

Abstract
Background
Ambient fine particulate matter (PM2.5) pollution is currently a serious environmental problem in China, but evidence of health effects with higher resolution and spatial coverage is insufficient.
Objective
This study aims to provide a better overall understanding of long-term mortality effects of PM2.5 pollution in China and a county-level spatial map for estimating PM2.5 related premature deaths of the entire country.
Method
Using four sets of satellite-derived PM2.5 concentration data and the integrated exposure-response model which has been employed by the Global Burden of Disease (GBD) to estimate global mortality of ambient and household air pollution in 2010, we estimated PM2.5 related premature mortality for five endpoints across China in 2010.
Result
Premature deaths attributed to PM2.5 nationwide amounted to 1.27 million in total, and 119,167, 83,976, 390,266, 670,906 for adult chronic obstructive pulmonary disease, lung cancer, ischemic heart disease, and stroke, respectively; 3995 deaths for acute lower respiratory infections were estimated in children under the age of 5. About half of the premature deaths were from counties with annual average PM2.5 concentrations above 63.61 μg/m3, which cover 16.97% of the Chinese territory. These counties were largely located in the Beijing-Tianjin-Hebei region and the North China Plain. High population density and high pollution areas exhibited the highest health risks attributed to air pollution. On a per capita basis, the highest values were mostly located in heavily polluted industrial regions.
Conclusion
PM2.5-attributable health risk is closely associated with high population density and high levels of pollution in China. Further estimates using long-term historical exposure data and concentration-response (C-R) relationships should be completed in the future to investigate longer-term trends in the effects of PM2.5.
Keywords: Multi-model PM2.5, Chronic mortality effect, Spatial, County-level, China
1. Introduction
Fine particulate matter (particles ≤2.5 μm in aerodynamic diameter; PM2.5) is a major concern for public health. PM2.5 has been found to be associated with both short-term and long-term adverse health effects (Dockery et al., 1993; Schwartz, 2000; Laden et al., 2000; Kunzli et al., 2001; Boldo et al., 2006; Chow et al., 2006; Pope and Dockery, 2013; Lu et al., 2015). According to the Global Burden of Disease (GBD) 2010 assessment, 3.2 million premature deaths per year were attributable to ambient PM2.5 exposure, and PM2.5 is one of the leading risk factors for premature mortality (Cohen et al., 2012). For China, ambient PM pollution ranked fourth in leading risk factors and was associated with 1.2 million premature deaths per year (Lim et al., 2012; Yang et al., 2013). Haze and smog (characterized by high concentrations of PM2.5) has been a critical social issue in China. An accurate assessment of the health effects related to PM2.5 exposure is needed for evidence-based priority setting at the local level in China.
The short-term effects of PM2.5 in China have been well studied in recent years (Guo et al., 2010; Chen et al., 2012; Lu et al., 2015), which has served as the corner stone of countermeasures and policy making. However, to-date, there has been little epidemiologic work on the chronic effects of PM2.5 in China, due in part to the lack of long-term air monitoring data and the lack of scientific exposure-response relationship for regions with high PM2.5 concentration. Techniques for deriving PM2.5 from remote sensing data based on ground monitoring data and land-use information have been evolving, and PM2.5 can now be determined with relatively high accuracy. Some models have been de-veloped to estimate long-term historical PM2.5 exposure, including satellite-based aerosol optical depth (AOD) models, land-use regression models, chemical transport model (CTM) simulations and other integrated models (Kloog et al., 2014; Brauer et al., 2016; Di et al., 2016; Ma et al., 2016; Van Donkelaar et al., 2016). These techniques have also been used to estimate the global and regional mortality associated with PM2.5 (Evans et al., 2013; Lim et al., 2012). However, previous studies are mostly based on single model for the PM2.5 exposure estimate, which bring much uncertainty. To better express modeling estimate uncertainty, the multi-model method has been applied in several studies especially studies on climate and health, which can be applied in the PM2.5 exposure estimates (Kinney et al., 2008; Jerrett et al., 2017; Silva et al., 2017).
To achieve a better exposure-response curve in more polluted regions, Burnett et al. (2014), building on Pope et al. (2009, 2011), developed integrated exposure-response functions (IERs) that constrain the shape of the concentration-response (C-R) relationship using epidemiologic data derived from higher exposure concentrations (e.g., household air pollution from the use of solid fuels, secondhand tobacco smoke, active tobacco smoking). Following GBD 2010, Apte et al. (2015) employed those IERs to estimate relative risks attributable to PM2.5 exposure for five major endpoints (for adults: ischemic heart disease (IHD), chronic obstructive pulmonary disease (COPD), lung cancer (LNC), and stroke; for children under the age of 5: acute lower respiratory infections (ALRI)) and estimated that 3.24 million premature deaths were attributable to PM2.5 worldwide in 2010, and this result is in accordance with the estimates of GBD 2010.
Following these achievements in estimating long-term exposure and attributive relative risk (RR) of PM2.5 for higher exposure concentrations, a few studies have attempted to estimate the long-term chronic effects of PM2.5 in China (Xie et al., 2016; J. Liu et al., 2016a; M. Liu et al., 2016b), using these satellite-derived PM2.5 data and similar methods to those employed by the GBD 2010 assessment and Apte et al. (2015). However, there are variations among these studies due to differentiations of data sources and modeling methods. The estimated PM2.5 exposure from each individual model also requires further verification and comparison. Furthermore, these previous studies are all based on city-level or grid data of populations at all ages, and failed to take into consideration multi-model PM2.5 data and the differences among age groups. In fact, the attributive relative risk (RR) varies greatly among different age groups and different counties within a city/province. China has > 2850 counties, and the county is a key unit for administration and policy making in China.
