

Abstract
Several studies have suggested that the neuropeptide oxytocin may enhance aspects of social communication in autism. Little is known, however, about its effects on non-social manifestations, such as restricted interests and repetitive behaviors. In the Empathizing-Systemizing Theory of autism, social deficits are described along the continuum of empathizing ability, whereas non-social aspects are characterized in terms of an increased preference for patterned or rule-based systems, called “systemizing.” We therefore developed an automated eye-tracking task to test whether children and adolescents with autism spectrum disorder (ASD) compared to matched controls display a visual preference for more highly organized and structured (“systemized”) real-life images. Then, as part of a randomized, double-blinded, placebo-controlled crossover study, we examined the effect of intranasal oxytocin on systemizing preferences in 16 male children with ASD, compared with 16 matched controls. Participants viewed 14 slides, each containing 4 related pictures (e.g. of people, animals, scenes, or objects) that differed primarily on the degree of systemizing. Visual systemizing preference was defined in terms of the fixation time and count for each image. Unlike control subjects who showed no gaze preference, individuals with ASD preferred to fixate on more highly systemized pictures. Intranasal oxytocin eliminated this preference in ASD participants, who now showed a similar response to control subjects on placebo. In contrast, control participants increased their visual preference for more systemized images after receiving oxytocin vs. placebo. These results suggest that, in addition to its effects on social communication, oxytocin may play a role in some of the non-social manifestations of autism.
Keywords: Autism spectrum disorder, oxytocin, systemizing, restricted interests, eye tracking
Almost seventy-five years ago, Leo Kanner first described a group of atypically developing children with two distinct symptom profiles: “autistic aloneness” and an “obsessive insistence on the preservation of sameness” (Kanner, 1943). Since that time, various diagnostic algorithms have characterized what has become known as Autism Spectrum Disorder (ASD), the most recent being the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (APA, 2013; Baker, 2013). Paralleling Kanner’s original description, the DSM-5 describes both social and non-social behavioral domains: 1) deficits in social communication, and 2) restricted, repetitive patterns of behavior, interests or activities. Although several theoretical frameworks such as Theory of Mind and Social Motivation Theory (S. Baron-Cohen, Leslie, & Frith, 1985; Chevallier, Kohls, Troiani, Brodkin, & Schultz, 2012) have been proposed to explain the social deficits seen in ASD, few have adequately accounted for the non-social behavioral differences, or captured the bi-dimensional nature of autism.
In 2009, Baron-Cohen formulated the Empathizing-Systemizing Theory of autism (S. Baron-Cohen, 2009), which integrated both social and non-social aspects in terms of deficits in empathy (understanding and feeling the mental states of others, or “empathizing”) and the drive to analyze or construct rule-based systems or patterns (termed “systemizing”). In individuals with ASD, empathizing traits are inversely correlated with systemizing preferences (S. Baron-Cohen, Richler, Bisarya, Gurunathan, & Wheelwright, 2003; Grove, Baillie, Allison, Baron-Cohen, & Hoekstra, 2013); in other words, individuals who score highest for systemizing traits (such as being more detail oriented, tending to follow a structured routine, and being rigidly governed by rules), are more likely to score lower in the empathizing domain (such as valuing relationships, judging the feelings of others, expressing emotions, etc.). Males tend to score higher in the systemizing domain, while females generally tend to score higher in the empathizing domain, which may also help to explain some of the gender differences in ASD (Simon Baron-Cohen, Knickmeyer, & Belmonte, 2005).
Consistent with the concept of systemizing, children with ASD appear to have a preference for predictable, repetitive patterns of sensory stimulation, as observed in the tendency to line up toys, categorize objects, and fixate on familiar patterns and interests. One study using automated eye tracking showed that a sample of young children with ASD had a visual preference for videos of computer generated geometric patterns over social stimuli (i.e. children moving rhythmically) (Pierce, Conant, Hazin, Stoner, & Desmond, 2011). In the current study, our first aim was to test whether children with ASD prefer to view more organized or structured real-life images with predictable, repetitive patterns. Using a novel eye-tracking paradigm viewing a range of systemized images, we obtained a quantitative assessment of interest or motivation based on gaze preference, independent of verbal or cognitive ability (Boraston & Blakemore, 2007).
In searching for clues regarding the etiology of ASD, few studies have successfully linked both social and non-social aspects of the condition within a single neurobiological framework (Strathearn, 2009). Over recent years, an increasing number of studies, both human and non-human mammalian, have suggested that the brain’s oxytocinergic system may play a role in the development or manifestation of ASD (Bartz & Hollander, 2008; Domes, Heinrichs, et al., 2013; Domes, Kumbier, Heinrichs, & Herpertz, 2013; Gordon et al., 2013; Modi & Young, 2012; Sala et al., 2011; Stavropoulos & Carver, 2013). Oxytocin is a neuromodulatory peptide hormone synthesized in the paraventricular and supraoptic nuclei of the hypothalamus, whose function has been linked with social bonding and attachment (Feldman, 2012; Insel, 2010; Kim, Fonagy, Koos, Dorsett, & Strathearn, 2014; Strathearn, Fonagy, Amico, & Montague, 2009; Strathearn, Iyengar, Fonagy, & Kim, 2012). Recently, more nuanced effects have been described in the areas of social salience and motivation, reward sensitivity, and stress reactivity (Crespi, 2016). Generally, oxytocin appears to diminish stress responses while increasing the salience and reward value of social cues.
