

Cancer cachexia and sarcopenia can occur frequently in patients with advanced cancer, and may negatively affect treatment outcomes. This article highlights the importance of assessing sarcopenia and describes the relationship between sarcopenia and patients' quality of life in patients with newly diagnosed, incurable cancer.
Keywords: Sarcopenia, Depression, Quality of life, Advanced cancer, Palliative care
Abstract
Background.
Patients with advanced cancer often experience muscle wasting (sarcopenia), yet little is known about the characteristics associated with sarcopenia and the relationship between sarcopenia and patients’ quality of life (QOL) and mood.
Materials and Methods.
As part of a randomized trial, we assessed baseline QOL (Functional Assessment of Cancer Therapy‐General [FACT‐G]) and mood (Hospital Anxiety and Depression Scale [HADS]) in patients within 8 weeks of diagnosis of incurable lung or gastrointestinal cancer, and prior to randomization. Using computed tomography scans collected as part of routine clinical care, we assessed sarcopenia at the level of the third lumbar vertebra with validated sex‐specific cutoffs. We used logistic regression to explore characteristics associated with presence of sarcopenia. To examine associations between sarcopenia, QOL and mood, we used linear regression, adjusted for patients’ age, sex, marital status, education, and cancer type.
Results.
Of 237 participants (mean age = 64.41 ± 10.93 years), the majority were male (54.0%) and married (70.5%) and had lung cancer (56.5%). Over half had sarcopenia (55.3%). Older age (odds ratio [OR] = 1.05, p = .002) and education beyond high school (OR = 1.95, p = .047) were associated with greater likelihood of having sarcopenia, while female sex (OR = 0.25, p < .001) and higher body mass index (OR = 0.79, p < .001) correlated with lower likelihood of sarcopenia. Sarcopenia was associated with worse QOL (FACT‐G: B = −4.26, p = .048) and greater depression symptoms (HADS‐depression: B = −1.56, p = .005).
Conclusion.
Sarcopenia was highly prevalent among patients with newly diagnosed, incurable cancer. The associations of sarcopenia with worse QOL and depression symptoms highlight the need to address the issue of sarcopenia early in the course of illness.
Implications for Practice.
This study found that sarcopenia, assessed using computed tomography scans acquired as part of routine clinical care, is highly prevalent in patients with newly diagnosed, incurable cancer. Notably, patients with sarcopenia reported worse quality of life and greater depression symptoms than those without sarcopenia. These findings highlight the importance of addressing muscle loss early in the course of illness among patients with incurable cancer. In the future, investigators should expand upon these findings to develop strategies for assessing and treating sarcopenia while striving to enhance the quality of life and mood outcomes of patients with advanced cancer.
Introduction
Cancer cachexia, a syndrome of weight loss and low muscle mass (sarcopenia), occurs frequently in patients with advanced cancer and can negatively impact their outcomes, including treatment tolerance and survival [1], [2], [3], [4], [5], [6]. Causes of cancer cachexia include reduced food intake, diminished physical activity, and abnormal metabolism [7], [8], [9]. Data suggest that patients with cancer cachexia experience poor treatment tolerance and worse morbidity and mortality compared with patients who maintain their weight and muscle mass [1], [2], [3], [4], [5], [6]. In addition, cachexia has been linked to worse physical function and loss of functional independence [6], [10], [11]. Thus, cancer cachexia is a common and detrimental problem for patients with cancer, yet it often goes unaddressed and has been understudied among patients with advanced cancer [12].
Previous studies addressing cancer cachexia have been limited by the lack of a standard definition [13]. Cachexia, sarcopenia, and solitary muscle loss represent different aspects of the muscle wasting spectrum and can have different clinical presentations and prognoses [14], [15]. Simply measuring body weight to quantify cachexia is not adequate, as this fails to account for fluid accumulation, large tumor burden, and the slow rate of visceral organ atrophy present in some patients with cancer [16], [17]. Loss of muscle mass occurs frequently in patients with advanced cancer, though clinicians are often unaware of their patients’ muscle mass by assessing body weight alone [6], [18]. Recently, an international consensus panel published a report clarifying the definition and classification of cancer cachexia [15]. This report highlighted the importance of assessing sarcopenia, defined by quantifying muscle mass using routinely collected computed tomography (CT), among patients with cancer. As a result, investigators studying cancer cachexia frequently use patients’ CT scans to assess sarcopenia. However, we lack data regarding the relationship between these CT scan measurements of sarcopenia and important patient‐reported outcomes, such as quality of life (QOL) and mood among patients with advanced cancer.
Understanding the association between sarcopenia and patients’ QOL and mood is particularly important for patients with advanced cancer, as efforts to improve these outcomes are essential components of caring for this population. Notably, patients with advanced cancer are more likely to suffer the consequences of sarcopenia than those with curable disease, as they often experience a high symptom burden, including nausea, poor appetite, and fatigue [19], [20]. Additionally, sarcopenia can negatively affect patients’ functional status and independence [6], [10], [11], which may influence both their physical and emotional well‐being. Importantly, the manifestations of sarcopenia often appear gradually, as the disease worsens, and clinicians may only discover the profound muscle loss late in the disease trajectory, when efforts to intervene are less likely to provide much benefit. Thus, studies are needed to define the prevalence and understand the impact of sarcopenia earlier in the disease course, at a time when patients may experience the benefits of interventions focused on maintaining and improving their muscle mass.
