant Nuss procedure preceded by transcatheter ASD device closure under TEE guidance without fluoroscopy. By avoiding conventional median sternotomy, the integrity of the chest wall is preserved, facilitating insertion of the Nuss bar, thereby optimizing the outcomes of the PE repair.
From a technical perspective, if the device closure is to be used to treat the ASD, the distortion of the heart by the posteriorly concaved sternum may affect the echocardiographic views.[8] And this may be also the reason for the size discrepancy of the ASD measured using TTE and TEE. In our case, the shape of the ASD shown under TEE was not significantly different from that under TTE and the guidance was straightforward throughout the implantation of the device.
In conclusion, concomitant hybrid repair of ASD and PE is well tolerated and feasible in carefully select cases.
Acknowledgments
Authors’ contributions: XD drafted the manuscript; XD, CH, and PH revised the manuscript; XY, LY managed the patient.
Footnotes
Abbreviations: ASD = atrial septal defect, PE = pectus excavatum, TEE = transesophageal echocardiography.
Ethics approval and consent to participate: Ethics approval and consent to participate for this retrospective clinical case report was waived by ethics committee of the institution.
Consent for publication: Written informed consent was obtained from the parents of the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by this journal.
The authors have no conflicts of interest to disclose.
References
- [1].Jones WG, Hoffman L, Devereux RB, et al. Staged approach to combined repair of pectus excavatum and lesions of the heart. Ann Thorac Surg 1994;57:212–4. [DOI] [PubMed] [Google Scholar]
- [2].Kao CH, Tsai CS, Huang TW, et al. The Nuss procedure for pectus excavatum at the time of atrial septal closure. Ann Thorac Surg 2010;89:985–6. [DOI] [PubMed] [Google Scholar]
- [3].Tuncer E, Vuran AC, Ozyuksel A, et al. Simultaneous repair of pectus excavatum and pulmonary valve implantation years after complete repair of tetralogy of Fallot. Gen Thorac Cardiovasc Surg 2017;65:127–9. [DOI] [PubMed] [Google Scholar]
- [4].Kandakure PR, Dhannapuneni R, Venugopal P, et al. Concomitant congenital heart defect repair and Nuss procedure for pectus excavatum. Asian Cardiovasc Thorac Ann 2014;22:212–4. [DOI] [PubMed] [Google Scholar]
- [5].Nuss D, Obermeyer RJ, Kelly RE. Nuss bar procedure: past, present and future. Ann Cardiothorac Surg 2016;5:422–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Lock JE, Cockerham JT, Keane JF, et al. Transcatheter umbrella closure of congenital heart defects. Circulation 1987;75:593–9. [DOI] [PubMed] [Google Scholar]
- [7].Tzifa A, Gordon J, Tibby SM, et al. Transcatheter atrial septal defect closure guided by colour flow Doppler. Int J Cardiol 2011;149:299–303. [DOI] [PubMed] [Google Scholar]
- [8].Mangovski L, Farkic M, Jovovic L. Transcatheter closure of atrial septal defect in a patient with Noonan syndrome after corrective surgery. Vojnosanit Pregl 2015;72:557–60. [DOI] [PubMed] [Google Scholar]