

Abstract
Introduction:
Odontogenic tumors (OTs) are a group of heterogeneous lesions derived from epithelial or ectomesenchymal tissues or both, which are part of the tooth-forming apparatus. They range from hamartomatous or nonneoplastic tissue proliferations to malignant neoplasms with metastatic capacity. OTs are comparatively rare, comprising about 4.79% of all oral and maxillofacial biopsy specimens diagnosed. Several retrospective studies carried out in Africa, Asia, Europe and America, show that differences exist in the relative frequency of the various histologic types. Very few studies are reported among Asians, especially from the Indian subcontinent. Hence, the present study is designed to determine the frequency of the OTs and compare them with reports of various other part of the world.
Study Design:
A retrospective study was carried out with the ethical clearance and permission from the authority. The histopathology records from the Department of Oral Pathology and Microbiology, within the period from January 1992 to June 2012 were obtained. A total number of OTs were analyzed for age, gender, site of the tumor and histopathological type. The odontogenic keratocyst now considered as kerato cysticodontogenic tumor (KCOT) was also included in the present study.
Results
Totally, 2652 tissue specimens were received for histopathologic examination out of which 127 were OTs. All these reported cases were benign except two cases of malignancy. Among these male: female ratio of 1.04:1 with an overall mandible: maxilla ratio of 1.01:1. The most common benign odontogenic tumor was KCOT (44.9%). Ameloblastomas were the second most common benign tumors (35.43%), followed by odontome (7.08%) and adenomatoid odontogenic tumor (4.72%). Age distribution showed a peak occurrence of the odontogenic tumor in the fourth decade (31.49%).
Conclusion:
OTs are rare lesions in the studied population and are represented mainly by the KCOT, ameloblastoma and odontoma. Data from the reviewed cases have shown a possible geographic variation of OTs. With the introduction of the KCOT in the 2005 WHO classification, this neoplasm is now one of the most prevalent OT types.
Keywords: Ameloblastoma, odontogenic keratocyst, odontogenic tumors
INTRODUCTION
Odontogenic tumors (OTs) are a rare group of lesions, found exclusively within the maxillofacial region that present heterogeneous behavior, ranging from hamartomatous tissue proliferation to malignant neoplasms with metastatic capacity.[1,2] OTs are derived from epithelial, ectomesenchymal or mesenchymal elements that are, or have been, part of the tooth-forming apparatus, and can occur intraosseously within the maxillofacial skeleton or extraosseously (peripherally) in the tooth-bearing mucosa.[3,4] Data from the literature show differences in the relative frequencies of these tumors.[3,5]
World health organization (WHO) published the first edition of the “Histological Typing of Odontogenic Tumors” in 1971, then the second edition in 1992. The latter has been widely cited ever since when reporting large series or isolated cases of OTs. However, because of the diversity of OTs, there are still many controversies to be addressed concerning classification, terminology and diagnosis of these lesions. In 2005, the third edition of WHO histological typing of OTs was published in which definitions of some pathological entities have been changed, and some new ones have been introduced.
These tumors range from hamartomatous or nonneoplastic tissue proliferations to malignant neoplasms with metastatic capacity. In humans, tumors of the odontogenic tissues are comparatively rare, comprising about 1% of all oral and maxillofacial biopsy specimens. Knowledge of prevalence of various types of OTs and their clinical characteristics can be extremely valuable both for pathologists and clinicians when developing a differential diagnosis and may lead to clues concerning the causes of these lesions.
Reports on the relative frequency of OTs from different parts of the world, covering different ethnic groups have been documented. Available literature on the relative frequency of OT is mostly among Americans and Africans. Very few studies are reported among Asians, especially from the Indian subcontinent. The aim of the present study is to determine the epidemiology and clinicopathologic presentation of this heterogeneous group of lesions seen at our institute over the period of January 1992 to June 2012 and to compare these data with previous reports.
MATERIALS AND METHODS
A retrospective study was carried out with the ethical clearance and permission from authorities. The pathology records of the Department of Oral Pathology and Microbiology were reviewed retrospectively for all of the lesions of the oral cavity and jaws seen from January 1992 to June 2012. A total of 127 lesions were classified as intraosseous OTs with the inclusion of KCOT during this period. All cases were analyzed for age, gender, site of tumor and histopathologic typing.