Using baseline data from a randomized trial, we sought to explore the relationships among sarcopenia (using consensus definitions that recommend assessing muscle mass with CT scans [15]), QOL, and mood in patients with newly diagnosed, incurable cancer. We hypothesized that a substantial proportion of patients would meet criteria for sarcopenia on CT scans, even at an early point in the disease trajectory, and these patients would report worse QOL and mood symptoms compared with those without sarcopenia. By studying the relationship between sarcopenia and patients’ QOL and mood, this study will inform future interventions seeking to address sarcopenia earlier in the disease course among patients with newly diagnosed, incurable cancer, ideally to improve their experience with the illness and health outcomes.
Materials and Methods
Study Design
As part of a randomized trial of early palliative care integrated with oncology care versus oncology care alone [21], we approached patients within 8 weeks of diagnosis with incurable cancer. For the current study, we utilized patient‐reported data collected at baseline after informed consent, but prior to patient randomization and the start of the intervention. The Dana‐Farber/Harvard Cancer Care Institutional Review Board approved the study protocol.
Patient Selection
The study sample was comprised of patients from Massachusetts General Hospital (MGH) Cancer Center with a confirmed diagnosis of incurable lung or noncolorectal gastrointestinal cancer within the previous 8 weeks and no prior therapy for metastatic disease. Other patient eligibility criteria included not receiving treatment with curative intent, an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2, age ≥18 years, plan to receive cancer care at MGH, and the ability to read and respond to questions in English or with minimal assistance from family or an interpreter. We did not enroll patients who were already receiving palliative care services, needed immediate referral for palliative care or hospice, or had significant psychiatric or other comorbid disease that would interfere with informed consent or study participation.
Study Measures
Sociodemographic and Clinical Factors.
Participants completed a demographic questionnaire that included race, ethnicity, smoking history, religion, relationship status, education, and income. We reviewed participants’ electronic medical records to obtain data on their age, sex, cancer diagnosis, ECOG performance status, and initial cancer treatment.
Quality of Life.
We measured participants’ QOL using the Functional Assessment of Cancer Therapy‐General (FACT‐G) [22]. The FACT‐G contains 27 items with subscales assessing well‐being across four domains (physical, functional, emotional, and social) during the past week. Higher scores indicate better QOL.
Depression and Anxiety.
We measured patients’ depression and anxiety symptoms using the Hospital Anxiety and Depression Scale (HADS) [23]. The 14‐item HADS contains two 7‐item subscales assessing depression and anxiety symptoms during the past week. Higher total and subscale scores indicate worse symptoms, and a score greater than 7 denotes clinically significant depression or anxiety.
Sarcopenia Measured on CT Scans.
We assessed for the presence of sarcopenia using CT scans collected as part of routine clinical care. We limited our study sample to only those patients with CT scans within 30 days before or after their baseline questionnaires and utilized only the CT scan closest to the date of the baseline questionnaire. We quantified skeletal muscle cross‐sectional area (CSA) in cm2 on a single axial image at the level of the third lumbar (L3) vertebral body with semi‐automated threshold‐based segmentation (OsiriX; Pixmeo, Bernex, Switzerland, http://www.osirix-viewer.com/). We used attenuation thresholds set at −29 and +150 Hounsfield units for skeletal muscle [24]. Figure 1 displays examples of patients with high and low muscle mass using our technique. We computed the lean muscle CSA in cm2 by summing the given tissue's pixels and multiplying the sum by the absolute unit pixel surface area. A research assistant (G.F.) performed the measurement, and a board‐certified radiologist (F.J.F.) with 8 years of experience verified each analysis. To assess inter‐ and intra‐analyst agreement, we randomly selected 40 images and then had these images re‐analyzed independently 9 months later by a second research assistant (J.M.) and by the primary analyst. We achieved excellent inter‐ and intra‐analyst agreement with intraclass correlation coefficients of 0.9965 and 0.9996, respectively. We normalized skeletal muscle CSA for stature and reported this skeletal muscle index as cm2/m2. For the current study, we defined sarcopenia as an L3 skeletal muscle index of <55 cm2/m2 for men and <39 cm2/m2 for women, as proposed by the international consensus for cancer cachexia [15].
Figure 1.

Computed tomography (CT) scans demonstrating patients with high (90th percentile) and low (10th percentile) muscle mass. Axial CT images of the third lumbar vertebra region, with skeletal muscle highlighted in red. (A): Image of a 61‐year‐old female patient with skeletal muscle index of 34.2 cm2/m2. (B): Image of a 53‐year‐old male patient with skeletal muscle index of 60.4 cm2/m2.
