

Abstract
Objective
We evaluated whether regular mobile phone text reminders improved patients’ retention in antiretroviral therapy (ART) care in Mozambique.
Design
SMSaúde was a randomised control trial of HIV-infected patients on ART who received regular text message reminder vs. standard of care at three public health facilities in Maputo Province, Mozambique. The primary outcome was retention in HIV care. Between November 2011 and March 2012, 830 eligible HIV-infected patients on ART were randomized 1:1 to the text reminder intervention or standard of care.
Methods
We used Kaplan-Meier estimators and log-rank tests to compare proportions of patients who received SMS reminders who were retained in HIV care compared to the control group which received standard of care. Post-hoc analyses were done using Cox proportional-hazards models stratified by urban/rural facility and when initiated ART (<3-months vs. >3-months). Hazard ratios and confidence intervals are reported. Analysis was with intention to treat.
Results
Patients who received text messages had lower attrition from HIV care at 12-months, though the difference was non-significant (RR=0.68, 95%CI=0.41–1.13). Among urban patients, text messages improved retention in HIV care (RR=0.54, 95% CI=0.31–0.95). Intervention patients newly initiated on ART (<3-months) had lower attrition compared to control patients (HR=0.54; 95% CI=0.23–0.91), especially urban newly initiated patients (HR=0.20, 95% CI=0.06–0.64). Text messages had no effect on retention among rural patients.
Conclusion
Text messages did not improve retention in HIV care for all patients on ART, but improved retention in care of urban patients and those who recently started ART and received text reminders compared with standard of care.
Trial Registration
INTRODUCTION
Retention in HIV care and adherence to antiretroviral therapy (ART) are the main challenges in preventing HIV-related morbidity and mortality among HIV-infected patients in Mozambique. In 2011, only 74% of patients enrolled in ART programs were still in the program 12-months after initiating treatment.1 Evidence from large-scale treatment programs in sub-Saharan Africa demonstrate that retention in care programs and treatment adherence decline over time.2 Despite various interventions to improve patient adherence and retention in HIV care in Mozambique, the number of patients who discontinue treatment is still increasing.1,3 For patients on ART, reduced loss to follow-up has important correlations with better clinical outcomes, including weight gain, recovery of CD4 count, reduction of viral load, and a lower likelihood of resistance, morbidity, and mortality.2–5 In addition, studies have also shown that access to HIV care, initiation of ART and optimal adherence decreases the risk of sexually transmitting HIV.6
One major challenge with improving HIV treatment efficacy is ensuring that patients adhere to their treatment, including medication and medical check-ups until completion.7 There is hence a need to improve retention in care and adherence to ART. While there may be many reasons for the lack of adherence, there may be ways to improve completion of treatment programs by maintaining better contact between healthcare staff and patients.7
Mobile phone technology has the potential to serve as a strategic intervention medium to improve patient management.8 Due to the widespread use and low cost of this technology, this technology pervades all age groups, many cultures and socioeconomic backgrounds, also in developing countries. Mobile phone technology allows communication across geographic boundaries and reaches people directly where they are located.8 Moving across socio-economic and cultural boundaries, cell phones have revolutionised communication and access to and delivery of information and services.
Several studies have demonstrated the potential of mobile phone text messaging to improve health services and, in turn, health outcomes.9–13 Mobile phone text messaging interventions have proven successful in increasing appointment attendance, increasing treatment adherence for a variety of conditions, disseminating public health information, and improving vaccination rates.9–14 Also, text message reminders have proven to be well suitable for supporting self-management and improvement of patients’ self-efficacy skills through, for instance, medication reminders10,15–19 and motivational text messages.10,20
Research about the effects of mobile phone text messages reminders on ART, medication and appointment adherence has shown mixed results, especially in resource-limited settings. Studies from two Kenyan trials suggest that text message can improve adherence to ART, reduce viral load and reduce treatment interruptions.10,21 Another study with patients from Kenya and Cameroon found that text messaging improved adherence to ART (adjusted odds ratio [aOR]= 1.46; 95% confidence interval [CI]= 1.13, 1.88; p=0.004).22 In the United States, daily text messaging was a feasible and acceptable way to remind HIV-positive youth with poor adherence to ART to take their medications and there was a significant increase in adherence rates post-intervention.23 In Brazil, text messaging improved ART adherence among women living with HIV.24 However, other research has shown no effect of text messaging on health interventions.14 Another study in Cameroon demonstrated that weekly standardized motivational text messages did not significantly improve ART adherence.20 In Scotland, text message appointment reminders for patients who persistently failed to attend their general practice appointments failed to show significant reduction in non-attendance rate.25.