Statistical analysis was carried out and determination of the incidence of OTs according to their histopathological type and of male: female ratio in various OTs was also done.
RESULTS
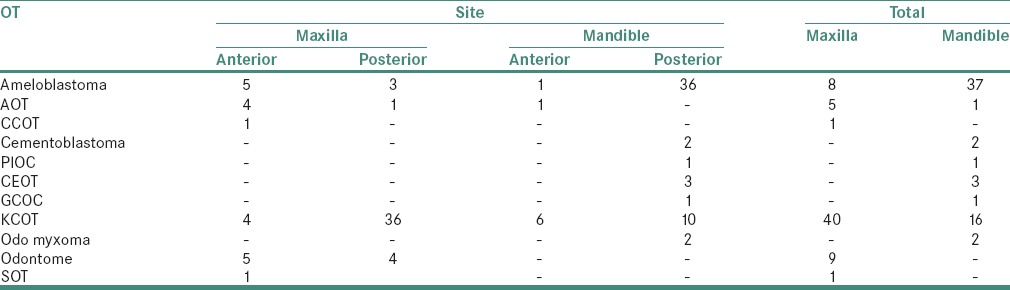
Retrospective study showed that among 2652 specimens received at the department of oral pathology Aurangabad, 127 were OT [Figures 1 and 2]. Age distribution showed a peak occurrence of the OT in the fourth decade (31.49%). 25.19% of the cases occurred in the third decades. KCOT was the most common tumor in the study and showed 32.14% cases in the third decade. Ameloblastoma, the second most common tumor in this study showed 35.5% of the cases occurring in the fourth decades. Odontomes showed peak occurrence in second decade with 88.8% cases while AOTs showed a peak occurrence in the third and fourth decade, with 33.3% cases [Figure 3]. Among 127 OT, 65 cases were in males and 62 in females, with a male: female ratio of 1.04:1 [Figure 4 and Table 1]. All these reported cases were benign except 2 cases one of which was of ghost cell odontogenic carcinoma and another was of primary intraosseous squamous cell carcinoma [Figure 5]. Most common benign OT was KCOT comprising of (44.9%). Ameloblastomas were the second most common benign tumors (35.43%), followed by odontome (7.08%) and adenomatoid odontogenic tumor (4.72%) [Table 2 and Figure 6]. In these reported cases 63 tumors were encountered in the mandible and 64 in the maxilla, with an overall mandible: maxilla ratio of 1.01:1 [Figure 7 and Table 3]. The maxilla and mandible were affected almost equally by most of OT. KCOT showed high predilection for maxilla (71.42%) with more common involvement of posterior part of maxilla (53.58%). Ameloblastoma showed a very high predilection for the mandible with 82.22% of the cases occurring in the mandiblewith posterior mandible, i.e., body and ramus part involvement in (71.11%). AOT and odontome both showed high predilection for maxilla 83.33% and 100%, respectively. Both of the lesions showed anterior maxillary involvement in 80% and 55.55% cases, respective.
Figure 1.
Diagrammatic presentation of incidence of odontogenic tumors in all reported cases at institute
Figure 2.
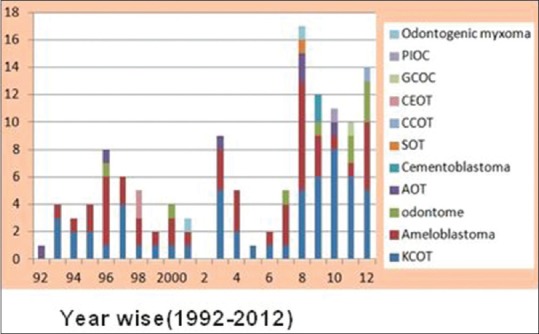
Diagrammatic presentation of year wise distribution of odontogenic tumors
Figure 3.
