

Abstract
Background:
Plaque control has been shown to have a pivotal role in maintaining optimal periodontal health. Toothbrushing as a mechanical plaque control tool is the most popular and effective option for self-performed oral health maintenance. However, the detrimental effects of bristle hardness and force exerted by toothbrushes on the tooth surface are the areas of concern.
Objective:
The aim of this in vitro study was to evaluate the abrasive effect of two different manual toothbrushes exerting predetermined forces on cemental surfaces of the teeth.
Materials and Methods:
Sixty extracted first molars were selected. Totally six experimental groups were formed based on the three predetermined forces 1.5, 3, and 4.5 Newton (N) and two types of manual toothbrushes, i.e., soft and medium bristle hardness. Buccal and lingual surfaces were independently brushed for 5000 cycles using specially designed toothbrushing machine. Throughout the experiment, type and quantity of toothpaste were kept constant. Post 5000 cycles of toothbrushing, change in surface roughness was measured using profilometer in microns and change in weight indicating loss of substance was measured in milligrams.
Results:
Abrasion of cementum is force dependent. Data revealed that both soft and medium bristle hardness toothbrushes cause significant cemental abrasion at 3 and 4.5 N forces.
Conclusions:
Higher is the force, more is the cemental surface abrasion. Soft bristled toothbrush causes more cemental abrasion than medium bristled toothbrush at 3 and 4.5 N forces.
Key words: Dental cementum, periodontitis, tooth abrasion, tooth cervix, toothbrushing
INTRODUCTION
Dental plaque is still considered to be only primary etiologic factor in the development of dental diseases. Thus, effective plaque control is the cornerstone of periodontal therapy to achieve and maintain good oral hygiene. Healthy periodontal tissues and absence of new carious lesions are primary indicators of the patient's effective plaque control measures. The most commonly used self-performed means of meticulous plaque removal by an individual is toothbrushing followed by the use of appropriate interdental aids.[1]
Since its inception in l857 by H. N. Wadsworth,[2] evidences corroborate the fact that toothbrushing performed at appropriate and regular intervals can be an effective tool in controlling dental plaque. Therefore, the use of toothbrush with fluoridated dentifrice is advocated as one of the best mechanical plaque control methods. Toothbrushing for at least 2 min, twice daily, is generally recommended by dental professionals as self-employed plaque control measures.[3] However, if toothbrushing is not done judiciously and methodically, it could result in abrasion of the soft tissues as well as hard tissues of the oral cavity.[4]
Abrasion of teeth was described first by Zsigmondy in 1894 as angular defects and later by Miller in 1907 as a wasting of tooth structure. Abrasion along with erosion and abfraction are now termed as noncarious cervical lesions.[5] Abrasion usually starts at cementoenamel junction and then progresses rapidly since enamel and cementum are very thin at this region. Abrasion process quickly destroys the relatively softer structures such as dentin and cementum. Root caries and teeth sensitivity are two most common clinical manifestations of this condition.[6] Patients often report to the clinics with the complaint of discomfort and sensitivity caused by underlying dentin exposure.
Hence, understanding the process of cementum surface wear caused by various manual toothbrushes at different pressures is a need of an hour. To the best of our knowledge, there have been no such in vitro studies addressing this issue. Application of a predetermined force by a manual toothbrush on the root surface cannot be ascertained in an in vivo setting due to difficulties in standardization. For this reason, construction of a customized toothbrushing apparatus, which would deliver preset constant force, was an absolute requirement. Therefore, this study was undertaken to quantify the abrasion process of cementum with variables namely preset constant forces delivered by the customized toothbrushing apparatus and two manual toothbrushes with different bristle hardness. Type of toothpaste and brushing cycles were kept constant.
MATERIALS AND METHODS
This in vitro study was carried out on sixty extracted right/left mandibular first molar teeth. Teeth were collected from systemically healthy patients (30–60 years) indicated for having Grade II/III mobility as given by Miller's mobility index due to chronic periodontitis.
Teeth from patients with adverse habits such as gutka or tobacco chewing and cigarette smoking were excluded. Also, teeth showing any signs of root caries, root resorption, preexisting wasting diseases such as abrasion, erosion, or abfraction were not included.