Mobile health or m-health interventions are in the early stages in Mozambique, compared, for example, with the burgeoning m-health programmes in neighbouring South Africa. To our knowledge this is the first study in Mozambique to analyse the impact of text message reminders in increasing retention in ART care, and one the first text message intervention in the public health care system, which may enable various players to take a significant role in m-health in Mozambique. The Mozambique Ministry of Health (MOH) has highlighted the importance of m-health to improve uptake of and retention in health services with future plans for a policy or working group. Data on the efficacy of text message reminders for retention in HIV care remain scarce. To address these problems, we launched SMSaúde - a randomised control trial in 2011 to evaluate the impact of text message reminders on adherence to ART care. The initiative involves a public-private partnership with Vodacom, who provided free text messages, modems, and technical support.
METHODS
Study design and participants
The SMSaúde study was designed to be a two-arm randomized controlled trial with the intervention being a structured series of text message reminders sent to HIV-infected adult patients on ART from one rural and two urban government-run health centers in Maputo Province. These health centers were selected by a convenience sample by the Maputo Provincial Directorate of Health to ensure similar quality and access to care across the network and included the following characteristics: availability of ART services for two or more years, availability of electronic patient databases (with regular supply of electricity), and availability of cell phone network in the community. The selected health centers included: 1) Matola II Health Center (urban), 2) Machava II Health Center (urban), 3) Namaacha Health Center (rural).
Randomization and allocation concealment
The study was launched in November 2011, and the final recruitment took place in March 2012. During the recruitment period, ART patients who presented for clinical consultation in these health centers were interviewed for eligibility and then randomised (1:1) to a control arm (standard care - including defaulter tracing conducted by lay counsellors only after patients had defaulted from treatment) or an intervention arm, that received automated text message reminders. Eligibility criteria included: 18 years of age or older, currently residing in Maputo Province, plans to reside in Maputo Province for at least 12-months, cell phone ownership, ability to read and write in Portuguese (self-reported), receiving first line ART, and taking ART for over 15 days. All patients received counselling prior to the initiation of ART regarding the importance of adherence and access to support groups with other people living with HIV in their community.
To guarantee allocation concealment, prior to enrolment per health facility an electronic randomisation list was generated with 50% probability to belong to one arm. Only the study’s statistician was aware of the study allocation. At recruitment the counsellor invited and enrolled patients unware of the randomization allocation. All clinicians and investigators were blinded to the study allocation. At each day of recruitment all recruited study identification and cell phone numbers was entered into the text message sending system which used the electronic randomisation list to send the message. All study staff and clinicians were blinded to randomization.
Interventions
Participants were followed up from April 2012 for 12-months, and the intervention ended in March 2013. During that period, short text messages were sent to intervention participant’s mobile phones. The message content was developed after extensive consultation utilising focus group discussions with ART patients and separate discussions with clinic staff. The focus group discussions showed that patients often linked happiness with being healthy, a key message that was integrated into the text message messages. All messages were less than 160 characters, so they could be received by all types of cell phones. Messages did not specifically mention HIV or ART to maintain confidentiality of HIV status (see Table 1 for messages). We conceptualized the messages and intervention after reviewing behavioural theory around factors associated with retention in care, including distance to health facility, economic priorities, and family factors.
Table 1.
SMSaude text message reminders sent to patients receiving antiretroviral and HIV care in Maputo Province, Mozambique
| Category | Example text messagesa |
|---|---|
| Welcome (at study initiation) | Good morning family!! Welcome to the health services of XXX Health Center! |
| Farewell (at end of study) | Thank you for your participation! Continue to take your medications and return to your Health Center for appointments. Khanimambo! (Thank you!) |
| Appointment | With health there is joy. Love yourself. Come to your Health Center for your next visit scheduled for xx-xx-xxxx day! |
| Medication | Hello! Your health is above all. Remember of your visit scheduled for xx-xx-xxxx day in your Health Center! We are waiting for you. |
| Educational | Hello. Your health is above all. Remember to take your pills every day at the same time and follow the advice of health personnel! |
All messages were translated from Portuguese
Messages were sent automatically using a modem connected to the cell phone network from each health centre. The SMSaúde platform pulled data from the electronic patient database, including upcoming drug pick-ups and clinical appointments, to send the automatic messages. Messages were divided into four categories: general messages (welcome and goodbye messages), appointment reminders, medication reminders, and educational messages. The first message was sent hours later after the health facility was closed. The last message was sent 7 days after the 12-month follow up or if the patient decided to leave the SMSaúde study. Both appointment reminders and medication reminders were sent 2 and 7 days prior to the date of clinical appointment and drug pick-up. Educational messages were sent every 60 days after the study initiation. The SMSaúde service sent one-way messages to which respondents could respond but would not receive follow-up responses. In the control group, participants did not receive text messages, but did receive the standard of care which included oral reminders about their upcoming drug pickups or medical appointments during their follow up visits.
