

Summary
We previously demonstrated the safety and effectiveness of a nonadmission-based model for TIA care (Monash TIA Triaging Treatment [M3T]). In this microcosting study, we used a pre–post cohort design with multivariable uncertainty analyses to compare actual resource utilization costs between M3T (years 2004–2007) and the previous admission-based model (2003). Average total episode costs per patient were significantly less for M3T (Australian dollars [AUD] 1,927.00, 95% confidence interval [CI] AUD 1,829.00–1,037.00) compared with the admission-based model (AUD 4,841.00, 95% CI AUD 4,178.00–5,590.00). Nonadmission care in M3T was substantially cost-saving with a median 3 (95% uncertainty interval 0.7–6.0) additional strokes averted per 100 patients treated, based on an observed 90-day stroke rate of 1.50% (95% CI 0.73%–3.05%) and 4.67% (95% CI 2.28%–9.32%) in the admission-based model.
TIA requires urgent treatment.1 A recent nationwide analysis of TIA care in the United States indicated 70% of patients were admitted for 2–6 days with average hospitalization charges of $17,000 USD per patient.2 However, rapid outpatient-based TIA management is safe and associated with low 90-day stroke rates (1%–3%).1,3–5 We have shown that a structured model of outpatient care, the Monash TIA Triaging Treatment (M3T) pathway, is safe and effective compared with a previous admission-based model.3 It is important to know whether such nonadmission models provide a cost advantage.
Simulated costing models of hospitalization for TIA provide inconclusive results on this issue.6,7 Few clinical studies provide cost estimates of individual aspects of TIA care.8–11 In the EXPRESS study, although an urgent walk-in TIA clinic was associated with fewer hospital bed costs compared with a nonurgent outpatient clinic, actual clinic costs were not compared.8 A Spanish study performed using composite hospital data found increased costs for hospitalization compared with a TIA clinic, but investigation costs were not measured.10 There are no cost-effectiveness studies of outpatient TIA care using more precise bottom-up microcosting based on comprehensive patient-level resource use.12 We conducted a microcosting economic evaluation of M3T compared with the previous model of routine hospital admission, hypothesizing that M3T would be cost-effective.
METHODS
M3T
M3T was implemented at Monash Medical Centre, a tertiary hospital catering to 23% of Melbourne's population (931,500 residents) in Australia. The protocol and safety of the M3T pathway have been reported.3 In M3T, all patients presenting to the emergency department (ED) with suspected TIA receive urgent CT brain imaging, ECG, and essential blood tests. Those with crescendo/recurrent TIA, persistent symptoms, other acute illness, or who live alone with no social support are admitted. Otherwise, if CT excludes hemorrhage, antiplatelet/anticoagulant therapy is commenced in the ED and patients are discharged. Carotid ultrasound is performed on an outpatient basis within 24 hours. Patients are then triaged and prioritized to attend a TIA clinic based on the underlying vascular mechanism. In the previous model of care, most patients were routinely admitted.
Sample, definitions, and resource use data
The study design is a sequential nonrandomized cohort comparison. The primary sample consisted of all patients presenting to the ED between May 2004 and December 2007 with symptoms suggestive of TIA irrespective of age, blood pressure, clinical features, duration of TIA, and presence of diabetes (ABCD2) score or final diagnosis, and managed in M3T.3 The comparison sample consisted of all patients presenting to the ED between January 2003 and January 2004 prior to M3T, who were assigned an ICD-10–Australian Modification (AM) TIA code (G45.8, G45.9).13 TIA diagnoses were confirmed by a stroke neurologist, defined as acute loss of focal cerebral or monocular function with symptoms lasting ⩽24 hours due to inadequate cerebral or ocular blood supply as a result of arterial thrombosis or embolism.14 Stroke was defined as per the WHO15 and 90-day stroke outcome determined by a combination of clinic assessment, telephone questionnaire, and medical record reviews. Details of all treatments and investigations (pathology, radiology, cardiac, EEG) from presentation, admission (if applicable), and clinic review were obtained from medical records and hospital databases. All TIA clinic attendances were established from the clinic booking database.
Cost data and outcomes
We used the common reference year of 2012 for the costs associated with each resource use item. All costs are presented in Australian dollars (AUD) and evaluated from the perspective of a health service provider.
Bed costs
Unit costs were obtained from the hospital finance department. These ranged from AUD 400 to 1,100 depending on duration of stay, and are inclusive for staffing, administration, and overheads.