A specially designed customized toothbrushing machine simulating manual toothbrushing action in a horizontal manner was constructed. It operated at 24 V with a motor having speed of 70 rpm. The machine has three major functional subassemblies:
clamp and position the tooth
To measure and exert the preset constant force
To hold the toothbrush and give strokes in horizontal motion.
Pre- and post-experimental surface roughness measurements of buccal and lingual surfaces of all the teeth were documented using profilometer. Profilometer is a measuring instrument used to trace a surface profile, to quantify its roughness. Digital weighing scale (AW-1K, LED Table Top [Industrial] Digital Weighing Scale, ATCO private Limited, New Delhi, India) with three used to weigh each tooth pre and post-experiment.
Popular brand toothbrushes (Oral-B ® CrossAction ® Pro-Health™ Toothbrush, The Procter and Gamble Company, Mumbai, India) with medium bristle hardness and soft bristle hardness were used. Standard toothpaste (Colgate Regular Toothpaste, Colgate-Palmolive (India) Limited, Mumbai, India) was used for all the instances.
Each extracted tooth was rinsed in saline to remove all the loose debris. Ultrasonic scaling was performed with piezoelectric ultrasonic scaler unit (Woodpecker Ultrasonic Scaler, Guilin, Guangxi, China) to remove any residual flecks of calculus. Teeth were then preserved in 10% neutral buffered formalin until further experimental procedure. The present study was carried out using three different forces. Based on the findings of Wiegand et al., an average toothbrushing force of approximately 1.6 ± 0.3 N is exerted by humans using manual brush.[7] Hence, to evaluate the effect of this average brushing force value exerted by humans in day-to-day life, the lowest force value for present study was set to be 1.5 N. Two more forces were selected with a constant increment of 1.5 N. Therefore 1.5, 3 and 4.5 N values were fixed. In addition, we also wanted to assess effect of toothbrush bristle hardness on the abrasion process of cementum. Evidences already suggest that hard-bristled toothbrush causes more hard tissue abrasion.[8] Thus, we decided to omit the use of hard-bristled toothbrush and evaluate effect of medium- and soft-bristled toothbrushes only. The same brand of toothbrushes was used, to eliminate bias. Each force was analyzed using both soft and medium toothbrush. Based on this, total six groups were formed.
Initially, three experimental groups were formed based on the preset constant force value that was being exerted during toothbrushing. Then, each experimental group was further subdivided into two subgroups based on the use of soft and medium toothbrush bristle hardness. Sixty extracted teeth were numbered 1–60 using permanent marker pen. Then, twenty teeth were randomly assigned to one of the three experimental groups using table of random numbers. In each experimental group, these 20 teeth were subdivided into two subgroups using same method of randomization. Each subgroup consisted of 10 extracted mandibular 1st molar teeth [Figure 1].
Figure 1.

Experimental groups
Buccal and lingual surfaces of each tooth was marked by letter B and L, respectively. Marking was done on the crown surface well above cementoenamel junction using a permanent marker pen. A groove was prepared on the buccal and lingual surfaces with a small round bur using a contra-angle micromotor handpiece 2 mm below cementoenamel junction. The groove provided a fixed reference point for pre- and post- measurement of surface roughness using profilometer. For all the teeth, surface roughness on buccal and lingual surface was measured in microns just below the reference groove described above.
Each tooth was weighed in milligrams using digital weighting machine having three decimals accuracy. The weight of each tooth was taken pre- and post-experimentation. The difference between pre- and post-experimental weight signifies the amount of tooth material lost during brushing process.
A scaled and labeled tooth was mounted on the machine [Figure 2] with the help of clamp (i and ii). Tooth was clamped in such a way that buccal side of each tooth would be facing the toothbrush bristles first. The slider (iv) with clamped tooth was then moved forward till it made its first contact with the toothbrush and then it was secured in position by tightening the allen screws (vi). Then, pressure on spring (v) was released and dial (vii) was set to zero marking. The slider of spring was then secured in this position using allen screws (ix). Once the zero, i.e., no force on the toothbrush brittles was achieved, the clamped tooth was then moved against the toothbrush till desired compression of spring was achieved. The desired compression of spring was indicated directly on the dial. This simply implied the value of the preset force was being exerted onto the tooth surface by the toothbrush. Based on the experimental group, either soft- or medium-bristled toothbrush was mounted inside the toothbrush holder (x). A standard toothpaste containing fluoride, in this case, Colgate Regular © toothpaste was then applied to the toothbrush in approximately fixed amount (pea size).