Therefore, to address the above problems, this study uses multi-model PM2.5 concentration data, county-level population data, and C-R relationships for the full range of PM2.5 concentrations to estimate the PM2.5 related health effects for each county in China, and analyzes the spatial patterns and regional characteristics of these estimates for the entire country.
2. Materials and methods
The key elements of the PM2.5 risk assessment include an exposure assessment, population in the study area, baseline health incidence information, and the PM2.5C-R function from epidemiological studies.
2.1. PM2.5 concentration data
We used the annual mean PM2.5 concentration in 2010 as the exposure in our model. The multi-source PM2.5 concentration estimates were based on four different satellite-derived models (Supplemental Table S1). We estimated annual mean PM2.5 concentration for each county using zonal statistic tools (Supplemental Fig. S1).
2.2. Demographic data
The county-level age-specific demographic data in this study are from the sixth demographic census of China in 2010. This dataset includes information on populations for each age group from 0 to 84 years old in 5-year intervals, and the group for 85 years of age or older. There were about 2860 counties in China in 2010, but we include 2826 counties in our model, and a total population of 1.325 billion, since demographic data for a few counties were missing or could not be matched with the county map (to join with the PM2.5 data).
2.3. Baseline mortality data
Ideally, the county-level estimates should use county-level baseline mortality data, but because these data are not available in China, we instead use provincial-level data. The age-specific mortality rate for each disease was obtained from Zhou et al. (2015) and the results of GBD 2013 studies (Naghavi et al., 2015). The data table is provided in the Supplementary Materials (Table S2 and Supplementary Materials-2).
2.4. The C-R function
A C-R function is a mathematical equation that describes the relationship between exposure (long-term exposure to PM2.5) and the risk of a health outcome (mortality of each endpoint). The C-R function expresses the relative risk of mortality associated with an incremental change in PM2.5 concentration. In this study, the C-R functions and relative risk (Eq. (1)) were based on the integrated exposure-response functions (IERs) GBD 2010 (Burnett et al., 2014) and Apte et al. (2015), across the full range of PM2.5 concentrations.
| (1) |
RRIER(z) represents the relative risk in the PM2.5 exposure concentration of z (in micrograms per meter cubed); zcfis the counterfactual concentration below which we assumed there is no additional risk. For very large z, RRIER approximates 1 + α. A power of PM2.5, δ, was included here to predict risk over a very large range of concentrations (Burnett et al., 2014).
2.5. Modeling
We adapted a calculation approach developed for GBD 2010 to estimate PM2.5-related premature mortality in each county, and the following five endpoints are included in our estimation: IHD, COPD, LNC, and stroke in adults, and ALRI in children under 5-years-old. For IHD and stroke, the RR is different between age strata, and for COPD and LNC, the RR in the same exposure concentration is the same for the entire group of adults (aged 25 or more) (Apte et al., 2015). We estimated the premature mortality Mij of each county (and of each age stratum for IHD and stroke) and disease endpoint j attributable to ambient PM2.5 for county i located in region k.
| (2) |
represents the hypothetical “underlying incidence” (i.e., cause-specific mortality rate) that would remain for region k if PM2.5 concentrations were reduced to the theoretical minimum risk concentration throughout that region.
Here, Pi is the population of county i, Ij,k is the reported regional average annual disease incidence (mortality) rate for endpoint j in region k, Ci represents the annual-average PM2.5 concentration in county i, RRj (Ci) is the relative risk for end point j at concentration Ci, and , as defined below, represents the average population-weighted relative risk for end point j within region k:
| (3) |
In addition to the absolute number of premature deaths associated with PM2.5, we also computed per-capita impacts. Per-capita mortality eliminates the influence of population density when examining spatial patterns of the effects of PM2.5. Furthermore, the territorial area differs significantly among different counties; a county with a large number of PM2.5 related deaths may still have a low per-unit-area mortality due to its large territorial area. To resolve this problem, an indicator of ‘per-unit-area mortality’ was applied to see the spatial patterns of PM2.5 related premature mortality. Therefore, the per-capita and per-unit-area mortality for each county were calculated, and maps were made to see the spatial variations in impacts independent of population density. Provincial-level statistics were also explored to see the variations among different provinces.
3. Results
3.1. Total attributive deaths for different diseases
For each of the 2826 counties, PM2.5-related deaths in 2010 by specific causes (stroke, COPD, LNC, IHD and ALRI) were evaluated. For the four types of PM2.5 exposure data and two types of cause-specific baseline mortality data, we obtained eight groups of estimates. The total number of premature deaths from stroke, COPD, LNC, IHD and ALRI attributable to ambient PM2.5 in 2010 ranges from 1.18 million to 1.38 million based on different model-inputs, and the PM2.5-related premature mortality was 95.72/105 persons (Table 1). The average number of premature deaths from the eight model estimates (1.27 million) is close to that of the results of GBD 2010 and is in accordance with previous studies (Fig. 1).
Table 1.
PM2.5-related premature deaths in China in 2010 (×1000 deaths).
