

Summary
Background
Snacking among US preschoolers has increased in recent decades, raising questions about whether snacking contributes to dietary excess.
Objectives
This research aimed to characterize snacking contributions to dietary excess and to evaluate associations with appetite and weight among preschool‐aged children.
Methods
This study is a cross‐sectional, observational study of 187 Hispanic low‐income preschoolers. Three 24‐h dietary recalls were used to assess snacking frequency and parameters of dietary excess including energy, saturated fat, trans fats and added sugars. Parental reports of child satiety responsiveness, food responsiveness, and enjoyment of food were obtained. Child height and weight were measured.
Results
Children consumed 28% (395 kcal) of daily energy from snacks eaten at 2.3 ± 1.0 occasions per day. Greater snacking frequency was associated with greater daily intakes of energy (p < 0.05) and added sugars (p < 0.001). Among overweight/obese children, higher enjoyment of food was associated with more frequent snacking and greater energy intake from snacks (p = 0.01). Inverse associations of enjoyment of food with snacking frequency and energy intake were seen among normal weight children (p < 0.05).
Conclusions
More frequent snacking among low‐income Hispanic preschoolers may contribute to excessive intakes of energy and added sugars, particularly among overweight/obese children with greater motivation to eat.
Keywords: Appetite, child, snacking, weight
Introduction
Prevailing wisdom says that young children need snacks, generally defined as foods eaten between meals, to meet nutritional needs. The American Academy of Pediatrics as well as the US Department of Agriculture recommend 2‐3 small snacks per day for preschool‐aged children 1, 2. However, secular increases in frequency of snacking among young children have raised concerns about the contribution of snacking to dietary excess and obesity. In 2009, US preschoolers consumed 182 calories more per day from snacks than in 1977 3. These trends are consistent across preschoolers from varied socioeconomic status and race/ethnicities 3. Data from the 2009–2010 National Health and Nutrition Examination Survey indicate that preschoolers currently snack almost three times daily, consuming approximately 400 calories or 28–29% of daily energy from snacks 3, 4. Desserts, sugar‐sweetened beverages, and salty foods are among the most frequently consumed snacks by US children 2–18 years 3. In 2009–2010, children's snacks consisted of 19–21% protein, 39–42% sugars and 25–27% fats 4. While children consume a significant amount of energy from snacks and snacks frequently eaten tend to be of poor nutritional quality, the extent to which snacking contributes to excessive dietary intakes is unclear, particularly among preschool‐aged children for whom snacks are believed to be nutritionally most important.
Whether snacking poses the same risk of dietary excess for all children is also unknown. Heavier children have been reported to be less responsive to satiety cues 5, 6 and more responsive to food cues 5, 7. In turn, there is evidence that these appetitive traits may influence weight gain in early development 6, 7. Taken together, such evidence suggests that snacking may pose a greater risk of dietary excess for overweight/obese children and those who demonstrate poor appetite regulation. To date, these hypotheses have not been tested.
This research was conducted to evaluate snacking contributions to dietary excess among low‐income Hispanic preschool‐aged children. In particular, associations of snacking frequency with children's intakes of energy, saturated, and trans fat and added sugars were characterized. Further, this research considered whether snacking poses the same risk of dietary excess for all children, by evaluating associations of child weight status and appetite with snacking frequency and energy. Understanding snacking contributions to children's diets addresses an important research need identified by the Dietary Guidelines for Americans Advisory Committee to evaluate effects of common variations in dietary patterns on nutrient intakes among small children 8. Further, the focus on Hispanic children is significant given that they are disproportionately affected by obesity 9.
Methods
Design
A secondary analysis of baseline data from a larger 18‐month longitudinal study of parental influences on eating self‐regulation during preschool among Hispanic children was conducted. Caregiver reports of child appetite were assessed by questionnaire, and caregiver reports of child food intake, including snacking, were assessed using three 24‐h recalls. Child height and weight were measured.
