

Abstract
Aim
To assess prevalence of stress and its sources among undergraduate health professional students at Makerere University.
Design
This was a descriptive cross‐sectional study using quantitative methods of data collection.
Methods
The study was conducted among 258 undergraduate health professional students (Medical, Dental and, Nursing students) at Makerere University. From each programme, students were recruited proportionately, while being selected conveniently from each year of study. Stress was measured using the General Health Questionnaire 12 and stressors assessed using a questionnaire developed from literature. After obtaining ethics approval, data were collected from consenting students. Data collected were analysed using SPSS statistical program.
Results
The prevalence of stress was found to be 57.4% and stressors of academic and psychosocial origin were most frequently reported. The top stressors included; academic curriculum (38%), dissatisfaction with class lectures (30.9%), long distance walk (29.5%), lack of time for recreation (28.9%), performance in examination (28.3%), lack of special guidance from faculty (26.7%) and high parental expectations (26.7%).
Keywords: health professions, nurses, nursing, stress, students, Uganda
1. INTRODUCTION
Health professionals’ training has been reported to be stressful (Paudel, Subedi, & Shrestha, 2013; Sreeramareddy et al., 2007). Stress is a highly unpleasant state of emotional arousal that humans experience in situations perceived as troublesome or challenging (Khodarahimi, Hashim, & Mohd‐Zaharim, 2012). It is experienced only when one perceives that the demands are greater than the individual and social resources that the person is able to mobilize (Lazarus, 1966). It is reported that health professional students undergo circumstances during their training that expose them to stress (Sreeramareddy et al., 2007). Romano (1992) noted that that personal or environmental events that cause stress are known as stressors and it is an individual's reaction to these that eventually cause stress (Romano, 1992).
Researchers have documented the prevalence of stress to be high among higher education students (Habeeb, 2010) and this is even worse among health professional students (Aktekin et al., 2001). A systematic review of literature on stress among health professional students revealed high prevalence of stress ranging from 14.3% to 56% (Salam, Yousuf, Bakar, & Haque, 2013). While these findings show high prevalence of stress, studies done particularly among health professional students in African universities have documented worrying levels of stress ranging from 21.6% to 86% (Amr, El‐Gilany, El‐Moafee, Salama, & Jimenez, 2011; Dessie, Ebrahim, & Awoke, 2014; Ofili, Oriaifo, Okungbowa, & Eze, 2009). In Uganda, data about stress among health professional students are scarce; however, a study done to explore academic stress among students of Mbarara University revealed that students had moderate levels of stress and it affected their academic performance negatively (Nakalema & Ssenyonga, 2014).
2. BACKGROUND
Although the problem of stress has widely been acknowledged in health professional training, little attention has been given to it especially by training institutions in developing countries. Consequently, students silently endure the effects of stress on their physical and mental well‐being. It is reported that 27% of health professional students develop psychological morbidities during training of which only 14% seek mental health care (Haoka et al., 2010). Various stress‐related illnesses, including anxiety, depression (Dahlin, Joneborg, & Runeson, 2005), somatoform disorders (Bramness, Fixdal, & Vaglum, 1991) and suicidal ideations (Dyrbye et al., 2008), have been documented among health professional students. Although this can be traced from various sources, stress plays a precipitating role. Appropriate strategies to reduce stress can only be devised if its sources are identified. Previous studies have documented the sources of stress to include academic, psychosocial and health‐related problems (Sreeramareddy et al., 2007). Frequently reported stressors include lack of support, leaving away from homes, financial difficulties and lack of home atmosphere (Al‐Dubai, Al‐Naggar, AlShagga, & Rampal, 2011; Polychronopoulou & Divaris, 2009). Additionally, large quantity of content to be learned, insufficient skill in medical practice, falling behind the reading schedule, heavy workload, performance pressure and the feeling of failing a course (Yusoff, Rahim, & Yaacob, 2010) have also been reported.
