

Abstract
Background:
Diabetes is a serious chronic disease during childhood. Because of the chronic nature of the disease, self-care is necessary. Education alone is not effective in providing care. Misunderstanding by the patients regarding diabetes during the training programs render telephone follow-up after training essential.
Materials and Methods:
This quasi-experimental study with two groups (experimental and control) was conducted in two phases in 2014. The study population consisted of 70 children of 10–18 years of age with type I diabetes (35 patients in the experimental group and 35 in the control group). The participants were randomly selected from the patients referring to the Sedigheh Tahereh Diabetic Research and Treatment Center in Isfahan, Iran. Data were collected using a researcher-made questionnaire on self-care and a glycosylated hemoglobin recording form. The experimental group received 12 weeks of telephone follow-up training by the center, whereas the control group received no follow-up.
Results:
The results showed that, after intervention, the total mean score of self-care in all aspects of diabetes care for children was significantly higher in the experimental group (p < 0.001). In addition, a statistically significant difference was observed between the experimental and control groups in terms of mean glycosylated hemoglobin after the intervention (p = 0.030).
Conclusions:
It can be concluded that telephone follow-up by a nurse can improve total self-care and glycosylated hemoglobin in patients with type I diabetes.
Keywords: Children, glycosylated hemoglobin, Iran, nurses, self-care, telephone follow-up, type 1 diabetes mellitus
Introduction
Each year, approximately 13000 children under 18 years of age are diagnosed with type I diabetes mellitus (DM), and this is the fifth leading cause of death in most countries.[1] The majority of young people are at risk of medical complications including diabetic ketoacidosis, neuropathy, and nephropathy,[2] hyperosmolar nonketotic coma, and hypoglycemia.[1] Pathogenesis and mortality due to these complications are considered as major health-care issues in the world.[3] The objective of encouraging self-care is to increase control and sense of responsibility for self-care management among patients with diabetes.[1] Panagioti et al. found Self-management support interventions to reduce health care utilisation without compromising outcomes.[4]
According to the World Health Organization (WHO), education is the basis and foundation of diabetes treatment, however, that alone will not lead to improvement of glycemic control; follow-up is essential for diabetic patients because wrong understanding of the disease among people with diabetes following training is common.[5,6] Therefore, implementing a follow-up program, in addition to strengthening knowledge, will help the development of attitudes and increase adherence to self-care behavior.[7] Given the high and growing prevalence of diabetes and the importance of its long-term follow-up, an inexpensive and applicable method which can be used for a large number of clients is needed.[5,6] Today, one of the methods for continuous control of diabetic patients is the promotion of self-care and the use of new technologies[6] such as telenursing. Telenursing is a tool for providing ongoing care for patients with chronic conditions.[5] Through creating an extensive connection between the patient and the hospital, telenursing leads to implementation of continuous care and maintenance of the well-being of patients.[2]
The study by Zolfaghari et al. aimed to evaluate the effectiveness of follow-up by nurses through telephone calls and short message services (SMS) on adherence to treatment.[8] They showed a significant difference in the rate of adherence to the diabetes treatment regimen (physical activity, diabetes medication, and diet) in patients with diabetes (p = 0.001) and a significant reduction in the amount of glycosylated hemoglobin in the follow-up group (0.93%).[8] In a randomized controlled trial, a 2.9 and 2% decrease in glycosylated hemoglobin was, respectively, observed in the test and control groups in patients with diabetes type 1 or 2 in the age group of 18 years.[9] However, this difference was not statistically significant (p = 0.455).[9] Ongoing relationships with patients, after visiting them at home, have a very important role in controlling diabetes. Studies on adults have illustrated that telephone follow-up by nurses with an effective plan to improve self-care, control blood sugar, and reduce symptoms in patients with diabetes showed favorable results. It seems that very little research in this area has been conducted on children. No follow-up was performed at the Sedigheh Tahereh Diabetic Research and Treatment Center, Isfahan, Iran, following the given instructions. Because diabetes is a chronic disease and given the critical situation of children because of exposure to peer groups at school, the researcher found telephone follow-up by the center after training to be imperative.