Figure 2.
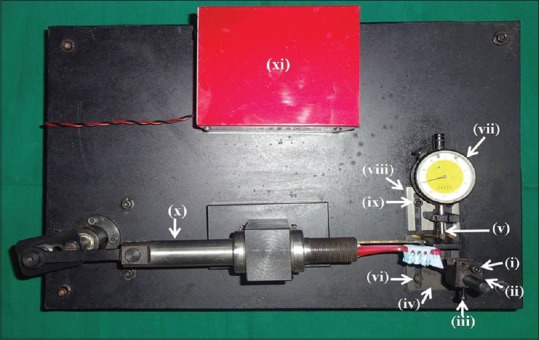
Brushing machine “novel toothbrushing simulator”
The toothbrushing procedure was then carried out till 5000 strokes were completed. One toothbrushing cycle was defined as one forward and one backward movement of the toothbrush. The time calculation was done based on motor speed which was 70 rpm. A digital stop-watch was used to precisely calculate the time required (~1 h 11 min) for completion of 5000 toothbrushing cycles. It corresponded to approximately 8–11 months of toothbrushing by an individual.[9] Once the buccal aspect of tooth was brushed for 5000 toothbrushing cycles, the tooth was unclamped. Then, it was indexed to lingual aspect and same procedure was repeated again as stated above. In order to control the frictional heat generated, each surface was brushed 10 min followed by 2 min rest interval. Distilled water was used as a coolant.
In this 71 min of toothbrushing of each surface, the toothbrush was changed once at 35th min mark which approximately corresponds to 3–4 months of toothbrushing. This was done as per the recommendation of changing toothbrush every 3–4 months.[10]
Once the buccal and lingual aspects of tooth were brushed, they were labeled and kept aside in 10% neutral formalin till toothbrushing of all the 10 teeth of one group was completed. Upon completion of toothbrushing for all the teeth in one group postexperimental measurements were recorded. Procedure was repeated for all the groups.
RESULTS
The post-experimental values were compared with pre-experimental values for each group, and the difference was analyzed using paired t-test. The effect of toothbrushing force and toothbrush bristle hardness on cemental abrasion was separately paired and (intergroup comparisons) analyzed using unpaired t-test. The paired and unpaired t-test were performed at the degree of freedom “9” and confidence interval of 95%.
For multiple groups' comparison of toothbrushing force and toothbrush bristle hardness as well as to determine the most significant combination of force value and toothbrush bristle hardness in causing cemental abrasion, Tukey's “honestly significant difference” test was used. For statistical analysis, (IBM India Pvt Ltd, Bangalore, India) was used.
Change in cemental surface roughness (difference between pre versus post brushing) measured as Ra value in μm showed statistically significant difference for all the groups comprising of both the soft- as well as medium-bristled toothbrushes at all the three forces [Figure 3 and Table 1]. This implies that brushing causes a significant change in surface finish.
Figure 3.
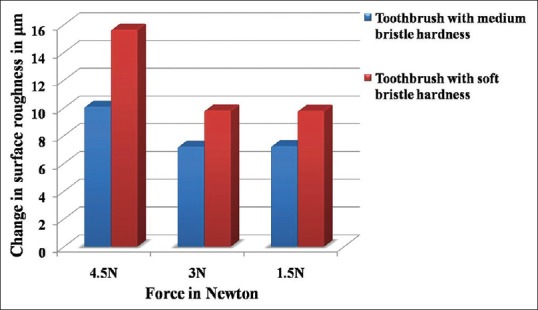
Comparative evaluation of change in surface roughness of teeth
Table 1.
Difference in mean surface roughness value (μm) of the teeth brushed with soft and medium bristle hardness toothbrush in Group A, B, C (AT 1.5, 3 and 4.5 newton preset force)
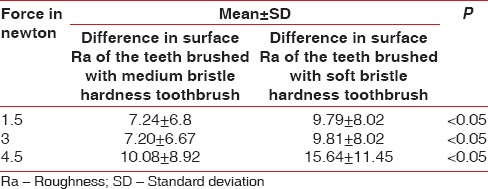
For intergroup comparison, the difference in mean surface roughness (Ra) value of cementum caused by soft- and medium-bristled toothbrush at 1.5, 3, and 4.5 N preset forces was performed using Tukey's “honestly significant difference” test. Results revealed no statistically significant difference in surface roughness values between all three forces for soft- as well as medium-bristled hardness toothbrushes [Figure 3 and Table 1].