With the goal of grooming future health professionals that are resilient, stress during training has to be identified and addressed. Motivated by the above facts, we conducted a study with a focus on documenting the prevalence of stress and its sources among health professional students at Makerere University. The study was to answer the following research questions:
What is the prevalence of stress among health professional students at Makerere University College of health sciences?
What stresses health professional students at Makerere University College of health sciences?
3. THE STUDY
3.1. Design
This was a descriptive cross‐sectional survey conducted among undergraduate health professional students at Makerere University College of Health Sciences from first year to fifth year. Health professional students in this study refers to students pursuing a bachelor's degree in nursing, dental surgery, and medicine and surgery.
3.2. Method
3.2.1. Sampling procedure
Proportionate sampling was used to select 320 students from the three programmes to participate in the study. Following stratified sampling, students were grouped according to year of study, from where students were recruited by convenience sampling. Data collection period was 10 days and every day at least 25 students were being recruited. Undergraduate medical, dental and nursing students found in the library, halls of residence and lecture rooms were identified. Written informed consent was obtained before data collection.
3.2.2. Data collection procedure
A preliminary questionnaire was made and pilot‐tested among 10 students at the College of Health Sciences at Makerere University and necessary adjustments were made and the final questionnaire was used to collect data. A total of 320 questionnaires were distributed to consenting students and only 258 were returned. Students were given 20 min to fill in the questionnaires shortly after which they were collected by the researcher. After the end of every data collection day, the researcher checked questionnaires for completion and those found incomplete were discarded and replaced in the following day of data collection.
3.2.3. Measurement of variables
An anonymous self‐administered questionnaire was used to assess prevalence of stress and its sources. It was structured into three sections; the first section covering social demographics including age, sex, programme, year of study and place of residence. Section II measured stress, while section III assessed the stressors.
Prevalence of stress was assessed using General Health Questionnaire (GHQ‐12), with items representing manifestations of stress (Goldberg, 1978). This tool has been used to study stress in various populations including submariners (Brasher, Sparshott, Weir, Day, & Bridger, 2012), dental students (Abu‐Ghazaleh, Rajab, & Sonbol, 2011), nursing students (Okwaraji & En, 2014) and medical students (Yusoff et al., 2011). In Uganda, the GHQ‐12 has been used to study posttraumatic stress among war affected population (Ayazi, Lien, Eide, Ruom, & Hauff, 2012). Its reliability in different studies has been found to range from 78–95% (Goldberg, 1978; Quek, Low, Razack, & Loh, 2001). It measures presence or absence of stress by identifying the manifestations of stress among respondents. In this questionnaire, respondents were asked to rate the presence of each of the manifestations in themselves during the past few weeks, using a scale “not at all,” “no more than usual,” “rather more than usual” and “much more than usual.” The instrument has six reversed items and six non‐reversed questions to make a total of 12 items. The scoring method was binary where the two least symptomatic answers were scored 0 and the two most symptomatic answers are scored 1. That is, for the reversed items, “not at all” and “no more than usual” responses were scored 1, while “rather more than usual” and “much more than usual” responses were scored 0. For non‐reversed items, “not at all” and no more than usual” was scored as 0, while “rather more than usual” and “much more than usual” responses were scored 1. A score of 4 and above was considered to be a stressed case (Goldberg, 1978).
To assess sources of stress, 20 items adopted from similar studies (Shah, Hasan, Malik, & Sreeramareddy, 2010; Sreeramareddy et al., 2007) and a review of literature were included in the questionnaire. These items were grouped as academic, psychosocial and health‐related. For each potential stressor, the frequency of occurrence rated as never, rarely, sometimes, often and always which were scored as 1, 2, 3, 4 and 5 respectively were asked. The students were asked to indicate whether any of the stressors had affected them by rating how often it was encountered. Responses of rarely and never were categorized as not causing stress, while sometimes/often and always were classified as causing stress.
3.3. Data analysis
Data were analysed using SPSSv21. The number and percentage of GHQ‐12 caseness were computed to determine the prevalence of stress. For stressors, percentage and frequency of occurrence were computed to determine severity of each of the stressor.
