

Abstract
Background
The correlation between the atherogenic index of plasma (AIP) and waist circumference (WC) remains unknown.
Methods
A total of 5351 middle-aged men living in Southeastern China were surveyed using the random stratified cluster sampling method. A WC of 90 cm or greater was indicative of abdominal obesity, and AIP was calculated as follows: log [triglyceride (TG)/high-density lipoprotein-cholesterol (HDL-C)].
Results
(1) A significantly higher AIP was observed in subjects with abdominal obesity than in those without abdominal obesity (P < 0·001). (2) Multivariate logistic regression analysis revealed an odds ratio of 1·93, 2·59 and 2·76 for abnormal AIP levels for the second, third and fourth WC quartiles, respectively (all P < 0·001) compared to the first WC quartile as a reference. (3) There was a linear correlation between WC and AIP, and a 1·0 cm increase in WC resulted in a 0·0175 rise in AIP. For AIP corresponding to moderate risk (0·12–0·21), WC was 85–90 cm; for AIP corresponding to high risk (> 0·21), WC was >90 cm.
Conclusions
AIP of 0·12–0·21 or >0·21 indicates a likelihood of borderline abdominal obesity or abdominal obesity, respectively, and the combination of WC and AIP may increase the specificity and sensitivity for detection of abdominal obesity in clinical practice. The results suggest that AIP may be used as a reference to estimate abdominal obesity.
Keywords: Atherogenic index of plasma (AIP), Waist circumference, Abdominal obesity
Background
Obesity has become an important public health concern worldwide, and abdominal obesity, which involves fat accumulation in the abdomen, is recognized as an independent risk factor for obesity-related diseases and death [1]. In China, obesity has become a major risk factor for the increased prevalence of cardiovascular diseases [2]. In the present study, waist circumference (WC) was used as an index to assess abdominal obesity in middle-aged men, and the correlation between WC and the atherogenic index of plasma (AIP) was evaluated to provide evidence for the development of a preventive and control strategy for atherosclerosis and cardiovascular diseases in community populations.
Methods
A total of 21 survey sites (11 sites in urban areas and 10 sites in rural areas) were sampled in the three cities of Suzhou, Wuxi and Changzhou, Jiangsu Province, China, during the period from January to December 2009 using the random stratified cluster sampling method. Three villages were randomly sampled from each survey site, and approximately 200 permanent adult residents (duration of residence >5 years) were randomly sampled from each village. A total of 12,130 residents were investigated, of whom 11,774 had complete medical data available and were enrolled in the analysis. A total of 5351 men of Chinese Han ethnicity and aged 40–64 years underwent subsequent investigations, including 2810 (52·51%) living in urban areas and 2541 (47·49%) living in rural areas. Those receiving lipid-regulating drugs or with malignant tumors, Cushing’s syndrome, a history of schistosome infections, severe hepatic and renal insufficiency, or incomplete medical records were excluded from this study. (Fig. 1).
Fig. 1.
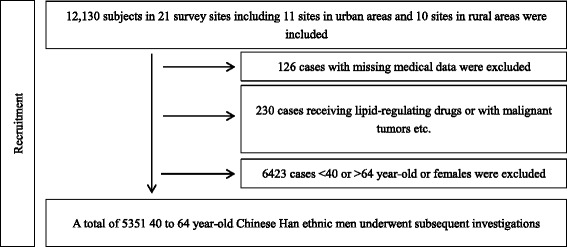
Participant Flowchat
The study protocol was approved by the Ethics Review Committee of our hospital, and signed informed consent was obtained from all participants.