Investigation costs
Each investigation was assigned the corresponding standard unit price from the 2012 Medicare Benefit Schedule16 of the Australian government.
Clinic costs
M3T clinics were conducted by stroke neurologists with 45 minutes allocated for a new consultation and 20 minutes for reviews. The unit cost of a clinic session (3.5 hours) includes room rent and salaries for neurologists, receptionists, and typists. In 2003, 2 clinics were conducted/week, and when M3T commenced, a third clinic was added along with an additional administrative session (doctor salary only) to facilitate rapid review of investigations, a cornerstone of M3T. Clinic costs were estimated as a proportion of the total session costs based on duration of appointment (e.g., 45-minute consultation = total session cost/3.5 hours × 45 minutes). Using this method, we established unit clinic costs of AUD 175.78 for an initial consultation and AUD 78.12 for review.
Economic outcomes
The primary outcome was the net difference in total average episode costs per patient between the admission-based model and M3T. An episode was defined as the initial ED presentation or hospitalization plus clinic attendance. Any clinic visit beyond 90 days up to 2 review consultations was also included in the episode cost estimation to fully capture the added financial implications of a clinic-based service. The costs of an episode were summed for each individual patient based on actual resource use. A negative dollar value was used to present cost savings for M3T compared with the admission-based model. A secondary outcome was to determine the cost-effectiveness of M3T compared with the admission-based model in terms of the net difference in costs per additional stroke averted. Our willingness-to-pay threshold of cost-effectiveness was a difference of AUD ⩽50,000 per stroke averted.17 Since costs and outcome beyond 3 months were not considered, discounting was unnecessary.
Statistical methods
Differences in total average per episode patient costs were calculated and 95% confidence intervals (CIs) around the average costs were produced using bias-corrected nonparametric bootstrapping over 10,000 iterations. The study was powered at 90% (α 0.05) to detect a minimum difference in per episode costs of AUD 825 between the 2 models. These analyses were performed using Stata (version 11.0, Stata Corporation, TX).
For cost-effectiveness analyses, univariable and multivariable uncertainty analyses were undertaken by varying the bed and clinic cost inputs over a normal distribution with a SD of 10% (e-Methods at Neurology.org/cp). The proportion of stroke-free patients per 100 patients treated was simulated using a triangular distribution of the CI of the observed proportions for the minimum and maximum values. All uncertainty analyses were performed using Monte Carlo simulation over 10,000 iterations and results described as means and 95% uncertainty intervals (UIs). The cost difference per episode was plotted against number of strokes averted on a cost-effectiveness scatterplot. When the majority of plotted points fall in the southeast quadrant, the model is more effective and less expensive, and considered dominant (cost-saving). When they fall in the northeast quadrant, the model is more effective but also more expensive, and may be considered cost-effective depending on the chosen willingness-to-pay threshold. Uncertainty simulations were conducted using @Risk software (version 5.0, Palisade Corporation, Ithaca, NY).
Alternate scenario analyses
We evaluated 3 alternate scenarios by varying either level of resource use or length of stay based on mandatory admission. First, we simulated an increase in radiologic and cardiac tests in M3T based on data from other rapid evaluation TIA systems.4,18 We also simulated 2 scenarios to show the effect of mandatory admission for our hospital, as in previous modeling analyses.6,7 This was achieved by assigning unit bed costs to all nonadmitted M3T patients for a simulated 48- or 24-hour admission. All comparisons were based on 160 annual presentations with suspected TIA to our hospital, and simulated proportions were drawn from a triangular distribution. All uncertainty and scenario analyses were conducted using @Risk software.
Standard protocol approvals, registrations, and patient consents
The Southern Health (Hospital) and Monash University Human Research Ethics Committees approved this study.