3.4. Ethics
Ethics approval was sought for and obtained from Makerere University school of Health sciences IRB. Participants were carefully explained to the purpose, content and implications of the study before written informed consent was obtained. Anonymous questionnaires were used to ensure confidentiality.
4. RESULTS
4.1. Baseline characteristics
Of the 320 students recruited, 258 (80.6%) responded. The students’ mean age was 22.69 (SD 2.95), with almost two‐thirds male (67.1%). Majority of the respondents were medical students (80.3%). More than half of the students reported residing in University halls (68.6%), while others resided in hostels, rentals and homes. Findings have been summarized in Table 1.
Table 1.
Baseline characteristics of the respondents
| Variable | N | % |
|---|---|---|
| Sex | ||
| Male | 173 | 67.1 |
| Female | 85 | 32.9 |
| Programme | ||
| Nursing | 30 | 11.6 |
| Dental surgery | 20 | 7.8 |
| Medicine and Surgery | 207 | 80.2 |
| Year of study | ||
| I | 63 | 24.4 |
| II | 38 | 14.7 |
| III | 67 | 26.0 |
| IV | 62 | 24 |
| V | 27 | 10.5 |
| Residence of the respondent | ||
| Hall | 177 | 68.6 |
| Hostel | 26 | 10.1 |
| Rental | 28 | 10.9 |
| Home | 26 | 10.1 |
4.2. Stress
The prevalence of stress among health professionals’ students was found to be 57.4%. The GHQ‐12 survey response frequencies have been tabulated in Table 2. Female students were more stressed (60%) compared with their male counterparts (Fig. 1); however, the difference was not statistically significant. Majority of the stressed students were nursing (63.3%), compared with medical and dental students with 57% and 50% respectively. The difference, however, was not statistically significant (p = .642).
Table 2.
Health professional students’ response to General Health Questionnaire 12
| Statement | Not at all | No more than usual | Rather more than usual | Much more than usual |
|---|---|---|---|---|
| Positively stated statements | ||||
| Felt constantly under strain | 68 (26.4%) | 69 (26.7%) | 86 (33.3%) | 31 (12%) |
| Couldn't overcome difficulties | 105 (40.7%) | 94 (36.4%) | 36 (14.0%) | 9 (3.3%) |
| eeling unhappy and depressed | 141 (54.7%) | 56 (21.7%) | 38 (14.7%) | 15 (5.8%) |
| Losing confidence | 163 (63.2%) | 54 (20.9%) | 29 (11.2%) | 8 (3.1%) |
| Thinking as self as worthless | 189 (73.3%) | 29 (11.2%) | 23 (8.9%) | 9 (3.5%) |
| Loss of sleep over worry | 163 (63.2%) | 50 (19.4%) | 23 (8.9%) | 18 (7.0%) |
| Negatively stated statements | ||||
| Able to sleep | 19 (7.4%) | 172 (66.7%) | 48 (18.6%) | 17 (6.6%) |
| Playing a useful part | 24 (9.3%) | 128 (49.6%) | 67 (26%) | 31 (12%) |
| Capable of making decisions | 15 (5.8%) | 83 (32.2%) | 91 (35.3%) | 65 (25.2%) |
| Able to enjoy day to day activities | 38 (14.7%) | 132 (51.2%) | 56 (21.7%) | 28 (10.9%) |
| Able to face problems | 14 (5.4%) | 114 (44.2%) | 74 (28.7%) | 49 (19.0%) |
| Feeling reasonably happy | 25 (9.7%) | 129 (50.0%) | 59 (22.9%) | 40 (15.5%) |
Figure 1.