All data were collected using a questionnaire designed by medical professionals. Health examinations included height, body weight, WC, blood pressure measurements, and blood lipid and glucose levels. Body mass index (BMI) was calculated using the following formula: BMI = body weight (kg)/height2 (m2). WC was measured using the method recommended by the World Health Organization. In brief, each subject was instructed to stand with the feet 25–30 cm apart and with the back straight to allow even distribution of body weight on two legs, and then the distance between the anterior superior iliac spine and the midpoint of the inferior margin of the 12th rib was measured at the end of a normal expiration. For biochemical examinations, all participants fasted for 8–12 h before collection of 5 mL of venous blood from the cubital vein the following morning. Levels of total cholesterol (TC), low-density lipoprotein-cholesterol (LDL-C), high-density lipoprotein-cholesterol (HDL-C), triglyceride (TG) and fasting blood glucose (FBG) were determined using the oxidase method, a homogeneous assay, an antibody-based homogeneous assay, the glycerol phosphate oxidase method, and the hexokinase method, respectively, on a fully automatic Hitachi 7180 biochemical analyzer (Hitachi, Tokyo, Japan).
Diagnostic criteria
According to the International Diabetes Federation 2005 criteria [3], abdominal obesity was defined as WC of ≥ 90 cm for men. AIP was calculated as log (TG/HDL-C) [4]. AIP risk was assigned into three groups: (1) low risk, AIP ≤ 0·11; (2) moderate risk, AIP ≥ 0·12 and ≤ 0·21; and (3) high risk, AIP > 0·21 [5]. Obesity was defined as BMI of ≥ 28 kg/m2 [6] and hypertension as systolic blood pressure (SBP) of ≥ 140 mmHg and/or diastolic blood pressure (DBP) of ≥ 90 mmHg, or currently undergoing antihypertensive therapy. Hyperglycemia was defined as FBG of >6·1 mmol/L or currently receiving antidiabetic agents, and hyperuricemia as serum uric acid (UA) of ≥ 420 mmol/L [7]. Hypertriglyceridemia was defined as TG of >1·7 mmol/L and hypercholesterolemia as TC of >5·18 mmol/L, while a HDL-C concentration of <1·04 mmol/L indicated low HDL-C and a concentration of >3·37 mmol/L indicated high LDL-C [8].
Statistical analysis
All measurement data are expressed as mean ± standard deviation, and all statistical analyses were performed using the statistical software SPSS version 11.5 (SPSS, Chicago, IL, USA). Differences in means among groups were tested for statistical significance using the chi-square test, and associations between WC and cardiovascular risk factors were examined using multivariate logistic regression analysis and linear correlation analysis. A P value <0·05 was considered statistically significant.
Results
Comparison of cardiovascular risk factors in subjects stratified by age and WC
Higher mean AIP, BMI, UA, SBP, DBP, TG, TC, LDL-C and FBG were observed in subjects with abdominal obesity compared to those with normal WC (all P < 0·001). However, no significant difference was seen in TC level between subjects with abdominal obesity and those with normal WC aged 60–64 years (P > 0·05). In addition, a lower mean HDL-C concentration was noted in subjects with abdominal obesity than in those with normal WC (P < 0·001) (Table 1).
