

Sir,
Proper care of patients with burns requires an accurate assessment of the extent of the burnt area. The common methods used to measure this are the Lund and Browder chart (LB),[1] the rule of nines[2] and the patient's palm size method (for smaller burns).[3] Among these, the LB method is the most accurate and popular method of assessing percentage.[4,5]
Burn wound assessment has to be done multiple times and by people with varying degrees of training and experience. The tool used for such an assessment must be as robust, precise and reliable as possible and should have the least possible scope for errors.
The conventional (adult) LB chart has anterior and posterior body schematics divided into regions which represent percentages of total body surface area. These regional percentages are often in fractions. The actual burnt area is usually irregular and covers only a part of the region on the chart. This has now to be accurately depicted onto the paper chart and calculations have to be done. First, the burnt fraction of the region has to be estimated and then the various fractions of different regions have to be added up. This estimation and calculations in fractions is difficult. Each time the observer makes an estimate and a calculation, there is a potential for an error. There can be significant errors and differences between different assessors,[6] and this can have a profound effect on treatment.
At our hospital, we have modified the adult LB chart in the following way [Figure 1]. Keeping the essential computational integrity of the LB chart intact, each region is subdivided into smaller areas by lines in such a manner that each resulting quadrilateral shape represents one quarter of 1% (0.25%). The assessor has to shade in or outline the burnt area on both anterior and posterior diagrams, then count the number of shaded or outlined quadrilaterals and divide by four to arrive at the total percentage of burnt body surface area. This counting of the squares and division by four is easily done and requires no dealing in fractions.
Figure 1.
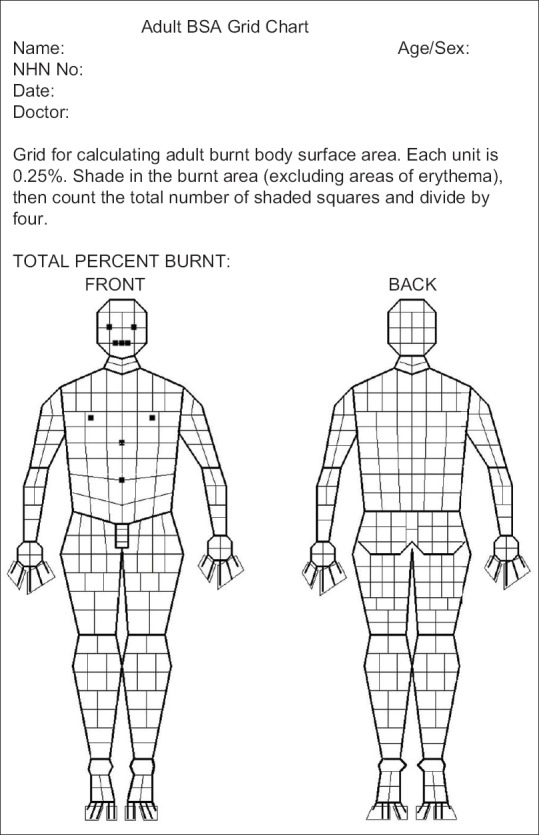
Adult body surface area grid chartAdult BSA grid chart
Thus, the resolution for this modified chart is 0.25%. Calculation can usually be done mentally and the result obtained can be easily counterchecked. Results are also consistent when repeated by different assessors. All that needs to be done is to count the number of shaded quadrilaterals and divide by four.
This modified LB chart was made using the open source GNU Image Manipulation Program.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Lund CC, Browder NC. The estimation of areas of burns. Surg Gynecol Obstet. 1944;79:352–8. [Google Scholar]
- 2.Sabiston DC Jr, editor. Textbook of Surgery. 13th ed. W B Saunders Company; 1986. p. 215. [Google Scholar]
- 3.Amirsheybani HR, Crecelius GM, Timothy NH, Pfeiffer M, Saggers GC, Manders EK. The natural history of the growth of the hand: I. Hand area as a percentage of body surface area. Plast Reconstr Surg. 2001;107:726–33. doi: 10.1097/00006534-200103000-00012. [DOI] [PubMed] [Google Scholar]
- 4.Hettiaratchy S, Papini R. Initial management of a major burn: II – Assessment and resuscitation. BMJ. 2004;329:101–3. doi: 10.1136/bmj.329.7457.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Seyyed MM, Amir M. A comparison of burn size estimation methods' accuracy applied by medical students. Future Med Educ J. 2014;4:36–40. [Google Scholar]
- 6.Harish V, Raymond AP, Issler AC, Lajevardi SS, Chang LY, Maitz PK, et al. Accuracy of burn size estimation in patients transferred to adult Burn Units in Sydney, Australia: An audit of 698 patients. Burns. 2015;41:91–9. doi: 10.1016/j.burns.2014.05.005. [DOI] [PubMed] [Google Scholar]