Materials and Methods
This quasi-experimental study with two groups (experimental and control) was performed in two stages in 2014. The study population consisted of children with type I diabetes in the age group of 10 to 18 years who were admitted to the Sedigheh Tahereh Diabetic Research and Treatment Center. With a 95% confidence interval and 84% statistical power, the number of participants for each group was calculated to be 35. The inclusion criteria included being a resident of Isfahan (Iran), in the age range of 10 to 18 years, diagnosed with type I diabetes at least 6 months prior to the study, having access to landline at home, not having any physical and mental problems or other chronic diseases, and not having experienced any stressful events at least 1 month prior to the study. The exclusion criteria included hospitalization, unwillingness to continue the study, occurrence of diabetic ketoacidosis or hyperosmolar hyperglycemic nonketotic syndrome, and experience of stressful events during the study. The participants were selected through random sampling method. After the approval of the ethics committee, the researcher visited the center and referred to the medical history files of patients with type I diabetes and prepared a list of patients who were covered by the center. Then, the participants were selected by a random draw from the mentioned list. Data were collected using a researcher-made questionnaire on self-care and a glycosylated hemoglobin recording form. The questionnaire consisted of three parts. The first part included 13 questions regarding demographic characteristics and the second part consisted of 4 questions on the disease. The third part included 43 questions related to self-care and incorporated 8 dimensions of self-care regarding the individual aspects. To determine the scientific validity and reliability of the tools, content validity and test–retest methods were used. The reliability coefficient of 0.95 was obtained. Data were collected through self-reporting by the child and measurement of glycosylated hemoglobin. Data gathering was performed at the time of enrollment and 12 weeks after the intervention. After registering the qualified candidates and obtaining the consent of their primary caregiver, questionnaires were completed by the children. Without the need for fasting, venous blood samples were taken to measure glycosylated hemoglobin. (The measurement of the glycosylated hemoglobin of all samples was performed in a laboratory using a Hitachi Autoanalyzer and Pars A1C kits). After this stage, the participants were assigned randomly to two groups of control and experimental, and the telephone intervention was implemented in the experimental group for 12 weeks. Phone calls were made by the researcher twice per week in the first month and once a week during the second and third months. The duration of the conversation was an average of 20 min. The content of the conversations included following up on the training provided by the center in connection with problems related to diabetes, obtaining each patient's specific complaints, analyzing the situation with the patient's assistance to determine the problem and finally providing a solution to the problem. Patients' questions were answered with regard to the level of their development, and the importance of implementing the methods taught was emphasized at the end of the conversation. In addition, the content of each conversation was recorded in a form consisting of two parts. The first part included the common problems of patients with diabetes and provided the necessary advice (on exercise, diet, insulin, etc.), and the second part was devoted to the specific needs of each client. In each session of the conversation, the needed guidance was provided and the content of the conversation was written in the forms. It is noteworthy that during the intervention period, the control group received training only from the center. Data were analyzed using the Statistical Package for the Social Sciences software (version 16, SPSS Inc., Chicago, IL, USA).
Ethical considerations
Researchers at all stages of the research paid careful attention to ethical principles. All the parents and children were given verbal and written information about the purpose and importance of the study. Written, informed consent was obtained from the parents of children before they completed the first questionnaire and they were free to withdraw from the study at any time.