Data management
Patient data were entered into Microsoft Access electronic database which has been widely used in Mozambique since 2007 for management of patients on ART.26 To ensure data quality, the electronic database contains rules for validating input data (e.g., maximum and minimum limits on numerous variables, maximum number of characters). At each study site, data were saved daily on a back-up drive. Each week, a compressed and encrypted copy of the data was placed on a CD-ROM and sent to ARK’s headquarters in Maputo. There the data were incorporated into a central database running on a server prepared for the study which was used for central monitoring of the evolution of data capturing, input error checking, and regular monitoring of the study.
For the study analysis of demographic (sex, age, residence, marital status and literacy) and clinical (weight, height, WHO stage, CD4 absolute count) data, date of last drug pickup, and defaulting status at end of 12-months was abstracted from the electronic patient database. We also included distance to health facility measured via GPS, according to patients’ address or zone of habitation when the patient’s address was not available. The primary outcome was retention in HIV care. The second outcomes was attrition (loss to follow-up from HIV care). Loss to follow-up from care was defined as having occurred in a patient when more than 60-days elapsed since the last documented drug pick up or clinical visit.
Statistical analysis
Baseline data for all included participants were summarised as median and quartiles (first and third, Q1, Q3) for continuous variables and number and percent for categorical variables. The primary outcome was retention in HIV care. We defined the proportion of retention in care as the complementary of the cumulative proportion of defaulting from treatment. By the time the trial was designed estimated retention in ART post 12 months of ART was 88%. Under that retention figure the required sample size to detect a 50% decrease in hazard rate of defaulting, with 80% power at an alpha of 5% was 860 and 72 patients lost to follow up. The calculations were implemented using the stpower logrank command from Stata 11. This overall sample was then distributed proportionally to volume of patients in ART of the chosen sites.
Proportion of patients retained in care were obtained using Kaplan–Meier estimator and a log-rank test was used for comparisons. Cox proportional-hazards models stratified by urban/rural and newly/long time initiated ART (<3-months or >3-months on ART) and hazard ratios and its 95% confidence intervals are reported. Primary analysis was by intention to treat. Data was analyzed using Stata 11 (StataCorp. 2009. Stata: Release 11. Statistical Software. College Station, TX: Stata Corp LP).
Ethics approval
All eligible participants provided their informed consent to participate in the study, which was approved by the National Bioethics Committee for Health (CNBS) of the Ministry of Health in Mozambique (IRB#: 00002657). Participants were informed about the randomisation of the study and that they had a 50/50 chance of receiving regular text message reminders and educational messages for the upcoming 12-months. The study was registered at Clinicaltrials.gov NCT01910493.
RESULTS
Recruitment, participant flow and characteristics of the study population
Of the 1,201 ART patients who were interviewed in the three selected health centers between November 2011 and March 2012, 830 (69%) were deemed eligible and enrolled. The major barriers to study eligibility were illiteracy (n=140, 38%), lack of ownership of a cell phone (n=99, 27%, of whom 82% were women), or both reasons (n=106, 29%). Other reasons for exclusion (n=21, 6%) included not living in the area or plans to move within the upcoming 12-months. Participants were randomized 1:1 to either the control (n=414) or intervention group (n=416) (Figure 1).
Figure 1.
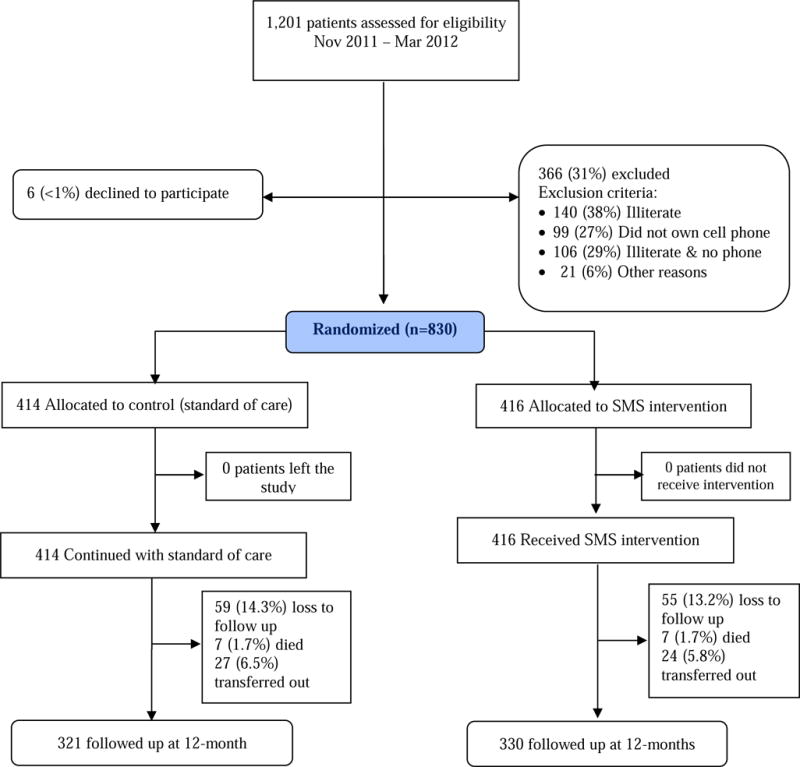
SMSaúde Study Flow Diagram: ART Cohort
Women accounted for 59.9% of the cohort; 73.5% in the rural facility vs. 57.3% in the urban facilities (data not tabled). The median age was 36.9 years (inter-quartile range [IQR] 31.3 – 44.9) and the median time on ART was 13.7 months (IRQ 4.2 – 26.6). Most participants had attained a primary level of education (73.5%), while 23.5% had attained a secondary or technical education level. More than half of the participants were either married or cohabited with a partner (57.4%), while one-third were single (34.7%); the remainder were widowed (7.7%). The details of participants’ characteristics are reported in Table 2. There were no differences between the control and intervention groups for any of the baseline socio-demographic variables.