| No. | PM2.5 data set | Mortality data set | COPD | LNC | ALRI | IHD | Stroke | Total | Per capita deaths/105 | /100 km2 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Satellite-Ma et al., 2016 | Zhou’s + GBD | 148.82 | 98.17 | 5.26 | 412.41 | 719.66 | 1384.31 | 104.47 | 14.55 |
| 2 | Satellite-Ma et al., 2016 | GBD | 121.34 | 90.69 | 4.07 | 412.41 | 719.66 | 1348.16 | 101.74 | 14.17 |
| 3 | GBD 2010 | Zhou’s + GBD | 133.62 | 88.79 | 4.61 | 392.12 | 674.68 | 1293.81 | 97.64 | 13.60 |
| 4 | GBD 2010 | GBD | 109.39 | 82.06 | 3.57 | 392.12 | 674.68 | 1261.82 | 95.23 | 13.26 |
| 5 | ACAG-dust | Zhou’s + GBD | 116.35 | 78.01 | 3.87 | 374.98 | 638.08 | 1211.28 | 91.41 | 12.73 |
| 6 | ACAG-dust | GBD | 94.97 | 72.14 | 2.99 | 374.98 | 638.08 | 1183.16 | 89.29 | 12.44 |
| 7 | NASA | Zhou’s + GBD | 125.45 | 84.01 | 4.27 | 381.57 | 651.21 | 1246.51 | 94.07 | 13.10 |
| 8 | NASA | GBD | 103.40 | 77.93 | 3.32 | 381.57 | 651.21 | 1217.42 | 91.88 | 12.80 |
| 9 | Average | 119.17 | 83.98 | 4.00 | 390.27 | 670.91 | 1268.31 | 95.72 | 13.33 |
Note: the left three column means the eight estimating scenarios based on the two kinds of cause-specific mortality data and four types of PM2.5 exposure data. The line No. 9 represents the average of the eight model estimates.
Fig. 1.
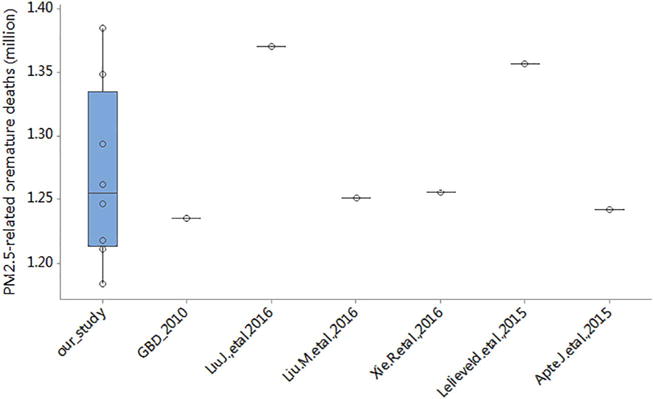
PM2.5-related premature deaths of our study and previous studies.
We compared our estimates with those of other recent studies in China and worldwide (Table S3), including the studies that adopted the IER model (Lim et al., 2012; Lelieveld et al., 2015; Rohde and Muller, 2015; J. Liu et al., 2016a; M. Liu et al., 2016b; Xie et al., 2016) (Fig. 1), and found that our 1.27 million estimate of national premature deaths attributed to PM2.5 in 2010 was close to the results of the following studies: 1.23 million of the GBD 2010 study (Lim et al., 2012), the 1.25 million by M. Liu et al. (2016b) (in 2012, including stroke, IHD and LNC) and the 1.25 million Xie et al. (in 2010, not including ALRI for children). M. Liu et al. (2016b) also used the IER models and a satellite-derived PM2.5 dataset (10 km resolution), and all-age population maps at 1 km resolution in 2010; the endpoint ALRI and COPD death was not included in their study. Xie et al. (2016) explored the long-term trend and spatial pattern of PM2.5 induced premature mortality in China between 2000 and 2010, based on the same 1 km × 1 km grid population density map of China and satellite retrieved PM2.5 concentrations and provincial health data. Our results were lower than the 1.36 million by Lelieveld et al. (2015), the 1.37 million by J. Liu et al. (2016a), and the 1.60 million reported by Rohde and Muller (2015). These differences in PM2.5 related mortality may be due to the use of different data sources for PM2.5 exposure data, the modeling scale, the population data, and the annual incidence rate of mortality for the five diseases. For example, Lelieveld et al. (2015) estimated the global premature deaths related to PM2.5 and O3 based on the method of the GBD 2010, but with an atmospheric chemistry–general circulation model to compute global air quality, combined with country-level population data and health statistics. J. Liu et al. (2016a) estimated the adult mortality attributable to PM2.5 exposure in China at a 45 km × 45 km resolution, using the IERs model but based on PM2.5 measurements from monitoring sites and a regional air quality model; the population data of their study was 1 km × 1 km grid data in 2010, which was not age-specified, and was projected to 2013 based on the provincial population from the China Statistical Yearbook; and they not include ALRI for children, and some north and northwest regions were out of consideration. Rohde and Muller (2015) carried out another study using the IERs, and obtained a PM2.5-attributable mortality of 1.6 million in China. Their population data and pollution data were prefecture city level and the incidence data were based of national average death rates.
Among the PM2.5-related premature deaths, the contribution of stroke is the largest (52.90%), followed by IHD (30.77%); COPD and LC in adults accounted for 9.40% and 6.62%, respectively, and the proportion of ALRI in children was the lowest at around 0.32% (Fig. 2 and Fig. 3; for each of the eight estimates, see Fig. S4). Adult IHD and stroke accounted for > 80% of combined PM2.5-attributable mortality for all five causes, which is higher than the ~70% of the previous global concentration-mortality relationships (Apte et al., 2015), and the 72% from GBD 2010.
Fig. 2.
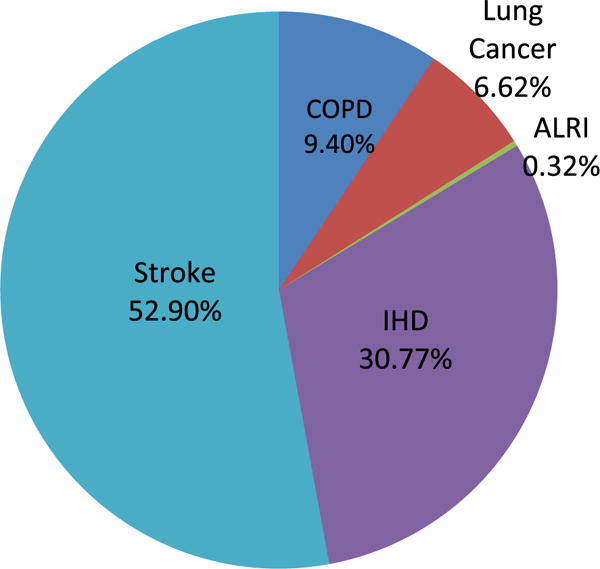
Proportions of PM2.5-related premature deaths for each endpoint.
