

Abstract
Context:
Different types of breathing exercises have varied effects on cardiovascular parameters and the stress levels in an individual.
Aim:
The aim of this study was to assess the effect of a modified form of isolated alternate nostril, slow breathing exercise on perceived stress, and cardiovascular parameters in young, male volunteers.
Settings and Design:
This was a randomized control study carried out at Advanced Centre for Yoga Therapy Education and Research, Department of Physiology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry in 2014.
Subjects and Methods:
Hundred healthy male volunteers were randomized into control group, n = 50 and slow breathing group (study), n = 50. Slow breathing exercise training was given to study group for 30 min a day, 5 times/week for 12 weeks, under the supervision of certified yoga trainers. Perceived Stress Scale (PSS) using Cohen's questionnaire, anthropometric parameters such as body mass index (BMI), waist-hip ratio (WHR), and cardiovascular parameters such as heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were recorded at baseline and after 12 weeks. The control group did not receive any intervention. Slow breathing exercise training was provided for the study group. During the study period, one volunteer opted out of the study group due to personal reasons.
Results:
HR, SBP, DBP, and PSS decreased significantly (P < 0.05) in the study group following 12 weeks slow breathing exercise training, while no significant change (P > 0.05) was observed in BMI and WHR. There was no significant change in the control group.
Conclusion:
Twelve weeks of modified slow breathing exercise reduced perceived stress and improved the cardiovascular parameters. The above results indicate that our modified slow breathing exercise is effective in reducing stress and improving the cardiovascular parameters.
Keywords: Blood pressure, heart rate, perceived stress, slow breathing exercise
Introduction
Yoga is a physical, mental, and spiritual discipline that includes different practices. The purpose of yoga is to improve the physical and psychological health and bring about an inner harmony.[1,2] Pranayama is the fourth limb of Ashtanga yoga out of a total of eight limbs mentioned by Patanjali. Pranayama is a Sanskrit word meaning “extension of life force.” “Prana” means life force which is the breath we inspire and “ayama” means to regulate or lengthen. Pranayama is the control of prana through the breath. Prana, as mentioned in vedic scriptures, is the universal cosmic energy. The science of pranayama deals with the monitoring and enrichment of this universal energy, which results in a relaxed but alert state of mind.
The great Indian seer Patanjali belonging to 200 BC with his in-depth understanding and vast knowledge of yoga has defined pranayama as a “regulation of the incoming and outgoing flow with retention of breath.”[3] Conscious guiding of breath gives rise to an increase in vitality, physical detoxification as well as an improvement in immunity. It also helps in the attainment of relaxation, inner peace, and clarity of mind.
There are different methods of pranayama varying from single nostril breathing to alternate nostril breathing. It consists of three phases: “Purak (inhalation), Kumbhaka (retention), and Rechak (exhalation). These three phases can be practiced in either slow or fast manner.[4] The physiological effects produced vary on the type of pranayama performed.[5,6,7] Studies report that slow and fast types of pranayama have different physiological effects in healthy subjects.[5] Furthermore, pranayama has a variable effect on cardiac and pulmonary function parameters.[8]
Slow and deep breathing is efficient as it reduces the ventilation in the dead space of the lungs. Shallow breathing replenishes air only at the base of the lungs in contrast to deep breathing that replenishes the air in all parts of the lung.[6] It decreases the effect of stress and strain on the body by shifting the balance of the autonomic system predominantly toward the parasympathetic system and improves the physical and mental health.[9,10]
Many researchers have found pranayama to be beneficial in treating stress-related disorders. Retention of breath also known as Kumbhaka enhances the level of vital energy in the body. The effects of pranayama, when practiced with kumbhaka, are substantially more than pranayama practiced alone.