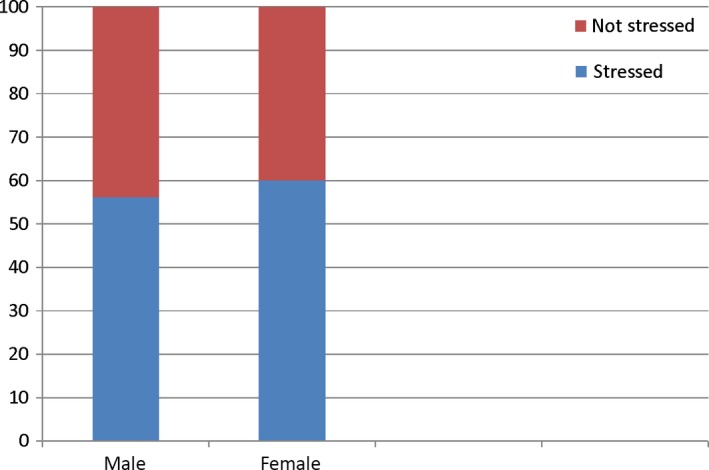
Percentage distribution of stress across gender
4.3. Sources of stress and severity
Students frequently reported academic and psychosocial stressors as most occurring. Occurrence and severity (number of respondents and percentages) of each stressor as reported by students have been summarized in Table 3. Stressors that were considered most stressful to students (rated almost/always) include academic curriculum (38%), dissatisfaction with class lectures (30.9%), long distance walk 76 (29.5%), lack of time for recreation (28.9%), performance in examination (28.3%), high parental expectations 69 (26.7%) and financial problems 63 (24.4%).
Table 3.
Percentage distribution of academic stressors among health professional students at Makerere University
| N(%) | |||
|---|---|---|---|
| Never/rarely | Sometimes | Often/always | |
| Potential stressor | |||
| Frequency of examination | 96 (37.2) | 99 (38.4) | 62 (24) |
| Performance in examination | 79 (30.6) | 103 (39.9) | 73 (28.3) |
| Academic curriculum | 92 (35.7) | 65 (25.2) | 98 (38) |
| Dissatisfaction with class lectures | 95 (36.8) | 82 (31.8) | 79 (30.9) |
| Non‐availability of learning materials | 129 (50) | 72 (27.9) | 49 (19) |
| Worry about what you will become | 162 (62.8) | 56 (21.7) | 39 (15.1) |
| Lack of time for recreation 1 | 114 (44.2) | 68 (26.4) | 74 (28.9) |
| Competition with peers | 171 (66.3) | 56 (21.7) | 27 (10.5) |
| Lack of special guidance from faculty | 104 (40.3) | 83 (32.2) | 68 (26.4) |
| Psychosocial factors | |||
| High parental expectations 1 | 140 (54.3) | 47 (18.2) | 69 (26.7) |
| Family problems | 159 (61.9) | 64 (24.8) | 34 (13.2) |
| Strikes at the university | 212 (82.2) | 35 (13.6) | 9 (3.5) |
| Long distance walk | 140 (54.3) | 40 (15.5) | 76 (29.5) |
| Inability to socialize with peers | 192 (74.4) | 38 (14.7) | 26 (10.1) |
| Financial problems | 103 (39.9) | 90 (34.9) | 63 (24.4) |
| Relationship with opposite sex | 188 (72.9) | 54 (20.9) | 14 (5.4) |
| Living conditions in hall/hostel | 162 (62.8) | 57 (22.1) | 35 (13.6) |
| Lack of interest in the course | 222 (86) | 24 (9.3) | 10 (3.9) |
| Health‐related stressors | |||
| Nutrition | 116 (64.3) | 54 (20.9) | 37 (14.3) |
| Physical illness | 194 (75) | 48 (18.6) | 14 (5.4) |
| Physical disability | 150 (96.9) | 3 (1.2) | 2 (0.8) |
| Alcohol/drug abuse | 252 (97.7) | 2 (0.8) | 2 (0.8) |
5. DISCUSSION
The study was conducted to test the following research questions: What is the prevalence of stress among undergraduate health professional students and what its sources are?