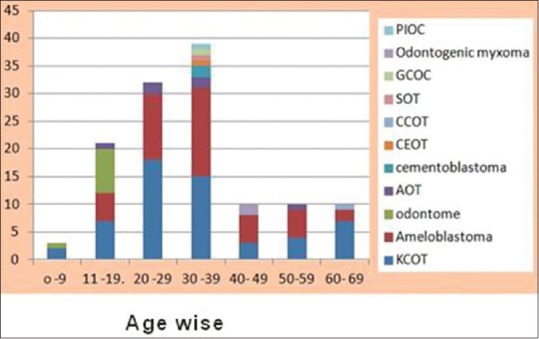
Diagrammatic presentation of age wise distribution of odontogenic tumors
Figure 4.
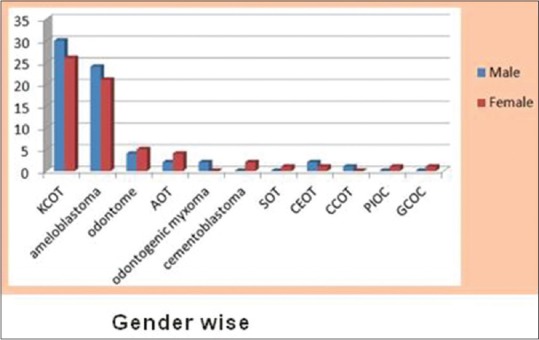
Diagrammatic presentation of gender wise distribution of odontogenic tumors
Table 1.
Gender-wise distribution of odontogenic tumors
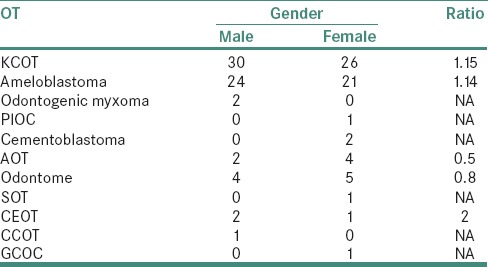
Figure 5.
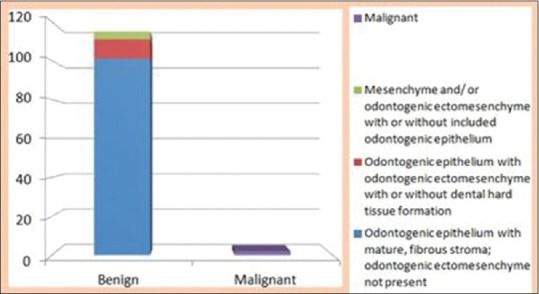
Diagrammatic presentation of odontogenic tumors depending on their nature
Table 2.
Odontogenic tumors depending on their histological type
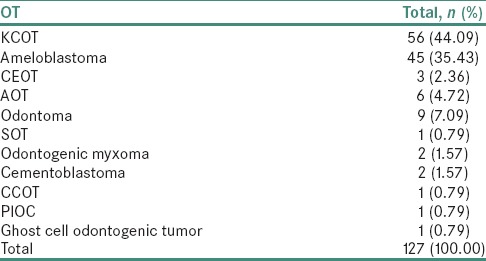
Figure 6.
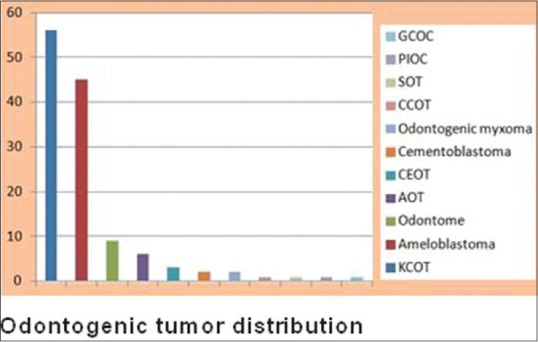
Diagrammatic presentation of odontogenic tumors depending on their histological type
Figure 7.
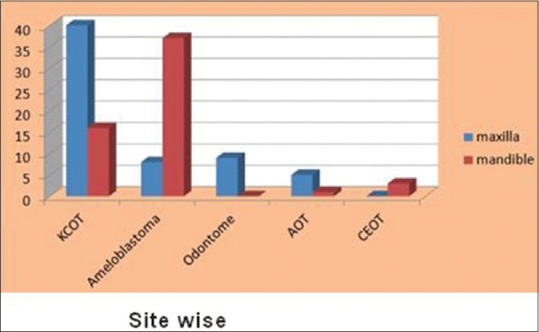
Diagrammatic presentation of odontogenic tumors depending on their occurrence at anatomical site
Table 3.