Statistical Analysis
We used descriptive statistics to analyze the frequencies, medians, means, and standard deviations (SDs) of the study variables for the overall study sample. We compared baseline characteristics of participants with and without sarcopenia using chi‐square or Fisher's exact test for the categorical variables and independent‐samples Student's t tests for the continuous variables. We used logistic regression, adjusted for variables with p < .25 on univariate analysis, to explore patient characteristics independently associated with the presence of sarcopenia. To examine the associations between sarcopenia (independent variable of interest) and patients’ QOL and mood (dependent variables), we computed linear regression models adjusting for potential confounders, including age, sex, marital status, education, and cancer type [25], [26]. We performed our statistical analyses using SPSS version 17.0 (IBM, Armonk, NY, www.ibm.com).
Results
Participant Sample
From May 2011 to July 2015, we enrolled 350 of 480 (72.9%) eligible patients, and for the current study we included 237 participants who had evaluable baseline CT scans. We compared participant characteristics between those with and without evaluable CT scans and found that these groups only differed across religion and not any other characteristic (supplemental online Table 1). Sample characteristics are presented in Table 1. Participants (mean age, 64.41 ± SD 10.93 years) were primarily white (93.2%), and the majority were male (54.0%) and married (70.5%) and had a lung cancer diagnosis (56.5%).
Table 1. Baseline characteristics of study participants.
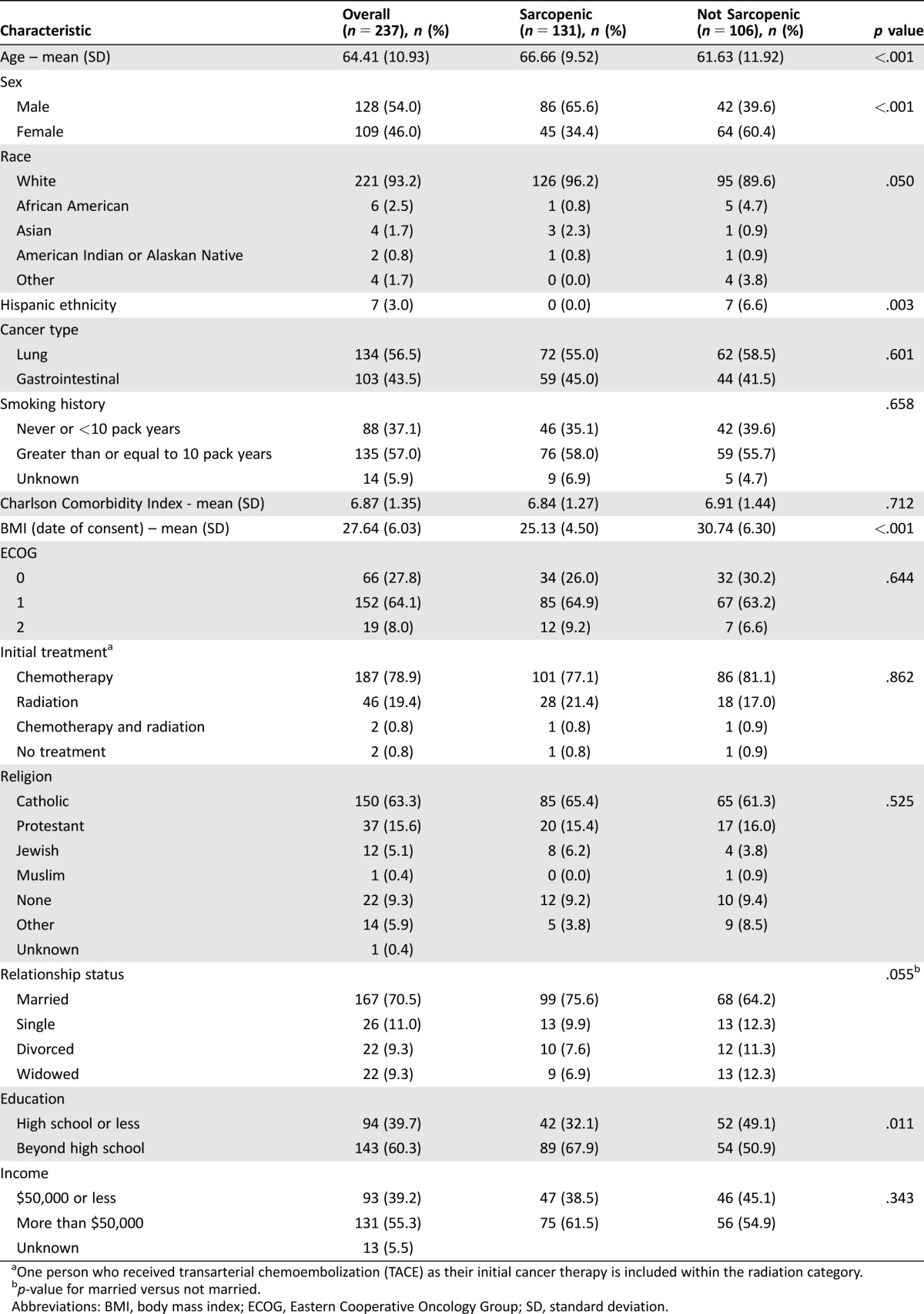
One person who received transarterial chemoembolization (TACE) as their initial cancer therapy is included within the radiation category.
p‐value for married versus not married.