5.1. Stress
The response rate was 80.6% which corresponds closely with that (70%–90%) obtained in similar studies (Fonseca et al., 2013; Yusoff et al., 2010). This high response rate is probably due to high individual perception of stress by students thus feeling the need to be actively involved in its identification and management. Results from this study further support available evidence that health professional students are stressed (Sabita Paudel et al., 2013; Saipanish, 2003; Salam et al., 2013). In this study, more than half (57.4%) of the respondents were stressed. The prevalence of stress has been found to vary considerably (14.3%–56%) among health professional students in Asia (Salam et al., 2013). Furthermore, high prevalence rates have been reported among African health professional students (21.6%–86%) (Amr et al., 2011; Dessie et al., 2014; Ofili et al., 2009). Basing on available evidence, it is not surprising that in this present study we found high prevalence rate (57.4%) among health professional students at Makerere University. It is reported that health professional students are stressed more than students from other faculties (Aktekin et al., 2001) and this stress affects not only their physical but also mental well‐being (Danz et al., 2007; Dyrbye, Thomas, & Shanafelt, 2005; Paudel et al., 2013) which ultimately may affect patient care in future.
5.2. Stressors
Respondents reported academic pressures to be the major sources of stress and these included academic curriculum, dissatisfaction with class lectures, lack of time for recreation and performance in examinations. These stressors ranked consistently high in our study and similar to what students in other educational settings and regions have identified with (Naidu, Adams, Simeon, & Persad, 2002; Yusoff et al., 2010). Available evidence shows that academic curriculum is a major stressor to students (Sreeramareddy et al., 2007). Indeed, we found that over two in five students identified academic curriculum as a major stressor. The probable account for this could be that Makerere University is currently transiting from problem‐based learning alone to incorporate in the lecture system and this new curriculum could be stressing to students. While this is true, it is difficult to compare stress levels of students during the previous curriculum and the present curriculum as no literature is available. In addition, aspects of the academic curriculum that are stressing to students were also not identified therefore further studies should look into this.
Majority of the students also pointed out performance in examination as a stressor. This finding has been documented by other researchers in various educational settings (Fonseca et al., 2013; Sreeramareddy et al., 2007). Over one in three students pointed out lack of time for recreation as a major stressor. Sreeramareddy et al. (2007) in his study got similar findings. The probable reason for lack of time for recreation is probably due to that fact that students usually have a tight schedule ranging from school work and clinical placements. This leaves them with no time for recreation. Inadequate learning materials was another important stressor identified in our study, it is not surprising that similar findings we documented among Nigerian dental students (Sofola & Jeboda, 2006). In Africa, many countries operate in a resource limited setting and in this regard, their education sector is not past the worst. As a result, many medical schools cannot afford to avail all the necessary learning materials needed by students.
Of the psychosocial stressors, students frequently pointed out long distance walk, 76 (29.5%); high parental expectations, 69 (26.7%); and financial problems 63 (24.4%) as major stressors. Long distance walk could probably be due to the fact that most students sleep in university halls of residence which are located at the main campus of the university which is over 1.5 km from the medical school. In addition, most of the students who join medical school have been in boarding schools therefore they find it hard adapting to the system of walking to school every day. Long distance was also identified as a stressor among Nigerian health professional students (Omigbodun, Onibokun, Yusuf, Odukogbe, & Omigbodun, 2004). Naturally, children do not want to disappoint their parents, as a result these students are pushed to read so much to please their parents. It is not astonishing that high parental expectations were pointed out by majority of the students as a key stressor. This finding is similar to what Shah et al. (2010) found among Pakistani medical students (Shah et al., 2010).
In addition, a study done among Ireland nursing students also documented financial constraints as a big stressor (Nicholl & Timmins, 2005). This agrees closely with findings from our study, it is possibly because generally in developing countries people live in a resource constrained environment where most are still below the poverty line. In this regard, Uganda is not spared. It is reported that over 34.6% of the people were still leaving on less than $1.9 by 2012 (Bank, 2016). In the light of this, families where most students come from cannot provide for their financial requirements in terms of scholastic materials and basic needs, let alone money for their personal needs.
Health‐related stressors were the least mentioned by students to be a source of stress.
5.3. Limitations of the study
The measurement of manifestations of stress being self‐report may not have been an accurate measure of stress.