RESULTS
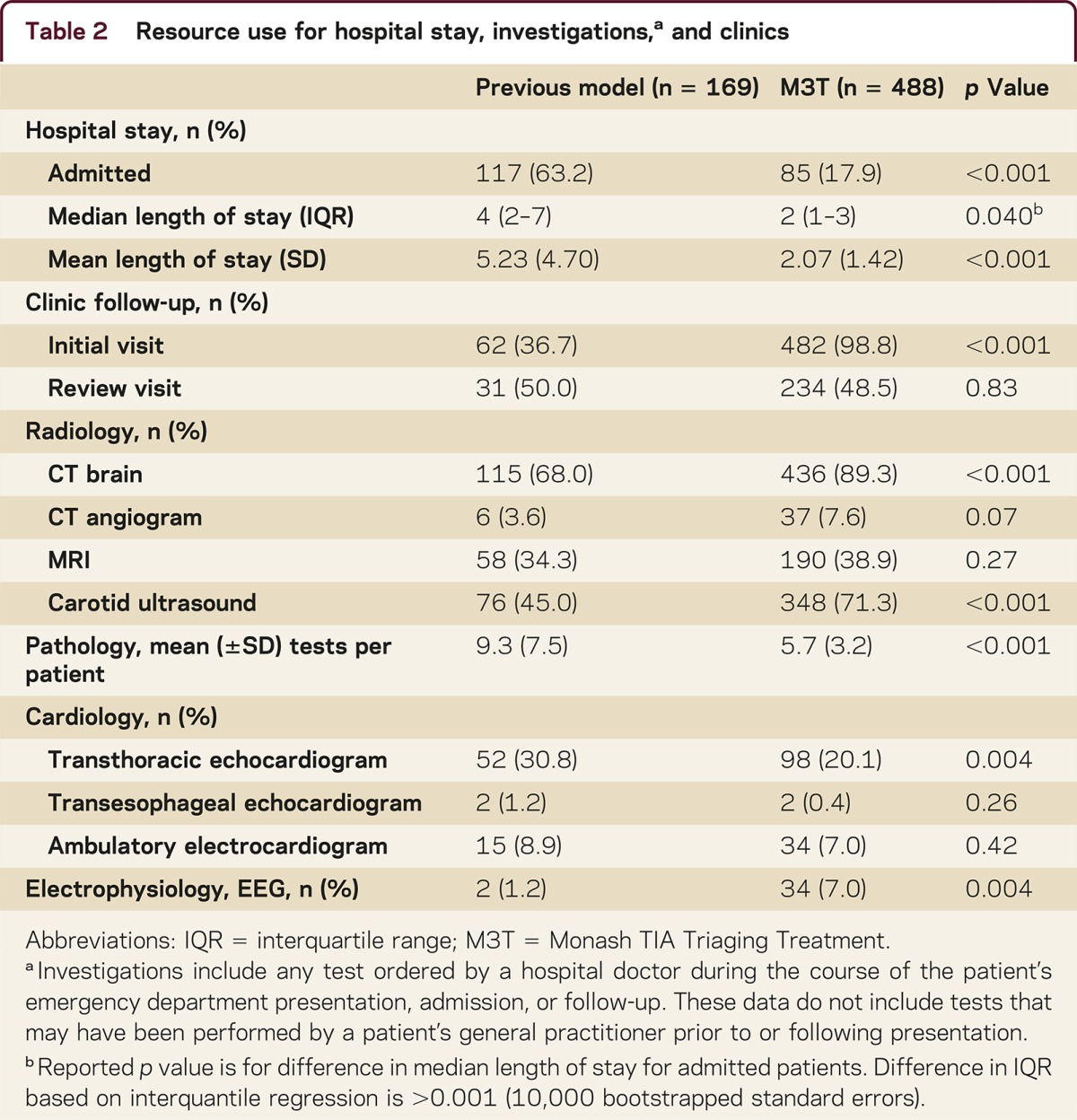
We treated 488 patients in M3T between 2004 and 2007 and 169 patients with the previous model in 2003 (table 1). Resource use is summarized in table 2. Admission occurred for 85/488 (17.4%) in M3T and 117/169 (62.9%) in the previous model. Mean length of stay during initial admission was 2.07 days (SD 1.42) for M3T and 5.23 days (SD 4.70) for the previous model. Compared with the previous model, more M3T patients attended clinics (p < 0.001), underwent CT brain (p < 0.001), carotid ultrasound (p < 0.001), and EEG (p = 0.004), but fewer underwent transthoracic echocardiography (p = 0.004). Overall, the mean number of blood tests per patient episode was less in M3T (p < 0.001). With near complete follow-up (94%), there were 7 stroke events within 90 days in each cohort (M3T: 7/488, 1.50% [0.73%–3.05%], previous model: 7/169, 4.67% [2.28%–9.32%], p = 0.03).