Participants
Convenience sampling was used to recruit 4–5‐year‐old Hispanic children and their caregivers from two Head Start programme districts in Houston, Texas. Eligibility for Head Start includes a family income equal to or below the federal poverty level. Participants were recruited through parent meetings, flyers sent home with children, and engagement of the Head Start manager and staff in recruitment and telephone calls to the home. Eligibility was assessed via phone. Children with food allergies and/or special diets were excluded. Parents provided consent for their own and their child's participation. Procedures were approved and carried out in accordance with standards of Baylor College of Medicine and Temple University Institutional Review Boards.
Procedures
Demographic, anthropometric, and questionnaire data were collected at the US Department of Agriculture/Agricultural Research Service Children's Nutrition Research Center at Baylor College of Medicine. Dietary recalls were completed via telephone interviews by trained staff.
Measures
Demographic information
Caregivers provided basic demographic information on child age, sex, race, caregiver sex, marital status, employment status, and education.
Child and caregiver body mass index
Child and caregiver weight (kg) and height (cm) were measured in duplicate by using electronic scales (Health‐o‐Meter model 752KL, Sunbeam Products, Inc.) and stadiometers (Seca model 214, Seca Inc.) to the nearest 0.1 kg and 0.1 cm, respectively. Child BMI‐for‐age percentiles and z‐scores were calculated in children in accordance with Centers for Disease Control reference standards 10. Child overweight (≥85th–<95th) and obesity (≥95th) were categorized by using BMI‐for‐age percentiles 11. Caregiver BMI scores were categorized as normal weight (BMI ≤ 24.9), overweight (BMI ≥ 25), or obese (BMI ≥ 30) 12.
Dietary intake
Two weekday and one weekend 24‐h dietary recalls were collected by trained research staff. All recalls were conducted via telephone. Caregivers were asked to complete the recalls for the child and were asked to obtain information from Head Start staff on meals consumed at the preschool program. Caregivers were provided a Food Amounts booklet with 2D measures as an aid to estimate portion size. The Nutrition Data System for Research Software version 2013 was used to estimate snacking and daily intakes of energy and selected macronutrients associated with dietary excess. The 2015 US Dietary Guidelines for Americans recommends reducing intake of macronutrients associated with excessive energy intake including solid fats (e.g. saturated and trans fats) and sugars, particularly those added during food processing 13. Therefore, this research focused on energy, saturated fat, trans fats and added sugar as the main parameters of excessive dietary intake. Total fat, total carbohydrate and sugars were also reported. Eating occasions were classified by participants (i.e. breakfast, lunch, dinner, snack, or other). Snacks were defined as any food and/or beverage characterized by participants as a snack. Following previous research, any food or beverage consumed within 15 min of the previous eating occasion was considered part of the previous occasion 3. Of 860 eating occasions defined as snacks in this dataset, 55 involved a beverage only. Additionally, of the 3124 food and beverage items consumed as part of a snack, 945 were beverages. All dietary data are presented as 3‐day mean values.
Parent report of children's eating behaviour
The Children's Eating Behaviour Questionnaire 14 (CEBQ) is a 35‐item questionnaire assessing parent perceptions of eight trait‐like dimensions of child eating behaviour. This study focused on satiety responsiveness (five items; e.g. ‘My child leaves food on his/her plate at the end of a meal’), food responsiveness (four items; e.g. ‘Given the choice, my child would eat most of the time’) and enjoyment of food (four items; e.g. ‘My child enjoys eating’) given associations with weight status 6, 7, 15 and evidence of genetic influence 16. Questions utilized a 5‐point ‘never’ to ‘always’ Likert‐type response options, with possible scores from 0 to 4. The CEBQ has demonstrated good internal consistency and test–retest reliability in ethnically diverse children 15, 17, including low‐income Hispanic children 18. Internal consistency (Cronbach's α) of the food responsiveness, enjoyment of food and satiety responsiveness subscales in this sample were 0.79, 0.72 and 0.68, respectively.