Abbreviations: BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; SD, standard deviation.
Sarcopenia
Over half (55.3%) of patients had sarcopenia (supplemental online Fig. 1). Patients with sarcopenia were older (66.66 years vs. 61.63 years, p < .001) and more likely to be male (65.6% vs. 39.6%, p < .001), of non‐Hispanic ethnicity (0.0% vs. 6.6%, p = .003), and educated beyond high school (67.9% vs. 50.9%, p = .011). Multivariable logistic regression analyses showed that older age (odds ratio [OR] = 1.05, p = .002), white race (OR = 5.03, p = .02), and education beyond high school (OR = 1.95, p = .047) were associated with higher likelihood of sarcopenia, whereas female sex (OR = 0.25, p < .001) and higher body mass index (BMI; OR = 0.79, p < .001) were associated with lower likelihood of sarcopenia (Table 2).
Table 2. Associations between patient characteristics and sarcopenia.
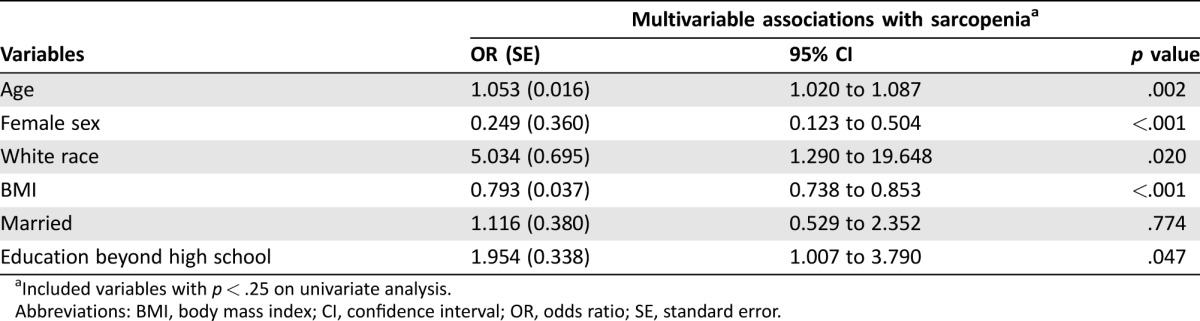
Included variables with p < .25 on univariate analysis.
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio; SE, standard error.
Associations Between Sarcopenia and Patient‐Reported Measures
Using linear regression adjusting for patients’ age, sex, marital status, education, and cancer type, we found that sarcopenia was associated with worse QOL (Table 3). Specifically, sarcopenia was associated with lower FACT‐G scores (unstandardized coefficient [B] = −4.26, standard error [SE] = 2.15, 95% confidence interval [CI] = −8.49 to −0.03, p = .048).
Table 3. Associations between sarcopenia and patient‐reported outcomes.
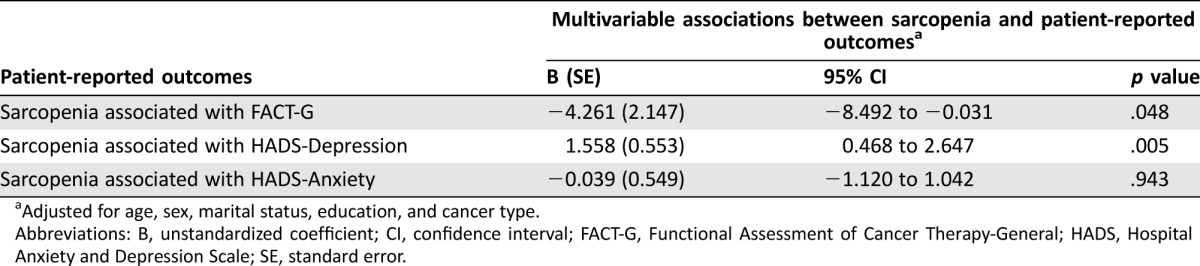
Adjusted for age, sex, marital status, education, and cancer type.
Abbreviations: B, unstandardized coefficient; CI, confidence interval; FACT‐G, Functional Assessment of Cancer Therapy‐General; HADS, Hospital Anxiety and Depression Scale; SE, standard error.
We also found an association between sarcopenia and HADS‐depression (Fig. 2). Patients with sarcopenia had higher rates of clinically significant depression symptoms (29.0% vs. 16.0%, p = .021). On multivariable linear regression, we found that sarcopenia was associated with higher HADS‐depression scores (B = 1.56, SE = 0.55, 95% CI = 0.47 to 2.65, p = .005). We did not find a significant association between sarcopenia and HADS‐anxiety (B = −0.04, SE = 0.55, 95% CI = −1.12 to 1.04, p = .943).
Figure 2.

Depression and anxiety among sarcopenic and nonsarcopenic patients.
Abbreviations: HADS, Hospital Anxiety and Depression Scale.