Table 1 Comparison of patient characteristics between M3T and the previous admission-based model
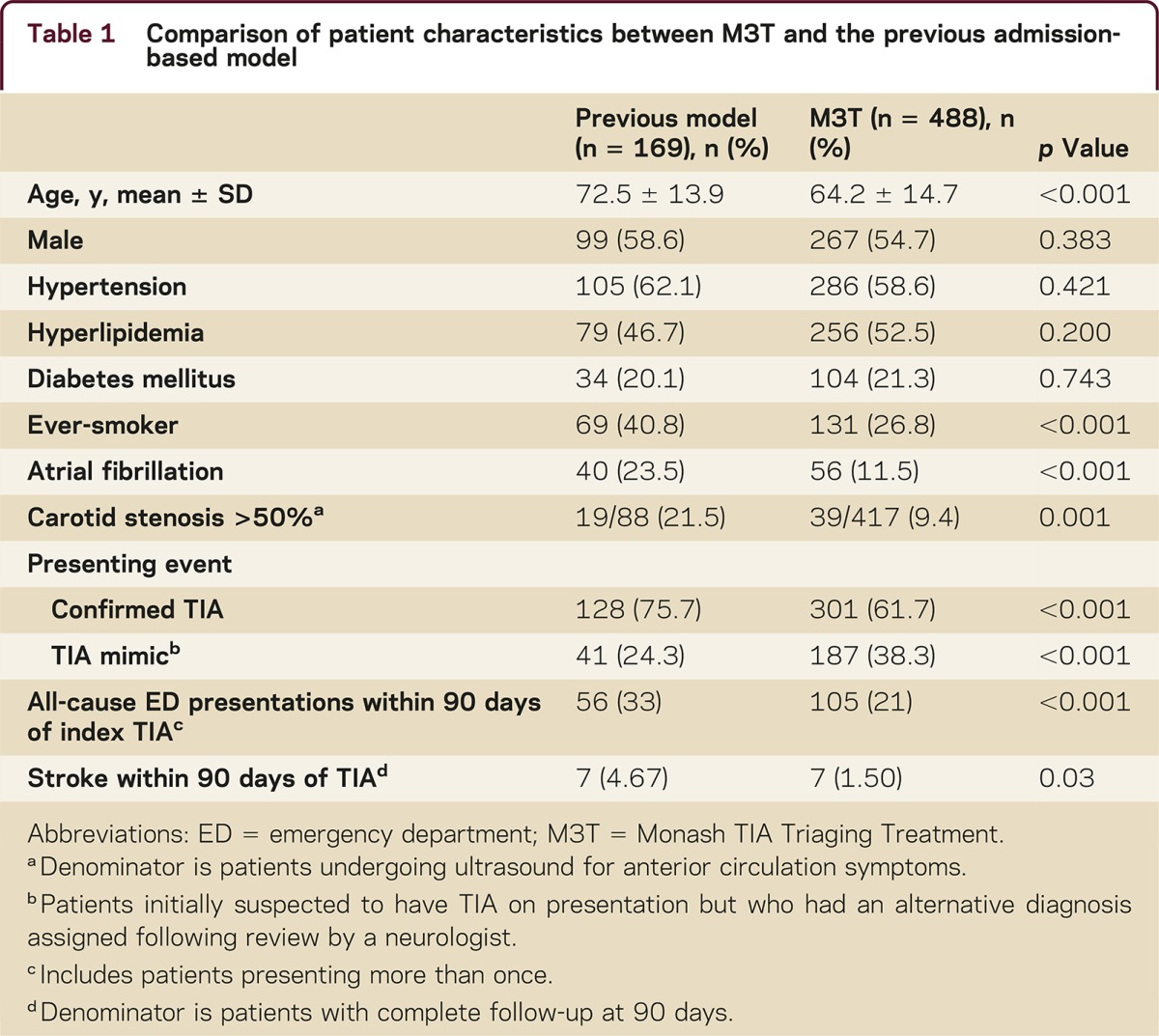
Table 2 Resource use for hospital stay, investigations,a and clinics
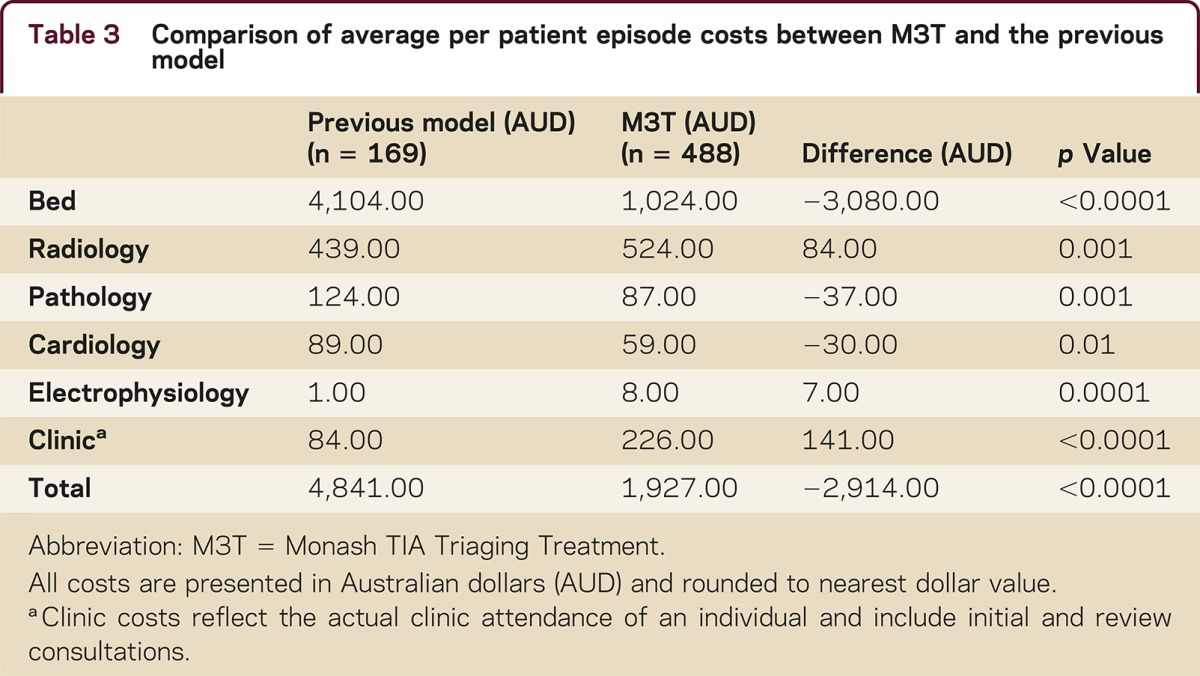
The average per patient episode cost was AUD 1,927.00 (95% CI AUD 1,828.00–2,037.00) in M3T compared with AUD 4,841.00 (95% CI AUD 4,178.00–5,590.00) in the previous model (p < 0.001). Categorized costs are presented in table 3. Bed costs were the greatest contributor of total costs in both models. Average annual clinic costs doubled from AUD 14,258.00 in 2003 to AUD 28,134.00 per annum from 2004 onwards in M3T (p < 0.001). This increase was offset by the significant reduction in average annual bed costs, which was AUD 240,142.00 in M3T, an average annual saving of AUD 578,069.00 compared with the previous model. Uncertainty analyses indicated that the difference in per patient episode costs may range between AUD –3,507.00 and AUD –2,300.00 (table e-1). The cost-effectiveness scatterplot for episode costs are presented in the figure. The majority (99.7%) of plotted points fell within the cost-saving quadrant in favor of M3T. M3T resulted in a median additional 3 (95% UI 0.7–6.0) strokes averted per 100 patients treated compared with the previous model of care.
Table 3 Comparison of average per patient episode costs between M3T and the previous model

Cost-effectiveness scatterplot of M3T compared with the previous model
Figure. The cost-effectiveness scatterplot is presented using Monte Carlo simulation over 10,000 iterations. Location of the plotted points is interpreted as follows with regard to the new model (Monash TIA Triaging Treatment [M3T]): (1) (northeast quadrant)—more effective, more expensive; (2) (northwest quadrant)—less effective, more expensive; (3) (southwest quadrant)—less effective, more expensive; (4) (southeast quadrant)—more effective, less expensive (cost-saving). * The blue diagonal line indicates the willingness-to-pay threshold of AUD 50,000 per strokes averted. Points falling below the line are considered cost-effective.