Fig. 3.
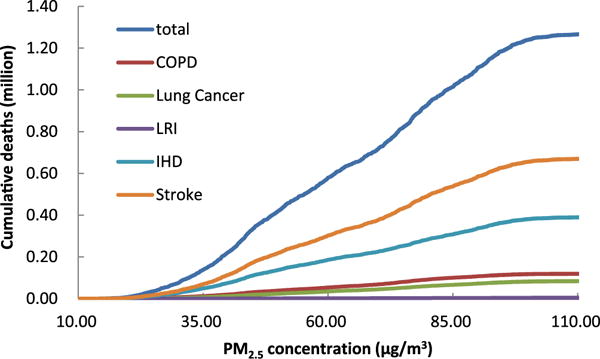
Cumulative numbers of PM2.5-related deaths for each endpoint.
3.2. Total attributive deaths for different diseases
> 58% of the premature deaths were from the elderly group (aged 65 or more); 33.66% in the age group 65–79 and 24.73% in the age group of 80 years old and up (Fig. S5). PM2.5-related premature mortality varies greatly among different age groups (Fig. S6) and increases with age. The oldest group (aged 80 or more) has the highest PM2.5-related premature mortality at 1497 premature deaths/105 persons; the youngest group (aged 5 or less) has the lowest, 5 deaths/105 persons. This indicated the PM2.5-related disease burden among the aged population is much higher than that in the younger.
3.3. The regional patterns in mortality from PM2.5
A map of county-level PM2.5 concentration and the total attributable deaths is shown in Fig. 4 (For specific causes, see Supplementary Information Fig. S2). We can see that the spatial pattern of PM2.5 related deaths follows the pattern of population density. The Beijing-Tianjin-Hebei Region and the North China Plain were the “center” regions with high PM2.5 concentration (Fig. 4-a) and attributable mortality (Fig. 4-b). The Yangtze River Delta Region, the Sichuan Basin (east of Sichuan Province), the central region of the Northeast Plain, the Wuhan Metropolitan Region, and the Changsha - Zhuzhou - Xiangtan Region were ‘sub-centers’ with high attributive mortality next to the above regions. According to the Twelfth Five-year Plan for Air Pollution Control of the Key Areas in China, these above regions are among the most polluted and fastest-developing regions of the ‘Three Districts and Ten Metropolitan Groups’ (The State Council of the People’s Republic of China, 2012). In comparison, the western, northwestern and southern parts of China had lower PM2.5 concentrations and lower disease burdens, especially in the counties with lower population densities. Counties with high levels of pollution and population density, such as Chaoyang and Haidian in Beijing and Nanyang and Luoyang in the North China Plain had the largest number of deaths related to PM2.5, while the highest per capita attributable deaths are all located in heavy-pollution industrial regions such as Anshan and Fushun in Liaoning Province, Tangshan and Hengshui in Hebei province and Kaifeng and Luohe in Henan Province. This regional pattern is generally consistent with previous estimates (J. Liu et al., 2016a; M. Liu et al., 2016b; Xie et al., 2016; Rohde and Muller, 2015; Fang et al., 2016), although there were some variations for different indices. Among the top 20 counties with the largest number of PM2.5 related premature deaths, five were located in Henan Province, three in Beijing and three in Shandong Province; the top three counties were Chaoyang in Beijing, Pudong in Shanghai and Dongguan in Guangdong Province, all highly populated regions. Among the top 20 counties with the highest per unit area deaths, Liaoning province had 5 and Tianjin had 4, and the top 3 counties were Shenhe and Heping in Shenyang, Liaoning Province, and Wuhua in Kunming, Yunnan Province. (For detailed information, please see Supplementary Information Table S4–S6).
Fig. 4.
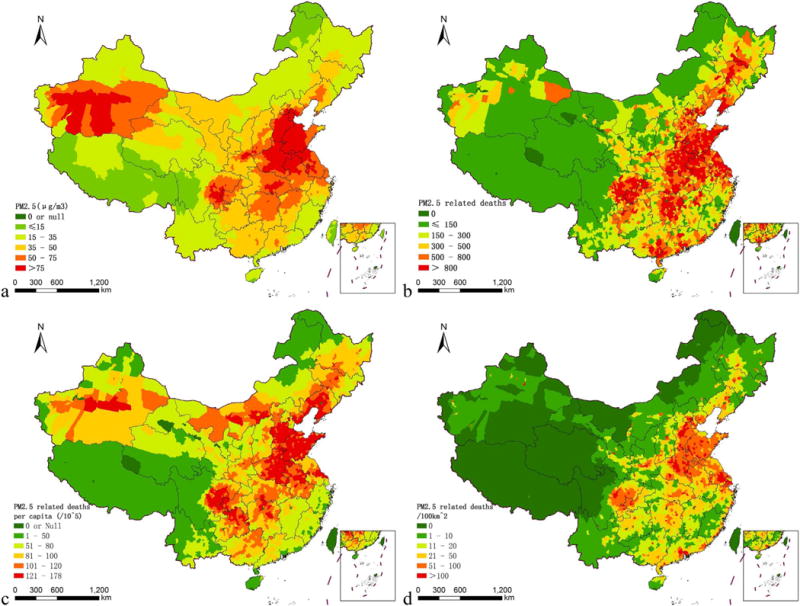
PM2.5 concentration (an average of the four models) and related deaths of China.