6. CONCLUSION
More than one half (57.4%) of health professional students are stressed. They reported the most frequently occurring stressors to be academic and psychosocial areas. Based on the findings, authors recommend the following;
There is need to strengthen peer mentorship among students so that those who have been through the system can guide the new entrants on how to manoeuvre through the system.
Further studies should be done to assess aspects of curriculum to identify which ones specifically stress students so as to guide appropriate consideration in curriculum reviews
Further studies should follow‐up students to analyse the effect of stress on various aspects of students.
CONFLICT OF INTERESTS
No conflict of interest has been declared by the authors.
AUTHOR CONTRIBUTIONS
Sharon Bright Amanya conceived the idea, designed the study protocol, collected data and did part of the analysis, drafted and reviewed the manuscript. Joyce Nakitende designed the study, collected and analysed data, and proof read the manuscript. Tom Denis Ngabirano contributed to the study design, analysis of the study findings and had significant intellectual input to the study and manuscript review. All authors approved the final manuscript.
ACKNOWLEDGEMENTS
The authors recognize the great support offered by Mr. Osingada Charles Peter, lecturer nursing department during the preparation of research protocol and implementation. Special thanks go to Dr. Rose Chalo Nabirye, Dean School of Health sciences Makerere University and Ms. Lydia Kabiri, Lecturer Nursing department for proof reading the manuscript. Mr. Denis Kalibbala, Department of Clinical epidemiology and biostatistics, Makerere University, and Prof. Edward Kumaketch, Lira University are appreciated for all the statistical help rendered. Mr. Boniface Obura, Lira University is also recognized for his great contribution in manuscript review. Above all, we thank the students who participated in this study for offering their time.
Amanya SB, Nakitende J, Ngabirano TD. A cross‐sectional study of stress and its sources among health professional students at Makerere University, Uganda. Nursing Open. 2018;5:70–76. https://doi.org/10.1002/nop2.113
REFERENCES
- Abu‐Ghazaleh, S. B. , Rajab, L. D. , Sonbol, H. N. (2011). Psychological stress among dental students at the University of Jordan. Journal of Dental Education, 75(8), 1107–1114. [PubMed] [Google Scholar]
- Aktekin, M. , Karaman, T. , Senol, Y. Y. , Erdem, S. , Erengin, H. , Akaydin, M. (2001). Anxiety, depression and stressful life events among medical students: A prospective study in Antalya, Turkey. Medical Education, 35(1), 12–17. https://doi.org/10.1046/j.1365-2923.2001.00726.x [DOI] [PubMed] [Google Scholar]
- Al‐Dubai, S. A. R. , Al‐Naggar, R. A. , AlShagga, M. A. , Rampal, K. G. (2011). Stress and coping strategies of students in a medical faculty in Malaysia. The Malaysian Journal of Medical Sciences: MJMS, 18(3), 57. [PMC free article] [PubMed] [Google Scholar]
- Amr, A. , El‐Gilany, A. H. , El‐Moafee, H. , Salama, L. , Jimenez, C. (2011). Stress among Mansoura (Egypt) baccalaureate nursing students. Pan African Medical Journal, 8, 26. https://doi.org/10.11604/pamj.2011.8.26.484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ayazi, T. , Lien, L. , Eide, A. H. , Ruom, M. M. , Hauff, E. (2012). What are the risk factors for the comorbidity of posttraumatic stress disorder and depression in a war‐affected population? a cross‐sectional community study in South Sudan. BMC Psychiatry, 12(1), 175 https://doi.org/10.1186/1471-244X-12-175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bank, W. (2016). Poverty and Equity. Available from: http://povertydata.worldbank.org/poverty/country/UGA. [last accessed 23 April 2017].