Table 1.
Comparison of cardiovascular risk factors in subjects stratified by age groups and WC (χ ± S)
| Age(years) | WC (cm) | n | BMI(kg/m2) | TG(mmol/L) | TC(mmol/L) | HDL-c(mmol/L) | LDL-c(mmol/L) | UA(μmol/L) | FBG(mmol/L) | SBP(mmHg) | DBP(mmHg) | AIP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 40–44 | <90 | 764 | 23.22 ± 2.45 | 1.92 ± 1.63 | 4.66 ± 0.85 | 1.24 ± 0.36 | 2.87 ± 1.14 | 374.76 ± 72.72 | 5.32 ± 0.79 | 124.7 ± 13.31 | 75.7 ± 11.09 | 0.12 ± 0.31 |
| ≥90 | 590 | 27.05 ± 2.53 | 2.69 ± 2 | 4.88 ± 0.88 | 1.12 ± 0.25 | 3.21 ± 0.91 | 405.85 ± 76.77 | 5.79 ± 1.59 | 133.84 ± 15.25 | 82.64 ± 11.03 | 0.31 ± 0.31 | |
| P Value | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| 45–49 | <90 | 689 | 23.22 ± 2.22 | 1.88 ± 1.58 | 4.78 ± 0.86 | 1.25 ± 0.35 | 2.93 ± 0.89 | 364.98 ± 70.34 | 5.44 ± 1.05 | 125.74 ± 13.95 | 77.15 ± 10.62 | 0.11 ± 0.31 |
| ≥90 | 661 | 26.96 ± 2.32 | 2.8 ± 2.16 | 4.94 ± 0.9 | 1.14 ± 0.31 | 3.27 ± 0.91 | 408.91 ± 82.37 | 5.91 ± 1.41 | 135.2 ± 16.03 | 83.54 ± 10.96 | 0.32 ± 0.32 | |
| P Value | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| 50–54 | <90 | 587 | 23.44 ± 2.09 | 1.74 ± 1.36 | 4.62 ± 0.88 | 1.26 ± 0.32 | 2.82 ± 0.82 | 366.16 ± 69.02 | 5.61 ± 1.39 | 127.43 ± 16.5 | 77.71 ± 11.12 | 0.08 ± 0.3 |
| ≥90 | 538 | 26.98 ± 2.45 | 2.45 ± 1.78 | 4.82 ± 0.94 | 1.16 ± 0.44 | 3.17 ± 0.9 | 399.92 ± 83.27 | 6.09 ± 1.62 | 135.37 ± 15.99 | 83.52 ± 10.6 | 0.26 ± 0.31 | |
| P Value | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| 55–59 | <90 | 467 | 23.58 ± 2.34 | 1.65 ± 1.28 | 4.64 ± 0.86 | 1.28 ± 0.29 | 2.79 ± 0.86 | 365.68 ± 73.55 | 5.65 ± 1.26 | 130.7 ± 17.54 | 78.63 ± 11.05 | 0.04 ± 0.3 |
| ≥90 | 499 | 26.89 ± 2.25 | 2.39 ± 2.02 | 4.82 ± 0.92 | 1.16 ± 0.37 | 3.14 ± 0.93 | 400.89 ± 78.69 | 6.12 ± 1.5 | 137.04 ± 17.85 | 82.93 ± 11.09 | 0.25 ± 0.31 | |
| P Value | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| 60–64 | <90 | 275 | 23.57 ± 2.19 | 1.69 ± 1.12 | 4.72 ± 0.77 | 1.27 ± 0.40 | 2.89 ± 0.83 | 367.46 ± 76.37 | 5.7 ± 1.03 | 134.29 ± 18.14 | 79.07 ± 11.57 | 0.06 ± 0.3 |
| ≥90 | 281 | 27.01 ± 2.26 | 2.25 ± 1.94 | 4.83 ± 0.89 | 1.17 ± 0.24 | 3.11 ± 0.89 | 391.6 ± 89.05 | 6.29 ± 1.78 | 141.99 ± 17.84 | 83.22 ± 10.37 | 0.21 ± 0.32 | |
| P Value | 0.00 | 0.00 | 0.10 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Total | <90 | 2782 | 23.36 ± 2.28 | 1.80 ± 1.47 | 4.68 ± 0.86 | 1.26 ± 0.42 | 2.86 ± 0.94 | 368.28 ± 71.95 | 5.50 ± 1.11 | 127.49 ± 15.72 | 77.31 ± 11.08 | 0.09 ± 0.31 |
| ≥90 | 2569 | 26.98 ± 2.38 | 2.56 ± 2.01 | 4.86 ± 0.91 | 1.15 ± 0.40 | 3.19 ± 0.91 | 402.88 ± 81.48 | 6.00 ± 1.56 | 136.02 ± 16.58 | 83.17 ± 10.86 | 0.28 ± 0.32 | |
| Total | 5351 | 25.10 ± 2.95 | 2.17 ± 1.79 | 4.77 ± 0.89 | 1.21 ± 0.41 | 3.02 ± 0.94 | 384.89 ± 78.59 | 5.74 ± 1.37 | 131.59 ± 16.69 | 80.12 ± 11.36 | 0.18 ± 0.33 | |
| P Value | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
Pearson correlation analysis of WC and cardiovascular risk factors
Pearson correlation analysis revealed that WC was positively correlated with AIP (r = 0·371), BMI (r = 0·786), UA (r = 0·283), SBP (r = 0·241), DBP (r = 0·224), TG (r = 0·266), TC (r = 0·139), LDL-C (r = 0·243) and FBG (r = 0·215) (all P < 0·001), and negatively correlated with HDL-C (r = −0·222) (P < 0·001).