Table 2.
Baseline socio-demographic and health information for patients on antiretroviral therapy in three health facilities in Mozambique, stratified by randomization to text message group or standard of care, 2011–2013
| Standard of care group (n =414) |
Intervention group (n=412) |
Total (n = 830) | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Categorical variables | ||||||
|
| ||||||
| Health center | ||||||
| Machava II | 191 | 46.1 | 190 | 45.7 | 381 | 45.9 |
| Matola II | 157 | 37.9 | 160 | 38.5 | 317 | 38.2 |
| Namaacha | 66 | 15.9 | 66 | 15.9 | 132 | 15.9 |
| Gender | ||||||
| Male | 172 | 41.5 | 163 | 39.2 | 333 | 40.1 |
| Female | 242 | 58.5 | 253 | 60.8 | 497 | 59.9 |
| Education | ||||||
| Illiterate | 7 | 1.7 | 5 | 1.2 | 12 | 1.7 |
| Primary | 305 | 73.7 | 305 | 73.3 | 610 | 73.5 |
| Secondary/technical | 95 | 22.9 | 100 | 24.0 | 195 | 23.5 |
| University | 5 | 1.2 | 2 | 0.5 | 7 | 0.8 |
| Missing | 2 | 0.5 | 4 | 1.0 | 6 | 0.7 |
| Marital status | ||||||
| Cohabitating | 215 | 51.9 | 213 | 51.2 | 428 | 51.6 |
| Single | 136 | 32.9 | 152 | 36.5 | 288 | 34.7 |
| Married | 30 | 7.2 | 18 | 4.3 | 48 | 5.8 |
| Widower | 33 | 8.0 | 31 | 7.5 | 64 | 7.7 |
| Missing | 0 | 0.0 | 2 | 0.5 | 2 | 0.2 |
| WHO stage | ||||||
| I | 146 | 35.3 | 148 | 35.6 | 294 | 35.4 |
| II | 91 | 22.0 | 75 | 18.0 | 166 | 20.0 |
| III | 143 | 34.5 | 162 | 38.9 | 305 | 36.7 |
| IV | 25 | 6.0 | 28 | 6.7 | 53 | 6.4 |
| Missing | 9 | 2.2 | 3 | 0.7 | 12 | 1.4 |
| Continuous variables | Median (Q1, Q3) | Median (Q1, Q3) | Median (Q1, Q3) | |||
| Age in years | 36.9 | (31.3, 45.7) | 36.9 | (31.2, 43.7) | 36.9 | (31.3, 44.9) |
| CD4 cell count (baseline) | 304 | (196, 468) | 320 | (202,486) | 313 | (200, 475) |
| Time on ART (baseline) in months | 13.1 | (4.5, 26.5) | 14.2 | (4.1, 26.7) | 13.7 | (4.2, 26.6) |
Q1: first quartile; Q3: third quartile.
Retention of participants
Overall, the retention in ART care was higher in the intervention group (93.8%, 95% CI= 90.5 – 95.7) than the control group (91.0%, 95% CI= 87.7 – 93.4), however text message reminders had a non-significant impact on retention in ART care (rate difference=2.8, 95% CI= −0.9 – 6.4, p=0.139). The retention among urban patients was also higher in the intervention group (94.3%, 95% CI=91.3 – 96.4) than in the control group (89.9%, 95% CI=86.1 – 93.1; rate difference=4.4, 95% CI= 0.4 – 8.5, p=0.032). Among rural patients, retention was higher in the control group (96.8%, 95% CI= 87.9 – 99.2) than in the intervention group (90.7%, 95% CI = 08.4 – 95.7) although this difference was not statistically different (rate difference=−6.1, 95% CI − 14.5 – 2.2, p=1.48). (Table 3).
Table 3.