Change in weight of tooth (pre versus post brushing) measured in milligrams showed statistically significant difference only for 3N and 4.5 N groups. Both the soft- and medium-bristled toothbrushes were caused a significant change in weight of teeth for 3 and 4.5 N forces [Figure 4 and Table 2]. The quantification of cemental abrasion is directly proportional to material loss. Thus, results showed that abrasion was more for 3 N and 4.5 N for both the type of toothbrushes.
Figure 4.
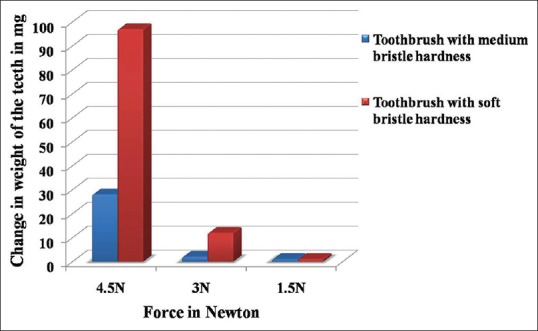
Comparative evaluation of change in weight of teeth
Table 2.
Difference in mean weight (mg) of the teeth brushed with soft and medium bristle hardness toothbrush in Group A, B, C (AT 1.5, 3 and 4.5 newton preset force)
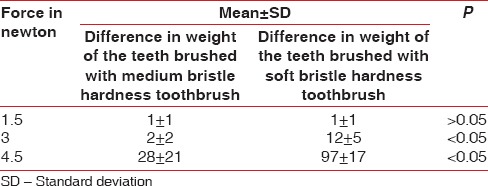
For intergroup comparison, the difference in weight of teeth caused by soft- and medium-bristled toothbrush at 1.5, 3, and 4.5 N preset forces was performed using Tukey's “honestly significant difference” test. Results showed that the difference in mean weight of the teeth caused by soft- as well as medium-bristled toothbrushes for 1.5 and 4.5 N as well as for 3 and 4.5 N was statistically significant [Figure 4 and Table 2]. This simply implies that soft- as well as medium-bristled toothbrushes at 4.5 N cause statistically significant abrasion of cementum.
DISCUSSION
Currently, both primary prevention of gingivitis as well as primary and secondary prevention of periodontitis is based on the achievement of sufficient plaque removal. This is achieved through active participation of patients by following the recommended mechanical plaque removal regimen which is daily habit of toothbrushing.
Although ignorance and improper methodology can cause more harm than any good, most important aspect of this is “excessive force” application by an individual while toothbrushing. This ultimately manifests as cervical abrasive lesions on the tooth as well as recessed gingival surfaces. Failing to acknowledge this, the condition propagates causing additional abrasion defects on exposed cemental surfaces in the presence of “excessive force.”
The crux here is to determine that optimal force value beyond which the abrasive process is actually initiated. At present, there is no such device which can estimate, preset and apply uniform well-controlled force in an in vivo setting. Most of the in vitro studies address and quantify the abrasion of enamel or dentinal surfaces only. There is a dearth of information on wearing of cementum by toothbrushing. Thus, rationale behind this “in vitro” study was to assess the abrasive potential of various preset forces on cemental surfaces and find out the optimal force value based on the regression analysis of force versus material loss.
Wiegand et al. in an observational study stated that an average toothbrushing force exerted by a human while brushing with a manual toothbrush is approximately 1.6 ± 0.3 N.[7] Thus, in the present study, we chose 1.5 N as the lowest force value to begin with. This value helped us to gauge the abrasion caused by a toothbrush at an average brushing force by a human being. Thereafter with the increment of 1.5 N; two more force values were selected, i.e., 3 N and 4.5 N. This allowed us to get a better and larger picture of abrasion of cementum with respect to increase in force.