Conventional anuloma viloma pranayama with inhalation, breath holding, and exhalation in the ratio of 1:4:2 is an advanced method not suitable for beginners, and the increased duration of kumbhaka can lead to harmful effects.[11] The prolonged phase of breath holding practiced in anuloma viloma pranayama is hard to practice for beginners and also not suitable for individuals with various health problems due to the inherent risk of cerebral hypoperfusion associated with breath holding for a prolonged period. Samvartti pranayama which involves equal phases of inhalation, exhalation, and breath retention is a simple technique recommended for beginners and persons with “Vata” imbalance.[12]
The slow, deep breathing exercise carried out in our study, was a modified form of anuloma viloma pranayama (alternate nostril breathing), with equal phases of inspiration, breath holding, and expiration (1:1:1 ratio).
Subjects and Methods
After obtaining approval from Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER) Scientific Advisory Committee and Human Ethics Committee, we recruited 100 healthy volunteers for our study. Subjects were selected based on the inclusion and exclusion criteria mentioned below. They were motivated to enroll for the study by explaining the benefits of slow breathing exercise.
Inclusion criteria
Healthy male volunteers in the age group of 18–30 years were included in the study.
Exclusion criteria
Individuals who are unable to perform breathing exercise due to reasons such as nasal pathology including deviated nasal septum, sinusitis and those with a history of chronic respiratory disease, cardiac disorders, diabetics, hypertensives, smokers, alcoholics, and athletes were excluded from the study.
Methodology
The total number of subjects recruited in this randomized control study was 100. The enrolled subjects were divided equally into control and study groups using simple randomization technique (random numbers generated using computer software). The control and study group consisted of 50 volunteers each. During the study, one volunteer opted out of the study group due to personal reasons, but there were no dropouts in the control group. At the end of 12 weeks of study, there were 49 volunteers in the study group and 50 volunteers in the control group.
We recorded the baseline parameters before the start of slow breathing exercise training. The subjects were advised to come at least 1 h after light breakfast and with light clothing. They were instructed not to perform any intensive exercise and avoid taking any hot or cold beverage, 30 min before the recording of parameters. We recorded the following parameters,
Anthropometric parameters
Height
It was measured by a wall-mounted stadiometer (Easy Care, Hong Kong).
Weight
It was measured using a digital weighing machine (Charder, Taiwan) with an error of 0.1 kg. The accuracy of the machine was checked routinely with other weighing machines available.
Body mass index
It was calculated using the height and weight measurements.
Waist-hip ratio
It was measured using an inch tape at the end of normal inspiration. Waist measurements were taken at the level of the umbilicus, and hip measurement was taken at the widest part of the buttocks.
Basal cardiovascular parameters
The subjects were made to lie down on a couch in the supine posture. After 10 min of supine rest heart rate (HR) (beats/minute), systolic blood pressure (SBP) and diastolic blood pressure (DBP) (mmHg) were measured using digital BP monitor (Citizen - CH 432B, Japan).
Perceived stress questionnaire (PSS)
The subjects were asked to sit comfortably in a chair, and the PSS printout was handed out to them. The subjects were instructed to read the questions at least twice before answering. They were asked to circle or tick the option which they felt was the appropriate response to the question provided. The subjects were invited to complete the entire set of 10 questions at a time and were not allowed to discuss among them.
The perceived stress questionnaire is an invaluable addition to the psychosomatic researcher's repository. Perceived Stress Scale (PSS) is used widely as an instrument for measurement of perceived stress. It gives us a measure of the degree to which a person feels a situation as stressful. The questions are not specific to any group of the population and are general in nature. They are simple, easy to understand and the responses can be easily grasped. The questionnaire is related to the feelings, emotions, and thoughts of the subject during the past month. The PSS can be administered within minutes, and the answers are easy to score, making it an economical method of assessing the subjective stress. The PSS consists of questions mostly related to the current levels of stress. It has been found that the PSS-10 questionnaire is a reliable and valid tool for assessing the stress perceived by students attending college.[13] It is inversely related to the emotional stress which is perceived by the subject.