- Bramness, J. , Fixdal, T. C. , Vaglum, P. (1991). Effect of medical school stress on the mental health of medical students in early and late clinical curriculum. Acta Psychiatrica Scandinavica, 84(4), 340–345. https://doi.org/10.1111/j.1600-0447.1991.tb03157.x [DOI] [PubMed] [Google Scholar]
- Brasher, K. , Sparshott, K. F. , Weir, A. B. C. , Day, A. J. , Bridger, R. S. (2012). Short report Two year follow‐up study of stressors and occupational stress in submariners. Occupational Medicine, 62, 563–565. https://doi.org/10.1093/occmed/kqs104 [DOI] [PubMed] [Google Scholar]
- Dahlin, M. , Joneborg, N. , Runeson, B. (2005). Stress and depression among medical students: A cross‐sectional study. Medical Education, 39(6), 594–604. https://doi.org/10.1111/j.1365-2929.2005.02176.x [DOI] [PubMed] [Google Scholar]
- Danz, N. P. , Niemi, G. J. , Regal, R. R. , Hollenhorst, T. , Johnson, L. B. , Hanowski, J. M. , … Kelly, J. R. (2007). Integrated measures of anthropogenic stress in the US Great Lakes basin. Environmental Management, 39(5), 631–647. https://doi.org/10.1007/s00267-005-0293-0 [DOI] [PubMed] [Google Scholar]
- Dessie, Y. , Ebrahim, J. , Awoke, T. (2014). Mental distress among university students in Ethiopia: A cross sectional survey. Pan African Medical Journal, 15(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dyrbye, L. N. , Thomas, M. R. , Massie, F. S. , Power, D. V. , Eacker, A. , Harper, W. , … Sloan, J. A. (2008). Burnout and suicidal ideation among US medical students. Annals of Internal Medicine, 149(5), 334–341. https://doi.org/10.7326/0003-4819-149-5-200809020-00008 [DOI] [PubMed] [Google Scholar]
- Dyrbye, L. N. , Thomas, M. R. , Shanafelt, T. D. (2005). Medical student distress: causes, consequences and proposed solutions. Mayo Clinic Proceedings, 80(12), 1613–1622. [DOI] [PubMed] [Google Scholar]
- Fonseca, J. , Divaris, K. , Villalba, S. , Pizarro, S. , Fernandez, M. , Codjambassis, A. , … Polychronopoulou, A. (2013). Perceived sources of stress amongst Chilean and Argentinean dental students. European Journal of Dental Education, 17(1), 30–38. https://doi.org/10.1111/eje.12004 [DOI] [PubMed] [Google Scholar]
- Goldberg, D. (1978). Manual of the General Health Questionnaire. Berkshire, England: NFER. [Google Scholar]
- Habeeb, K. A. (2010). Prevalence of stressors among female medical students taibah university. Journal of Taibah University Medical Sciences, 5(2), 110–119. https://doi.org/10.1016/S1658-3612(10)70140-2 [Google Scholar]
- Haoka, T. , Sasahara, S. I. , Tomotsune, Y. , Yoshino, S. , Maeno, T. , Matsuzaki, I. (2010). The effect of stress‐related factors on mental health status among resident doctors in Japan. Medical Education, 44(8), 826–834. https://doi.org/10.1111/j.1365-2923.2010.03725.x [DOI] [PubMed] [Google Scholar]
- Khodarahimi, S. , Hashim, I. H. , Mohd‐Zaharim, N. (2012). Perceived stress, positive‐negative emotions, personal values and perceived social support in Malaysian undergraduate students. International Journal of Psychology and Behavioral Sciences, 2(1), 1–8. [Google Scholar]
- Lazarus, R. S. (1966). Psychological stress and the coping process. New York, NY: McGraw‐Hill. [Google Scholar]
- Naidu, R. S. , Adams, J. S. , Simeon, D. , Persad, S. (2002). Sources of stress and psychological disturbance among dental students in the West Indies. Journal of Dental Education, 66(9), 1021–1030. [PubMed] [Google Scholar]
- Nakalema, G. , & Ssenyonga, J. (2014). Academic stress: Its causes and results at a Ugandan university. African Journal of Teacher Education, 3(3). https://journal.lib.uoguelph.ca/index.php/ajote/article/view/2762/3253 [Google Scholar]