Odontogenic tumors depending upon their occurrence at anatomical site
DISCUSSION
Few reports have been published in the English language literature using the 2005 WHO classification of OTs.
According to the 1992 WHO classification, reports from the Americas, including the United States, Mexico, Chile and Brazil, have shown odontoma as the most common OT, representing 45% to 75% of all OTs. Reports from China, Nigeria, India, Sri Lanka, United Republic of Tanzania and Istanbul have shown the ameloblastoma as the most frequent OT.[6,7]
However, this reported variation may be due to two reasons. Over-or under-reporting has a direct influence on this phenomenon. Moreover, most odontomes are discovered on routine radiograph and do not produce clinical symptoms. This may be responsible for the low incidence of odontomes observed in the Indian population because most patients in our environment do not seek medical consultation unless there are symptoms suggesting an obvious pathology. This geographic variation may also be due to genetic and/or environmental influences.[8]
Using the 2005 WHO classification of OTs, Reports from Fernandes in 2005 in Brazilian population and Luo and Li in 2009 from Chinese population showed that the Keratocystic odontogenic tumor (KCOT) as the most frequent OT, followed by the ameloblastoma and odontome. Results of our study were in consistent with the study by Luo and Li.[9,10]
OTs affected patients over a wide range of ages, with a median of 35 years, similar to data reported by Rafael et al.[6] and Jing et al.[11]
Data from the present study showed that KCOT was the most frequent OT, occurring mainly in the posterior region of the maxilla. This finding was similar to results of Servato et al.[12,13] Avelar et al. reported that ameloblastoma exhibits no gender predilection.[14] Controversially Fernandes et al. reported a slight female predilection, but in the present study both KCOT and ameloblastoma showed slight male predilection. Similar to other patient series, most cases occurred in the second, third and fourth decades of life.[9]
Of all ameloblastomas, 68% were solid multicystic ameloblastoma, 26.66% were of the unicystic type; while other studies reported different percentage like Rafael et al. reported 15% unicystic cases and Buchner et al. reported that 46% of ameloblastomas in their series were unicystic.[4,6]
Rafael et al. reviewed 3406 cases and indicated a preponderance of KCOTs in males (61.09%), and data from the present study show a slight male predilection of this neoplasm, being the most prevalent OT in females.[6] Geographic variation seems to influence the gender predilections of this OT. A report from Japan, with 183 cases of KCOTs, found no gender predilection, with a male: female ratio of 1.05:1.00. As reported in the literature, the posterior region of the mandible was the most affected site.
Several reported series have documented odontome as the most prevalent OT,[2,4,10] but data from the study by Rafael et al. 2011shown that odontome is the third most prevalent OT similar to Avelar et al. occurring mainly in the anterior region of the maxilla.[6,14]
Two cases of each, i.e., odontogenic myxoma, and cementoblastoma was found in the present study. Single cases of squamous OT and calcifying cystic odontogenic tumor each were the least frequent benign OTs in the present study.
There was most striking finding of the malignant OT in the present study, within this study we found 2 malignant OT. One was of primary intraosseous squamous cell carcinoma originating from KCOT and another case was of Ghost cell odontogenic carcinoma. According to Osterne Rafael et al. (2011) study malignant OTs accounted for only 3.84% of the 3406 OT.[6] Primary intraosseous squamous cell carcinoma (65 cases), followed by ameloblastic carcinoma (44 cases) were the most prevalent forms of malignant OT. Only 3 cases of ameloblastic fibrosarcoma were found within the 3406 OT. All malignant OT, with the exception of the clear cell odontogenic carcinoma, exhibited a male predilection. These data concerning malignant OTs emphasize the rarity of these lesions reported in literature.