To exert a preset constant force in an in vitro setting, a “novel toothbrushing simulator” was designed and constructed. The intention of using this set-up was to apply a constant force value and a horizontal/oscillating toothbrushing action which would simulate the normal toothbrushing style of an individual as closely as possible. Review of available literature revealed that “horizontal scrub method” is the commonly employed toothbrushing method by most of the individuals in a studied population.[8] Hence, in the present study, we decided to simulate this 'horizontal scrub toothbrushing action'. The “novel toothbrushing simulator” has various components that allowed us to change the settings according to chosen parameters. These settings were mainly to accommodate the anatomical variation of human teeth, positioning of the toothbrush with respect to the mounted tooth etc. An analog dial was incorporated to determine and set the accurate force value to be exerted during toothbrushing procedure.
To eliminate the morphological variations in different type of teeth, we chose only mandibular first molar. During routine toothbrushing, buccal and lingual surfaces are the ones which come in contact with toothbrush. Thus, we tried to simulate this process by brushing only buccal and lingual surfaces.
The prime objective of the present study was to evaluate the abrasive effects of 'toothbrushes' at various force values. Thus, to avoid the effect of difference in abrasivity of various toothpastes, a single standard toothpaste was used. Colgate regular toothpaste was chosen for the present study because it is the most commonly used toothpaste among the Indian population. It has RDA value of 68, is subclassified as “low” abrasive toothpaste. Every time with the change of toothbrush, a standard quantity (pea size) of toothpaste was used as recommended by ADA.[11]
One of the highlights of this study is the fact that periodontally involved teeth were selected as opposed to healthy teeth because in the healthy extracted teeth, cementum is harder (20 KHN) than cementum of the teeth exposed to periodontal diseases (17 KHN).[12] Hence, results from such work would be more meaningful as selected teeth in the present study were affected by preexisting periodontal infection and inflammation. By choosing only periodontally affected teeth, we tried to eliminate the bias of variation in hardness of cementum surfaces between healthy and periodontally affected teeth.
Based on the observations of this study, it was concluded that the abrasion of cementum increases proportionate to increase in force. When all the forces, i.e., 1.5, 3, and 4.5 N were compared by Tukey's “honestly significant difference” test, it revealed that only 3 and 4.5 Newton forces caused significant abrasion of cementum. 1.5 N failed to cause statistically significant abrasion of cementum for either soft- or medium-bristled toothbrushes. This is in accordance with the study done on enamel and dentin by Wiegand et al.[13] and Ganss et al.[14]
When the effects of soft- and medium-bristled hardness toothbrushes on cementum abrasion was evaluated using Tukey's honestly significant difference” test, both caused significant abrasion at 3 and 4.5 N force only. However, toothbrush with soft bristle hardness was causing more statistically significant abrasion of cementum as compared to toothbrush with medium bristle hardness. Similar findings were reported by Dyer et al.[15] and Wiegand et al.[16] who reported soft bristles caused more abrasion than hard bristles.
Regression analysis of our data revealed that 1.8 N is the threshold force value at or beyond which significant abrasion of cementum can occur. This value is quite close to the average force (1.6 ± 0.3 N) exerted by an individual using a manual toothbrush in day to day life as stated by Wiegand et al.[7]
Limitations
Results may differ in the presence of intra-oral factors. Effects of only “horizontal toothbrushing technique” were tested. Cemental abrasion without toothpaste was not evaluated. Abrasion defects were measured two dimensionally using two-dimensional profilometer. Three dimensional profilometer might provide more accurate details of abrasion defects.
CONCLUSIONS
Abrasion of cementum seems to be a force dependent process. Higher the force more significant is the amount of abrasion. Based on the data, we can conclude that use of soft and medium hardness toothbrushes at 1.5 N caused no significant cemental abrasion. However, at 3 and 4.5 N forces, significant abrasion of cementum was observed. Contrary to general belief, i.e., abrasion is proportional to increase in bristle hardness; our study revealed that toothbrush with soft bristle hardness at 1.8 N or beyond causes significantly more abrasion than a toothbrush with medium bristle hardness.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors wish to thank Mr. Pradeep K. Joshi for his assistance.