Statistical analyses
Analyses were conducted by using SAS Version 9.3 (Cary, NC). Descriptive statistics were calculated for all variables of interest. ANOVA was used to evaluate associations between snacking frequency and children's snack and daily nutrient intakes, including energy saturated fat, trans fat and added sugar. Unadjusted models are presented; results did not differ from those produced by sensitivity analyses adjusting for child age (months) and gender, and parent educational attainment, marital status, employment status and BMI. Pearson's correlations were used to describe bivariate relationships between child weight and appetite traits. Ordinary least squares regression was used to evaluate child appetite and weight status as predictors of snacking frequency and energy consumed from snacks. Interactions between child weight status and each appetitive trait were tested in separate models to avoid potential co‐linearity and to avoid interpreting three‐way interactions. All data are presented as mean ± SD unless otherwise indicated. Statistical significance was inferred from p values ≤0.05.
Results
Participant demographics
Analyses were performed with data from 181 of 187 children who had complete dietary data. Demographic characteristics of those children and caregivers are presented in Table 1. Of 181 children, 94 were male and 87 were female. All children identified as Hispanic or Latino and were between the ages of 4 to 5y. All interviewed caregivers were female, and all but two identified as the mother of the enrolled child. Most caregivers were married or cohabiting (70%, n = 126) and most were unemployed (77%, n = 140), with close to a majority reporting a high school diploma or less (65%, n = 118).
Table 1.
Sociodemographic characteristics of study sample (n = 181)
| Child | % (n) |
|---|---|
| Gender | |
| Female | 48.1 (87) |
| Male | 51.9 (94) |
| Age (years) | |
| 4 | 65.8 (119) |
| 5 | 34.3 (62) |
| BMI percentile | 73.5 (25.8)† |
| Weight status | |
| Underweight | 1.1 (2) |
| Normal weight | 51.4 (93) |
| Overweight | 21.6 (39) |
| Obese | 26.0 (47) |
| Caregiver | % (n) |
|---|---|
| Marital status | |
| Single | 30.4 (55) |
| Married/co‐habiting | 69.6 (126) |
| Employment | |
| Employed | 22.7 (41) |
| Not employed | 77.4 (140) |
| Educational attainment | |
| <High school | 40.3 (73) |
| Completed high school | 24.9 (45) |
| Some college/completed college | 34.8 (63) |
| Weight status‡ | |
| Normal weight | 17.1 (28) |
| Overweight | 31.1 (51) |
| Obese | 51.8 (85) |
Mean (SD).
BMI not reported for pregnant caregivers (n = 14) and those missing weight measurements (n = 1).
Snacking frequency, energy and macronutrient intakes
The number of daily snacking occasions ranged from 1 to 5.3, with a mean of 2.3 snacking occasions per day. Most children either consumed one (~30% of the sample) or two snacks (~40% of the sample) daily; however, approximately one in four children consumed three or more snacks daily. Neither snacking frequency nor snacking energy intake was associated with child (i.e. age, weight status) and caregiver demographic characteristics (i.e. marital status, education, employment and weight status) (data not shown). Children's daily energy intake from snacks was 395 kcal, representing 28% of total daily energy intake (Supplemental table). Similar proportions of daily saturated and trans fat intakes (28–29%) were consumed from snacks. However, more than 40% of children's daily intakes of added sugars came from snacks.
As shown in Table 2, children who snacked more frequently tended to consume greater amounts of energy from snacks (p < 0.0001). More frequent snacking was also associated with greater intakes of saturated fats, trans fats and added sugars from snacks (all p < 0.0001). Additionally, more frequent snacking was associated with greater daily intakes of energy, carbohydrates, sugars and added sugars (all p < 0.001). Conversely, more frequent snacking was associated with a lower percentage of daily energy from fat (p < 0.001).
Table 2.
