

Abstract
Background:
The current standard of treatment for advanced hepatocellular cancer Hepatocellular carcinoma (HCC) is Sorafenib. Data regarding its tolerance and adverse event profile in Indian patients is scarce.
Materials and Methods:
The primary aim of this analysis was to assess the adverse events (Grade 3 and Grade 4 as per CTCAE v4.0) and requirements for dose reduction with sorafenib in advanced HCC. Details of consecutive patients started on 800 mg/day dosing were obtained from a prospectively maintained database (over a period of 6 months) and analyzed.
Results:
Thirty-nine patients were available for inclusion in the study. Median age was 58 years (range: 20–75). All patients were classified as Barcelona clinic liver cancer C. Common side effects seen were liver dysfunction (38.5%), hand-foot-syndrome-rash (HFSR) (Grade 2 and 3-25.6%), fatigue (Grade 2 and Grade 3–10.3%), and diarrhea (7.7%). Dose reduction was required in 43.6% of patients. Drug interruptions/cessation was required in 38.5% of patients within the first four months of treatment. Nearly 41% of patients required cessation of sorafenib due to intolerable side-effects while 28.2% stopped sorafenib due to progressive disease. At a median follow-up of 4.9 months, median event-free survival (EFS) was 4.20 months (95% confidence interval: 3.343–5.068).
Conclusion:
A higher incidence of liver dysfunction and HFSR is seen in Indian patients as compared to published data. A significant proportion of patients required cessation of sorafenib due to adverse events in our series. However, EFS remains on par with that seen in larger studies with sorafenib in advanced HCC.
Keywords: Adverse events, hepatocellular carcinoma, India, liver dysfunction, sorafenib
Introduction
The current standard of treatment for advanced hepatocellular carcinoma (HCC) is sorafenib, an oral multikinase inhibitor[1] and its superiority over supportive care has been shown in two-Phase 3 trials, with a slightly lower survival benefit in the Asian population as compared to the outcomes in the SHARP trial.[2,3]
Materials and Methods
The primary aim of this analysis was to assess the adverse events and requirements for dose reduction with sorafenib 800 mg/day dosing in consecutive patients with advanced HCC while the secondary end-point was evaluation of event-free survival (EFS). Details of consecutive patients were obtained from a prospectively maintained trial database evaluating the incidence of hand-foot syndrome as part of another ongoing study in our institution. Patients enrolled in the study from 1.1.2016 to 1.7.2016 were screened for entry into the study. The reason for using this database was specifically because patients were consecutive, and patients were started on full dose in this study rather than lower doses as is sometimes used in clinical practice. The short time-frame from which patient data were selected is also because our primary aim was an assessment of tolerance with full doses rather than an evaluation of outcomes although this was a secondary end-point. From this database, patients who satisfied the following criteria were included:
Unresectable HCC, not feasible for further liver-directed therapy (LDT)
Child Pugh A and B
Barcelona clinic liver cancer (BCLC) B (if not feasible for LDT) and BCLC C
Started on sorafenib 800 mg/day dosing.
Before starting sorafenib, investigations that were mandatory included a complete hemogram, renal function tests, liver function tests, serum sodium and potassium levels, thyroid function tests, 24 h urinary protein, and electrocardiography and two-dimensional echo. Standard dose reduction criteria while on sorafenib were used.[3]
Baseline demographic details including comorbidities, disease status, and vascular involvement were obtained. Grade 3 and Grade 4 adverse events (as per Common Terminology Criteria for Adverse Events (CTCAE) version 4.0) were extracted for analysis from hospital electronic medical records.
EFS was calculated from the start of therapy to the date of progression (radiological), permanent cessation of drug due to adverse events or otherwise, loss to follow-up, or death from any cause (if disease had not progressed). Median EFS was estimated using Kaplan–Meier method. SPSS version 20 (IBM)was used for statistical input and analysis.