Modified slow breathing exercise training
The control group did not undergo any form of breathing exercise. The study group was given slow breathing exercise training under the guidance of a trained, certified yoga instructor at the Advanced Centre for Yoga Therapy, Education and Research (ACYTER), JIPMER. Practice sessions were conducted 5 days/week in the morning for 30 min under our direct supervision and subjects were motivated to practice the same at their home daily on other days. Pranayama training was given for a total duration of 12 weeks. Attendance register was maintained for yoga training sessions, and the data were obtained only from subjects whose attendance was at least 80%.
The technique of modified slow breathing exercise
Anuloma viloma pranayama is a form of slow, rhythmic, alternate nostril breathing. Traditional anuloma viloma consists of inhalation, kumbhaka, and exhalation in the ratio of 1:4:2. Our slow breathing exercise is a modified version of the anuloma viloma pranayama in the ratio of 1:1:1, which was standardized by Pal et al. The breathing exercise training was given in a well-ventilated room, and it was ensured that there was no nasal obstruction before the start of breathing exercise. Breathing exercise was performed under the supervision of a trained instructor at the Yoga Center, and the count duration was maintained with the help of a metronome.
The right nostril is blocked with the aid of right thumb, and air is breathed in through the left nostril slowly for a count of 6 secs. Then, with the help of right index finger, the left nostril is also blocked (both nostrils closed), and the breath is held for a count of 6 secs. Now the right thumb is released from the right nostril, and air is breathed out for a count of 6 secs.
Air is breathed in again for a count of 6 secs through the right nostril which is still open. Then, the right nostril is also blocked with the right thumb (both nostrils closed) and breath is held for a count of 6 secs. Now, the left nostril is opened by releasing the right index finger, and the air is breathed out for a count of 6 secs, thus completing one cycle [Figure 1].
Figure 1.
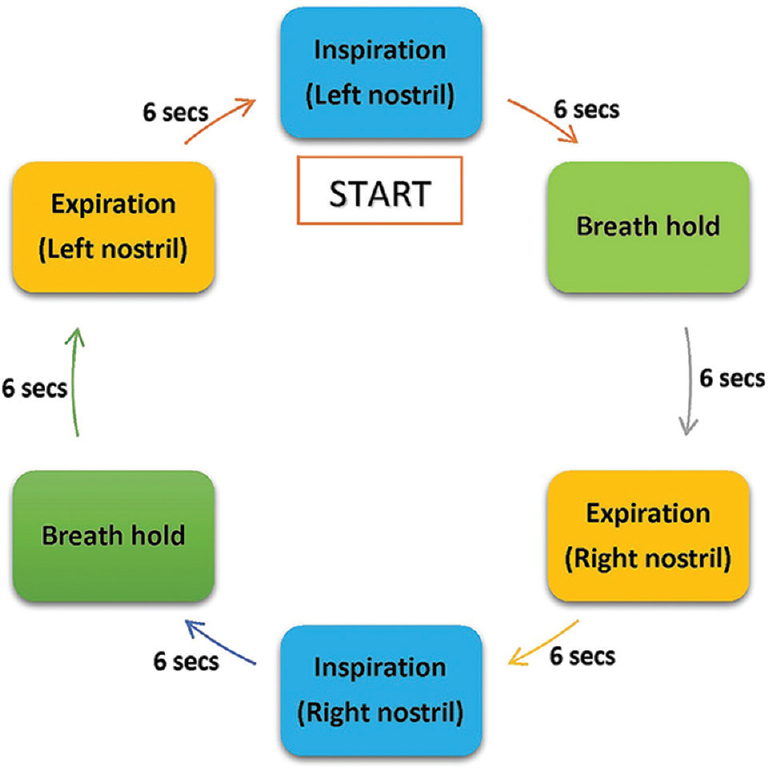
Schematic overview of a single cycle of modified, alternate nostril, slow breathing exercise
The cycle has to be repeated for 30 min. A rest of 5 min will be provided in between after 15 min of the practice session. The instructor at the ACYTER center counts from 1 to 6, and the volunteers follow accordingly. The components of this slow breathing exercise are depicted in Figure 1.