Children's snacking and total daily intakes by daily snacking frequency (n = 181)
| Snack frequency (occasions per day) | |||||
|---|---|---|---|---|---|
| 1 per day (n = 60) | 2 per day (n = 77) | 3 per day (n = 31) | ≥4 per day (n = 19) | ||
| Mean (SE) | Mean (SE) | Mean (SE) | Mean (SE) | Estimate of linear trend (P df = 1) | |
| Snack intake | |||||
| Energy (kcal) | 249.0 (21.7) | 409.3 (19.1) | 541.8 (30.2) | 629.5 (46.6) | <0.001 |
| Fat (g) | 7.8 (1.0) | 12.5 (0.8) | 15.2 (1.3) | 17.3 (2.1) | <0.001 |
| Saturated fat (g) | 3.1 (0.4) | 4.8 (0.3) | 6.0 (0.5) | 7.0 (0.8) | <0.001 |
| Trans fat (g) | 0.35 (0.07) | 0.54 (0.06) | 0.62 (0.09) | 0.83 (0.14) | 0.002 |
| % Snack energy | 26.6 (1.1) | 26.8 (1.0) | 23.9 (1.6) | 24.1 (2.4) | 0.21 |
| Carbohydrate (g) | 39.3 (3.5) | 65.7 (3.1) | 91.1 (4.8) | 106.8 (7.4) | <0.001 |
| Sugars (g) | 24.2 (2.5) | 41.6 (2.1) | 62.0 (3.4) | 69.6 (5.2) | <0.001 |
| Added sugars (g) | 12.2 (1.9) | 20.8 (1.7) | 28.4 (2.6) | 33.7 (4.0) | <0.001 |
| % Snack energy | 64.8 (0.02) | 64.8 (0.01) | 68.6 (0.02) | 68.6 (0.03) | 0.18 |
| Total daily intake | |||||
| Energy (kcal) | 1341.7 (50.2) | 1382.5 (44.3) | 1421.4 (69.9) | 1625.4 (107.9) | 0.02 |
| Fat (g) | 47.5 (2.3) | 46.8 (2.1) | 46.7 (3.2) | 50.0 (5.0) | 0.66 |
| Saturated fat (g) | 17.1 (0.9) | 16.4 (0.8) | 16.5 (1.2) | 18.3 (1.9) | 0.57 |
| Trans fat (g) | 1.8 (0.1) | 1.7 (0.1) | 1.7 (0.2) | 1.9 (0.3) | 0.62 |
| % Daily energy | 31.3 (0.01) | 30.2 (0.01) | 29.0 (0.01) | 27.1 (0.01) | 0.005 |
| Carbohydrate (g) | 178.4 (7.2) | 193.8 (6.3) | 205.6 (10.0) | 247.0 (15.4) | <0.001 |
| Sugars (g) | 91.0 (4.5) | 104.3 (3.9) | 116.4 (6.2) | 139.4 (9.6) | <0.001 |
| Added sugars (g) | 39.5 (3.4) | 50.3 (2.9) | 51.5 (4.6) | 70.6 (7.1) | <0.001 |
| % Daily energy | 53.4 (0.01) | 56.3 (0.01) | 58.2 (0.01) | 61.4 (0.02) | <0.001 |
Associations of snacking frequency and energy with child weight and appetite
Almost half of the children were either overweight or obese (47%, n = 86). Parent ratings of satiety responsiveness (mean ± SD = 2.9 ± 0.5), food responsiveness (mean ± SD = 2.2 ± 0.9) and enjoyment of food (mean ± SD = 3.8 ± 0.7) were associated with child weight status. Higher child BMI‐for‐age z‐scores were associated with lower satiety responsiveness (r = −0.22, p < 0.01), higher food responsiveness (r = 0.16, p < 0.05), and greater enjoyment of food (r = 0.16, p < 0.05).
