

Abstract
Background
HIF1α, miR-210 and its downstream targets ISCU, COX-10, RAD52 and PTEN are all part of the placental hypoxia-responsive network. Tight regulation of this network is required to prevent development of maternal–fetal complications such as fetal growth restriction. HIF1α expression is increased in preeclamptic placentae, but little is known about its association with birth weight in normal pregnancies.
Methods
We measured placental levels of HIF1α, miR-20a, miR-210, ISCU, COX-10, RAD52 and PTEN in 206 mother–newborn pairs of the ENVIRONAGE birth cohort.
Results
Placental HIF1α gene expression was inversely associated with the ponderal index (PI): for a doubling in placental HIF1α expression, PI decreased by 6.7% (95% confidence interval [CI] 1.3 to 12.0%, p = 0.01). Placental RAD52 expression also displayed an inverse association with PI, a doubling in gene expression was associated with a 6.2% (CI 0.2 to 12.1% p = 0.04) decrease in PI. As for birth weight, we observed a significant association with placental miR-20a expression only in boys, where a doubling in miR-20a expression is associated with a 54.2 g (CI 0.6 to 108 g, p = 0.05) increase in birth weight.
Conclusions
The decrease in fetal growth associated with expression of hypoxia-network members HIF1a, RAD52 and miR-20a indicates that this network is important in potential intrauterine insults.
Keywords: Birth weight, Gene expression, HIF1α, Hypoxia, Placenta
Background
Fetal growth is dependent on genetic, placental and maternal factors. The fetus is thought to have an inherent growth potential that, under normal circumstances, results in a healthy newborn of appropriate size. The maternal–placental–fetal units act in harmony to provide the needs of the fetus while supporting the physiologic changes of the mother. The most common cause of low birth weight (LBW) at term in Western societies is placental insufficiency [1]. LBW infants have a 10–20-fold increased risk of dying in the perinatal period [2] and are at increased risk of developing chronic diseases including type 2 diabetes, hypertension and heart disease in later life [3]. Fetal growth restriction is the second leading cause of perinatal morbidity and mortality [4]. The ponderal index has been installed as an indicator of fetal growth particularly able to identify normal weight newborns (birth weight above 2500 g) with higher probability to develop disease such as hypoglycemia and hyperbilirubinemia (lower ponderal index) [5]. Placental development is dependent on tight regulation of oxygen tension [6]. Hypoxia-inducible factor 1α (HIF1α) plays an important role in control of placental oxygenation. Normal pregnancy is hallmarked by a state of oxidative stress, in which placental mitochondria generate reactive oxygen species [7]. Feto-placental hypoxia, hallmarked by increased levels of HIF1α, has been associated with development of preeclampsia [8]. A placental mRNA/miRNA network involving microRNA (miR)-210, iron sulfur-cluster assembly enzyme (ISCU) and HIF1α was proposed to regulate mitochondrial function during preeclampsia [9]. HIF1α is at the core of the hypoxia-responsive network able to target mRNAs and miRNAs executing diverse cellular functions [10]. HIF1α not only induces expression of miRNAs-20a and -210, these miRNAs in turn were shown to downregulate HIF1α [11, 12]. Preeclampsia is one of the most common pregnancy complications and it is believed that an inadequate blood flow in the placenta is responsible for this [13]. Preeclampsia could lead to fetal growth restriction. Fetal growth restriction is associated with increased fetal and perinatal morbidity and mortality, even in the absence of preeclampsia [14]. Little is known on the relation between HIF1α expression in placental tissue from normal term pregnancies and fetal growth. As tight regulation of oxygen levels is essential for proper fetal-placental development, we hypothesize placental expression levels of the hypoxia-responsive network are associated with measures of fetal growth in normal pregnancies. We analyzed expression of 7 members from the hypoxia-regulation network in placental tissue (Fig. 1), by examining miR-20a and miR-210 and mRNA HIF1α, cytochrome C oxidase-10 (COX-10), ISCU, phosphatase and tensin homolog (PTEN), and DNA repair protein RAD52 expression levels.
Fig. 1.
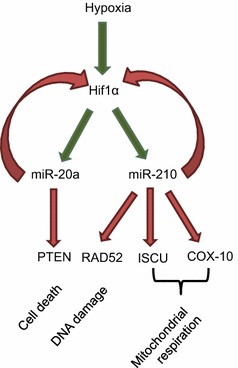
Hypoxia-responsive network in the placenta. miR-20a and miR-210 expression is upregulated via HIF1α. These miRNAs in turn regulate a broad spectrum of genes under hypoxia, including genes involved in mitochondrial biogenesis (ISCU), the respiratory chain (COX10), DNA double strand break repair (RAD52) and cell death (PTEN). miR-20a and miR-210 have both been shown to target HIF1α itself as well
Methods
Study design and population
From the ongoing population-based Birth Cohort Study ENVIRONAGE (ENVIRonmental influence ON AGEing), 206 mother–child pairs recruited between September 2011 and January 2014 at East Limburg Hospital (Genk, Belgium) were included in the current study. Inclusion criteria were singleton pregnancy and ability to fill out questionnaires in Dutch. The overall participation rate of eligible mothers was 61% [15] and we previously demonstrated the cohort represents birth in Flanders well [16].