All these together constitute one complete cycle and the total time for one cycle is 36 s. The duration of inspiration, expiration, and the breath holding time is equal. The cycle starts with inspiration through the left nostril and ends with expiration through the same left nostril. All the parameters were again recorded after 12 weeks of slow breathing exercise, and statistical analysis of data was performed.
Statistical analysis
Data were summarized using descriptive statistics such as mean and standard deviation for all the recorded parameters. The normality of the continuous data was tested using Kolmogorov–Smirnov test. The comparison of anthropometric, basal cardiovascular parameters, and PSS between the control and study group was carried out using an unpaired t-test.
The intragroup comparison of anthropometric, basal cardiovascular parameters and PSS was carried out using paired t-test.
Results
A total of 100 volunteers were recruited for the study and divided equally into 50 in study and 50 in control group using simple randomization technique. One volunteer opted out of the study group due to personal reasons. The control group did not undergo any intervention whereas the study group underwent 12 weeks of modified slow breathing exercise.
The baseline anthropometric, cardiovascular parameters and stress score between the control and study group showed no significant difference [Table 1]. Hence, they can be considered comparable to the present study. After 12 weeks of slow breathing exercise, the changes in body mass index (BMI) and waist-hip ratio were statistically significant, but the reduction in the mean values do not appear to be clinically significant (0.16 kg/m2, 0.003) in the day-to-day life [Table 2].
Table 1.
Comparison of baseline parameters between the control and study group
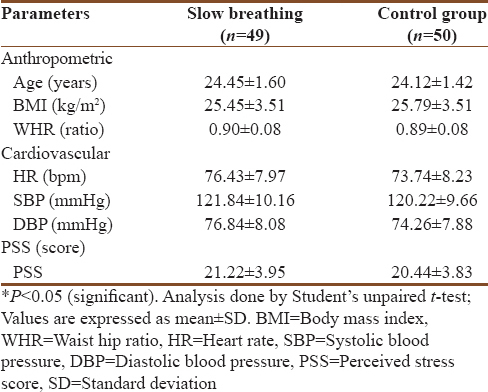
Table 2.
Comparison of parameters before and after 12 weeks of slow breathing exercise in the study group
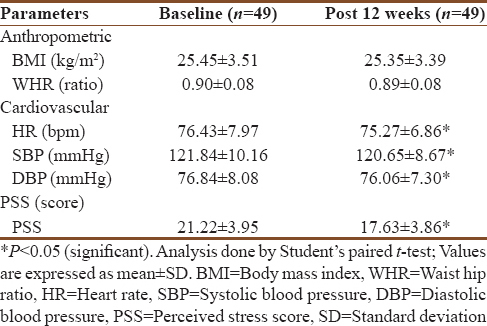
There was a significant reduction in HR from baseline compared to the control group. The SBP and DBP values following 12 weeks of slow, deep breathing exercise also showed a statistically significant reduction, but the marginal reduction in blood pressure seems to be clinically insignificant [Table 2].
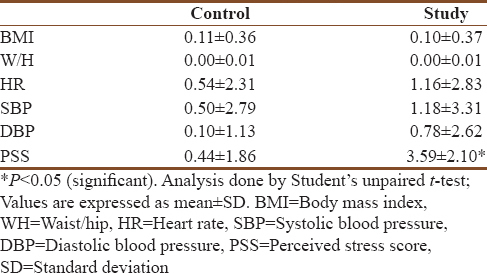
The reduction in PSS achieved following the practice of slow, deep breathing exercise for 12 weeks was extremely significant [Table 2]. The magnitude of change (delta change) of the Perceived Stress Score in the study group was significant compared to that of the control group [Table 3].
Table 3.