Parent reports of child appetite and weight were evaluated as predictors of snacking frequency and energy. Neither child appetite nor weight status was associated with snacking frequency or energy consumed from snacks when considered independently as main effects. Rather, associations of child appetite with snacking frequency and energy appeared to differ by child weight status (Fig. 1). Among overweight/obese children, snacking frequency (panel a, p = 0.01) and energy consumed from snacks (panel b, p = 0.01) were higher among children with greater enjoyment of food, whereas the opposite relationship was seen for normal weight children. Similarly, among overweight/obese children, energy consumed from snacks tended to be greater among children with higher food responsiveness (panel d, p = 0.05), whereas the association was not significant for normal weight children. Interactions of satiety responsiveness and child weight status were not significant for the outcomes of snacking frequency or energy intake from snacks (panels e and f).
Figure 1.
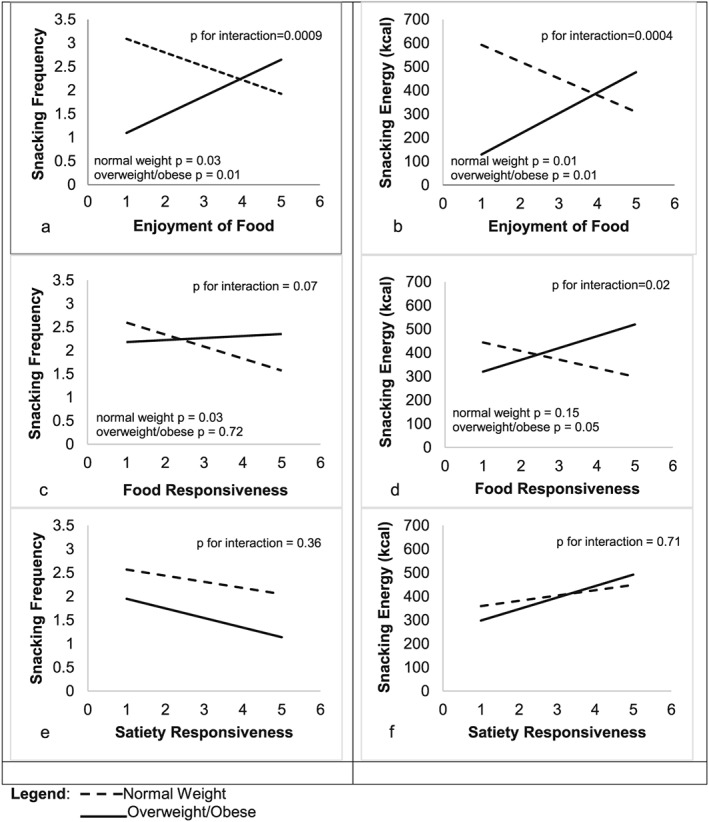
Associations of appetite characteristics with daily snacking frequency and energy by children's weight status. Interactions of child appetite and weight status to predict snacking frequency and energy were tested by using ordinary least squares regression. Greater snacking frequency (a) and energy (b) were observed among overweight/obese children with greater enjoyment of food (p = 0.01). Greater snacking energy was also observed among overweight/obese children with greater food responsiveness (d, p = 0.05)
Discussion
Surprisingly few studies have considered snacking contributions to dietary intake among young children for whom snacks are believed to be most important 3, 4, 19, 20, 21. In this study, more frequent snacking among Hispanic preschoolers was associated with greater intakes of nutrients that are recommended to be consumed in limited quantities (e.g. added sugar). This analysis was also the first to evaluate the role of child appetite and weight in snacking contributions to dietary excess among preschool‐aged children. Among preschoolers with overweight and obesity, energy consumed from snacks was higher among children who demonstrated high food enjoyment and food responsiveness. These findings provide new evidence that snacking may confer greatest risk of dietary excess for overweight and obese children with greater food motivation.