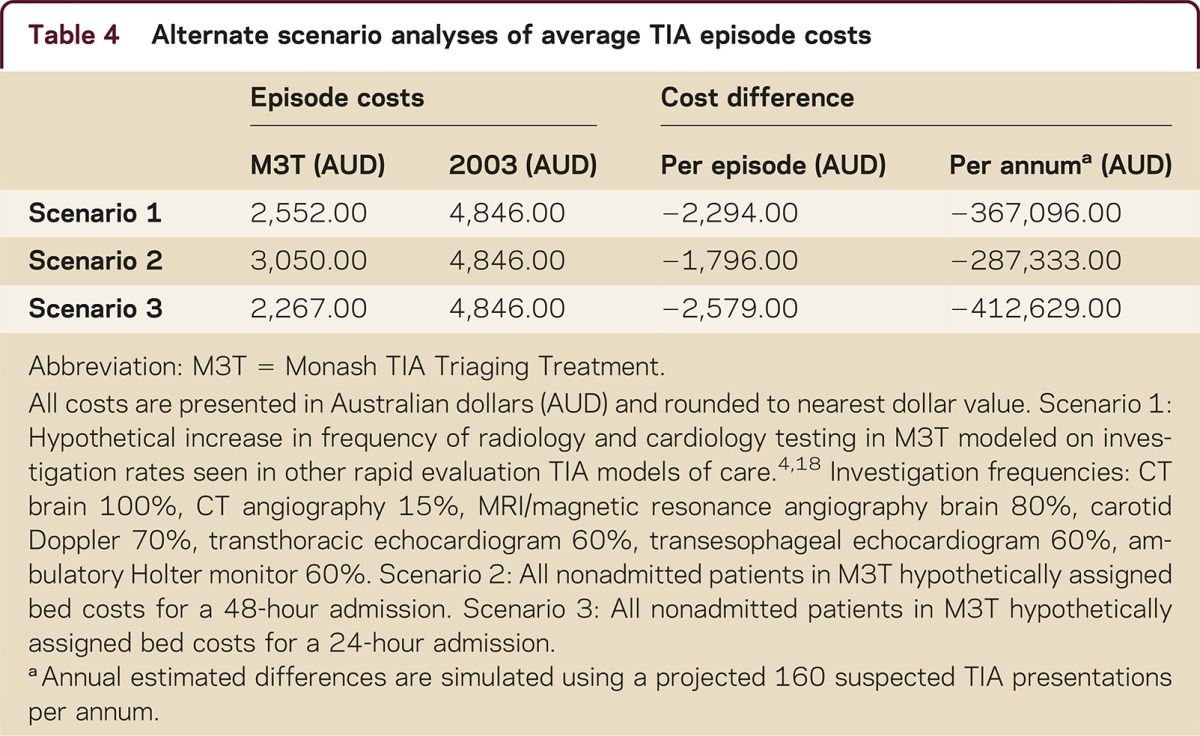
Alternate scenario analyses are presented in table 4. Increasing investigation resource use in M3T or mandatory brief admission increased its costs although cost-savings remained overall. Mandatory 48-hour or 24-hour admission would have increased total annual costs for M3T by approximately AUD 180,000 and AUD 55,000, respectively.
Table 4 Alternate scenario analyses of average TIA episode costs
DISCUSSION
We present a comprehensive microcosting study evaluating the cost-effectiveness of a nonadmission-based TIA model of care. Such a model is substantially cost-saving compared with routine hospital admission while being safe in terms of number of strokes averted.
Although previous reports suggested that nonadmission-based care may be less expensive,9,10 our results confirm this based on comprehensive patient-level data. In phase 2 of the EXPRESS study,1 patients with suspected TIA deemed by their primary care physician to not require hospitalization were directly referred to a walk-in TIA clinic, leading to reduced hospital costs.8 However, clinic costs were not evaluated in EXPRESS. In another study,11 an ED-based rapid diagnostic protocol for TIA was associated with a saving of USD 657 per patient compared with inpatient care despite an extra 2 days of hospital admission in the latter. This may be an underestimate, given that the large difference in mean hospitalization charges for TIA in the United States between hospital admission for 24 hours (∼USD 10,000) and for 2 days (∼USD 17,000). Moreover, unlike M3T, costs of patient follow-up could not be estimated in that study. Importantly, in M3T, a net cost shift from inpatient to outpatient settings did not occur, and a true reduction in per-patient episode costs was achieved. We estimate that only 23 patients needed to be treated in M3T per annum to offset the extra weekly clinic costs, suggesting its feasibility even in hospitals with small caseloads.
It has been argued that hospitalization for TIA expedites investigations.19,20 In M3T, there was no difference in time to investigations or treatment between admitted and nonadmitted patients.3 Admission may be appropriate in smaller hospitals without neurologists or structured pathways. However, it is possible that structured nonadmission-based pathways could be modified to suit even nontertiary settings. Improved access to thrombolysis has also been advocated as a reason for hospitalization.6 In a simulation study, the 48-hour stroke rate needed to be at least 20% (an unlikely scenario in the current era of secondary prevention) before cost-effectiveness could be achieved by immediate provision of tissue plasminogen activator.7 In M3T, the proportion of patients with stroke within 2 days of TIA was only 0.85%, and admission for this period would have inflated annual hospital costs by AUD 180,000 without any additional clinical benefit.