CONCLUSION
OTs are rare lesions in the studied population and are represented mainly by the KCOT, ameloblastoma and odontoma. These neoplasms show clinicopathologic features that allow separation from other oral cavity lesions. OTs exhibits a female preponderance, and most cases are diagnosed in the second to fourth decades of life. Data from the reviewed cases have shown a possible geographic variation of OTs. With the introduction of the KCOT in the 2005 WHO classification, this neoplasm is now one of the most prevalent OT types.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Philipsen HP, Reichart PA. Revision of the 1992-edition of the WHO histological typing of odontogenic tumours. A suggestion. J Oral Pathol Med. 2002;31:253–8. doi: 10.1034/j.1600-0714.2002.310501.x. [DOI] [PubMed] [Google Scholar]
- 2.Mosqueda-Taylor A. New findings and controversies in odontogenic tumors. Med Oral Patol Oral Cir Bucal. 2008;13:E555–8. [PubMed] [Google Scholar]
- 3.Barnes L, Eveson JW, Reichart P, Sidransky D, editors. World Health Organization classification of tumours. Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Publishing Group; 2005. [Google Scholar]
- 4.Buchner A, Merrell PW, Carpenter WM. Relative frequency of central odontogenic tumors: A study of 1,088 cases from Northern California and comparison to studies from other parts of the world. J Oral Maxillofac Surg. 2006;64:1343–52. doi: 10.1016/j.joms.2006.05.019. [DOI] [PubMed] [Google Scholar]
- 5.Sriram G, Shetty RP. Odontogenic tumors: A study of 250 cases in an Indian teaching hospital. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:e14–21. doi: 10.1016/j.tripleo.2008.02.021. [DOI] [PubMed] [Google Scholar]
- 6.Osterne RL, Brito RG, Alves AP, Cavalcante RB, Sousa FB. Odontogenic tumors: A 5-year retrospective study in a Brazilian population and analysis of 3406 cases reported in the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111:474–81. doi: 10.1016/j.tripleo.2010.10.018. [DOI] [PubMed] [Google Scholar]
- 7.Tawfik MA, Zyada MM. Odontogenic tumors in Dakahlia, Egypt: Analysis of 82 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e67–73. doi: 10.1016/j.tripleo.2009.09.003. [DOI] [PubMed] [Google Scholar]
- 8.Ochsenius G, Ortega A, Godoy L, Peñafiel C, Escobar E. Odontogenic tumors in Chile: A study of 362 cases. J Oral Pathol Med. 2002;31:415–20. doi: 10.1034/j.1600-0714.2002.00073.x. [DOI] [PubMed] [Google Scholar]
- 9.Fernandes AM, Duarte EC, Pimenta FJ, Souza LN, Santos VR, Mesquita RA, et al. Odontogenic tumors: A study of 340 cases in a Brazilian population. J Oral Pathol Med. 2005;34:583–7. doi: 10.1111/j.1600-0714.2005.00357.x. [DOI] [PubMed] [Google Scholar]
- 10.Luo HY, Li TJ. Odontogenic tumors: A study of 1309 cases in a Chinese population. Oral Oncol. 2009;45:706–11. doi: 10.1016/j.oraloncology.2008.11.001. [DOI] [PubMed] [Google Scholar]
- 11.Santos JN, Pinto LP, de Figueredo CR, de Souza LB. Odontogenic tumors: Analysis of 127 cases. Pesqui Odontol Bras. 2001;15:308–13. doi: 10.1590/s1517-74912001000400007. [DOI] [PubMed] [Google Scholar]
- 12.Servato JP, de Souza PE, Horta MC, Ribeiro DC, de Aguiar MC, de Faria PR, et al. Odontogenic tumours in children and adolescents: A collaborative study of 431 cases. Int J Oral Maxillofac Surg. 2012;41:768–73. doi: 10.1016/j.ijom.2012.02.021. [DOI] [PubMed] [Google Scholar]
- 13.Servato JP, Prieto-Oliveira P, de Faria PR, Loyola AM, Cardoso SV. Odontogenic tumours: 240 cases diagnosed over 31 years at a Brazilian university and a review of international literature. Int J Oral Maxillofac Surg. 2013;42:288–93. doi: 10.1016/j.ijom.2012.05.008. [DOI] [PubMed] [Google Scholar]
- 14.Avelar RL, Antunes AA, Santos Tde S, Andrade ES, Dourado E. Odontogenic tumors: Clinical and pathology study of 238 cases. Braz J Otorhinolaryngol. 2008;74:668–73. doi: 10.1016/S1808-8694(15)31375-6. [DOI] [PMC free article] [PubMed] [Google Scholar]