Study approval was obtained from the ethics committees of East Limburg Hospital and Hasselt University and has been carried out according to the declaration of Helsinki. Written informed consent was obtained from the mothers prior to participation. Information on maternal age, smoking behavior (mother and co-residents), ethnicity, pre-pregnancy BMI and parity was obtained through questionnaires. Perinatal parameters such as newborn’s sex, birth date, birth weight and gestational age were collected from birth records. Ponderal index (PI) was calculated according to Rohrer’s formula, PI = (birth weight in grams/birth length in cm3) × 100.
Sample collection
Placentas were collected within 10 min after delivery and frozen at − 20 °C. Placentas were thawed minimally to obtain tissues biopsies for RNA extraction. To minimize the impact of within-placenta variability, biopsies were taken 1–1.5 cm below the chorio-amniotic membrane at 4 fixed locations across the placenta and stored overnight in RNA later and then preserved at − 20 °C until use.
RNA extraction
Total RNA and miRNA were extracted from pooled placenta biopsies using the miRNeasy mini kit (Qiagen, KJ Venlo, the Netherlands) according to the manufacturer’s instructions. Pooled placental samples from 4 biopsies were used to minimize intra-placental variation. Quality control of the extracted total RNA and miRNA was assessed by spectrophotometry (Nanodrop ND-1000; Isogen Life Science, De Meern, the Netherlands) and, for a random subset of the samples, 2100 Bionanalyzer (Applied Biosystems, Foster City, CA). The average (± SD) yield of total RNA per placenta was 4.3 (± 1.2) µg with average A260/280 and A260/230 ratio of 1.96 (± 0.02) 1.85 (± 0.18), respectively. DNase treatment was performed on extracted RNA samples according to the manufacturer’s instructions (Turbo DNA-free kit, Ambion, Life Technologies, Diegem, Belgium). Isolated RNA was stored at − 80 °C until further use. We previously reported [17] the variability within the four individual biopsies in a subset of ten placental tissues. Within the four biopsies of each placenta the Ct values for miRNA expression varied between 2 and 9% (CV). We therefore opted to use pooled samples from the 4 biopsies to minimize inter-placental differences.
Gene expression analysis
A maximum amount of 3 μg of total RNA was reverse transcribed into cDNA for gene expression analysis using the GoScript Reverse Transcription System (Promega, Madison, WI, USA) on a Veriti 96 well Thermal cycler (TC-5000, Techne, Burlington, NJ, USA). cDNA was stored at − 20 °C until use. A quantitative real-time polymerase chain reaction (qPCR) was set up by adding 2 μL of a 10 ng/μL dilution of cDNA together with TaqMan Fast Advanced Master Mix (Life Technologies, Foster City, CA, USA) and PrimeTimeTM assay (Integrated DNA Technologies, Coralville, IA, USA) for target mRNAs HIF1α, RAD52, COX-10, ISCU and PTEN in a final reaction volume of 10 μL. Standard cycling conditions were used to analyze samples in a 7900HT Fast Real-Time PCR system (Life Technologies, Foster City, CA, USA). Cq values were collected with SDS2.3 software. MIQE guidelines were taken into account [18]. Amplification efficiencies were between 90 and 110% for all assays. Raw data were processed to normalized relative gene expression values with qBase plus software (Biogazelle, Zwijnaarde, Belgium) using IPO8, POLR2A, UBC, GAPDH as reference genes for data normalization. Technical replicates were included when the difference in Cq value was < 0.5.
miRNA expression analysis
For analysis of miR-20a and miR-210 expression, RNA was reverse transcribed using the Megaplex reverse transcription (RT) stemloop primer pool A (Applied Biosystems, Foster City, CA) according to the manufacturer’s protocol. Briefly, 375 ng total RNA was reverse transcribed as follows: 2 min at 16 °C, 1 min at 42 °C and 1 min at 50 °C, for 40 cycles (Thermocycler PCR, Techne, Staffordshire, UK). Afterwards, cDNA was stored at − 20 °C for a maximum of 1 week until qRT-PCR measurements were performed. miRNA qRT-PCR analysis was performed using Taqman miRNA assays (Applied Biosystems, Foster City, CA), according to the manufacturer’s protocol. An input of 5 ng cDNA was used for PCR reactions, which were run on a 7900HT Fast Real-Time PCR System (Applied Biosystems, Foster City, CA), as follows: a polymerase activation for 2 min at 50 °C, a denaturation step for 10 min at 95 °C and an anneal/extension step (40 cycles) for 15 s at 95 °C and for 1 min at 60 °C. For normalization the endogenous control RNU6 was used. In order to minimize the technical variation between the different runs of the same miRNA assay, inter-run calibrators (IRCs) were used. Cq values were collected with SDS 2.3 software and the relative miRNA expression was calculated using the 2−ΔΔCq method (qBase plus; Biogazelle, Belgium). All samples were analyzed in triplicate. Replicates were included when the ΔCq was < 0.5.