In the United States, TIA care in ED observation units contributes substantially to growing health care costs.2 However, in a previous study, even with an accelerated ED observation unit, a median of 25.6 hours was required for investigations and treatment, and without any further provision for specialist follow-up.11 Compared with M3T, a 24-hour admission model may be marginally cheaper (by AUD 150 per patient), but only if no further specialist follow-up was required. Moreover, for this to be an effective model, all investigations (including complex diagnostic angiography), treatment, and specialist review would need to be complete within 24 hours prior to the patient leaving the ED. This raises several feasibility issues in countries with systems similar to Australia. In our unit, only 16% of MRI scans occurred within 48 hours (unpublished data, 2010). To date, there has been no evaluation of the safety of transfer of incomplete care to a primary care physician. Furthermore, Australian hospitals do not have specialists on-site 24/7. Admitted patients are predominantly managed by junior doctors (registrars) who are not on-site after hours and on weekends, but are called back only if necessary. Thus, a comprehensive 24-hour ED observation unit appears infeasible in an Australian or similar setting.
A major strength of our study is the bottom-up microcosting approach, in contrast to decision tree cost-modeling6,7 or admission-averted costing only.8 Microcosting allows greater exploration of results compared with top-down approaches, which often use average per diem costs according to patient diagnosis-related groups (DRG). The most frequently applied ICD-10-AM code for TIA (G45.9) is also assigned to patients experiencing vasospasm following a subarachnoid hemorrhage and the most representative DRG (B69 TIA and other precerebral occlusion) additionally includes other related diagnoses. This approach may underestimate outpatient costs and overestimate inpatient costs for TIA care. A limitation of our analysis is the use of a sequential study design rather than a parallel prospective cohort or randomized controlled trial design. An additional limitation is the imbalance in numbers and the differences between the 2 cohorts with regards to risk factors. Nevertheless, we have shown in our previously published evaluation of M3T that correcting for these imbalances still led to lower adjusted odds of stroke in M3T than in the prior model (odds ratio 0.46, 95% CI 0.12–1.68, p = 0.24).3 Although our comparison was over different time periods, we used standardized unit prices from 2012 to limit cohort effects and enhance generalizability. Our sensitivity analyses contribute to the wider applicability of our results, but with important caveats. Bed costs, clinical expertise, and funding were specific to our hospital, and may differ for other hospitals and countries. Actual cost estimates may also vary depending on whether more expensive tests such as MRI/magnetic resonance angiography or CT angiography are preferred, or if the proportion of TIA mimics needing attention increases. Our analysis may not be extrapolated to settings where TIA patients do not routinely present to the ED, such as in the EXPRESS study, in which primary care physicians select patients to refer directly to a clinic.1
STUDY FUNDING
No targeted funding reported.
DISCLOSURES
L.M. Sanders has received a NHMRC postgraduate research scholarship, Stroke Fellowship (2009) cofunded by the Stroke Unit (Monash Medical Centre) and Boehringer Ingelheim, and a Clinical Academic Fellowship jointly funded by Monash University and Monash Health. D.A. Cadilhac has received a NHMRC/Heart Foundation Career Development Fellowship. V.K. Srikanth has received a NHMRC/Heart Foundation Career Development Fellowship and serves on the editorial boards of International Journal of Stroke and Frontiers of Neurology. C.P. Chong reports no disclosures. T.G. Phan serves on the speakers' bureaus for and has received speaker honoraria from Bayer, Genzyme, and Boehringer Ingelheim and serves on a scientific advisory board for Genzyme. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.
Supplementary Material
Correspondence to: velandai.srikanth@monash.edu
Funding information and disclosures are provided at the end of the article. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.
Footnotes
Supplemental data at http://cp.neurology.org/lookup/suppl/doi:10.1212/CPJ.0000000000000095/-/DC1
Correspondence to: velandai.srikanth@monash.edu
Funding information and disclosures are provided at the end of the article. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.