Results
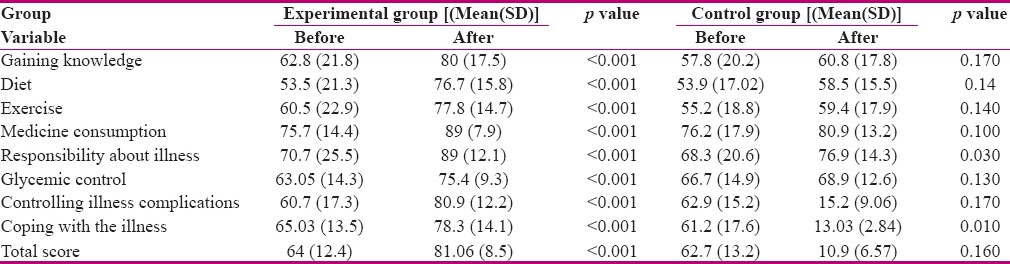
Participants in the two experimental and control groups were similar in terms of all demographic characteristics, clinical data, self-care, and baseline glycosylated hemoglobin levels [Tables 1 and 2]. Mean glycosylated hemoglobin reduced by 14% in the experimental group (before the intervention: 10.4%, after the intervention: 8.64%). In the control group, mean glycosylated hemoglobin (before the intervention: 9.92, after the intervention: 9.44) reduced by 0.48%. Paired t-test showed a statistically significant difference between the mean glycosylated hemoglobin before and after the intervention in the experimental group (p = 0.001). However, this difference was not statistically significant in the control group (p = 0.100). Independent t-test showed a statistically significant difference between experimental and control groups in terms of mean glycosylated hemoglobin after the intervention (p = 0.030) [Table 3]. In this study, the mean self-care score increased by 17.06% in all the dimensions in the experimental group (before the intervention: 64, after the intervention: 81.06). In the control group, mean self-care score (before the intervention: 62.7, after the intervention: 65.6) increased by 2.9%. Paired t-test showed a statistically significant difference between the mean self-care score before and after the intervention in the experimental group (p < 0.001). Nevertheless, this difference was not statistically significant in the control group (p > 0.050). The independent t-test showed that there were no significant differences between the two groups regarding the mean score of self-care before the intervention (p > 0.050) [Table 4].
Table 1.
Demographic characteristics of the participants in the experimental and control groups before the study
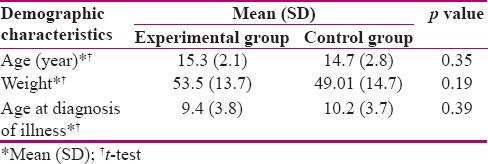
Table 2.
Comparison of the characteristics of the disease in patients in the experimental and control groups before the study
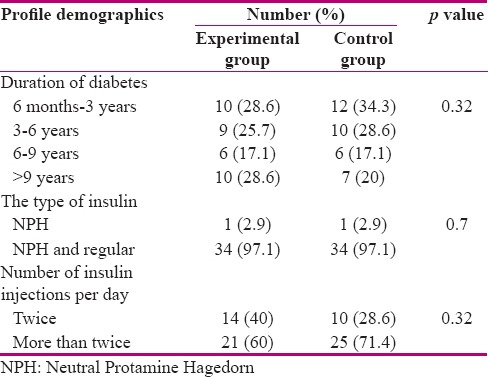
Table 3.
Comparison of HbA1C values before and after the intervention in the experimental and control groups

Table 4.
Comparison of the self-care score in different aspects before and after the intervention in the experimental and control groups
Discussion
The results showed significant differences in the mean score of self-care in all aspects (obtaining information, diet, exercise, medications, accountability, blood sugar control, disease symptoms control, coping with illness) and mean glycosylated hemoglobin in experimental and control groups after 12 weeks of telephone follow-ups. The effectiveness of long-distance follow-up methods on strengthening the self-care support system in type II diabetes has been confirmed.
The media used in the present study was telephone that is the most widely used, most accessible, and cheapest of the methods. The main advantage of telephone follow-up was the ability to strengthen behaviors and create more consistency in the treatment without the patients having to visit the clinics.[10] In the study by Parizad et al., follow-up by telephone and SMS led to a significant improvement in self-care, adherence to diet, physical activity, self-monitoring of blood glucose, medication adherence, and foot care in patients with type II diabetes in the age group of 18 to 55 years.[11] They also showed a significant decrease in mean glycosylated hemoglobin score in the experimental group after the intervention.[11] These results were consistent with the results of the present study. Lorig et al. evaluated the effect of nursing telephone follow-up on promoting self-care among adolescents with diabetes type II.[12] They showed a significant improvement in patients' self-care; 6 months of telephone follow-up led to improved self-monitoring of blood glucose in the experimental group, and the difference between the two groups was significant. Furthermore, the experimental group showed a significant difference in glycosylated hemoglobin, health disorder, symptoms of hypoglycemia and hyperglycemia, and self-effectiveness compared to the control group.[12] The results of this study were consistent with results of the study by Lorig et al.,[12] with the exception that in the present study, type I diabetes, which is the most common and most serious chronic disease of childhood and adolescence, and self-care as the basis for the prevention of disease complications were considered.