With respect to per-capita mortality (Fig. 4-c), vast regions of the North China Plain, including Henan, Shandong, and the southern part of Hebei Province had the highest values. Among the top 20 counties with the highest per capita premature deaths, seven were in Liaoning Province, five were in Hebei Province and five in Henan Province, and the top three counties were Lishan in Anshan, Liaoning Province, Guye district in Tangshan, Hebei Province, and Gulou District in Kaifeng, Henan Province. In highly populated regions such as the Beijing-Tianjin-Hebei region, the Pearl River Delta region, and the Yangtze River Delta region, the per-capita mortality is relatively low despite the high PM2.5 concentration and the large number of attributive deaths. Per-capita mortality in areas of central China such as Hunan, Hubei and Guizhou province were also high, albeit relatively lower than the above-mentioned regions.
The spatial pattern of ‘per-unit-area mortality’ is similar to those for total deaths and per-capita deaths, but still has some differences (Fig. 4-d). Counties in the Yangtze River Delta region and in some metropolitan areas such as Shanghai, Beijing and Tianjin had high ‘per-unit-area mortality’ for both the high levels of pollution and population density. The Pearl River Delta region, where the PM2.5 concentration is relatively low, had high ‘per-unit-area mortality’ mainly resulting from the high population density.
3.4. The cumulative mortality from PM2.5
About one half of the total 1.27 million attributive deaths were under/above the annual average concentration of 63.61 μg/m3, about 0.45 million (35.51% of total deaths) deaths were from counties with annual average PM2.5 concentrations of higher than 75.00 μg/m3, and 0.14 million (10.95%) from counties lower than 35.00 μg/m3 (Fig. 5). For the entire country, there were about 373.2 million people (28.16% of Chinese population) living in areas where the annual average concentration of ambient PM2.5 was above 75.00 μg/m3, and only 227.5 million people (17.17%) were living in areas where the annual concentration was under 35 μg/m3 (China national standard) in 2010 (Fig. S3). This finding documents the very high levels of PM2.5 exposures in China, especially in densely populated regions. The results also indicate that the PM2.5 related mortality rate is 61.0/105 in the cleanest areas (annual average PM2.5 concentrations lower than 35.00 μg/m3) and 120.7/105 in the most polluted areas (annual average PM2.5 concentrations higher than 75.00 μg/m3). This difference is mainly related to the different RRs which resulted from different exposure levels. According to our comparison (Fig. S8, S9), the RRs of all age groups for all end points in the most polluted areas are significantly higher than those in the cleanest areas. For baseline incidence however, there are no significant differences between the cleanest areas and the most polluted areas.
Fig. 5.
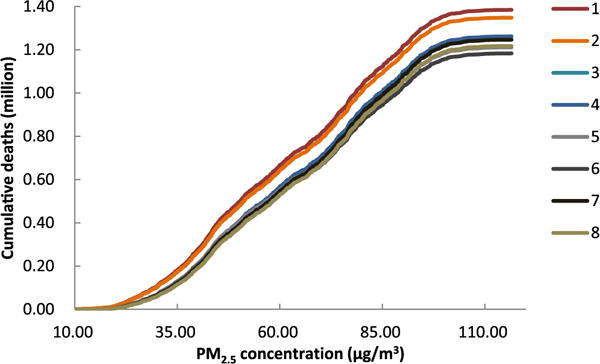
Cumulative numbers of PM2.5-related deaths (Note: Number 1–8 represents eight estimates based on eight sets of data sources, as listed in Table 1).
3.5. Provincial-level comparison
At the provincial level, the top four provinces with the highest PM2.5-related deaths were Shandong, Henan, Hebei, and Sichuan, and these regions also had high level of air pollution and population density. The provinces in northern China such as Liaoning, Hebei, Shandong and Henan province had the highest per-capita attributed mortality from PM2.5, and Tibet, Yunnan and Hainan had the lowest. Shanghai, Beijing, Tianjin and Shandong were the top four provinces/cities which had the highest per-unit-area mortality, and Tibet, Xinjiang, Qinghai and Inner Mongolia, were the lowest four (see Fig. 6).
Fig. 6.
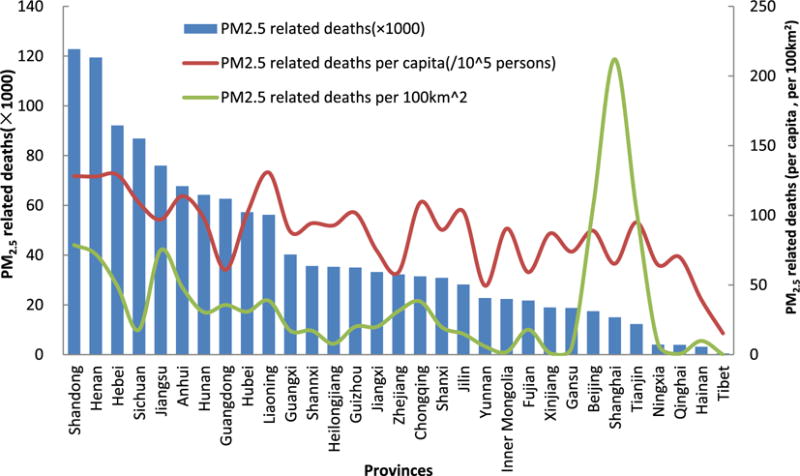
The regional patterns in premature mortality from PM2.5 in China (The main vertical axes indicate the number of PM2.5 related premature deaths, and the secondary vertical axes indicate the per-capita deaths and per-unit-area mortality attributed to PM2.5).