A handful of studies have reported associations of snacking with parameters of dietary excess. Associations of snacking frequency with snacking and daily energy are consistent with a previous analysis of US children aged 2–18 years by Nicklas, O'Neil and Fulgoni, in which a variety of snacking patterns was associated with higher daily energy intakes compared with not snacking 20. The association of more frequent snacking with increased daily energy intake observed in this study suggests that children may not compensate for energy consumed at snacking occasions by eating less at meals. While more frequent snacking among children may be associated with greater energy intakes, the extent to which the observed energy intakes were excessive is not possible to discern at an individual level given that children's energy requirements were not assessed. In this study, mean daily energy intakes at each level of snacking frequency were roughly close to the 1200–1600 kcal d−1 range of estimated energy needs for children 3–5 years 13. The amount of energy consumed from snacks by children who consumed more than two snacks daily, however, exceeded the mean energy consumed from snacks by US preschoolers (464 kcal, based on an upper limit for daily energy needs of 1600 kcal d−1 for 3–5‐year‐old children 13 and an assumption of 28–29% of daily energy consumed snacks 4). Moreover, greater snacking frequency was related to children's intake of several nutrients believed to contribute to excessive energy intake and recommended to be limited in children's diets 13. These findings align with those from studies of older children which demonstrate that snacking frequency is positively associated with excess intake of added sugars 22 and solid fat 20.
The relationship between snacking and weight status among children is debated. Several studies, including a meta‐analysis, have observed an inverse relationship between eating frequency (i.e. number of eating occasions) and body weight 23, while others found no relationship 24 or a positive association among children consuming diets high in sweetened beverages, salty snacks and sweet foods 25. In this study, the association of child weight status with energy consumed from snacks varied by children's food responsiveness and enjoyment of food. Enjoyment of food and food responsiveness represent trait‐like dimension of eating behaviour that, like other aspects of appetite, has a heritable component 16. Although, distinct dimensions both reflect heightened food approach or motivation to eat 15 and have been positively associated with child weight 6, 15. That higher snacking frequency and energy intakes were seen among normal weight children with lower levels of enjoyment of food could represent a ‘grazing’ pattern of eating. In contrast, overweight children with greater enjoyment of food snacked more frequently and had higher intakes of snacking and daily energy as well as added and total sugars. Overall, these findings suggest that snacking may not pose appreciable risk of dietary excess for normal weight preschoolers but may be problematic for overweight and obese children with greater appetitive drives. These findings may also reflect a more general predisposition of overweight/obese children towards reward sensitivity. A recent representative cross‐sectional study of Belgian adolescents showed associations of reward sensitivity and unhealthy snacks 26. Further, previous research has observed greater deficits in reward sensitivity and inhibitory control among heavier children that appear to contribute to overeating tendencies 27, 28. Prospective or experimental studies are needed to disentangle relationships between child appetite, snacking behaviours, and self‐regulatory abilities.
Several limitations qualify the interpretation of this research. First, the findings need to be replicated in children of other racial/ethnic groups as meal and snacking patterns may reflect sociocultural influences. The use of a convenience sample may also limit the representativeness and generalizability of the findings. At the same time, the observed mean snacking frequency and energy (as a proportion of daily energy intake) were similar to national estimates for children 2–6 years based on National Health and Nutrition Examination Survey data 3, 4. Second, that caregivers provided data on both child snacking as well as child appetite may have introduced measurement bias. Parents of overweight children have been observed to underreport children's food intake 29. If present in these data, this type of bias would hypothetically underestimate associations between the variables of interest. Finally, psychometric properties of the CEBQ are not yet well‐described in ethnically diverse samples. A confirmatory factor analysis of the CEBQ among low‐income Hispanics and African Americans in New York City, NY, revealed some deviations from the original factor structure 30, although comparisons with the original model were only indirect. However, this study observed acceptable internal consistencies for the subscales of interest. Further, associations of child appetite with BMI‐for‐age z‐scores observed in this study are consistent with those reported in white and higher income samples 15.
In conclusion, this research provides new evidence that frequent snacking may contribute to greater intakes of energy and added sugars among low‐income Hispanic preschoolers. Findings further suggest that overweight/obese children with stronger appetitive drive may be particularly at risk of excessive intakes from snacks. These findings suggest that providing frequent snacking opportunities may be more detrimental than beneficial for overweight/obese preschoolers who are oriented towards food. Additional research is needed to understand the temporal relationships between appetitive traits, snacking behaviours and child weight as well as how to optimally structure snacking for those children with heightened food motivation.