REFERENCES
- 1.Van der Weijden F, Slot DE. Oral hygiene in the prevention of periodontal diseases: The evidence. Periodontol 2000. 2011;55:104–123. doi: 10.1111/j.1600-0757.2009.00337.x. [DOI] [PubMed] [Google Scholar]
- 2.Lang NP, Lindhe J. Mechanical supragingival plaque control. In: Van der Weijden F, Slot DE, Echeverria JJ, Lindhe J, editors. Clinical Periodontology and Implant Dentistry. Volume 2: Clinical Concepts. 6th ed. Oxford: John Wiley and Sons Ltd; 2015. p. 679. [Google Scholar]
- 3.Williams K, Ferrante A, Dockter K, Haun J, Biesbrock AR, Bartizek RD, et al. One- and 3-minute plaque removal by a battery-powered versus a manual toothbrush. J Periodontol. 2004;75:1107–13. doi: 10.1902/jop.2004.75.8.1107. [DOI] [PubMed] [Google Scholar]
- 4.Alexander JF, Saffir AJ, Gold W. The measurement of the effect of toothbrushes on soft tissue abrasion. J Dent Res. 1977;56:722–7. doi: 10.1177/00220345770560070301. [DOI] [PubMed] [Google Scholar]
- 5.Grippo JO, Simring M, Coleman TA. Abfraction, abrasion, biocorrosion, and the enigma of noncarious cervical lesions: A 20-year perspective. J Esthet Restor Dent. 2012;24:10–23. doi: 10.1111/j.1708-8240.2011.00487.x. [DOI] [PubMed] [Google Scholar]
- 6.Addy M. Tooth brushing, tooth wear and dentine hypersensitivity – Are they associated? Int Dent J. 2005;55:261–7. doi: 10.1111/j.1875-595x.2005.tb00063.x. [DOI] [PubMed] [Google Scholar]
- 7.Wiegand A, Burkhard JP, Eggmann F, Attin T. Brushing force of manual and sonic toothbrushes affects dental hard tissue abrasion. Clin Oral Investig. 2013;17:815–22. doi: 10.1007/s00784-012-0788-z. [DOI] [PubMed] [Google Scholar]
- 8.Heasman PA, Holliday R, Bryant A, Preshaw PM. Evidence for the occurrence of gingival recession and non-carious cervical lesions as a consequence of traumatic toothbrushing. J Clin Periodontol. 2015;42(Suppl 16):S237–55. doi: 10.1111/jcpe.12330. [DOI] [PubMed] [Google Scholar]
- 9.Wiegand A, Attin T. Design of erosion/abrasion studies – Insights and rational concepts. Caries Res. 2011;45(Suppl 1):53–9. doi: 10.1159/000325946. [DOI] [PubMed] [Google Scholar]
- 10.Carranza FA, Camargo PM. Plaque control for the periodontal patient. In: Dorothy PA, editor. Carranza's Clinical Periodontology. St. Louis, Mo.: Saunders Saunders, An imprint of Elsevier; 2006. p. 731. [Google Scholar]
- 11.Macdonald E, North A, Maggio B, Sufi F, Mason S, Moore C, et al. Clinical study investigating abrasive effects of three toothpastes and water in an in situ model. J Dent. 2010;38:509–16. doi: 10.1016/j.jdent.2010.03.007. [DOI] [PubMed] [Google Scholar]
- 12.Cirano FR, Romito GA, Todescan JH. Determination of root dentin and cementum micro hardness. Braz J Oral Sci. 2004;3:420–4. [Google Scholar]
- 13.Wiegand A, Köwing L, Attin T. Impact of brushing force on abrasion of acid-softened and sound enamel. Arch Oral Biol. 2007;52:1043–7. doi: 10.1016/j.archoralbio.2007.06.004. [DOI] [PubMed] [Google Scholar]
- 14.Ganss C, Hardt M, Blazek D, Klimek J, Schlueter N. Effects of toothbrushing force on the mineral content and demineralized organic matrix of eroded dentine. Eur J Oral Sci. 2009;117:255–60. doi: 10.1111/j.1600-0722.2009.00617.x. [DOI] [PubMed] [Google Scholar]
- 15.Dyer D, Addy M, Newcombe RG. Studies in vitro of abrasion by different manual toothbrush heads and a standard toothpaste. J Clin Periodontol. 2000;27:99–103. doi: 10.1034/j.1600-051x.2000.027002099.x. [DOI] [PubMed] [Google Scholar]
- 16.Wiegand A, Schwerzmann M, Sener B, Magalhaes AC, Roos M, Ziebolz D, et al. Impact of toothpaste slurry abrasivity and toothbrush filament stiffness on abrasion of eroded enamel - An in vitro study. Acta Odontol Scand. 2008;66:231–5. doi: 10.1080/00016350802195041. [DOI] [PubMed] [Google Scholar]