Risk differences and risk ratios of retention in antiretroviral care comparing text message intervention to standard of care in three health facilities in Mozambique, 2011–2013
|
|
||||||
|---|---|---|---|---|---|---|
| Rate Differences | Rate Ratios | |||||
|
|
||||||
| Control | Intervention | PE (95%CI) | p | PE (95%CI) | p | |
| Retention at 12 months %, (95% CI)* | ||||||
| All sites | 91.0 (87.7 – 93.4) | 93.8 (90.9 – 95.7) | 2.8 (−0.9 – 6.4) | 0.1393 | – | |
| Urban | 89.9 (86.1 – 93.1) | 94.3 (91.3 – 96.4) | 4.4 (0.4 – 8.5) | 0.0320 | – | |
| Rural | 96.8 (87.9 – 99.2) | 90.7 (80.4 – 95.7) | −6.1 (−14.5 – 2.2) | 0.1482 | – | |
| Attrition incidence per 100 person-years within first 12 months of follow up, PE (95% CI) | ||||||
| All sites | 9.5 (6.8 – 13.1) | 6.4 (4.3 – 9.5) | −3.0 (−7.0 – 1.0) | 0.1389 | 0.68 (0.41 – 1.13) | 0.1386 |
| Urban | 10.7 (7.6 – 15.0) | 5.8 (3.7 – 9.1) | −4.9 (−9.3 – −0.4) | 0.0306 | 0.54 (0.31 – 0.95) | 0.0324 |
| Rural | 3.2 (0.8 – 12.9) | 10.0 (4.5 – 22.2) | 6.8 (−2.4 – 15.9) | 0.1661 | 3.10 (0.63 – 15.34) | 0.1662 |
PE = point estimate;
95%CI = 95% confidence interval
Kaplan-Meier based estimates at end of 12 months of follow up and differences of retentions tested using z-test
Overall, the attrition incidence was 9.5 in the control group (95% CI= 6.8 – 13.1) vs 6.4 (95% CI= 4.3 – 9.5) in the intervention group per 100 person years on ART, though it was not statistically different (incidence rate ratio (IRR) 0.68, 95% CI= 0.41 – 1.13, p=0.139). Among urban patients, those in the intervention group had a lower attrition incidence (attrition incidence=5.8, 95% CI= 3.7 – 9.1) compared to patients in the control group (attrition incidence=10.7, 95% CI= 7.6 – 15.0; IRR=0.54, 95% CI 0.31 – 0.95, p=0.031). Among rural patients, attrition incidence was not different between the standard of care and text message reminder group (IRR=3.10, 95% CI=0.63 – 15.34, p=0.166). (Table 3).
Among those who recently initiated ART (< 3-months) the risk of attrition in HIV care among patients who received text message reminders was one-third of that in the control arm (hazard ratio [HR]= 0.33, 95% CI=0.12–0.91, p=0.033), and was lowest in urban patients newly initiated on ART (HR=0.20, 95% CI=0.06 -0.64, p=0.006) and among non-newly initiated urban patients who received text messages (HR=0.34, 95% CI=0.12, 0.96, p=0.04). Rural patients who received text messages did not have any differences in attrition (Table 4).
Table 4.
Hazard ratio of retention in ART care and follow up time in cohort comparing text message reminders to standard of care in three health centers in Mozambique (2011–2013)
|
|
||
|---|---|---|
| HR* (95%CI) | p | |
| All sites | ||
| Intervention arm | 0.46 (0.20 – 1.06) | 0.068 |
| All sites‡ | ||
| Intervention and newly initiated on ART** | 0.33 (0.12 – 0.91) | 0.033 |
| Intervention and at non-newly initiated on ART** | 0.54 (0.23 – 1.31) | 0.176 |
| Urban‡ | ||
| Intervention and newly initiated on ART** | 0.20 (0.06 – 0.64) | 0.006 |
| Intervention and non-newly initiated on ART** | 0.34 (0.12 – 0.95) | 0.040 |
| Rural‡ | ||
| Intervention and newly initiated on ART** | 7.5 (0.27 – 212.38) | 0.237 |
| Intervention and non-newly initiated on ART** | 6.2 (0.44 – 87.63) | 0.175 |
95%CI – 95% confidence interval
From Proportion Hazard Cox regression fitted respectively for all, urban and rural sites with intervention and interaction of arm and time of follow up.