Funding
NIH NICHD R01 HD062567‐01A1/05 (SOH, JOF, TO) and NICHD R21 HD074554 (JOF)
Conflict of Interest Statement
No conflict of interest was declared.
Supporting information
Supplemental table: Descriptive statistics for snacking and daily intakes of nutrients among Hispanic preschoolers (n = 181)
Supporting info item
Author Contributions
SOH, JOF and TMO designed the research; NEMC and KV conducted the research; ER, KWB, AD and TAC analyzed the data; all authors wrote the paper; JOF, SOH and KWB had primary responsibility for final content.
Rudy, E. , Bauer, K. W. , Hughes, S. O. , O'Connor, T. M. , Vollrath, K. , Davey, A. , Correa, N. E. M. , Chen, T.‐A. , and Fisher, J. O. (2018) Interrelationships of child appetite, weight and snacking among Hispanic preschoolers. Pediatric Obesity, 13: 38–45. doi: 10.1111/ijpo.12186.
References
- 1. U.S. Department of Agirculture . Meal and snack pattern B. 2016. [WWW document]. URL http://www.choosemyplate.gov/downloads/PatternB1000cals.pdf.
- 2. American Academy of Pediatrics . Committee on nutrition In: Kleinman RE. (ed.). Pediatric Nutrition Handbook. University of Michigan: American Academy of Pediatrics: Elk Grove, IL, 2004. [Google Scholar]
- 3. Piernas C, Popkin BM. Trends in snacking among U.S. children. Health Aff (Millwood) 2010; 29: 398–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Agricultural Research Service . Table 25: Snacks: percentages of selected nutrients contributed by foods eaten at snack occasions, by gender and age, in the United States, 2009–2010. What We Eat in America, NHANES 2009–2010. Washington, D.C.: US Department of Agriculture; 2012.
- 5. Cross MB, Hallett AM, Ledoux TA, O'Connor DP, Hughes SO. Effects of children's self‐regulation of eating on parental feeding practices and child weight. Appetite 2014; 81: 76–83. [DOI] [PubMed] [Google Scholar]
- 6. Mallan KM, Nambiar S, Magarey AM, Daniels LA. Satiety responsiveness in toddlerhood predicts energy intake and weight status at four years of age. Appetite 2014; 74: 79–85. [DOI] [PubMed] [Google Scholar]
- 7. van Jaarsveld CH, Boniface D, Llewellyn CH, Wardle J. Appetite and growth: a longitudinal sibling analysis. JAMA Pediatr 2014; 168(4): 345–350. [DOI] [PubMed] [Google Scholar]
- 8. Dietary Guidelines Advisory Committee . Scientific Report of the 2015 Dietary Guidelines Advisory Committee 2015; http://www.health.gov/dietaryguidelines/2015‐scientific‐report/PDFs/Scientific‐Report‐of‐the‐2015‐Dietary‐Guidelines‐Advisory‐Committee.pdf.
- 9. Ogden C, Carrol M, Kit B, Flegal K. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014; 11(8): 806–814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Kuczmarski RJ, Ogden CL, Guo SS, et al. CDC growth charts for the United States: methods and development. Vital Health Stat 11 2000; 2002: 1–190. [PubMed] [Google Scholar]
- 11. Barlow SE. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 2007; 120: S164–192. [DOI] [PubMed] [Google Scholar]
- 12. Centers for Disease Control and Prevention . About BMI for Adults. 2015. [WWW document] URL http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html.