Multivariate logistic regression analysis of various WC quartiles and cardiovascular risk factors
All subjects were assigned to WC quartiles: (1) first quartile (Q1), WC ≤ 84 cm; (2) second quartile (Q2), WC ≥ 85 and ≤ 89 cm; (3) third quartile (Q3), WC ≥ 90 and ≤ 94 cm; and (4) fourth quartile (Q4), WC ≥ 95 cm. After adjustment for age, SBP, DBP, BMI, UA, TC, LDL-C and FBG, multivariate logistic regression analysis revealed an odds ratio of 1·93, 2·59 and 2·76 for abnormal AIP levels in Q2, Q3 and Q4 for WC (all P < 0·001) with WC Q1 as the reference (Table 2).
Table 2.
Multivariate logistic regression analysis of various quartiles of WC and cardiovascular risk factors
| WC group | N | Regression Coefficient | Wald chi square value | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| Q1(WC ≤ 84 cm) | 1463 | 1.00 | |||
| Q2(WC85-89 cm) | 1319 | 0.66 | 27.40 | 1.93 (1.51–2.46) | 0.00 |
| Q3(WC90-94 cm) | 1326 | 0.95 | 61.90 | 2.59 (2.05–3.29) | 0.00 |
| Q4(WC ≥ 95 cm) | 1243 | 1.02 | 62.83 | 2.76 (2.15–3.55) | 0.00 |
Notes: Age, SBP, DBP, BMI, UA, TC, LDL-C and FBG were adjusted
Detection rates of abdominal obesity in various AIP quartiles
The chi-square test revealed an increase in the detection rate of abdominal obesity with increasing AIP quartile (P < 0·001): the detection rate of abdominal obesity was 2·52 times greater in AIP Q4 than in AIP Q1 (Table 3).
Table 3.
Detection rates of abdominal obesity in various quartiles of AIP
| AIP groups | n(WC ≥ 90 cm) | Detection Rates(%) | Chi square value | P value |
|---|---|---|---|---|
| Q1(≤ − 0.050) | 1337 (352) | 26.31 | 600.831 | 0.000 |
| Q2(>-0.050 ≤ 0.133) | 1338 (594) | 44.42 | 33.210 | 0.000 |
| Q3(>0.133 ≤ 0.389) | 1339 (737) | 55.04 | 27.222 | 0.000 |
| Q4(>0.390) | 1337 (886) | 66.26 | 283.059 | 0.000 |
| Total | 5351 (2569) | 48.01 | 16.957 | 0.000 |
Note: Linear-by-Linear Association 456.202, P = 0.000
Linear regression analysis of WC and mean AIP
WC was classified into 27 groups (group 1, WC ≤ 75 cm; Groups 2–26, WC = 76–100 cm; and group 27, WC ≥101 cm) and the mean AIP was calculated in each group. Linear regression analysis revealed a linear correlation between WC and AIP; a 1·0 cm increase in WC resulted in a 0·0175 rise in AIP (Fig. 2).
Fig. 2.