REFERENCES
- 1.Rothwell PM, Giles MF, Chandratheva A. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370:1432–1442. doi: 10.1016/S0140-6736(07)61448-2. [DOI] [PubMed] [Google Scholar]
- 2.Qureshi AI, Adil MM, Zacharatos H, Suri MF. Factors associated with length of hospitalization in patients admitted with transient ischemic attack in United States. Stroke. 2013;44:1601–1605. doi: 10.1161/STROKEAHA.111.000590. [DOI] [PubMed] [Google Scholar]
- 3.Sanders LM, Srikanth VK, Jolley DJ. Monash transient ischemic attack triaging treatment: safety of a transient ischemic attack mechanism-based outpatient model of care. Stroke. 2012;43:2936–2941. doi: 10.1161/STROKEAHA.112.664060. [DOI] [PubMed] [Google Scholar]
- 4.Lavallee PC, Meseguer E, Abboud H. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6:953–960. doi: 10.1016/S1474-4422(07)70248-X. [DOI] [PubMed] [Google Scholar]
- 5.Olivot JM, Wolford C, Castle J. Two aces: transient ischemic attack work-up as outpatient assessment of clinical evaluation and safety. Stroke. 2011;42:1839–1843. doi: 10.1161/STROKEAHA.110.608380. [DOI] [PubMed] [Google Scholar]
- 6.Nguyen-Huynh MN, Johnston SC. Is hospitalization after TIA cost-effective on the basis of treatment with tPA? Neurology. 2005;65:1799–1801. doi: 10.1212/01.wnl.0000187067.93321.fa. [DOI] [PubMed] [Google Scholar]
- 7.Joshi JK, Ouyang B, Prabhakaran S. Should TIA patients be hospitalized or referred to a same-day clinic? A decision analysis. Neurology. 2011;77:2082–2088. doi: 10.1212/WNL.0b013e31823d763f. [DOI] [PubMed] [Google Scholar]
- 8.Luengo-Fernandez R, Gray AM, Rothwell PM. Effect of urgent treatment for transient ischaemic attack and minor stroke on disability and hospital costs (EXPRESS study): a prospective population-based sequential comparison. Lancet Neurol. 2009;8:235–243. doi: 10.1016/S1474-4422(09)70019-5. [DOI] [PubMed] [Google Scholar]
- 9.Teles de Araujo M, Canhao P. Cost study of transient ischemic attack patients in a transient ischemic attack clinic [in Portuguese] Acta Med Port. 2011;24:681–686. [PubMed] [Google Scholar]
- 10.Martinez-Martinez MM, Martínez-Sánchez P, Fuentes B. Transient ischaemic attacks clinics provide equivalent and more efficient care than early in-hospital assessment. Eur J Neurol. 2013;20:338–343. doi: 10.1111/j.1468-1331.2012.03858.x. [DOI] [PubMed] [Google Scholar]
- 11.Ross MA, Compton S, Medado P, Fitzgerald M, Kilanowski P, O'Neil BJ. An emergency department diagnostic protocol for patients with transient ischemic attack: a randomized controlled trial. Ann Emerg Med. 2007;50:109–119. doi: 10.1016/j.annemergmed.2007.03.008. [DOI] [PubMed] [Google Scholar]
- 12.Drummond MF, McGuire A. Economic Evaluation in Health Care: Merging Theory With Practice. New York: Oxford University Press; 2001:286.
- 13.National Centre for Classification of Health (Australia). The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM). Lidcombe, Australia: National Centre for Classification in Health; 2006.
- 14.Hankey G, Warlow C. Evolution of the concepts of TIAs. In: Hankey G, editor. Transient Ischaemic Attacks of the Brain and Eye. London: WB Saunders; 1994:1–9.
- 15.Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ. 1980;58:113–130. [PMC free article] [PubMed] [Google Scholar]
- 16.Medicare Benefits Schedule Book. Canberra: Australian Government Department of Health and Ageing; 2012.
- 17.Peacock SJ, Richardson JR, Carter R, Edwards D. Priority setting in health care using multi-attribute utility theory and programme budgeting and marginal analysis (PBMA) Soc Sci Med. 2007;64:897–910. doi: 10.1016/j.socscimed.2006.09.029. [DOI] [PubMed] [Google Scholar]
- 18.Wasserman J, Perry J, Dowlatshahi D. Stratified, urgent care for transient ischemic attack results in low stroke rates. Stroke. 2010;41:2601–2605. doi: 10.1161/STROKEAHA.110.586842. [DOI] [PubMed] [Google Scholar]
- 19.Health Care Guideline: Diagnosis and Treatment of Ischaemic Stroke. 10th ed. Bloomington, MN: Institute for Clinical Systems Improvement; 2012.
- 20.Johnston SC, Albers GW, Gorelick PB. National Stroke Association recommendations for systems of care for transient ischemic attack. Ann Neurol. 2011;69:872–877. doi: 10.1002/ana.22332. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.