Statistical analysis
SAS software (Version 9.3 SAS Institute, Cary, NC, USA) was used for statistical analysis. The relative quantities of mRNA expression were log-transformed because of their non-normal distribution. The collected data are presented as categorical data with frequencies (%) or numbers and as continuous data with mean (± SD). The association between relative placental mRNA/miRNA expression at birth and birth weight or ponderal index was assessed using a linear regression model. The model was corrected for the following covariates: newborn’s gender, ethnicity (European and non-European) and gestational age (weeks), maternal age (years), smoking status (never-smoker, past-smoker or current-smoker), educational status (low, middle or high) and parity (1, 2 or ≥ 3).
Results
General characteristics of the study population
Detailed maternal and newborn characteristics are shown in Table 1. Maternal age averaged (± SD) 29.3 ± 4.4 years. 69.9% of the population never smoked and 56.2% had a high educational level. The average maternal pre-gestational BMI was 24.3 ± 4.7 kg/m2. 53.7% of the newborns were female and 90.2% were of European decent. Gestational age averaged 39.2 weeks and ranged from 36 to 41 weeks. Mean ponderal index was 2.68 (± 0.29) g/cm3 and birth weight 3431 (± 447) g. Half (50.5%) of the newborns were their mothers’ first child and 2.9% were delivered by Caesarian-section (C-section).
Table 1.
Demographic characteristics of the study population (n = 206)
| Characteristics | Mean ± SD/Frequency (%) | |
|---|---|---|
| Boys (n = 96) | Girls (n = 110) | |
| Maternal | ||
| Age, years | 29.3 ± 4.4 | 29.5 ± 4.4 |
| Pre-gestational BMI, kg/m2 | 24.6 ± 4.6 | 24.2 ± 5.2 |
| Smoking status | ||
| Never-smoker | 64 (66.7) | 79 (72.2) |
| Past-smoker | 16 (16.7) | 18 (16.5) |
| Current-smoker | 16 (16.7) | 13 (11.3) |
| Parity | ||
| 1 | 47 (49.0) | 57 (51.8) |
| 2 | 37 (38.5) | 45 (40.9) |
| ≥ 3 | 12 (12.5) | 8 (7.3) |
| Education | ||
| Low | 13 (13.8) | 10 (9.2) |
| Middle | 37 (39.4) | 29 (26.6) |
| High | 44 (46.8) | 71 (64.2) |
| Newborn | ||
| Gestational age, weeks | 39.2 ± 1.4 | 39.3 ± 1.2 |
| Birth weight, g | 3483 ± 483 | 3385 ± 410 |
| Ponderal index, kg/m3 × 100 | 2.63 ± 0.24 | 2.72 ± 0.24 |
| Ethnicity | ||
| European-Caucasian | 85 (88.5) | 101 (91.74) |
| Non-European | 11 (11.5) | 9 (8.26) |
| C-section | 3 (3.1) | 3 (2.6) |
Placental expression of hypoxia-related factors in association with birth weight and ponderal index
Expression of the placental hypoxia network was negatively associated with the ponderal index. Placental HIF1α gene expression was inversely associated with PI: for a doubling in placental HIF1α expression, PI decreased by 6.7% (95% confidence interval [CI] 1.3 to 12.0%, p = 0.01) when analyzing both sexes together, with similar estimates in boys and girls. Placental RAD52 expression also displayed an inverse association with PI for boys and girls, a doubling in gene expression was associated with a 6.2% (CI 0.2 to 12.1% p = 0.04) decrease in PI. No significant associations with the other analyzed hypoxia-network genes and ponderal index could be observed, although there was a trend for a negative association between PI and miR-20a expression in girls and boys, where a doubling in gene expression was associated with a 2.08% (CI − 0.2 to 4.4%, p = 0.08) decrease in PI (Table 2, Fig. 2).
Table 2.