Discussion
In this exploratory analysis of patients with newly diagnosed, incurable lung and gastrointestinal cancer, we found that sarcopenia was associated with worse QOL and greater depression symptoms. Notably, patients in our sample were newly diagnosed, yet over half met criteria for sarcopenia on CT images acquired for routine clinical care. We also demonstrated a statistically significant relationship between the presence of sarcopenia and certain patient characteristics, such as age and sex. The remarkably high rates of sarcopenia in our sample, coupled with the negative impact of low muscle mass on patient outcomes in this population, underscore the critical need to address this issue early in the disease course for patients with advanced cancer.
Our work highlights the considerably high prevalence of sarcopenia among patients with newly diagnosed, incurable cancer. Over half of patients met criteria for sarcopenia, which is higher than a prior study involving patients with lung and gastrointestinal cancer, and may be related to the fact that our study involved patients with advanced cancer, whereas the prior study included patients of all stages [27]. A more comprehensive understanding of the frequency and impact of sarcopenia in this population can be instrumental in (a) identifying patients at risk for experiencing sarcopenia, (b) understanding how sarcopenia can influence patient outcomes, and (c) providing additional services to meet the supportive care needs of these patients. Additionally, by demonstrating the negative association between sarcopenia and patients’ QOL and mood soon after their cancer diagnosis, our work provides compelling evidence supporting the need for interventions, such as consultation with nutrition specialists or recommendations for exercise, to address sarcopenia and target patients earlier in their cancer course [28], [29], [30], [31]. Thus, our study successfully identifies the highly prevalent and problematic issue of sarcopenia in patients with newly diagnosed, incurable cancer, which can enable us to better support this population, improve the quality of their care, and enhance patient outcomes.
To our knowledge, this is the first study to report that sarcopenia, assessed using CT scans collected as part of routine care, is associated with both QOL and depression symptoms in patients with newly diagnosed, incurable cancer. Researchers have postulated that the physical decline associated with sarcopenia reduces patients’ functional ability, which can adversely impact the QOL of patients with cancer [32], [33]. Similarly, the relationship between depressive symptoms and patients’ lack of appetite and diminished physical activity may provide a mechanism linking sarcopenia and depression among patients with cancer [33], [34], [35], [36]. Importantly, our findings will inform future efforts to address sarcopenia earlier in the cancer trajectory in order to improve outcomes for this highly symptomatic population [19], [37], [38], [39]. By evaluating patients with advanced cancer for the presence of sarcopenia at the time of diagnosis using routinely performed CT scans, we can identify those at higher risk for poor physical and emotional well‐being and begin to implement strategies to better meet the needs of these individuals.
Notably, we identified patient characteristics associated with the presence of sarcopenia. We found that older patients were more likely to meet criteria for sarcopenia, a finding that aligns with the geriatric literature [6], [40], [41]. Research suggests that older patients frequently experience diminished skeletal muscle mass and changes in muscle quality, thought to be related to neurologic, metabolic, hormonal, nutritional, and physical‐activity‐related factors [41], [42], [43]. In turn, these changes in muscle mass and function can lead to disability, diminished mobility, functional dependence, and falls [11], [44], [45]. Clinically, our findings support the need for oncologists to screen for sarcopenia in older adults with advanced cancer and address their nutritional and functional status early in the course of their care. We also found that female patients were less likely to have sarcopenia than males, consistent with previous work [6], [46], [47]. A potential explanation is that the pattern of muscle loss may differ between male and female patients, as research has previously demonstrated [48], [49], [50]. Moreover, another explanation may relate to the different sex‐specific cutoffs used to quantify sarcopenia, which although consistent with consensus guidelines, may differ in certain populations. In addition, we found that education beyond high school was associated with higher likelihood of sarcopenia. This finding is hypothesis‐generating, and additional research should seek to confirm and expand upon this result. Collectively, our findings help identify individuals at higher risk for having sarcopenia soon after the diagnosis of advanced cancer and should help inform future efforts to target these patients with interventions tailored to their needs.
Several limitations of our study warrant consideration. First, we performed this study at a single academic cancer center in a patient sample with limited racial and ethnic diversity. Thus, our findings may not generalize to other, more heterogeneous populations, and additional research should seek to confirm our results in more diverse populations. Second, this study included patients who had enrolled in a randomized trial of early palliative care, and these patients may differ from those who choose not to participate in clinical trials. Also, by excluding patients already receiving palliative care services and those who needed immediate referral for palliative care or hospice, we may be underestimating the prevalence of sarcopenia, as these excluded patients may have had more advanced sarcopenia than those enrolled. Third, we did not collect information about whether patients utilized other services, such as physical and occupational therapy or dietary and nutrition services, which may affect patients’ ability to maintain muscle mass [30], [51], [52], [53]. Notably, participants are unlikely to have extensively received these services, as we conducted the study early in patients’ disease course. In addition, we lack information regarding weight loss for the participants in this study, and therefore cannot comment on how weight change influences sarcopenia and patient‐reported outcomes. Furthermore, although prior research has shown differential effects of sarcopenia on patient outcomes depending on patient BMI, we do not have the sample size for BMI‐specific subgroup analyses [6], [27]. Finally, the cross‐sectional nature of our study allows us only to report associations between sarcopenia and patients’ QOL and mood, and thus we cannot state the directionality of the relationships. In addition, without longitudinal data, our study does not provide information about how changes in muscle mass throughout the cancer trajectory may further influence patients’ QOL and mood.