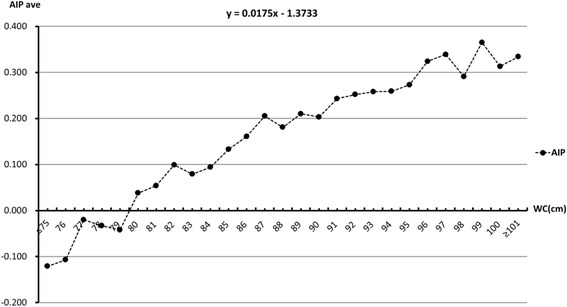
Linear regression analysis of WC and mean AIP
Discussion
Abdominal obesity, also known as central obesity, is mainly characterized by the deposition of fat in the subcutaneous abdominal region and perivisceral region. It has been shown that excessive accumulation of body fat may cause an increase in the prevalence of multiple cardiovascular risk factors, including hyperinsulinemia, insulin resistance, hypertension and dyslipidemia, which are considered the major causes of obesity-induced cardiovascular diseases [9]. We found a significantly higher AIP in subjects with abdominal obesity than in those without abdominal obesity (t = −22·276, P < 0·001), and WC was positively correlated with BMI, AIP, UA, SBP, DBP, TG, TC, LDL-C and FBG, and negatively correlated with HDL-C. In addition, we found that AIP increases with WC, and a rise in AIP resulted in an increase in the detection rate of abdominal obesity. These results demonstrate that WC and AIP are parameters associated with lipid metabolism, and an increase in WC is indicative of abnormal deposition of visceral fat in the abdomen, while a rise in AIP is indicative of dyslipidemia.
Results from the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study showed that among patients undergoing treatment with statins alone, the incidence of primary endpoint events was greater in those with high TG and low HDL-C levels than in other patients [10]. However, Pietro Scicchitano et al. [11] proposed functional food and nutraceuticals have the potential to become the future of primary prevention in dyslipidaemia treatment in cardiovascular disease prevention. Therefore, management of atherogenic dyslipidemia, which is characterized by hypertriglyceridemia and low HDL-C concentrations, should be a focus of attention [12].
It has been found that AIP is negatively associated with LDL particle diameter [4], and an increase in AIP indicates a rise in the proportion of small dense LDL (sdLDL) [13]. Relative to LDL, sdLDL is more likely to be oxidized and promote the production of foam cells, and sdLDL is therefore accepted as a strong risk factor for atherosclerosis and a predictive factor for emergency cardiovascular events [14]. In 2002, sdLDL was identified as a major risk factor for coronary heart disease by the National Cholesterol Education Program, and its detection was recommended by the program [15]. However, all currently available approaches used to detect sdLDL have limitations and are difficult to popularize in clinical practice. By contrast, measurement of AIP is simple, economical and feasible. Although AIP is a calculated value, it is a sensitive indicator of dyslipidemia, and may indirectly reflect the diameter of LDL-C particles [13]. We therefore hypothesized that the combination of WC and AIP may increase the specificity and sensitivity of the detection of abdominal obesity in clinical practice.
We observed a linear correlation between WC and AIP, and a 1·0 cm increase in WC resulted in a 0·0175 increase in AIP. When WC increased from 84 to 90 cm, AIP increased from 0·094 to 0·203, and AIP was ≥ 0·243 when WC was ≥ 91 cm, indicating that WC was ≤ 84, 85–90 and >91 cm for AIP corresponding to low (≤ 0·11), moderate (0·12–0·21) and high risk (> 0·21), respectively. These results demonstrate that moderate-risk AIP indicates borderline abdominal obesity, and high-risk AIP indicates the presence of abdominal obesity.