Changes in relative placental mRNA and miRNA expression associated with ponderal index and birth weight, for a doubling in gene expression
| Gene | Ponderal index | Birth weight | ||
|---|---|---|---|---|
| % change (95% CI) | p-value | % change (95% CI) | p-value | |
| Girls and boys (n = 206) | ||||
| HIF1α | − 6.68 (− 12.01, − 1.34) | 0.01 | − 10.79 (− 83.67, 62.09) | 0.77 |
| COX-10 | 0.26 (− 9.96, 10.49) | 0.96 | 45.70 (− 94.56, 185.97) | 0.52 |
| ISCU | − 1.20 (− 8.18, 5.78) | 0.73 | 7.58 (− 86.83, 101.99) | 0.87 |
| RAD52 | − 6.16 (− 12.10, − 0.22) | 0.04 | − 47.73 (− 127.70, 32.24) | 0.24 |
| PTEN | − 4.57 (− 10.27, 1.13) | 0.12 | − 11.20 (− 88.94, 32.24) | 0.78 |
| miR-210 | − 1.18 (− 3.36, 0.99) | 0.28 | − 5.42 (− 34.84, 24.00) | 0.72 |
| miR-20a | − 2.08 (− 4.37, 0.22) | 0.08 | 3.52 (− 27.55, 34.59) | 0.82 |
| Boys (n = 96) | ||||
| HIF1α | − 7.67 (− 16.18, 0.83) | 0.08 | − 96.16 (− 210.5, 18.17) | 0.10 |
| COX-10 | 3.03 (− 19.66, 13.59) | 0.72 | − 16.74 (− 250.22, 216.74) | 0.89 |
| ISCU | 7.81 (− 18.33, 3.21) | 0.16 | − 30.88 (− 188.06, 126.31) | 0.70 |
| RAD52 | − 5.14 (− 13.98, 3.70) | 0.25 | 76.71 (− 201.02, 47.59) | 0.22 |
| PTEN | − 1.77 (− 12.33, 8.80) | 0.74 | 3.01 (− 146.07, 152.09) | 0.97 |
| miR-210 | − 0.93 (− 4.38, 2.51) | 0.59 | − 4.56 (− 51.57, 42.45) | 0.85 |
| miR-20a | − 0.25 (− 4.43, 3.93) | 0.91 | 54.19 (0.57, 107.82) | 0.05 |
| Girls (n = 110) | ||||
| HIF1α | − 7.56 (− 14.97, − 0.14) | 0.05 | 7.15 (− 88.27, 102.58) | 0.88 |
| COX-10 | 5.54 (− 8.46, 19.55) | 0.43 | 160.21 (− 20.17, 340.59) | 0.08 |
| ISCU | 2.73 (− 6.81, 12.27) | 0.57 | 33.04 (− 87.12, 153.19) | 0.59 |
| RAD52 | − 5.19 (− 13.91, 3.53) | 0.24 | − 72.35 (− 181.64, 36.94) | 0.19 |
| PTEN | 5.22 (− 12.56, 2.11) | 0.16 | − 15.45 (− 110.14, 79.25) | 0.75 |
| miR-210 | − 0.86 (− 3.90, 2.18) | 0.58 | 11.27 (− 28.00, 50.54) | 0.57 |
| miR-20a | − 2.06 (− 5.02, 0.91) | 0.17 | − 15.46 (− 53.97, 23.04) | 0.43 |
Fig. 2.

Association between ponderal index, birthweight and hypoxia-responsive network expression in placental tissue. Models were adjusted for newborns’ ethnicity, gestational age, maternal age, smoking and educational status of the mother, maternal pre-pregnancy BMI, and parity. Analysis in girls and boys combined was furthermore adjusted for newborns’ gender. Estimates are presented as an absolute change in PI (a) or birthweight (b) for a doubling in gene or miRNA expression
Estimated changes are shown with their 95% confidence intervals and p-values. Estimates were adjusted for newborns’ ethnicity, gestational age, maternal age, smoking and educational status of the mother, maternal pre-pregnancy BMI, and parity. Analysis in girls and boys combined was furthermore adjusted for newborns’ gender.
As for birth weight, we observed a significant association with placental miR-20a expression only in boys, where a doubling in miR-20a expression is associated with a 54.2 g higher birth weight (CI 0.6 to 108 g, p = 0.05). Finally, a trend towards a negative association between COX-10 expression in girls and birth weight was observed, where a doubling in gene expression is associated with a 160 g increase (CI − 20.2 to 340.6, p = 0.08) in birth weight (Table 2). All analyses were corrected for newborns’ ethnicity, gestational age, maternal age, smoking and educational status of the mother, maternal pre-pregnancy BMI, and parity.
We tested the interaction terms of newborns parity and expression of hypoxia-network genes and microRNAs expression on birthweight and the ponderal index. Only the interaction term for RAD52 expression*parity was significant for birthweight (p = 0.036). When analyzing the association between gene/miRNA expression and birthweight subdivided by parity, we did not found any significant associations.
Discussion
We here report on the expression of the placental hypoxia-responsive network involving HIF1α and several of its target genes/miRNAs and its association with fetal growth parameters. The relationship between low birth weight or low ponderal index and chronic disease has been established in several publications [5, 19, 20]. As such, an inverse relationship between birth weight and blood pressure in childhood was already observed in the 1980s by David Barker [21], which can lead to development of cardiovascular disease (reviewed in [22]).