4. Discussion
We applied a range of state of the art exposure databases to generate new findings on spatial patterns of mortality related to PM2.5 in China. There are several important differences in our analysis compared to previous studies. First, this study was conducted using multi-model PM2.5 exposures and a spatial scale at the county-level that covers all of China. The multi-model PM2.5 data better expresses the uncertainties related to exposure estimates in assessing disease burden. Second, previous studies based their estimates on gridded all-age population and did not fully cover all of China for missing values. In contrast, we used higher and more relevant “age-specified, county-level population”, which captures more detailed demographic information. Third, all of our modeling processes were carried out at the county level, which is a significant advancement compared to the grid, city, or provincial levels. In addition, our study covered 99% of the 2860 counties in China, and our results not only confirmed and improved the results found in previous studies but also added additional spatial richness.
In comparison to surface station measurements, satellite-derived PM2.5 concentrations have advantages in terms of spatial coverage, particularly in the vast rural regions not covered by monitoring networks. Different kinds of models have been developed to estimate the exposure of PM2.5 concentration from satellite images. After comparing several sources of satellite-derived PM2.5 concentrations, we found that the general spatial patterns of these estimates among different models coincided with each other in the large spatial scale, but many differences were found in smaller scales (Fig. S1). Therefore, to better express the uncertainties introduced by alternative exposure methods, we applied multi-model concentration estimates to obtain more reliable exposure inputs.
Previous estimates of the long-term health effects of PM2.5 in China mainly used gridded, provincial, or city-level all-age population data, which are larger scale geographical units compared to counties. By using counties, we were better able to account for differences in demographic and social conditions that vary on fine spatial scales. For example, the aging phenomenon and the urbanization in China has led to great variation of the population age-structure between counties (National Bureau of Statistics of China, 2011; Chen and Hao, 2014). Health status, immunity, and mortality rates differ greatly among different counties and age groups. More detailed modeling using high resolution (county-level and age-specified) population data can better account for these factors in estimating PM2.5-related health effects.
Cardiovascular and cerebrovascular disease (IHD and stroke) accounted for the majority of the premature deaths related to PM2.5 pollution, and the elderly accounted for the majority of the premature deaths from these two endpoints. The incidence and mortality of these two diseases are higher than the other three diseases in China (National Health and Family Planning Commission of the PRC, 2015; Sui et al., 2016). Our study found the proportion of PM2.5-attributable mortality for IHD and stroke account for ~80% of the total number of all five causes combined. This is somewhat higher than the ~70% reported by the GBD study for the entire world. The comparison among age groups and different endpoints indicates that the elderly population groups and theses with cardiovascular and cerebrovascular disease are more vulnerable and sensitive to PM2.5 pollution, and should pay more attention to protect them from PM2.5 exposure.
The counties with high PM2.5-related-mortality are mainly located in the heavily polluted and densely populated regions like Beijing-Tianjin-Hebei region and the North China Plain. This highlights the urgency for China to control air pollution in these regions. Still, a considerable number of premature deaths were seen in other regions with lower average concentration of the air PM2.5. For example, some counties with relatively low PM2.5 concentration but high population density in Shanghai and Guangdong had large numbers of premature deaths (Fig. S7). Also, the Pearl River Delta region, where the PM2.5 concentration is relatively low, had a high ‘per-unit-area mortality’ resulting from the high population density. These information is important for making priority emission-reducing policies for different regions. For the highly-populated regions, policies and air quality standards may need to be stricter to avoid more PM2.5 related premature deaths.
In recent years, the Chinese government has taken measures to control the pollution. According to the 13th Five-Year Plan of National Environmental Protection of China (Zhao, 2014), by the year 2030, all counties in China will reach the national standard. The disease burden of PM2.5 will likely decline if the emission reduction targets are reached. Nevertheless, Combined with the acceleration of aging (National Bureau of Statistics of China, 2011; Wang and Chen, 2014), the disease burden from air pollution is likely to remain heavy in spite of the planned improvement of air quality. To reduce the health effects of PM2.5, China needs continuous efforts in pollution reduction. Measures and improvement should be step by step, under the guidance of scientific evidence.
Our study has the advantage in the spatial resolution and reliability for both PM2.5 exposure and population data. These new results add useful spatial dimensions to previous health burden estimates for China. However, it is important to keep in mind that this is an ecological study of the impact of PM2.5 on deaths at the county-level of China. It is known that analysis of health impacts of air pollution can be subject to large uncertainties (Kinney et al., 2010; Roman et al., 2008). First, we did not take all age groups into consideration. The ‘5–24’ age group was not considered in our model, which may lead to some underestimation of the health burden. However, people of this age group are young and relatively healthier than those of other age groups, and might have better resistance to air pollution related premature deaths. Secondly, baseline mortality data for each disease was available at the provincial level. Optimally, county-level estimates should use county-level base-line mortality data, but these data were not available. Therefore, we adopted provincial baseline mortality data, and an implicit assumption in our approach is that the underlying disease incidence is spatially invariant within each province. To support more accurate studies in the future, China should systematically collect and make available statistics for county-level disease-specific baseline mortality. Another uncertainty could come from the IER model applied in this study. To consider a wide range of exposures, Burnett et al. (2014) developed the IER model to estimate the PM2.5-related deaths. The RRs from secondhand smoking, active smoking, and household air pollution were integrated to form the IER model. A comparison done between the RRs observed in China and those evaluated by the IER model suggests that the IER model can yield sensible results in the risk analysis over the range of concentrations that prevail in China (Burnett et al., 2014). However, the 95% confidence interval (CI) of the RRs developed from the IERs was somewhat wide, and more information should be collected from epidemiologic studies in China to obtain better RRs. In addition, the adverse effect of PM2.5 exposure could be accumulated for longer time periods, so it is also necessary to estimate the long-term cumulative effects of PM2.5.