Peimani et al. in a quasi experimental study evaluated research Effectiveness of short message service-based intervention (SMS) on self-care in type 2 diabetes.[13] The result of this study showed that after 12 weeks, although HgA1c levels did not significantly change, significant decline was observed in FBS and mean BMI in both intervention groups. The results of the present study were similar to that of this study, but in the present study, 1 index for self care was assessed and HbA1c was reduce in experimental group.[13] Tavsanli et al. examined blood sugar control and consultation with visual phones.[14] Their findings showed that glycosylated hemoglobin level had reduced in the intervention group after 3 months.[14] The abovementioned study investigated the effect of counseling by telephone on the glycosylated hemoglobin index, whereas the impact of follow-up on self-care was studied in the present study and the glycosylated hemoglobin index was used for the reliability of the results. Bell et al. investigated the support of self-care, healthy diet, active lifestyle, and self-monitoring in patients with type II diabetes.[15] The findings showed a significant difference in glycosylated hemoglobin between the two groups.[15] The results of this study were in line with the present study. However, the studied population included the age group of over 18 years, which was different from the study population of the present study.
Self care is an essntial element in treating a person with diabetes; and maneging diabets is of prime importance.the aim study eas to investigate the pedictors of adherence to self-care behavior among women with type 2 diabetes.[16] The study by karimy et al. showed the multiple regression models revealed 59.9% of the variance of self-care behavior with self efficacy, perceived barrier, benefit and susceptibiity performance improvements in self-care, mean fasting blood sugar, and body mass index in patients with type II diabetes.[16] Their results were similar to the results of the present study. Their intervention was performed through the use of a training website, however, in the present study, the follow-up was conducted by telephone. Aliha et al. found that after 12 weeks of telephone follow-up, adherence to treatment had increased by 83.8% and glycosylated hemoglobin level had decreased by 1.4% in the experimental group.[7] Piette et al. observed higher blood sugar control, foot care, and weight management, and that fewer problems regarding medication had occurred in the experimental group.[17] However, no significant changes were observed in glycosylated hemoglobin compared to before the intervention, which was inconsistent with the findings of the present study.[17] This discrepancy in the results can be explained as the result of the difference in the age group, the study population size, and the duration of follow-up between the two studies.
Lehmkuhl et al. observed a reduction in the glycosylated hemoglobin level in both study groups of children of 9–17 years of age with type I diabetes, however, this reduction was not statistically significant. This may be due to the study's low sample size; the participants consisted of 32 teenagers.[2] The overall objective of encouraging individuals to perform self-care was to gain more control and responsibility.[1]
Limitations to the present study were the participants may have received education from other sources in addition to the educational program of the present study, and their interest and psychological state may have affected their responses.
Conclusion
The results of the current study showed that telephone follow-up by a nurse increased the mean scores of self-care in children with diabetes. The results of this study can help managers in planning and guiding nurses in effective training of patients with diabetes. In addition, this method is more effective and convenient for patients who cannot refer to treatment centers due to the geographical aspect. Moreover, a large number of patients in a wide range of geographical areas could be trained by this method.
Financial support and sponsorship
Isfahan University of Medical Sciences, Isfahan, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
This article was extracted from the final thesis of a graduate student with project number 93014. Our sincere appreciation goes to the Sedigheh Tahereh Endocrinology and Metabolism Research Center affiliated to Isfahan University of Medical Sciences, the research deputy, the study participants, parents, and all the professors who contributed to the preparation of this study.
References
- 1.Meerabeau L, Wright K. Long-term conditions nursing care and management. 1st ed. Blackwell Publishing Ltd; 2011. pp. 119–120.pp. 247pp. 271 [Google Scholar]
- 2.Lehmkuhl HD, Storch EA, Cammarata C, Meyer K, Rahman O, Silverstein J, et al. Telehealth behavior therapy for the management of type 1 diabetes in adolescents. J Diabetes Sci Technol. 2010;4:199–208. doi: 10.1177/193229681000400125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.World Health Organization and International Diabetes Federation. Diabetes action now: An initiative of World Health Organization International Diabetes Federation. [Last accessed on 2012 May 02]. Available from: http://www.who.int/entity/diabetes/actionnow/en/consultation .