Although WC intuitively reflects abdominal fat accumulation, it fails to quantify and differentiate visceral fat and subcutaneous fat. Considering the limitations and inconvenience of computed tomography and magnetic resonance imaging in clinical practice, a simpler way to identify abdominal obesity is of great significance for the prevention and control of cardiovascular diseases in community populations. The WC cutoff point for abdominal obesity remains controversial. The World Health Organization and International Diabetes Federation recommend WC ≥ 90 cm for men and ≥80 cm for women as the cutoff points for abdominal obesity in the Asian Pacific region [3, 16]. The Working Group on Obesity in China recommends WC ≥ 85 cm for men and ≥ 80 cm for women as the cutoff points for abdominal obesity [6], while the 2011 Chinese Guidelines for Prevention of Cardiovascular Diseases recommend WC cutoff points of ≥ 90 cm for men and ≥ 85 cm for women for abdominal obesity [8]. In addition, the Japan Society for the Study of Obesity recommends WC cutoff points of 85 cm for men and 90 cm for women [17], and 85 cm was predicted as the WC cutoff point for insulin resistance in middle-aged Japanese men [18]. He and colleagues reported WC cutoff points of 83–85 cm for men and 73–76 cm for women in China [19], and our recent study showed that an appropriate WC cutoff point was 85 cm for abdominal obesity in middle-aged men living in Suzhou, Wuxi and Changzhou areas of Jiangsu Province, southeastern China [20]. In the present study we found that WC was 85–90 cm when AIP was 0·12–0·21, which strongly supports the previous results. Therefore, we suggest that WC cutoff points for abdominal obesity should be defined according to local epidemiological profiles.
Our study has some limitations. First, computed tomography or magnetic resonance imaging was not performed to quantitatively differentiate visceral fat and subcutaneous fat. Second, the effects of race, gender, age, region and economic levels on moderate- and high-risk AIP levels require further investigation.
Conclusion
In conclusion, moderate- or high-risk AIP indicates a likelihood of borderline abdominal obesity or abdominal obesity, respectively, and the combination of WC and AIP may increase the specificity and sensitivity of the detection of abdominal obesity in clinical practice. Our results suggest that AIP may be used as a reference to identify abdominal obesity.
Acknowledgements
Not applicable.
Funding
The research leading to these results received funding from the National Natural Science Foundation of China (Grant No.: 81600346), Natural Science Foundation of Jiangsu Province, China (Grant No.: BK2011162 and BK20151115), the R & D Fund of Wuxi Municipal Science & Technology Bureau, China (Grant No.: CSE00705, CMB21S1301 and CMB41S1701), and Jiangsu Department of Health, China (Grant Nos.: H200739, BJ14023, Z201519, BJ15032, BJ15033 and H201639).
Availability of data and materials
The datasets used and/or analyzed during the current study will be available from the corresponding author on reasonable requests after study completion.
Abbreviations
- AIP
Atherogenic index of plasma
- BMI
Body mass index
- DBP
Diastolic blood pressure
- FBG
Fasting blood glucose
- HDL-C
High-density lipoprotein-cholesterol
- LDL-C
Low-density lipoprotein-cholesterol
- SBP
Systolic blood pressure
- TC
Total cholesterol,
- TG
Triglyceride
- UA
Uric acid
- WC
Waist circumference
Authors’ contributions
Study conception and design: ZS, SS, YL and CY. Literature search: FL, YF, HL and WY. Data collection and analysis: FL, YF and HL. Data interpretation: ZS and SS. Writing: SS, YL and CY. All authors read and approved the final manuscript.
Authors’ information
Not applicable.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Review Committee of the Taihu Rehabilitation Hospital of Jiangsu Province (SG-MEC-2007-12). Written informed consent was obtained from all participants following a detailed description of the purpose of the study.
Consent for publication
Written informed consent for publication of their clinical details was obtained from the patients. Copies of the consent form are available for review by the Editor of this journal.