Regulation of oxygen tension is tightly controlled throughout gestation, and follows a distinct pattern. During the first trimester, the placenta develops under low oxygen tension, a physiologic form of hypoxia, oxygen tension, as well as HIF1α expression, increase towards the end of the first trimester (week 11 of gestation) [23, 24]. From this point onwards, the placenta is well-oxygenated throughout the remainder of gestation and a physiologic state of normoxia exists. If placental oxygen tension drops towards the end of pregnancy, a hypoxic or ischemic condition arises that can be detrimental for both mother and fetus. HIF1α expression achieves two peaks during the first trimester, one around week 7–10 of gestation, another one around week 14–18. Levels drop much lower around the time of birth [24]. PTEN expression on the other hand was reported higher during the first trimester pregnancy as compared to any time in the normal menstrual cycle [25]. PTEN expression of villous trophoblasts was decreasing as the pregnancy advanced. PTEN expression decreased parallel to the development of placenta. Expression of PTEN in decidual cells was significantly stronger in placental tissues of spontaneous abortion than placental tissues from normal pregnancies at the first and third trimester [26]). miR-210 expression remains at fairly constant levels throughout healthy pregnancies, whereas its expression is increased in pregnancies complicated by preeclampsia between 26 and 38 weeks of gestation, this association disappears after 38 weeks of gestation [27].
We observed significant negative associations between placental HIF1α, RAD52 and the ponderal index in newborn girls and boys. Moreover, we found a significant positive association between placental expression of miR-20a and birth weight in newborn boys only. Our findings support the importance of expression of these genes in the placenta for normal fetal growth. Decreased expression of HIF1α has previously been reported in placental tissue from pregnancies complicated by preeclampsia compared to normal pregnancies [8, 28]. Preeclampsia is hallmarked by hypertension and proteinuria and is associated with significant maternal morbidity and mortality [29]. Preeclampsia is characterized by placental hypoxia and/or ischemia, excessive oxidative stress, in association with endothelial dysfunction [30]. Whether HIF1α expression is associated with intrauterine growth restriction (IUGR) is not clear. Some studies report no detected differences in placental HIF1α expression between IUGR babies versus babies born from normal singleton pregnancies [31], whereas others have reported increased expression of HIF1α in maternal plasma [32]. Zhang et al. reported higher HIF1α expression in placental shares from twins with IUGR compared to normal twins, although no significant correlation with birth weight could be established [33]. These apparent differences could stem from differences in tissue type, study population and study size.
The incidence of childhood cancer is estimated to increase but the causes remain uncertain [34, 35]. Insults to the genome in the perinatal period are likely to contribute to carcinogenesis and may be more important relative to other life stages because of the higher probability that mutated and genomically unstable cells could populate the rapidly growing tissues of an infant [36]. Mutations of the genome may have particularly adverse consequences in early life, including developmental defects and immune system dysfunction [36, 37]. Gene expression related to DNA damage and immune response among children is observed to correlate with micronuclei frequency (MN) as a consequence of exposure to environmental pollutants [38, 39]. As for RAD52, this is the first time that expression of this DNA damage marker was reported to be associated with measures of fetal growth. RAD52 is a key player in DNA doublestrand break repair and homologous recombination. It forms a heptameric ring, catalyses DNA annealing and mediates Rad51-catalysed strand invasion [40]. The process of DNA repair has previously been linked with changes in birth weight, as a genome-wide methylation study in the Norwegian mother and child cohort identified increased levels of X-ray repair cross complementing 3 (XRCC3) methylation to be associated with increased birth weight [41]. They noted an inverse association between DNA damage gene expression (through increased methylation) and birth weight consistent with our findings. Furthermore, a positive association between DNA damage markers and birthweight was recently reported in the Australian DADHI cohort, where genome damage was measured by scoring MN as a biomarker of both chromosome breakage and/or loss; nucleoplasmic bridges as a biomarker of DNA mis-repair and/or telomere end fusions and nuclear buds were measured as biomarker of gene amplification and/or the removal of unresolved DNA repair complexes. Infant birth weight was associated positively with all the aforementioned chromosomal lesions in cord blood from term newborns [42].
To our knowledge, this is the first report investigating the association between expression of the hypoxia-regulation network including HIF1α and several of its downstream targets and newborn growth characteristics in term babies from normal pregnancies. We herewith provide evidence that tight regulation of oxygen tension/hypoxia is important also in healthy pregnancies and show that lower expression is associated with lower birth weight and ponderal index. The public health significance of this finding is important as it provides molecular evidence for the explanation of epidemiological studies that low-birth-weight babies have an increased risk for the development of cardiovascular disease in later life.
We did not identify any associations between placental miR-210 expression and fetal growth characteristics, although miR-210 is a target of HIF1α [43] and has been shown to be increased in placental tissue from preeclamptic women [9]. As miR-210 itself is known to target HIF1α and thereby functions in a negative feedback loop, and other mRNAs such as Akt and p53 can also regulate miR-210 expression [44, 45], this could explain why we did not observe an association with fetal growth in our current analyses.
As such, our study involves a large sample size and expression profiling was performed in placental tissue, the main regulator of fetal development. The current findings must be interpreted within the context of its limitations. At this time we cannot make any predictions on the role of the hypoxia-regulating network in postnatal child growth and adult disease risk. As we only collect placentae at birth, we cannot make any conclusions on dynamics of expression throughout pregnancy.