Comparison of magnitude of change (delta) in control and study group
Discussion
Stress is considered to be a state, where the emotional and psychological component ceases to be in harmony with the physical component of health. The effects of stress are not only limited to the psychological component but also extends its wings to affect the physiological aspect of wellbeing, by altering the levels of various hormones.[14] The 10-item Perceived Stress Scale (PSS-10) is a popular Likert type rating scale developed to quantify the psychological construct “perceived stress.”[15]
The breath we take acts as a connecting bridge between the mind and body and pranayama serves as a tool to manipulate the bridge. “Pranayama consists of three phases: Purak (inhalation), Kumbhaka (retention), and Rechak (exhalation) that can either be practiced in a slow or fast manner.”[4] The various physiological and psychological effects of pranayama are believed to be due to the difference in the duration of different breath cycles. It also depends on the amount of involvement of the usage of mouth, nostrils, laryngeal muscle constriction, glottis position, and the tidal capacity of that particular individual.[16]
The slow, deep breathing carried out in our study was a modified form of anuloma viloma pranayama standardized by Pal et al.,[7] with equal phases of inspiration, breath holding, and expiration (1:1:1 ratio).
There was a significant reduction in HR, SBP, and DBP following the practice of 12 weeks of slow deep breathing exercise. Resting HR is primarily determined by the parasympathetic tone and a decrease in HR and BP indicates a shift toward parasympathetic activity or a decrease in sympathetic activity.[17,18] When the mind is at rest, and in a relaxed state, the parasympathetic activity predominates, and the peripheral vascular resistance decreases. This increase in parasympathetic activity leads to a decrease in resting HR and a reduction in the sympathetic tone in the blood vessels of skeletal muscles, thereby decreasing the peripheral vascular resistance and bringing about a reduction in DBP.
The decrease in SBP might have been due to the reduced responsiveness of end organs to circulating noradrenaline, following relaxation by slow breathing exercise.[19] Although the pre- and post-values of HR, SBP, and DBP showed a statistically significant reduction, the magnitude of reduction (delta change) of HR, SBP, and DBP was not statistically significant in both the control and study group. The above results emphasize the fact that the small reduction achieved in the above parameters is not considered significant in a clinical scenario despite the statistical significance achieved. Whether a further increase in the duration of pranayama of more than 12 weeks would have led to both a statistical and clinically significant reduction in the magnitude (delta change) of the above parameters, is yet to be seen.
In our study, 12 weeks of slow, deep breathing exercise showed a very significant reduction (P < 0.0001) in the perceived stress score (PSS) from 21.20 ± 3.96 to 17.20 ± 2.84, which is in agreement with previous studies showing similar results.[20,21] The magnitude of change (delta) of PSS in the study group was both statistically and clinically significant, indicating the effectiveness of the slow, breathing exercise in alleviating stress. The postulated mechanism by which pranayama causes a reduction in stress, is by a decrease in the levels of serum cortisol and also by a direct reduction of sympathetic activity creating a dominance of the parasympathetic tone. Decreased cortisol levels are associated with an increased feeling of well-being, reduction in anxiety, and an increased threshold for stress perception.[22]
Slow breathing exercise as a part of yoga alleviates stress and revamps the antioxidant status of the individual.[23] The practice of pranayama is associated with increased vigor and has a positive effect on the mood. It can be used as a self-restraint technique for stabilizing various effective states in an individual.[24]
The modified slow breathing exercise practiced in our volunteers was effective in reducing the perceived stress. Although studies involving alternate nostril, slow breathing exercise have shown similar results on perceived stress, they mostly involved a longer duration of breath holding when compared to inhalation and exhalation. Our modified method includes a uniform and equal phases of breath holding in the ratio of 1:1:1.
Breath holding, when practiced improperly for longer periods, can lead to severe brain damage resulting from the anoxia and requires supervised practice under a trained instructor. Furthermore, there lies a practical difficulty in remembering the unequal ratio (1:4:2) during practice by illiterate subjects. The equal ratio (1:1:1) of breathing practiced in our study alleviates the extra focus needed to concentrate on the unequal breathing ratio (1:4:2) in traditional Anuloma viloma pranayama, thereby enabling the subject to focus more on the breathing rather than on the ratio of breathing.
Yogic literature advice a subject to start with inhalation and exhalation without breath holding, at least for 2 months and then gradually incorporate breath holding with inhalation and exhalation. This emphasizes the difficulty associated with breath holding in the beginners of pranayama practice. The benefits of breath holding are delayed by at least one month or two due to the above reason. The equal ratio of inhalation, exhalation, and breath holding in our study makes it easier for the beginners to practice and attain the benefits of breath holding right from the onset.