- 13. U.S. Department of Health and Human Services and U.S. Department of Agriculture . Dietary Guidelines for Americans, 8th edn. Government Printing Office: Washington, D.C., 2015. [Google Scholar]
- 14. Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the Children's Eating Behaviour Questionnaire. J Child Psychol Psychiatry 2001; 42: 963–970. [DOI] [PubMed] [Google Scholar]
- 15. French SA, Epstein LH, Jeffery RW, Blundell JE, Wardle J. Eating behavior dimensions. Associations with energy intake and body weight. A review. Appetite 2012; 59: 541–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Carnell S, Wardle J. Appetite and adiposity in children: evidence for a behavioral susceptibility theory of obesity. Am J Clin Nutr 2008; 88: 22–29. [DOI] [PubMed] [Google Scholar]
- 17. Mallan KM, Liu WH, Mehta RJ, Daniels LA, Magarey A, Battistutta D. Maternal report of young children's eating styles. Validation of the Children's Eating Behaviour Questionnaire in three ethnically diverse Australian samples. Appetite 2013; 64: 48–55. [DOI] [PubMed] [Google Scholar]
- 18. Frankel LA, O'Connor TM, Chen TA, Nicklas T, Power TG, Hughes SO. Parents' perceptions of preschool children's ability to regulate eating. Feeding style differences. Appetite 2014; 76: 166–174. [DOI] [PubMed] [Google Scholar]
- 19. Jahns L, Siega‐Riz AM, Popkin BM. The increasing prevalence of snacking among US children from 1977 to 1996. J Pediatr 2001; 138: 493–498. [DOI] [PubMed] [Google Scholar]
- 20. Nicklas TA, O'Neil CE, Fulgoni VL. Relationship between snacking patterns, diet quality and risk of overweight and abdominal obesity in children. Int J Child Health and Nutr 2013; 2: 189–200. [Google Scholar]
- 21. Bremner B, Langenhoven ML, Swanepoel AS, Steyn M. The snacking habits of white preschool children. S Afr Med J 1990; 78: 472–475. [PubMed] [Google Scholar]
- 22. Dwyer JT, Evans M, Stone EJ, et al. Adolescents’ eating patterns influence their nutrient intakes. J Am Diet Assoc 2001; 101: 798–801. [DOI] [PubMed] [Google Scholar]
- 23. Lioret S, Touvier M, Lafay L, Volatier JL, Maire B. Are eating occasions and their energy content related to child overweight and socioeconomic status? Obesity 2012; 16: 2518–2523. [DOI] [PubMed] [Google Scholar]
- 24. Carson V, Janssen I. The mediating effects of dietary habits on the relationship between television viewing and body mass index among youth. Pediatr Obes 2012; 7: 391–398. [DOI] [PubMed] [Google Scholar]
- 25. Rodriguez‐Ramirez S, Mundo‐Rosas V, Garcia‐Guerra A, Shamah‐Levy T. Dietary patterns are associated with overweight and obesity in Mexican school‐age children. Arch Latinoam Nutr 2011; 61: 270–278. [PubMed] [Google Scholar]
- 26. De Cock N, Van Lippevelde W, Vervoort L, et al. Sensitivity to reward is associated with snack and sugar‐sweetened beverage consumption in adolescents. Eur J Nutr 2015; 55(4): 1623–1632. [DOI] [PubMed] [Google Scholar]
- 27. Nederkoorn C, Coelho JS, Guerrieri R, Houben K, Jansen A. Specificity of the failure to inhibit responses in overweight children. Appetite 2012; 59: 409–413. [DOI] [PubMed] [Google Scholar]
- 28. van den Berg L, Pieterse K, Malik JA, et al. Association between impulsivity, reward responsiveness and body mass index in children. Int J Obes (Lond) 2011; 35: 1301–1307. [DOI] [PubMed] [Google Scholar]
- 29. Fisher JO, Johnson RK, Lindquist C, Birch LL, Goran MI. Influence of body composition on the accuracy of reported energy intake in children. Obes Res 2000; 8: 597–603. [DOI] [PubMed] [Google Scholar]
- 30. Sparks MA, Radnitz CL. Confirmatory factor analysis of the Children's Eating Behaviour Questionnaire in a low‐income sample. Eat Behav 2012; 13: 267–270. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental table: Descriptive statistics for snacking and daily intakes of nutrients among Hispanic preschoolers (n = 181)
Supporting info item