- 4.Maria P, Gerry R, Nicola S, Elizabeth M, Anne R, Anne K, et al. Self-management support interventions to reduce health care utilisation without compromising outcomes: A systematic review and meta-analysis. BMC Health Services Research. 2014;14:356. doi: 10.1186/1472-6963-14-356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kawaguchi T, Azuma M, Ohta K. Development of a telenursing system for patients with chronic conditions. J Telemed Telecare. 2004;10:239–44. doi: 10.1258/1357633041424395. [DOI] [PubMed] [Google Scholar]
- 6.Pena V, Watson AJ, Kvedar JC, Grant RW. Mobile phone technology for children with type 1 and type 2 diabetes: A parent survey. J Diabetes Sci Technol. 2009;3:1481–9. doi: 10.1177/193229680900300630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Aliha JM, Asgari M, Khayeri F, Ramazani M, Farajzadegan Z, Javaheri J. Group education and nurse-telephone follow-up effects on blood glucose control and adherence to treatment in type 2 diabetes patients. Int J Prev Med. 2013;4:797–802. [PMC free article] [PubMed] [Google Scholar]
- 8.Zolfaghari M, Mousavifar A, Pedram S, Haghani H. The impact of nurse short message services and telephone follow-ups on diabetic adherence: Which one is more effective? J Clin Nurs. 2011;21:1922–31. doi: 10.1111/j.1365-2702.2011.03951.x. [DOI] [PubMed] [Google Scholar]
- 9.Wong FK, Mok MP, Chan T, Tsang MW. Nurse follow-up of patients with diabetes: Randomized controlled trial. J Adv Nurs. 2005;50:391–402. doi: 10.1111/j.1365-2648.2005.03404.x. [DOI] [PubMed] [Google Scholar]
- 10.Wu L, Forbes A, Griffiths P, Milligan P, While A. Telephone follow-up to improve glycaemic control in patients with Type 2 diabetes: Systematic review and meta-analysis of controlled trials. Diabetic Med. 2010;27:1217–25. doi: 10.1111/j.1464-5491.2010.03113.x. [DOI] [PubMed] [Google Scholar]
- 11.Parizad N, Hemmati Maslakpak M, Khalkhali HR. Promoting Self-Care in Patients with Type 2 Diabetes: Tele-Education. Hakim Res J. 2013;16:220–7. [Google Scholar]
- 12.Lorig K, Ritter PL, Villa F, Piette JD. Spanish Diabetes Self-Management With and Without Automated Telephone Reinforcement Two randomized trials. Diabetes Care. 2008;31:408–14. doi: 10.2337/dc07-1313. [DOI] [PubMed] [Google Scholar]
- 13.Peimani M, Rambod C, Omidvar M, Larijani B, Ghodssi-Ghassemabadi R, Tootee A, et al. Effectiveness of short message service-based intervention (SMS) on self-care in type 2 diabetes: A feasibility study. Prim Care Diabetes. 2016;10:251–8. doi: 10.1016/j.pcd.2015.11.001. [DOI] [PubMed] [Google Scholar]
- 14.Tavşanlı NG, Karadakovan A, Saygili F. The use of videophone technology (telenursing) in the glycaemic control of diabetic patients: A randomized controlled trial. J Diabetes Res Clin Metab. 2013;2:1–7. [Google Scholar]
- 15.Bell AM, Fonda SJ, Walker MS, Schmidt V, Vigersky RA. Mobile phone-based video messages for diabetes self-care support. J Diabetes Sci Tech. 2012;6:310–9. doi: 10.1177/193229681200600214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Karimy M, Araban M, Zareban I, Taher M, Abedi A. Determinants of adherence to self-care behavior among women with type 2 diabetes: An explanation based on health belief model. Med J Islam Repub Iran. 2016;30:368. [PMC free article] [PubMed] [Google Scholar]
- 17.Piette JD, Weinberger M, Kraemer FB, McPhee SJ. Impact of automated calls with nurse follow-up on diabetes treatment outcomes in a Department of Veterans Affairs Health Care System: A Randomized Controlled Trial. Diabetes Care. 2001;24:202–8. doi: 10.2337/diacare.24.2.202. [DOI] [PubMed] [Google Scholar]