Results
Baseline demographic and disease characteristics
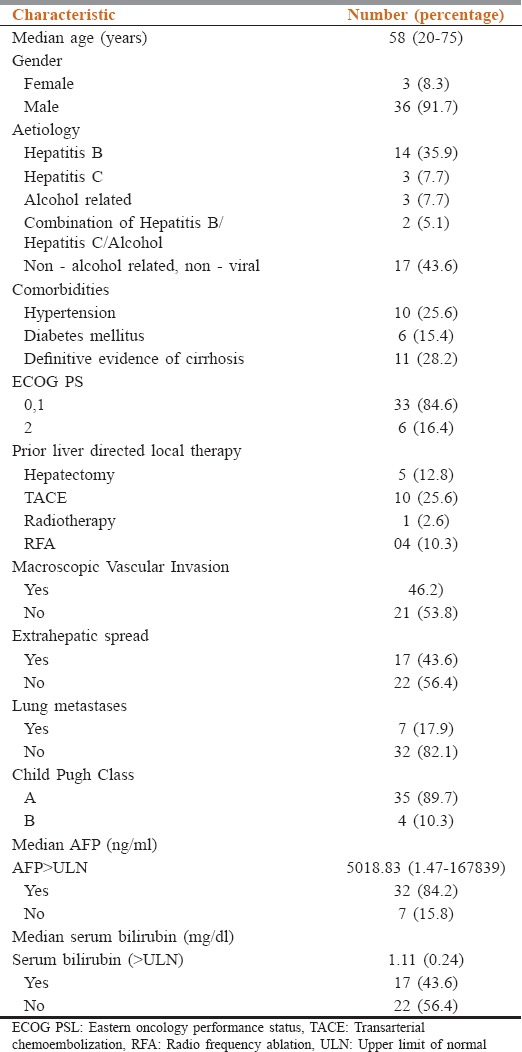
Thirty-nine patients satisfied the predetermined inclusion criteria within the given time-frame, and their records were analyzed. Median age of patients in the study was 58 years (range: 20–75). Prior LDT received was transarterial chemoembolization, hepatectomy, radiofrequency ablation, and radiotherapy in 25.6%, 12.8%, 10.3%, and 2.6% of patients, respectively. Macroscopic vascular invasion was seen in 46.2% of patients. All patients were classified as BCLC C status. AFP levels above upper limits were noted in 84.2% of patients. Other baseline characteristics are enumerated in Table 1.
Table 1.
Baseline demographic and clinical characteristics
Drug administration, adverse events, and event-free survival
Common adverse events seen hand-foot syndrome-rash (HFSR) (Grade 2 and Grade 3%–25.6%), transamintis/hyperbilirubinemia (38.5%), fatigue (Grade 2 and Grade 3%–10.3%), and diarrhea (7.7%). Dose reductions were required in 43.6% of patients. 38.5% of patients required either temporary (≥1 week) or permanent cessation of sorafenib during the initial 4 months of treatment.
At a median follow-up of 4.9 months, the median EFS was 4.2 months (95% confidence interval: 3.3-5.0). Till cutoff date into the analysis, 15.4% of patients were still on sorafenib while the remaining patients required permanent cessation of sorafenib due to radiological progression (28.2%), adverse events (41%), and clinical deterioration/deterioration of Eastern Cooperative Oncology Group performance status (10.3%), respectively.
Discussion
Data from the SHARP trial shows that 86 patients (38%; n = 226) stopped the drug due to adverse events and this percentage population contributed to a greater extent as a reason for cessation of the drug than disease progression itself.[3] The corresponding proportion in the Asia Pacific trial was 19.5%, with 30.9% of patients requiring dose reduction.[2] However, a larger proportion of patients seems to stop the drug in the real world. The well-conducted SOFIA study from Italy, comprising 296 nontrial patients, had 40% of patients stopping sorafenib due to significant adverse events; a further 16% required cessation due to deterioration of liver function, without actual progression.[4]
The focus of this small study was to identify how consecutive Indian patients tolerated sorafenib in the real-world setting. As opposed to carefully selected patients in trials, patients treated in clinical practice have a higher incidence of comorbidities such as hypertension and diabetes mellitus, less stringent monitoring as well as issues of compliance. This is also seen in our series where 25.6%, 15.4%, and 28.2% of patients had evidence of hypertension, diabetes mellitus, and established cirrhosis. Potentially, these patients would require constant monitoring while on sorafenib, with a careful watch out for dose modifications of sorafenib and concomitant medications, as well as deterioration of HCC and comorbidity status.