Conclusion
In summary, we demonstrated that patients with newly diagnosed, incurable cancer experience high rates of sarcopenia assessed using CT scans performed as part of routine clinical care. It is noteworthy that patients with sarcopenia report worse QOL and greater depression symptoms, as this highlights an important need for interventions to address muscle loss early in the course of illness among patients with incurable cancer. Future research should focus on determining the optimal timing and modality of efforts to assess and treat sarcopenia while working to improve the QOL and mood outcomes of patients with advanced cancer.
See http://www.TheOncologist.com for supplemental material available online.
Supplementary Material
Acknowledgments
This study was supported by grants from the National Institute of Nursing Research (R01 NR012735) and the National Cancer Institute (K24 CA181253).
Contributed equally as co‐first authors
Contributed equally as co‐senior authors
Footnotes
For Further Reading: Hánah N. Rier, Agnes Jager, Stefan Sleijfer et al. The Prevalence and Prognostic Value of Low Muscle Mass in Cancer Patients: A Review of the Literature. The Oncologist 2016;21:1396‐1409.
Implications for Practice: An increasing number of studies underline the clinical value of low muscle mass as a prognostic factor for adverse outcomes in cancer patients. However, studies show large heterogeneity because of the lack of a standardized approach to measure muscle mass and the lack of reference populations. As a result, the interpretation of data and further progress are severely hampered, hindering the implementation of muscle measurement in oncological care. This review summarizes the methods of diagnosing low muscle mass in cancer patients, the difference between underlying syndromes such as sarcopenia and cachexia, and the association with clinical outcomes described so far.
Author Contributions
Conception/design: Ryan D. Nipp, Georg Fuchs, Areej El‐Jawahri, Julia Mario, Fabian M. Troschel, Joseph A. Greer, Emily R. Gallagher, Vicki A. Jackson, Avinash Kambadakone, Theodore S. Hong, Jennifer S. Temel, Florian J. Fintelmann
Provision of study material or patients: Ryan D. Nipp, Georg Fuchs, Areej El‐Jawahri, Julia Mario, Fabian M. Troschel, Joseph A. Greer, Emily R. Gallagher, Vicki A. Jackson, Avinash Kambadakone, Theodore S. Hong, Jennifer S. Temel, Florian J. Fintelmann
Collection and/or assembly of data: Ryan D. Nipp, Georg Fuchs, Areej El‐Jawahri, Julia Mario, Fabian M. Troschel, Joseph A. Greer, Emily R. Gallagher, Vicki A. Jackson, Avinash Kambadakone, Theodore S. Hong, Jennifer S. Temel, Florian J. Fintelmann
Data analysis and interpretation: Ryan D. Nipp, Georg Fuchs, Areej El‐Jawahri, Julia Mario, Fabian M. Troschel, Joseph A. Greer, Emily R. Gallagher, Vicki A. Jackson, Avinash Kambadakone, Theodore S. Hong, Jennifer S. Temel, Florian J. Fintelmann
Manuscript writing: Ryan D. Nipp, Georg Fuchs, Areej El‐Jawahri, Julia Mario, Fabian M. Troschel, Joseph A. Greer, Emily R. Gallagher, Vicki A. Jackson, Avinash Kambadakone, Theodore S. Hong, Jennifer S. Temel, Florian J. Fintelmann
Final approval of manuscript: Ryan D. Nipp, Georg Fuchs, Areej El‐Jawahri, Julia Mario, Fabian M. Troschel, Joseph A. Greer, Emily R. Gallagher, Vicki A. Jackson, Avinash Kambadakone, Theodore S. Hong, Jennifer S. Temel, Florian J. Fintelmann
Disclosures
The authors indicated no financial relationships.