5. Conclusion
Following the methods of the GBD 2010 and the study of Apte et al. (2015), using four sources of satellite-derived PM2.5 concentration data and county-level age-specified population data across China in 2010, we estimated the PM2.5 related mortality for each county in China and observed significant spatial variations. This study provides a refined estimation of historical health effects attributable to outdoor PM2.5 in China at the county-level in 2010. To our knowledge, this is the first study to quantify the health consequences of China’s PM2.5 pollution at the county-level. Although some limitations exist, this work contributes valuable insights into the strong spatial variations of PM2.5 related health burdens in China. The findings of this study provide important implications for urban planners and policy makers regarding priority areas of national joint air pollution prevention and control in China. Moreover, open publication of our county-level health effects datasets also makes it possible to further explore the determinants of these health impacts.
Supplementary Material
Acknowledgments
This research was funded by grants from (1) National Natural Science Foundation of China (Grant: 21277135, 91543111), (2) Science Foundation for Young Scientists of National Institute of Environmental Health, Chinese Center for Disease Control and Prevention, (3) National High-level Talents Special Support Plan of China for Young Talents, (4) Environmental Health Development Project of National Institute of Environmental Health, Chinese Center for Disease Control and Prevention, and (5) the National Institutes of Health Institutional Research T32 Training Grant (ES023770).
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.envint.2017.10.015.
Footnotes
Author contribution
Q. W. and T. L. designed the study. Q. W. and J. W. cleaned the data and analyzed data. Q. W., M. H. and P. K. wrote the paper. All the authors contributed to interpret the results.
Conflict of interest
The authors declare there are no existed conflicts of interest.
References
- Apte JS, Marshall JD, Cohen AJ, et al. Addressing global mortality from ambient PM2.5. Environ Sci Technol. 2015;49(13):8057–8066. doi: 10.1021/acs.est.5b01236. [DOI] [PubMed] [Google Scholar]
- Boldo E, Medina S, Le Tertre A, et al. Apheis: health impact assessment of long-term exposure to PM2.5 in 23 European cities. Eur J Epidemiol. 2006;21(6):449–458. doi: 10.1007/s10654-006-9014-0. [DOI] [PubMed] [Google Scholar]
- Brauer M, Freedman G, Frostad J, et al. Ambient air pollution exposure estimation for the global burden of disease 2013. Environ Sci Technol. 2016;50(1):79–88. doi: 10.1021/acs.est.5b03709. [DOI] [PubMed] [Google Scholar]
- Burnett RT, Pope CA, Ezzati M, et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect. 2014;122:397–403. doi: 10.1289/ehp.1307049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen MH, Hao GC. Research on regional difference decomposition and influence factors of population aging in China. China Popul Resour Environ. 2014;24(4):136–141. [Google Scholar]
- Chen RJ, Kan HD, Chen B, et al. Association of particulate air pollution with daily mortality: the China air pollution and health effects study. Am J Epidemiol. 2012;175(11):1173–1181. doi: 10.1093/aje/kwr425. [DOI] [PubMed] [Google Scholar]
- Chow JC, et al. Health effects of fine particulate air pollution: lines that connect. J Air Waste Manage Assoc. 2006;56:1368–1380. doi: 10.1080/10473289.2006.10464545. [DOI] [PubMed] [Google Scholar]
- Cohen A, Anderson H, Brauer M, Burnett R. The Global Burden of Disease attributable to Outdoor Air Pollution: estimates from the GBD 2010 project. [C] ISEE Conference. 2012:S-135. [Google Scholar]
- Di Q, Kloog I, Koutrakis P, Lyapustin A, Wang Y, Schwartz J. Assessing PM2.5 exposures with high spatiotemporal resolution across the continental United States. Environ Sci Technol. 2016;50 doi: 10.1021/acs.est.5b06121. http://dx.doi.org/10.1021/acs.est.5b06121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dockery DW, et al. An association between air-pollution and mortality in 6 United-States cities. N Engl J Med. 1993;329:1753–1759. doi: 10.1056/NEJM199312093292401. [DOI] [PubMed] [Google Scholar]
- Evans J, van Donkelaar A, Martin RV, Burnett R, Rainham DG, Birkett NJ, et al. Estimates of global mortality attributable to particulate air pollution using satellite imagery. Environ Res. 2013;120:33–42. doi: 10.1016/j.envres.2012.08.005. [DOI] [PubMed] [Google Scholar]
- Fang D, Wang Q, Li H, et al. Mortality effects assessment of ambient PM2.5, pollution in the 74 leading cities of China. Sci Total Environ. 2016;569–570:1545–1552. doi: 10.1016/j.scitotenv.2016.06.248. [DOI] [PubMed] [Google Scholar]
- Guo YM, Barnett AG, Zhang YS, et al. The short-term effect of air pollution on cardiovascular mortality in Tianjin, China: comparison of time series and case–crossover analyses. Sci Total Environ. 2010;409(2):300–306. doi: 10.1016/j.scitotenv.2010.10.013. [DOI] [PubMed] [Google Scholar]
- Jerrett M, Turner MC, Beckerman BS, et al. Comparing the health effects of ambient particulate matter estimated using ground-based versus remote sensing exposure estimates. Environ Health Perspect. 2017;125:552–559. doi: 10.1289/EHP575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kinney PL, O’Neill MS, Bell ML, et al. Approaches for estimating effects of climate change on heat-related deaths: challenges and opportunities. Environ Sci Pol. 2008;11(1):87–96. [Google Scholar]
- Kinney PL, Roman HA, Walker KD, et al. On the use of expert judgment to characterize uncertainties in the health benefits of regulatory controls of particulate matter. Environ Sci Pol. 2010;13(5):434–443. [Google Scholar]