Computed from interaction between intervention arm and indicator less than 3 months on ART; the reference for is respectively control arm and less than 3 months on ART, and control arm and at least 3 months on ART
Non pre-specified analysis – it includes adjustment for time on ART as an indicator for less than 3 months and its interaction with intervention. This way the differential effect due to experience of ART is captured
DISCUSSION
Our study demonstrated that regular text message reminders and educational messages did not improve retention in HIV care overall among patients on ART in Mozambique. In post hoc analysis, weekly text message reminders were effective at improving retention in care among urban patients, and among patients who had recently initiated ART. Overall retention in the study, and in ART care, was excellent, with approximately 90% remaining in care when compared to 74% in the Government health facilities in 2011 as measured by patients enrolled in ART program12-months after initiating treatment.1 In our study text messages had no effect on rural retention in HIV care. A variety of factors likely contributed to the observed lack of impact in rural areas. These factors could include underlying transport constraints in rural areas (increased distance from health facility was significantly associated with discontinuing treatment in the rural cohort); poor location of the selected rural health center (near an international border with Swaziland, where cell phone network was weak); likely frequent migration away from the facility sites; problems with consistent cell phone network coverage; and poor access to electricity, which limits the participants’ ability to charge their cell phones.
Other studies found that treatment support such weekly text message messages (vs. daily text message messages), increased counselling and text message combined, as well as treatment supporters were effective at improving ART adherence compared to the standard of care.11 A recent US study among adolescents and young adults found that self-reported ART adherence was higher among those who received personalized daily text message messages.12 Further, a systematic review found that text message reminders can help improve adherence in other chronic diseases such as diabetes, or infectious diseases such as tuberculosis.27 text message messaging have been shown to improve attendance at appointments and behaviour change outcomes.27 However, adherence to ART is easier improved by text message as generally the drugs are at home and a reminder suffices. However, retention includes more logistical and structural determinants (transport, absence from work, migration, etc.) than simply addressing treatment adherence. This is a strength of our study, as we analysed retention in HIV care in urban and rural government clinics, and we did not limit our intervention to adherence to medication.
More research is needed to explore avenues to improve access to mobile health, or m-health, interventions in illiterate women, such as the use of family cell phones. Past research has shown that women in low-income countries are 21% less likely to own a cell phone than men. This gender gap represents at least 300 million women in the developing world without access to a potentially life-enhancing tool.28 In 2011, 29% of the Mozambique population owned a cell phone, and the vast majority of cell phone owners today are men. As we expand our study, we intend to explore the possibility of family cell phone ownership of a cell phone for inclusion in the study because many women have husbands or other family members with cell phones. We will also explore the use of voice messaging to improve the reach among illiterate populations. Designing m-health strategies in rural contexts remains a challenge due to weak infrastructure, illiteracy, and poor cell phone penetration. The role of community health workers in delivering educational messages and referring back to health services is also considered. We intend to address these challenges in an upcoming study of the rural population.
Limitations
There are several limitations to our study including the short time frame, the limited geography and hence limited generalisability of the study, and limited study eligibility. The study only followed patients for 12-months. Study results are thereby limited to short-term follow-up. The limited area of the Maputo Province did not allow us to include rural areas that are not on the national border or areas with poor cell phone coverage, which is typical in most rural areas of Mozambique. Finally, this intervention was limited to literate patients with mobile phones. Despite these limitations, the study found that text message reminders improved retention in care among urban and newly enrolled ART patients in Mozambique.
Further, research on text message messaging has shown that sending too frequent, overly long, and repetitive text message reminders can lead to habituation.29,30 Boredom or a reduction in novelty can result in diminishing effect on adherence to whatever behaviour change the text message is trying to promote. Similarly, at the start of a study or intervention, patients may be enthusiastic and interested in the novel process (because it is intrinsically pleasing), which could diminish over time as the novelty wanes.31–34 As a result, longer-term studies of outcomes are needed to evaluate the impact of boredom, or novelty may have on the participants.
Conclusion
Our study showed that retention in HIV care among patients on ART in Mozambique was unchanged among those who received regular text message reminders over 12-months. We did find that text message reminders did impact retention in care among urban patients and among patients who had started on treatment within the past 3-months, when patients are more likely to drop out of care and/or treatment. However, prominent knowledge gaps include the absence of research on cost-effectiveness, long-term outcomes, and patient satisfaction. More research is needed to understand if text message messaging can improve HIV care for HIV-infected individuals before they initiate ART. We will continue to work on improving the reach of this technology-based solution to other populations.
Acknowledgments
We acknowledge the time and collaboration from the patients and their family, the health care team staff, data collectors and analysts, the Mozambican Ministry of Health and Vodacom. Jose Nhavoto wishes to acknowledge the support of his Professors Gunnar Klen and Age Gronlund.
Sources of Funding: Cesar de Sousa and Orvalho Agusto have received honoraria from Absolute Return for Kids (ARK). ARK funded the entire intervention, with additional support from Vodacom Mozambique.
Footnotes
Conflicts of Interest: For the remaining authors none were declared.