Our results indeed indicate the benefit of simplified, uniform ratio, alternate nostril, slow breathing exercise in alleviating stress and the results are similar to that of traditional anuloma viloma pranayama but without the difficulty associated with different ratios and prolonged breath holding time.
However, the effectiveness of our modified breathing exercise in reducing blood pressure and BMI to a clinically significant level is debatable. Hence, further studies are needed which incorporates a longer duration of the intervention period to see whether any clinically significant result can be achieved in the blood pressure and anthropometric parameters.
Conclusion
A multitude of breathing exercises and yogic asanas have been in use to achieve a significant reduction in stress acquired by the hectic and imbalanced lifestyle. However, a single and uncomplicated tool suitable for beginners and individuals with health ailments is the need of the hour. Our modified breathing exercise is a single, simple yet an effective tool in reducing the stress levels which could be practiced by everyone ranging from the untrained to the well-trained individual. Hence, it may be stated that the modified form of slow breathing exercise with an equal ratio of inhalation, breath holding, and exhalation adopted by us is effective in reducing the levels of stress and a concomitant decrease in the perceived stress score (PSS). There were no noticeable side effects observed during the practice of modified slow breathing exercise and there was good subject compliance.
Limitations and future scope
In our randomized control study, double-blinded conditions could not be attempted which could provide a potential rater bias. Although a medical history was obtained from all the subjects, our study did not exclude any psychological conditions as it requires a detailed evaluation of the subject. However, as an added advantage, it allowed us to see the effect of our modified breathing exercise on the psychological ailments if any existed. Our aim was to assess the effect of modified slow breathing exercise on stress, regardless of the cause of stress. The biochemical parameters for assessing stress levels such as serum cortisol, vanillylmandelic acid, metanephrine, interleukin-6, thiobarbituric acid reactive substances could have provided a more objective measure of stress, which we could not incorporate in the present study. Hence, future studies can be conducted ensuring double-blinded conditions with the inclusion of biochemical parameters for a more accurate evaluation of stress. Furthermore, the study period of breathing practice could be extended more than 12 weeks to see if any clinically significant results could be obtained with respect to blood pressure and BMI. A battery of tests to exclude preexisting psychological disorders can be done.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
I sincerely thank yoga instructor Sri. Dayanidy G for providing expert slow breathing training. I also thank all the technical staff who have extended their support throughout the duration of my project. I extend my deepest gratitude to the director of JIPMER for his support.
References
- 1.Madanmohan T, Mahadevan SK, Balakrishnan S, Gopalakrishnan M, Prakash ES. Effect of six weeks yoga training on weight loss following step test, respiratory pressures, handgrip strength and handgrip endurance in young healthy subjects. Indian J Physiol Pharmacol. 2008;52:164–70. [PubMed] [Google Scholar]
- 2.Khalsa SB. Yoga as a therapeutic intervention: A bibliometric analysis of published research studies. Indian J Physiol Pharmacol. 2004;48:269–85. [PubMed] [Google Scholar]
- 3.Vivekanand S. Patanjali's Yoga Sutras. 1st ed. New Delhi: Solar Books; 2015. p. 144. [Google Scholar]
- 4.Jennifer C. The effect of rhythmic breathing on blood pressure in hypertensive adults. Journal of undergraduate research. 2000;1:78–98. [Google Scholar]