- Kloog I, Chudnovsky AA, Just AC, et al. A new hybrid spati-otemporal model for estimating daily multi-year PM2.5, concentrations across northeastern USA using high resolution aerosol optical depth data. Atmos Environ. 2014;95(1):581–590. doi: 10.1016/j.atmosenv.2014.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kunzli N, et al. Assessment of deaths attributable to air pollution: should we use risk estimates based on time series or on cohort studies? Am J Epidemiol. 2001;153:1050–1055. doi: 10.1093/aje/153.11.1050. [DOI] [PubMed] [Google Scholar]
- Laden F, et al. Association of fine particulate matter from different sources with daily mortality in six US cities. Environ Health Perspect. 2000;108:941–947. doi: 10.1289/ehp.00108941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lelieveld J, Evans JS, Fnais M, et al. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature. 2015;525(7569):367–371. doi: 10.1038/nature15371. [DOI] [PubMed] [Google Scholar]
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu J, Han Y, Xiao T, et al. Estimating adult mortality attributable to PM2.5, exposure in China with assimilated PM2.5, concentrations based on a ground monitoring network. Sci Total Environ. 2016a;568:1253–1262. doi: 10.1016/j.scitotenv.2016.05.165. [DOI] [PubMed] [Google Scholar]
- Liu M, Huang Y, Ma Z, et al. Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ Int. 2016b;98:75–81. doi: 10.1016/j.envint.2016.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu F, Xu D, Cheng Y, et al. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ Res. 2015;136:196–204. doi: 10.1016/j.envres.2014.06.029. [DOI] [PubMed] [Google Scholar]
- Ma ZW, Hu XF, Andrew MS, Robert L, Zhang Q, Xue YG, Tong SL, Bi J, Huang L, Liu Y. Satellite-based spatiotemporal trends in PM2.5 concentrations: China, 2004–2013. Environ Health Perspect. 2016;124(2):184–192. doi: 10.1289/ehp.1409481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naghavi M, Wang H, Lozano R, Davis A, Liang X, Zhou M, Vollset SE, et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385(9963):117–171. doi: 10.1016/S0140-6736(14)61682-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Bureau of Statistics of China. China Statistical Yearbook. China Statistical Publishing House; Beijing: 2011. [Google Scholar]
- National Health and Family Planning Commission of the PRC. 2014 Report on Chinese Resident’s Chronic Disease and Nutrition. 2015 Source: en.nhfpc.gov.cn.
- Pope CA, Dockery DW. Air pollution and life expectancy in China and beyond. Proc Natl Acad Sci U S A. 2013;110(32):12861–12862. doi: 10.1073/pnas.1310925110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pope CA, Burnett RT, Krewski D, Jerrett M, Shi Y, Calle EE, Thun MJ. Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke: shape of the exposure-response relationship. Circulation. 2009;120:941–948. doi: 10.1161/CIRCULATIONAHA.109.857888. [DOI] [PubMed] [Google Scholar]
- Pope CA, Burnett RT, Turner MC, Cohen A, Krewski D, Jerrett M, Gapstur SM, Thun MJ. Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: shape of the exposure-response relation-ships. Environ Health Perspect. 2011;119:1616–1621. doi: 10.1289/ehp.1103639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rohde RA, Muller RA. Air pollution in China: mapping of concentrations and sources. PLoS One. 2015;10(8):e0135749. doi: 10.1371/journal.pone.0135749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roman HA, Walker KD, Walsh TL, et al. Expert judgment assessment of the mortality impact of changes in ambient fine particulate matter in the US. Environ Sci Technol. 2008;42(7):2268–2274. doi: 10.1021/es0713882. [DOI] [PubMed] [Google Scholar]
- Schwartz J. Harvesting and long term exposure effects in the relation between air pollution and mortality. Am J Epidemiol. 2000;151:440–448. doi: 10.1093/oxfordjournals.aje.a010228. [DOI] [PubMed] [Google Scholar]
- Silva RA, West JJ, Lamarque JF, et al. Future global mortality from changes in air pollution attributable to climate change. Nat Clim Chang. 2017:1–6. doi: 10.1038/nclimate3354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sui H, Chen W, Wang W. Interpretation of report on cardiovascular diseases in China (2015) Chin J Cardiovasc Med. 2016;21(4):259–261. [Google Scholar]
- The State Council of the People’s Republic of China. The Twelfth Five-year Plan for the Control of Air Pollution for the Key Areas in China 2012 [Google Scholar]
- Van Donkelaar A, Martin RV, Brauer M, Hsu NC, Kahn RA, Levy RC, Lyapustin A, Sayer AM, Winker DM. Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ Sci Technol. 2016;50(7):3762–3772. doi: 10.1021/acs.est.5b05833. [DOI] [PubMed] [Google Scholar]
- Wang XQ, Chen PJ. Population ageing challenges health care in China. Lancet. 2014;383(9920):870. doi: 10.1016/S0140-6736(14)60443-8. [DOI] [PubMed] [Google Scholar]
- Xie R, Sabel CE, Lu X, et al. Long-term trend and spatial pattern of PM2.5 induced premature mortality in China. Environ Int. 2016;201697:180–186. doi: 10.1016/j.envint.2016.09.003. [DOI] [PubMed] [Google Scholar]
- Yang G, Wang Y, Zeng Y, Gao G, Liang X, Zhou M, Wan X, Yu S, Jiang Y, Naghavi M, Vos T, Wang H, Lopez A, Murray C. Rapid health transition in China, 1990–2010: findings from the global burden of disease study 2010. Lancet. 2013;381(9882):1987–2015. doi: 10.1016/S0140-6736(13)61097-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao HL. The thoughts and formation of the 13th five-year plan of National Environmental Protection of China. Environ Prot. 2014;42(22):28–32. [Google Scholar]
- Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the global burden of disease study 2013. Lancet. 2015;387(10015):251–272. doi: 10.1016/S0140-6736(15)00551-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.