References
- 1. Dewys WD, Begg C, Lavin PT et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med 1980;69:491–497. [DOI] [PubMed] [Google Scholar]
- 2. Fearon KC. Cancer cachexia: Developing multimodal therapy for a multidimensional problem. Eur J Cancer 2008;44:1124–1132. [DOI] [PubMed] [Google Scholar]
- 3. Shachar SS, Deal AM, Weinberg M et al. Skeletal muscle measures as predictors of toxicity, hospitalization, and survival in patients with metastatic breast cancer receiving taxane‐based chemotherapy. Clin Cancer Res 2017;23:658–665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Shachar SS, Williams GR, Muss HB et al. Prognostic value of sarcopenia in adults with solid tumours: A meta‐analysis and systematic review. Eur J Cancer 2016;57:58–67. [DOI] [PubMed] [Google Scholar]
- 5. Del Fabbro E, Parsons H, Warneke CL et al. The relationship between body composition and response to neoadjuvant chemotherapy in women with operable breast cancer. The Oncologist 2012;17:1240–1245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Prado CM, Lieffers JR, McCargar LJ et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population‐based study. Lancet Oncol 2008;9:629–635. [DOI] [PubMed] [Google Scholar]
- 7. Tisdale MJ. Mechanisms of cancer cachexia. Physiol Rev 2009;89:381–410. [DOI] [PubMed] [Google Scholar]
- 8. Mantovani G, Macciò A, Lai P et al. Cytokine activity in cancer‐related anorexia/cachexia: Role of megestrol acetate and medroxyprogesterone acetate. Semin Oncol 1998;25(2 suppl 6):45–52. [PubMed] [Google Scholar]
- 9. Argilés JM, Alvarez B, López‐Soriano FJ. The metabolic basis of cancer cachexia. Med Res Rev 1997;17:477–498. [DOI] [PubMed] [Google Scholar]
- 10. Gewandter JS, Dale W, Magnuson A et al. Associations between a patient‐reported outcome (PRO) measure of sarcopenia and falls, functional status, and physical performance in older patients with cancer. J Geriatr Oncol 2015;6:433–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc 2002;50:889–896. [DOI] [PubMed] [Google Scholar]
- 12. Velikova G, Wright P, Smith AB et al. Self‐reported quality of life of individual cancer patients: Concordance of results with disease course and medical records. J Clin Oncol 2001;19:2064–2073. [DOI] [PubMed] [Google Scholar]
- 13. Loprinzi CL. Management of cancer anorexia/cachexia. Support Care Cancer 1995;3:120–122. [DOI] [PubMed] [Google Scholar]
- 14. Muscaritoli M, Anker SD, Argiles J et al. Consensus definition of sarcopenia, cachexia and pre‐cachexia: joint document elaborated by Special Interest Groups (SIG) “cachexia‐anorexia in chronic wasting diseases” and “nutrition in geriatrics.” Clin Nutr 2010;29:154–159. [DOI] [PubMed] [Google Scholar]
- 15. Fearon K, Strasser F, Anker SD et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol 2011;12:489–495. [DOI] [PubMed] [Google Scholar]
- 16. Broughman JR, Williams GR, Deal AM et al. Prevalence of sarcopenia in older patients with colorectal cancer. J Geriatr Oncol 2015;6:442–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Heymsfield SB, McManus CB. Tissue components of weight loss in cancer patients: A new method of study and preliminary observations. Cancer 1985;55(1 suppl):238–249. [DOI] [PubMed] [Google Scholar]
- 18. Thoresen L, Frykholm G, Lydersen S et al. Nutritional status, cachexia and survival in patients with advanced colorectal carcinoma. Different assessment criteria for nutritional status provide unequal results. Clin Nutr 2013;32:65–72. [DOI] [PubMed] [Google Scholar]
- 19. Teunissen SC, Wesker W, Kruitwagen C et al. Symptom prevalence in patients with incurable cancer: A systematic review. J Pain Symptom Manage 2007;34:94–104. [DOI] [PubMed] [Google Scholar]
- 20. Davis MP, Dreicer R, Walsh D et al. Appetite and cancer‐associated anorexia: A review. J Clin Oncol 2004;22:1510–1517. [DOI] [PubMed] [Google Scholar]
- 21. Temel JS, Greer JA, El‐Jawahri A et al. Effects of early integrated palliative care in patients with lung and GI cancer: A randomized clinical trial. J Clin Oncol 2017;35:834–841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Cella DF, Tulsky DS, Gray G et al. The Functional Assessment of Cancer Therapy scale: Development and validation of the general measure. J Clin Oncol 1993;11:570–579. [DOI] [PubMed] [Google Scholar]
- 23. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361–370. [DOI] [PubMed] [Google Scholar]
- 24. Mitsiopoulos N, Baumgartner RN, Heymsfield SB et al. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J Appl Physiol (1985). 1998;85:115–122. [DOI] [PubMed] [Google Scholar]
- 25. Parker PA, Baile WF, de Moor C et al. Psychosocial and demographic predictors of quality of life in a large sample of cancer patients. Psychooncology 2003;12:183–193. [DOI] [PubMed] [Google Scholar]
- 26. Nipp RD, Greer JA, Traeger L et al. Which patients experience improved quality of life (QOL) and mood from early palliative care (PC)? J Clin Oncol 2014;32,(suppl 31):16a. [Google Scholar]
- 27. Martin L, Birdsell L, Macdonald N et al. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol 2013;31:1539–1547. [DOI] [PubMed] [Google Scholar]