- Nicholl, H. , & Timmins, F. (2005). Programme‐related stressors among part‐time undergraduate nursing students. Journal of Advanced Nursing, 50(1), 93–100. https://doi.org/10.1111/j.1365-2648.2004.03352.x [DOI] [PubMed] [Google Scholar]
- Ofili, A. , Oriaifo, I. , Okungbowa, E. , Eze, E. U. (2009). Stress and psychological health of medical students in a Nigerian university. Nigerian Journal of Clinical Practice, 12(2), 128–133. [PubMed] [Google Scholar]
- Okwaraji, F. , & En, A. (2014). Burnout and psychological distress among nurses in a Nigerian tertiary health institution. African Health Sciences, 14(1), 237–245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Omigbodun, O. O. , Onibokun, A. C. , Yusuf, B. O. , Odukogbe, A. A. , Omigbodun, A. O. (2004). Stressors and counseling needs of undergraduate nursing students in Ibadan, Nigeria. Journal of Nursing Education, 43(9), 412–415. [DOI] [PubMed] [Google Scholar]
- Paudel, S. , Subedi, N. , Shrestha, A. (2013). Stress and its relief among undergraduate dental students in a tertiary health care centre in eastern Nepal. Dentistry, 3(157), 2161–1122. [Google Scholar]
- Polychronopoulou, A. , & Divaris, K. (2009). Dental students’ perceived sources of stress: A multi‐country study. Journal of Dental Education, 73(5), 631–639. [PubMed] [Google Scholar]
- Quek, K. F. , Low, W. Y. , Razack, A. H. , Loh, C. S. (2001). Reliability and validity of the General Health Questionnaire (GHQ‐12) among urological patients: A Malaysian study. Psychiatry and Clinical Neurosciences, 55(5), 509–513. https://doi.org/10.1046/j.1440-1819.2001.00897.x [DOI] [PubMed] [Google Scholar]
- Romano, J. L. (1992). Psychoeducational interventions for stress management and well‐being. Journal of Counseling & Development, 71(2), 199–202. https://doi.org/10.1002/j.1556-6676.1992.tb02200.x [Google Scholar]
- Saipanish, R. (2003). Stress among medical students in a Thai medical school. Medical Teacher, 25(5), 502–506. https://doi.org/10.1080/0142159031000136716 [DOI] [PubMed] [Google Scholar]
- Salam, A. , Yousuf, R. , Bakar, S. M. A. , Haque, M. (2013). Stress among medical students in Malaysia: A systematic review of literatures. International Medical Journal, 20(6), 649–655. [Google Scholar]
- Shah, M. , Hasan, S. , Malik, S. , Sreeramareddy, C. T. (2010). Perceived stress, sources and severity of stress among medical undergraduates in a Pakistani medical school. BMC Medical Education, 10(1), 2 https://doi.org/10.1186/1472-6920-10-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sofola, O. , & Jeboda, S. (2006). Perceived sources of stress in Nigerian dental students. European Journal of Dental Education, 10(1), 20–23. https://doi.org/10.1111/j.1600-0579.2006.00391.x [DOI] [PubMed] [Google Scholar]
- Sreeramareddy, C. T. , Shankar, P. R. , Binu, V. S. , Mukhopadhyay, C. , Ray, B. , Menezes, R. G. (2007). Psychological morbidity, sources of stress and coping strategies among undergraduate medical students of Nepal. BMC Medical Education, 7(1), 26 https://doi.org/10.1186/1472-6920-7-26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yusoff, M. S. B. , Rahim, M. S. B. , Yaacob, M. J. (2010). Prevalence and sources of stress among Universiti Sains Malaysia medical students. The Malaysian Journal of Medical Sciences: MJMS, 17(1), 30. [PMC free article] [PubMed] [Google Scholar]
- Yusoff, M. , Yee, L. Y. , Wei, L. H. , Siong, T. C. , Meng, L. H. , Bin, L. X. , Rahim, A. F. A. (2011). A study on stress, stressors and coping strategies among Malaysian medical students. International Journal of Students’ Research, 1(2), 45 https://doi.org/10.5549/IJSR.1.2.45-50 [Google Scholar]