Conclusions
We observed significant associations between hypoxia-network members HIF1, RAD52 and miR-20a expression and ponderal index as well as birth weight as measures of fetal growth in term newborns. The inverse relationship between fetal growth and expression of hypoxia-network members HIF1, RAD52 and miR-20a indicates that this network is important in potential intrauterine insults.
Authors’ contributions
TN coordinates the ENVIRONAGE birth cohort and managed funding. NM organized the field work with help of WG. KV did the statistical analysis, the quality control of the database and drafted the manuscript. MT performed the m(i)RNA measurements under supervision of KV. All authors have helped with data interpretation. All authors read and approved the final manuscript.
Acknowledgements
Not applicable.
Competing interests
The authors declare they have no competing interests.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the research committee from Hasselt University and Hospital East-Limburg and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from the mothers prior to participation.
Funding
The ENVIRONAGE birth cohort is supported by grants from the European Research Council (ERC-2012-StG 310898) and Flemish Research Council (FWO G073315N). Karen Vrijens is a postdoctoral fellow of the FWO (12D7714N).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- AKT
serine-threonine protein kinase
- BMI
body mass index
- C-section
Caesarian-section
- COX-10
cytochrome C oxidase-10
- GAPDH
glyceraldehyde-3-phosphate dehydrogenase
- HIF1α
hypoxia-inducible factor 1α
- IPO8
importin 8
- IRC
inter run calibrator
- ISCU
iron sulfur-cluster assembly enzyme
- IUGR
intrauterine growth restriction
- LBW
low birth weight
- miR
microRNA
- MIQE
minimum information for publication of quantitative real-time PCR experimens
- MN
micronuclei
- PI
ponderal index
- POLR2A
RNA polymerase II subunit A
- PTEN
phosphatase and tensin homolog
- RNU6
RNA, U6 small nuclear
- TP53
tumor protein 53
- UBC
ubiquitin C
- XRCC3
X-ray repair cross complementing 3
Contributor Information
Karen Vrijens, Phone: 32-11-268327, Email: Karen.vrijens@uhasselt.be.
Maria Tsamou, Email: maria.tsamou@uhasselt.be.
Narjes Madhloum, Email: narjes.madhloum@uhasselt.be.
Wilfried Gyselaers, Email: wilfried.gyselaers@zol.be.
Tim S. Nawrot, Email: tim.nawrot@uhasselt.be
References
- 1.Henriksen T, Clausen T. The fetal origins hypothesis: placental insufficiency and inheritance versus maternal malnutrition in well-nourished populations. Acta Obstet Gynecol Scand. 2002;81(2):112–114. doi: 10.1034/j.1600-0412.2002.810204.x. [DOI] [PubMed] [Google Scholar]
- 2.Monk D, Moore GE. Intrauterine growth restriction–genetic causes and consequences. Semin Fetal Neonatal Med. 2004;9(5):371–378. doi: 10.1016/j.siny.2004.03.002. [DOI] [PubMed] [Google Scholar]
- 3.Barker DJ. Developmental origins of adult health and disease. J Epidemiol Commun Health. 2004;58(2):114–115. doi: 10.1136/jech.58.2.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Peleg D, Kennedy CM, Hunter SK. Intrauterine growth restriction: identification and management. Am Fam Physician. 1998;58(2):453–460. [PubMed] [Google Scholar]
- 5.Nili FMM, Mobine J. The value of ponderal index as a prognostic factor in predicting complications in term neonates. Med J Islam Repub Iran. 2003;17(3):197–201. [Google Scholar]
- 6.Adelman DM, Gertsenstein M, Nagy A, et al. Placental cell fates are regulated in vivo by HIF-mediated hypoxia responses. Genes Dev. 2000;14(24):3191–3203. doi: 10.1101/gad.853700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang Y, Walsh SW. Increased superoxide generation is associated with decreased superoxide dismutase activity and mRNA expression in placental trophoblast cells in pre-eclampsia. Placenta. 2001;22(2–3):206–212. doi: 10.1053/plac.2000.0608. [DOI] [PubMed] [Google Scholar]
- 8.Rajakumar A, Brandon HM, Daftary A, et al. Evidence for the functional activity of hypoxia-inducible transcription factors overexpressed in preeclamptic placentae. Placenta. 2004;25(10):763–769. doi: 10.1016/j.placenta.2004.02.011. [DOI] [PubMed] [Google Scholar]