References
- 1.Republic of Mozambique National AIDS Council. Global AIDS Response Progress Report. Mozambique: 2012. http://www.unaids.org/en/dataanalysis/knowyourresponse/countryprogressreports/2012countries/ce_MZ_Narrative_Report%5B1%5D.pdf. [Google Scholar]
- 2.Mannheimer SB, Matts J, Telzak E, et al. Quality of life in HIV-infected individuals receiving antiretroviral therapy is related to adherence. AIDS Care. 2005;17(1):10–22. doi: 10.1080/09540120412331305098. http://www.ncbi.nlm.nih.gov/pubmed/15832830. Accessed April 15, 2013. [DOI] [PubMed] [Google Scholar]
- 3.Wandeler G, Keiser O, Pfeiffer K, et al. Outcomes of antiretroviral treatment programs in rural Southern Africa. J Acquir Immune Defic Syndr. 2012;59(2):e9–e16. doi: 10.1097/QAI.0b013e31823edb6a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zolopa A, Andersen J, Powderly W, et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: a multicenter randomized strategy trial. PLoS One. 2009;4(5):e5575. doi: 10.1371/journal.pone.0005575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ivers LC, Kendrick D, Doucette K. Efficacy of antiretroviral therapy programs in resource-poor settings: a meta-analysis of the published literature. Clin Infect Dis. 2005;41(2):217–224. doi: 10.1086/431199. [DOI] [PubMed] [Google Scholar]
- 6.Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505. doi: 10.1056/NEJMoa1105243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nhavoto JA, Grönlund Å, Chaquilla WP. SMSaúde: Design, Development, and Implementation of a Remote/Mobile Patient Management System to Improve Retention in Care for HIV/AIDS and Tuberculosis Patients. JMIR mHealth uHealth. 2015;3(1):e26. doi: 10.2196/mhealth.3854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shaw RJ, Bosworth HB, Hess JC, et al. Development of a Theoretically Driven mHealth Text Messaging Application for Sustaining Recent Weight Loss. JMIR mHealth uHealth. 2013;1(1):e5. doi: 10.2196/mhealth.2343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lester RT, Gelmon L, Plummer FA. Cell phones: tightening the communication gap in resource-limited antiretroviral programmes? AIDS. 2006;20(17):2242–2244. doi: 10.1097/QAD.0b013e3280108508. [DOI] [PubMed] [Google Scholar]
- 10.Pop-Eleches C, Thirumurthy H, Habyarimana JP, et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011;25(6):825–834. doi: 10.1097/QAD.0b013e32834380c1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mills EJ, Lester R, Thorlund K, et al. Interventions to promote adherence to antiretroviral therapy in Africa: a network meta-analysis. Lancet HIV. 2014;1(3):e104–e111. doi: 10.1016/S2352-3018(14)00003-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Garofalo R, Kuhns LM, Hotton A, Johnson A, Muldoon A, Rice D. A Randomized Controlled Trial of Personalized Text Message Reminders to Promote Medication Adherence Among HIV-Positive Adolescents and Young Adults. AIDS Behav. 2015 Sep; doi: 10.1007/s10461-015-1192-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Horvath T, Azman H, Kennedy GE, Rutherford GW. Mobile phone text messaging for promoting adherence to antiretroviral therapy in patients with HIV infection. Cochrane Database Syst Rev. 2012;(3):CD009756. doi: 10.1002/14651858.CD009756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bjørnholt K, Christiansen E, Atterman Stokholm K, Hvolby A. The effect of daily small text message reminders for medicine compliance amongst young people connected with the outpatient department for child and adolescent psychiatry. A controlled and randomized investigation. Nord J Psychiatry. 2016;70(4):285–289. doi: 10.3109/08039488.2015.1106580. [DOI] [PubMed] [Google Scholar]
- 15.Sahm L, MacCurtain A, Hayden J, Roche C, Richards HL. Electronic reminders to improve medication adherence–are they acceptable to the patient? Pharm World Sci. 2009;31(6):627–629. doi: 10.1007/s11096-009-9327-7. [DOI] [PubMed] [Google Scholar]
- 16.Vervloet M, van Dijk L, Santen-Reestman J, et al. SMS reminders improve adherence to oral medication in type 2 diabetes patients who are real time electronically monitored. Int J Med Inform. 2012;81(9):594–604. doi: 10.1016/j.ijmedinf.2012.05.005. [DOI] [PubMed] [Google Scholar]
- 17.Vervloet M, van Dijk L, Santen-Reestman J, van Vlijmen B, Bouvy ML, de Bakker DH. Improving medication adherence in diabetes type 2 patients through Real Time Medication Monitoring: a randomised controlled trial to evaluate the effect of monitoring patients’ medication use combined with short message service (SMS) reminders. BMC Health Serv Res. 2011;11:5. doi: 10.1186/1472-6963-11-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Foreman KF, Stockl KM, Le LB, et al. Impact of a text messaging pilot program on patient medication adherence. Clin Ther. 2012;34(5):1084–1091. doi: 10.1016/j.clinthera.2012.04.007. [DOI] [PubMed] [Google Scholar]