Competing interests
The authors report no relationships that could be construed as a conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Matsuzawa Y. Establishment of a concept of visceral fat syndrome and discovery of adiponectin. Proc Jpn Acad Ser B Phys Biol Sci. 2010;86:131–141. doi: 10.2183/pjab.86.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhu ZM. Obesity related cardiovascular risk and its appropriate intervention. Chin J Endocrinol Metab. 2011;27:707–710. [Google Scholar]
- 3.Alberti KG, Zimmet P, Shaw J, IDF Epidemiology Task Force Consensus Group. The metabolic syndrome: a new worldwide definition. Lancet 2005; 366: 1059–1062. doi: 10.1016/S0140-6736(05)67402-8. [DOI] [PubMed]
- 4.Frohlich J, Dobiasova M. Fractional esterification rate of cholesterol and triglycerides to HDL-cholesterol are powerful predictors of positive findings on coronary angiography. Clin Chem. 2003;49:1873–1880. doi: 10.1373/clinchem.2003.022558. [DOI] [PubMed] [Google Scholar]
- 5.Dobiasova M. Atherogenic index of plasma [log (triglycerides/HDL-cholesterol)]: theoretical and practical implications. Clin Chem. 2004;50:1113–1115. doi: 10.1373/clinchem.2004.033175. [DOI] [PubMed] [Google Scholar]
- 6.Cooperative Meta-analysis Group of China Obesity Task Force Predictive value of body mass index and waist circumference to risk factors of related diseases in Chinese adult population. Chin J Epidemiol. 2002;23:5–10. [PubMed] [Google Scholar]
- 7.Endocrinology Division of Chinese Medical Association Chinese expert consensus about hyperuricemia and gout treatment. Chin J Endocrinol Metab. 2013;29:913–920. [Google Scholar]
- 8.Chinese Society of Cardiology of Chinese Medical Association, Editorial Board of Chinese Journal of Cardiology Chinese guidelines for prevention of cardiovascular diseases. Chin J Cardiol. 2011;39:3–22. [PubMed] [Google Scholar]
- 9.Carr MC, Brunzell JD. Abdominal obesity and dyslipidemia in the metabolic syndrome: importance of type 2 diabetes and familial combined hyperlipidemia in coronary artery disease risk. J Clin Endocrinol Metab. 2004;89:2601–2607. doi: 10.1210/jc.2004-0432. [DOI] [PubMed] [Google Scholar]
- 10.Scott R. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010;362:1563–1574. doi: 10.1056/NEJMoa1001282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Scicchitano P, Cameli M, Maiello M, et al. Nutraceuticals and dyslipidaemia: beyond the common therapeutics. J Funct Foods. 2014;6:11–32. doi: 10.1016/j.jff.2013.12.006. [DOI] [Google Scholar]
- 12.Chinese Society of Cardiology of Chinese Medical Association Chinese expert consensus on blood lipid related cardiovascular residual risk control. Chin J Cardiol. 2012;40:547–553. [PubMed] [Google Scholar]
- 13.Dobiasova M. AIP-atherogenic index of plasma as a significant predictor of cardiovascular risk: from research to practice. Vnitr Lek. 2006;52:64–71. [PubMed] [Google Scholar]
- 14.Jia WP, Xiang KS, Chen L, Lu JX, Wu YM. Epidemiological study on obesity and its comorbidities in urban Chinese older than 20 years of age in shanghai. China Obesity reviews. 2002;3:157–165. doi: 10.1046/j.1467-789X.2002.00071.x. [DOI] [PubMed] [Google Scholar]
- 15.National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002; 106: 3143–3421. [PubMed]
- 16.Obesity Group of Endocrine Society of Chinese Medical Association Expert consensus on prevention and treatment of obesity in Chinese adults. Chin J Endocrinol Metab. 2011;27:711–717. [Google Scholar]
- 17.Examination Committee of Criteria for 'Obesity Disease' in Japan and Japan Society for the Study of Obesity. New criteria for 'obesity disease' in Japan. Circ J. 2002;66:987–92. [DOI] [PubMed]
- 18.Tabata S, Yoshimitsu S, Hamachi T, Abe H, Ohnaka K, Kono S. Waist circumference and insulin resistance: a cross-sectional study of Japanese men. BMC Endocr Disord. 2009;9:1. doi: 10.1186/1472-6823-9-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.He Y, Zeng Q, Tian JL, Chen ZH, Zhao XL. Waist to height ratio as a predictor of dyslipidemia for Chinese adults. Chin J Health Manage. 2013;7:9–13. [Google Scholar]
- 20.Shen SW, Lu Y, Qi HJ, et al. Waist-to-height ratio is an effective indicator for comprehensive cardiovascular health. Sci Rep. 2017;7:43046. doi: 10.1038/srep43046. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study will be available from the corresponding author on reasonable requests after study completion.