43.6% of patients in this series had a nonhepatitis B/hepatitis C and nonalcohol-related etiology of HCC. Whether this is related to an undiagnosed or underdiagnosed underlying nonalcoholic fatty liver disease needs to be investigated further in the Indian setup, where cardiovascular risk factors and diseases have a high incidence and prevalence.[5]
Within the confines of this small series, we were able to identify the clinically relevant side effects seen in Indian patients. We noted a very high incidence of liver dysfunction (38.5%) and HFSR (25.6%), in our patients as compared to published data. This leads further credence to the role of certain polymorphisms in vascular endothelial growth factor receptors causing higher incidences of HFSR.[6] The prophylactic role of urea-based creams in reducing the incidence of HFSR as well as improving the quality of life may need wider application in our setup to reduce the distress to patients due to this side effect.[7]
The markedly high incidence of Grade 3 and Grade 4 liver dysfunction in this series is unexpected although the small sample size is a major confounding factor. Per se, reported literature from large studies shows <1% incidence of severe liver dysfunction with sorafenib in HCC.[8] Whether this is due to separate polymorphisms in cytochrome P450 3A4, the use of concomitant medications including unidentified over the counter supplements, or more rapid deterioration of disease status needs evaluation in a much larger cohort of Indian patients. Another factor that may play a role in such high incidences of hepatic dysfunction is the fact that a number of patients have received prior LDT (resulting in potential cumulative liver insults) in this study.
The high incidences of HFSR and liver dysfunction, along with fatigue were the major reasons for dose reductions required in our patients (43.6%). More importantly, 38.5% of our patients required interruption or cessation of sorafenib in the initial 4 months of treatment, and further, 41% required permanent cessation due to intolerable side effects. This percentage constitutes a significant proportion of patients who are unable to tolerate the initial standard recommended dose of 800 mg/day. While evidence for starting treatment at a lower dose in a select group of patients does not exist, there is some evidence that patients who are exposed to sorafenib for longer periods, although at lower doses, do better than patients who are unable to receive the drug for longer durations. This is based on post hoc analysis of the SOFIA study, where an increase in survival was seen in patients who received a half-dose of sorafenib for more than 70% of the treatment period compared with patients who received either full-dose or half-dose of sorafenib for <70% of the treatment period (21.6 vs. 9.6 months).[4] This also makes the case for ensuring compliance and continuing sorafenib even at lower doses, if tolerance is an issue.
The assessment of survival outcomes was not one of the primary end-points of this study, due to the short planned follow-up. However, the median event free survival of 4.2 months is on par with published data and is a reinforcement of sorafenib being the current standard of treatment in unresectable HCC not feasible for LDTs.
Conclusion
Monitoring of Indian patients while on sorafenib for HCC is important due to the higher incidence of adverse events seen. There is a higher incidence of liver dysfunction and HFSR in Indian patients than seen with published data from other countries. A significant proportion of patients required cessation of sorafenib due to adverse events in our series. Despite the adverse event profile, EFS remains on par with that seen in larger studies with sorafenib in advanced HCC.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Wilhelm S, Carter C, Lynch M, Lowinger T, Dumas J, Smith RA, et al. Discovery and development of sorafenib: A multikinase inhibitor for treating cancer. Nat Rev Drug Discov. 2006;5:835–44. doi: 10.1038/nrd2130. [DOI] [PubMed] [Google Scholar]
- 2.Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25–34. doi: 10.1016/S1470-2045(08)70285-7. [DOI] [PubMed] [Google Scholar]
- 3.Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–90. doi: 10.1056/NEJMoa0708857. [DOI] [PubMed] [Google Scholar]
- 4.Iavarone M, Cabibbo G, Piscaglia F, Zavaglia C, Grieco A, Villa E, et al. Field-practice study of sorafenib therapy for hepatocellular carcinoma: A prospective multicenter study in Italy. Hepatology. 2011;54:2055–63. doi: 10.1002/hep.24644. [DOI] [PubMed] [Google Scholar]
- 5.Gupta S, Gudapati R, Gaurav K, Bhise M. Emerging risk factors for cardiovascular diseases: Indian context. Indian J Endocrinol Metab. 2013;17:806–14. doi: 10.4103/2230-8210.117212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Qin C, Cao Q, Li P, Wang S, Wang J, Wang M, et al. The influence of genetic variants of sorafenib on clinical outcomes and toxic effects in patients with advanced renal cell carcinoma. Sci Rep. 2016;6:20089. doi: 10.1038/srep20089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ren Z, Zhu K, Kang H, Lu M, Qu Z, Lu L, et al. Randomized controlled trial of the prophylactic effect of urea-based cream on sorafenib-associated hand-foot skin reactions in patients with advanced hepatocellular carcinoma. J Clin Oncol. 2015;33:894–900. doi: 10.1200/JCO.2013.52.9651. [DOI] [PubMed] [Google Scholar]
- 8.Van Hootegem A, Verslype C, Van Steenbergen W. Sorafenib-induced liver failure: A case report and review of the literature. Case Reports Hepatol. 2011;2011:941395. doi: 10.1155/2011/941395. [DOI] [PMC free article] [PubMed] [Google Scholar]