- 5.Madanmohan T, Vijayalakshmi P, Udupa K, Bhavanani AB, Prakash ES. Review of Shavasana studies conducted at JIPMER during 2001-2002y. Yoga Mimamsa. 2003;35:26–34. [Google Scholar]
- 6.Bijlani RL, Manjunatha S. Understanding Medical Physiology: A Textbook for Medical Students. 3rd ed. New Delhi: Jaypee Brothers Publishers; 2010. Understanding Medical Physiology: A Textbook for Medical Students; p. 872. [Google Scholar]
- 7.Pal GK, Velkumary S, Madanmohan T. Effect of short-term practice of breathing exercises on autonomic functions in normal human volunteers. Indian J Med Res. 2004;120:115–21. [PubMed] [Google Scholar]
- 8.Veerabhadrappa SG, Baljoshi VS, Khanapure S, Herur A, Patil S, Ankad RB, et al. Effect of yogic bellows on cardiovascular autonomic reactivity. J Cardiovasc Dis Res. 2011;2:223–7. doi: 10.4103/0975-3583.89806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Udupa KN, Singh RH. The scientific basis of yoga. JAMA. 1972;220:1365. doi: 10.1001/jama.1972.03200100075029. [DOI] [PubMed] [Google Scholar]
- 10.Bhargava R, Gogate MG, Mascarenhas JF. Autonomic responses to breath holding and its variations following pranayama. Indian J Physiol Pharmacol. 1988;32:257–64. [PubMed] [Google Scholar]
- 11.Krishnananda S. The Study and Practice of Yoga. 1st ed. Uttaranchal: Divine Life Society; 2009. p. 639. [Google Scholar]
- 12.Swami M. Hatha Yoga Pradipika. 4th ed. Bihar: Bihar School of Yoga; 1999. p. 645. [Google Scholar]
- 13.Roberti JW, Harrington LN, Storch EA. Further psychometric support for the 10-item version of the perceived stress scale. J Coll Couns. 2006;9:135–47. [Google Scholar]
- 14.Taelman J, Vandeput S, Spaepen A, Huffel S. Influence of mental stress on heart rate and heart rate variability. In: Sloten J, Verdonck P, Nyssen M, Haueisen J, editors. 4th European Conference of the International Federation for Medical and Biological Engineering. 1st ed. Berlin, Heidelberg: Springer; 2009. pp. 1366–9. [Google Scholar]
- 15.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–96. [PubMed] [Google Scholar]
- 16.Holland AE, Hill CJ, Jones AY, McDonald CF. Breathing exercises for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;10:CD008250. doi: 10.1002/14651858.CD008250.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gopal KS, Bhatnagar OP, Subramanian N, Nishith SD. Effect of yogasanas and pranayamas on blood pressure, pulse rate and some respiratory functions. Indian J Physiol Pharmacol. 1973;17:273–6. [PubMed] [Google Scholar]
- 18.Upadhyay Dhungel K, Malhotra V, Sarkar D, Prajapati R. Effect of alternate nostril breathing exercise on cardiorespiratory functions. Nepal Med Coll J. 2008;10:25–7. [PubMed] [Google Scholar]
- 19.Hoffman JW, Benson H, Arns PA, Stainbrook GL, Landsberg GL, Young JB, et al. Reduced sympathetic nervous system responsivity associated with the relaxation response. Science. 1982;215:190–2. doi: 10.1126/science.7031901. [DOI] [PubMed] [Google Scholar]
- 20.Sharma VK, Trakroo M, Subramaniam V, Rajajeyakumar M, Bhavanani AB, Sahai A. Effect of fast and slow pranayama on perceived stress and cardiovascular parameters in young health-care students. Int J Yoga. 2013;6:104–10. doi: 10.4103/0973-6131.113400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bhimani NT, Kulkarni NB, Kowale A, Salvi S. Effect of Pranayama on stress and cardiovascular autonomic function. Indian J Physiol Pharmacol. 2011;55:370–7. [PubMed] [Google Scholar]
- 22.McCall M. How might yoga work? An overview of potential underlying mechanisms. J Yoga Phys Ther. 2015;3:2–4. [Google Scholar]
- 23.Bhattacharya S, Pandey US, Verma NS. Improvement in oxidative status with yogic breathing in young healthy males. Indian J Physiol Pharmacol. 2002;46:349–54. [PubMed] [Google Scholar]
- 24.Harvey JR. The effect of yogic breathing exercises on mood. J Am Soc Psychosom Dent Med. 1983;30:39–48. [PubMed] [Google Scholar]