- 9.Muralimanoharan S, Maloyan A, Mele J, et al. MIR-210 modulates mitochondrial respiration in placenta with preeclampsia. Placenta. 2012;33(10):816–823. doi: 10.1016/j.placenta.2012.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Huang X, Le QT, Giaccia AJ. MiR-210–micromanager of the hypoxia pathway. Trends Mol Med. 2010;16(5):230–237. doi: 10.1016/j.molmed.2010.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yang W, Wei J, Sun T, et al. Effects of knockdown of miR-210 in combination with ionizing radiation on human hepatoma xenograft in nude mice. Radiat Oncol. 2013;8:102. doi: 10.1186/1748-717X-8-102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Taguchi A, Yanagisawa K, Tanaka M, et al. Identification of hypoxia-inducible factor-1 alpha as a novel target for miR-17-92 microRNA cluster. Cancer Res. 2008;68(14):5540–5545. doi: 10.1158/0008-5472.CAN-07-6460. [DOI] [PubMed] [Google Scholar]
- 13.Maynard SE, Min JY, Merchan J, et al. Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J Clin Invest. 2003;111(5):649–658. doi: 10.1172/JCI17189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McIntire DD, Bloom SL, Casey BM, et al. Birth weight in relation to morbidity and mortality among newborn infants. N Engl J Med. 1999;340(16):1234–1238. doi: 10.1056/NEJM199904223401603. [DOI] [PubMed] [Google Scholar]
- 15.Janssen BG, Madhloum N, Gyselaers W, Bijnens E, Clemente DB, Cox B, Hogervorst J, Luyten L, Martens D, Peusens M, Plusquin M, Provost E, Roels HA, Saenen ND, Tsamou M, Vriens A, Winckelmans E, Vrijens K, Nawrot TS. Cohort Profile: The ENVIRonmental influence ON early AGEing (ENVIRONAGE): a Birth Cohort Study. Int J Epidemiol. 2017;46(5):1386–1387m. doi: 10.1093/ije/dyx033. [DOI] [PubMed] [Google Scholar]
- 16.Cox B, Martens E, Nemery B, et al. Impact of a stepwise introduction of smoke-free legislation on the rate of preterm births: analysis of routinely collected birth data. BMJ. 2013;346:f441. doi: 10.1136/bmj.f441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tsamou M, Vrijens K, Madhloum N, Lefebvre W, Vanpoucke C, Nawrot TS. Air pollution-induced placental epigenetic alterations in early life: a candidate miRNA approach. Epigenetics. 2016 doi: 10.1080/15592294.2016.1155012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bustin SA, Benes V, Garson JA, et al. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin Chem. 2009;55(4):611–622. doi: 10.1373/clinchem.2008.112797. [DOI] [PubMed] [Google Scholar]
- 19.Gillman MW. Developmental origins of health and disease. N Engl J Med. 2005;353(17):1848–1850. doi: 10.1056/NEJMe058187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Barker DJ, Osmond C, Simmonds SJ, et al. The relation of small head circumference and thinness at birth to death from cardiovascular disease in adult life. BMJ. 1993;306(6875):422–426. doi: 10.1136/bmj.306.6875.422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Barker DJ, Osmond C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet. 1986;1(8489):1077–1081. doi: 10.1016/S0140-6736(86)91340-1. [DOI] [PubMed] [Google Scholar]
- 22.Dasinger JH, Alexander BT. Gender differences in developmental programming of cardiovascular diseases. Clin Sci (Lond). 2016;130(5):337–348. doi: 10.1042/CS20150611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pringle KG, Kind KL, Sferruzzi-Perri AN, Thompson JG, Roberts CT. Beyond oxygen: complex regulation and activity of hypoxia inducible factors in pregnancy. Hum Reprod Update. 2010;16(4):415–431. doi: 10.1093/humupd/dmp046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ietta F, et al. Dynamic HIF1A regulation during human placental development. Biol Reprod. 2006;75(1):112–121. doi: 10.1095/biolreprod.106.051557. [DOI] [PubMed] [Google Scholar]
- 25.Guzeloglu-Kayisli O, et al. Regulation of PTEN (phosphatase and tensin homolog deleted on chromosome 10) expression by estradiol and progesterone in human endometrium. J Clin Endocrinol Metab. 2003;88(10):5017–5026. doi: 10.1210/jc.2003-030414. [DOI] [PubMed] [Google Scholar]
- 26.Tokyol C, Aktepe F, Husniye Dilek F, Yilmazer M. Comparison of placental PTEN and beta1 integrin expression in early spontaneous abortion, early and late normal pregnancy. Upsala J Med Sci. 2008;113(2):235–242. doi: 10.3109/2000-1967-231. [DOI] [PubMed] [Google Scholar]
- 27.Lee DC, et al. miR-210 targets iron-sulfur cluster scaffold homologue in human trophoblast cell lines: siderosis of interstitial trophoblasts as a novel pathology of preterm preeclampsia and small-for-gestational-age pregnancies. Am J Pathol. 2011;179(2):590–602. doi: 10.1016/j.ajpath.2011.04.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rajakumar A, Whitelock KA, Weissfeld LA, et al. Selective overexpression of the hypoxia-inducible transcription factor, HIF-2alpha, in placentas from women with preeclampsia. Biol Reprod. 2001;64(2):499–506. doi: 10.1093/biolreprod/64.2.499. [DOI] [PubMed] [Google Scholar]