- 28. Baldwin C, Spiro A, Ahern R et al. Oral nutritional interventions in malnourished patients with cancer: A systematic review and meta‐analysis. J Natl Cancer Inst 2012;104:371–385. [DOI] [PubMed] [Google Scholar]
- 29. Galvão DA, Taaffe DR, Spry N et al. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: A randomized controlled trial. J Clin Oncol 2010;28:340–347. [DOI] [PubMed] [Google Scholar]
- 30. Segal RJ, Reid RD, Courneya KS et al. Resistance exercise in men receiving androgen deprivation therapy for prostate cancer. J Clin Oncol 2003;21:1653–1659. [DOI] [PubMed] [Google Scholar]
- 31. Courneya KS, Segal RJ, Mackey JR et al. Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial. J Clin Oncol 2007;25:4396–4404. [DOI] [PubMed] [Google Scholar]
- 32. Keogh JW, MacLeod RD. Body composition, physical fitness, functional performance, quality of life, and fatigue benefits of exercise for prostate cancer patients: A systematic review. J Pain Symptom Manage 2012;43:96–110. [DOI] [PubMed] [Google Scholar]
- 33. Illman J, Corringham R, Robinson D Jr. et al. Are inflammatory cytokines the common link between cancer‐associated cachexia and depression? J Support Oncol 2005;3:37–50. [PubMed] [Google Scholar]
- 34. Bukberg J, Penman D, Holland JC. Depression in hospitalized cancer patients. Psychosom Med 1984;46:199–212. [DOI] [PubMed] [Google Scholar]
- 35. Jeejeebhoy KN. Malnutrition, fatigue, frailty, vulnerability, sarcopenia and cachexia: Overlap of clinical features. Curr Opin Clin Nutr Metab Care 2012;15:213–219. [DOI] [PubMed] [Google Scholar]
- 36. Dy SM, Lorenz KA, Naeim A et al. Evidence‐based recommendations for cancer fatigue, anorexia, depression, and dyspnea. J Clin Oncol 2008;26:3886–3895. [DOI] [PubMed] [Google Scholar]
- 37. Miovic M, Block S. Psychiatric disorders in advanced cancer. Cancer 2007;110:1665–1676. [DOI] [PubMed] [Google Scholar]
- 38. Lutz S, Norrell R, Bertucio C et al. Symptom frequency and severity in patients with metastatic or locally recurrent lung cancer: A prospective study using the Lung Cancer Symptom Scale in a community hospital. J Palliat Med 2001;4:157–165. [DOI] [PubMed] [Google Scholar]
- 39. Chang VT, Hwang SS, Feuerman M et al. Symptom and quality of life survey of medical oncology patients at a Veterans Affairs medical center: A role for symptom assessment. Cancer 2000;88:1175–1183. [DOI] [PubMed] [Google Scholar]
- 40. Cruz‐Jentoft AJ, Landi F, Topinková E et al. Understanding sarcopenia as a geriatric syndrome. Curr Opin Clin Nutr Metab Care 2010;13:1–7. [DOI] [PubMed] [Google Scholar]
- 41. Doherty TJ. Invited review: Aging and sarcopenia. J Appl Physiol (1985) 2003;95:1717–1727. [DOI] [PubMed] [Google Scholar]
- 42. Roubenoff R, Hughes VA. Sarcopenia: Current concepts. J Gerontol A Biol Sci Med Sci 2000;55:M716–M724. [DOI] [PubMed] [Google Scholar]
- 43. Welle S. Cellular and molecular basis of age‐related sarcopenia. Can J Appl Physiol. 2002;27:19–41. [DOI] [PubMed] [Google Scholar]
- 44. Lauretani F, Russo CR, Bandinelli S et al. Age‐associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J Appl Physiol (1985) 2003;95:1851–1860. [DOI] [PubMed] [Google Scholar]
- 45. Landi F, Liperoti R, Russo A et al. Sarcopenia as a risk factor for falls in elderly individuals: Results from the ilSIRENTE study. Clin Nutr 2012;31:652–658. [DOI] [PubMed] [Google Scholar]
- 46. Barret M, Antoun S, Dalban C et al. Sarcopenia is linked to treatment toxicity in patients with metastatic colorectal cancer. Nutr Cancer 2014;66:583–589. [DOI] [PubMed] [Google Scholar]
- 47. Morishita S, Kaida K, Tanaka T et al. Prevalence of sarcopenia and relevance of body composition, physiological function, fatigue, and health‐related quality of life in patients before allogeneic hematopoietic stem cell transplantation. Support Care Cancer 2012;20:3161–3168. [DOI] [PubMed] [Google Scholar]
- 48. Melton LJ 3rd, Khosla S, Crowson CS et al. Epidemiology of sarcopenia. J Am Geriatr Soc 2000;48:625–630. [PubMed] [Google Scholar]
- 49. Janssen I, Heymsfield SB, Wang ZM et al. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J Appl Physiol (1985) 2000;89:81–88. [DOI] [PubMed] [Google Scholar]
- 50. Goodpaster BH, Park SW, Harris TB et al. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J Gerontol A Biol Sci Med Sci 2006;61:1059–1064. [DOI] [PubMed] [Google Scholar]
- 51. Bauer JD, Capra S. Nutrition intervention improves outcomes in patients with cancer cachexia receiving chemotherapy: A pilot study. Support Care Cancer 2005;13:270–274. [DOI] [PubMed] [Google Scholar]
- 52. Mello M, Tanaka C, Dulley FL. Effects of an exercise program on muscle performance in patients undergoing allogeneic bone marrow transplantation. Bone Marrow Transplant 2003;32:723–728. [DOI] [PubMed] [Google Scholar]
- 53. Pergolotti M, Williams GR, Campbell C et al. Occupational therapy for adults with cancer: Why it matters. The Oncologist 2016;21:314–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.