- 19.Petrie KJ, Perry K, Broadbent E, Weinman J. A text message programme designed to modify patients’ illness and treatment beliefs improves self-reported adherence to asthma preventer medication. Br J Health Psychol. 2012;17(1):74–84. doi: 10.1111/j.2044-8287.2011.02033.x. [DOI] [PubMed] [Google Scholar]
- 20.Mbuagbaw L, Thabane L, Ongolo-Zogo P, et al. The Cameroon Mobile Phone SMS (CAMPS) trial: a randomized trial of text messaging versus usual care for adherence to antiretroviral therapy. PLoS One. 2012;7(12):e46909. doi: 10.1371/journal.pone.0046909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lester RT, Ritvo P, Mills EJ, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838–1845. doi: 10.1016/S0140-6736(10)61997-6. [DOI] [PubMed] [Google Scholar]
- 22.Mbuagbaw L, van der Kop ML, Lester RT, et al. Mobile phone text messages for improving adherence to antiretroviral therapy (ART): an individual patient data meta-analysis of randomised trials. BMJ Open. 2013;3(12):e003950. doi: 10.1136/bmjopen-2013-003950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dowshen N, Kuhns L, Johnson A, Holoyda B, Garofalo R. 91. Text Message Reminders to Improve Adherence to Antiretroviral Therapy for HIV-Positive Youth. J Adolesc Heal. 2011;48(2):S64–S65. doi: 10.1016/j.jadohealth.2010.11.138. [DOI] [Google Scholar]
- 24.da Costa TM, Barbosa BJP, Gomes e Costa DA, et al. Results of a randomized controlled trial to assess the effects of a mobile SMS-based intervention on treatment adherence in HIV/AIDS-infected Brazilian women and impressions and satisfaction with respect to incoming messages. Int J Med Inform. 2012;81(4):257–269. doi: 10.1016/j.ijmedinf.2011.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fairhurst K, Sheikh A. Texting appointment reminders to repeated non-attenders in primary care: randomised controlled study. Qual Saf Health Care. 2008;17(5):373–376. doi: 10.1136/qshc.2006.020768. [DOI] [PubMed] [Google Scholar]
- 26.Pati R, Lahuerta M, Elul B, et al. Factors associated with loss to clinic among HIV patients not yet known to be eligible for antiretroviral therapy (ART) in Mozambique. J Int AIDS Soc. 2013;16:18490. doi: 10.7448/IAS.16.1.18490. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3679527&tool=pmcentrez&rendertype=abstract. Accessed April 1, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mbuagbaw L, Mursleen S, Lytvyn L, Smieja M, Dolovich L, Thabane L. Mobile phone text messaging interventions for HIV and other chronic diseases: an overview of systematic reviews and framework for evidence transfer. BMC Health Serv Res. 2015;15(1):33. doi: 10.1186/s12913-014-0654-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.GSMA Development Fund. Cherie Blair Foundation for Women, Vital Wave Consulting. Women & Mobile: A Global Opportunity. 2010 http://www.cherieblairfoundation.org/uploads/pdf/women_and_mobile_a_global_opportunity.pdf.
- 29.Hardy H, Kumar V, Doros G, et al. Randomized controlled trial of a personalized cellular phone reminder system to enhance adherence to antiretroviral therapy. AIDS Patient Care STDS. 2011;25(3):153–161. doi: 10.1089/apc.2010.0006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Strandbygaard U, Thomsen SF, Backer V. A daily SMS reminder increases adherence to asthma treatment: a three-month follow-up study. Respir Med. 2010;104(2):166–171. doi: 10.1016/j.rmed.2009.10.003. [DOI] [PubMed] [Google Scholar]
- 31.Ho LY, Camejo L, Kahook MY, Noecker R. Effect of audible and visual reminders on adherence in glaucoma patients using a commercially available dosing aid. Clin Ophthalmol. 2008;2(4):769–772. doi: 10.2147/opth.s3284. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2699814&tool=pmcentrez&rendertype=abstract. Accessed April 1, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Charles T, Quinn D, Weatherall M, Aldington S, Beasley R, Holt S. An audiovisual reminder function improves adherence with inhaled corticosteroid therapy in asthma. J Allergy Clin Immunol. 2007;119(4):811–816. doi: 10.1016/j.jaci.2006.11.700. [DOI] [PubMed] [Google Scholar]
- 33.Andrade ASA, McGruder HF, Wu AW, et al. A programmable prompting device improves adherence to highly active antiretroviral therapy in HIV-infected subjects with memory impairment. Clin Infect Dis. 2005;41(6):875–882. doi: 10.1086/432877. [DOI] [PubMed] [Google Scholar]
- 34.Costa FA, Guerreiro JP, Melo MN, et al. Effect of reminder cards on compliance with antihypertensive medication. Int J Pharm Pract. 2005;13(3):205–211. doi: 10.1211/ijpp.13.3.0006. [DOI] [Google Scholar]