- 29.Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33(3):130–137. doi: 10.1053/j.semperi.2009.02.010. [DOI] [PubMed] [Google Scholar]
- 30.Powe CE, Levine RJ, Karumanchi SA. Preeclampsia, a disease of the maternal endothelium: the role of antiangiogenic factors and implications for later cardiovascular disease. Circulation. 2011;123(24):2856–2869. doi: 10.1161/CIRCULATIONAHA.109.853127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rajakumar A, Jeyabalan A, Markovic N, et al. Placental HIF-1 alpha, HIF-2 alpha, membrane and soluble VEGF receptor-1 proteins are not increased in normotensive pregnancies complicated by late-onset intrauterine growth restriction. Am J Physiol Regul Integr Comp Physiol. 2007;293(2):R766–R774. doi: 10.1152/ajpregu.00097.2007. [DOI] [PubMed] [Google Scholar]
- 32.Ashur-Fabian O, Yerushalmi GM, Mazaki-Tovi S, et al. Cell free expression of hif1alpha and p21 in maternal peripheral blood as a marker for preeclampsia and fetal growth restriction. PLoS ONE. 2012;7(5):e37273. doi: 10.1371/journal.pone.0037273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Zhang GL, He ZM, Shi XM, et al. Discordant HIF1A mRNA levels and oxidative stress in placental shares of monochorionic twins with selective intra-uterine growth restriction. Placenta. 2015;36(3):297–303. doi: 10.1016/j.placenta.2014.12.019. [DOI] [PubMed] [Google Scholar]
- 34.Barrington-Trimis JL, Cockburn M, Metayer C, et al. Trends in childhood leukemia incidence over two decades from 1992 to 2013. Int J Cancer. 2017;140(5):1000–1008. doi: 10.1002/ijc.30487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Georgakis MK, Karalexi MA, Kalogirou EI, et al. Incidence, time trends and survival patterns of childhood pilocytic astrocytomas in Southern-Eastern Europe and SEER, US. J Neurooncol. 2017;131(1):163–175. doi: 10.1007/s11060-016-2284-9. [DOI] [PubMed] [Google Scholar]
- 36.Fenech MF. Nutriomes and personalised nutrition for DNA damage prevention, telomere integrity maintenance and cancer growth control. Cancer Treat Res. 2014;159:427–441. doi: 10.1007/978-3-642-38007-5_24. [DOI] [PubMed] [Google Scholar]
- 37.Pedersen M, Wichmann J, Autrup H, et al. Increased micronuclei and bulky DNA adducts in cord blood after maternal exposures to traffic-related air pollution. Environ Res. 2009;109(8):1012–1020. doi: 10.1016/j.envres.2009.08.011. [DOI] [PubMed] [Google Scholar]
- 38.Rossnerova A, Spatova M, Rossner P, Jr, et al. Factors affecting the frequency of micronuclei in asthmatic and healthy children from Ostrava. Mutat Res. 2011;708(1–2):44–49. doi: 10.1016/j.mrfmmm.2011.01.004. [DOI] [PubMed] [Google Scholar]
- 39.van Leeuwen DM, Gottschalk RW, Schoeters G, et al. Transcriptome analysis in peripheral blood of humans exposed to environmental carcinogens: a promising new biomarker in environmental health studies. Environ Health Perspect. 2008;116(11):1519–1525. doi: 10.1289/ehp.11401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mortensen UH, Lisby M, Rothstein R. Rad52. Curr Biol. 2009;19(16):R676–R677. doi: 10.1016/j.cub.2009.06.001. [DOI] [PubMed] [Google Scholar]
- 41.Engel SM, Joubert BR, Wu MC, et al. Neonatal genome-wide methylation patterns in relation to birth weight in the Norwegian Mother and Child Cohort. Am J Epidemiol. 2014;179(7):834–842. doi: 10.1093/aje/kwt433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Singh MT, Hor P, Almond M, Owens T, Hague J, Fenech M. Infant birth outcomes are associated with DNA damage biomarkers as measured by the cytokinesis block micronucleus cytome assay: the DADHI study. Mutagenesis. 2017;32:355–370. doi: 10.1093/mutage/gex001. [DOI] [PubMed] [Google Scholar]
- 43.Camps C, Buffa FM, Colella S, et al. hsa-miR-210 is induced by hypoxia and is an independent prognostic factor in breast cancer. Clin Cancer Res. 2008;14(5):1340–1348. doi: 10.1158/1078-0432.CCR-07-1755. [DOI] [PubMed] [Google Scholar]
- 44.Takikawa T, Masamune A, Hamada S, et al. miR-210 regulates the interaction between pancreatic cancer cells and stellate cells. Biochem Biophys Res Commun. 2013;437(3):433–439. doi: 10.1016/j.bbrc.2013.06.097. [DOI] [PubMed] [Google Scholar]
- 45.Mutharasan RK, Nagpal V, Ichikawa Y, et al. microRNA-210 is upregulated in hypoxic cardiomyocytes through Akt- and p53-dependent pathways and exerts cytoprotective effects. Am J Physiol Heart Circ Physiol. 2011;301(4):H1519–H1530. doi: 10.1152/ajpheart.01080.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.