In studies involving healthy individuals, intranasally administered oxytocin enhances feelings of empathy (Hurlemann et al., 2010) and many other characteristics associated with the empathizing trait, such as mentalizing (Domes, Heinrichs, Michel, Berger, & Herpertz, 2007), trust (Kosfeld, Heinrichs, Zak, Fischbacher, & Fehr, 2005), emotion recognition (Domes et al., 2010) and eye gaze (Guastella, Mitchell, & Dadds, 2008). These effects of oxytocin appear to be mediated via functional changes in specific brain regions such as the amygdala and the nucleus accumbens, which are involved in emotion processing and social motivation (Gordon et al., 2016). However, the biological mechanisms by which oxytocin may affect systemizing have not been well studied. One group showed the effect of oxytocin on amygdala functioning to be moderated by individual levels of “systemizing” (Hirosawa et al., 2012), suggesting that oxytocin may indirectly influence systemizing via its effect on empathizing in the amygdala. As empathizing and systemizing are strongly negatively correlated (Grove et al., 2013), increasing social attunement may diminish the preference for structure and predictability.
Earlier studies in autism using a single dose of intranasal oxytocin revealed promising effects, such as increased emotion recognition when observing the eye region of human faces (Andari et al., 2010; Domes, Kumbier, et al., 2013; Guastella et al., 2010), enhanced brain amygdala response to social cues (Domes, Heinrichs, et al., 2013; Domes, Kumbier, et al., 2013), and increased reciprocated social interaction (Andari et al., 2010). Repeated dose studies have been few in number and have shown mixed results. Initial studies showed no significant effects on social interaction skills, repetitive behaviors, or clinical outcomes (Dadds et al., 2014; Guastella et al., 2015), but more recent trials have demonstrated modest effects with regard to social behavior and clinical ratings (Watanabe et al., 2015; Yatawara, Einfeld, Hickie, Davenport, & Guastella, 2015). Few studies have examined the effect of oxytocin on non-social behaviors such as systemizing preference in autism. In one preliminary study, adults with ASD who were given a peripheral infusion of oxytocin showed reduced repetitive behavior (Hollander et al., 2003). Another pilot study testing the chronic administration of intranasal oxytocin in ASD adults showed a marginally significant decrease in lower-ordered repetitive behaviors such as stereotyped movements, but no difference in higher-order behaviors such as compulsions or insistence on sameness (Anagnostou et al., 2012). Our second aim was therefore to test whether acutely administered intranasal oxytocin would diminish visual systemizing preferences in ASD.
In summary, we sought to 1) test whether children and adolescents with ASD preferentially view more highly organized/structured images, using a novel preferential looking eye tracking paradigm, and 2) examine the effect of intranasal oxytocin on these visual systemizing preferences. We hypothesized that participants with ASD would show a visual preference for more highly systemized real-life photographs, compared with matched-control participants, and that this preference would be reduced after administration of intranasal oxytocin.
Methods
Participants
Twenty males with ASD (mean age 12.5 years) were recruited through the Autism Treatment Network (ATN) and Simons Simplex Collection (SSC) at Baylor College of Medicine/Texas Children’s Hospital’s Autism Center. All participants with ASD were assessed by a trained clinician who ensured that they met clinical criteria for Autistic Disorder or Asperger’s Disorder according to DSM-IV criteria. The Autism Diagnostic Interview-Revised (ADI-R) and the Autism Diagnostic Observation Schedule (ADOS) (Lord, Rutter, DiLavore, & Risi, 1999) were used to confirm that each participant met formal, standardized criteria for a diagnosis of ASD. All of the SSC children except one received an ADOS Module 3, indicating that they were verbally fluent and spoke in complete, complex sentences. The remaining child received an ADOS Module 2, indicating at least phrase speech and/or simple sentences. These children also received the Differential Abilities Scales-II (DAS-II), which revealed a mean full-scale IQ of 92.3±12.6, verbal IQ of 92.5±18.4, and non-verbal IQ 97.0±12.5. All participants were aged between 8 and 19 years; were English speaking; and were not intellectually impaired, as established by developmentally appropriate psychometric testing. Exclusion criteria included uncorrected visual impairment; neurological disease, such as stroke, brain tumor, or seizure disorder; or a history of meningitis or encephalitis.
The participants with ASD were matched by age and race to a group of typically developing males (mean age 13.2 years), who were recruited from a community database at the Children’s Nutrition Research Center, Baylor College of Medicine. Prior to enrollment, control participants were screened by phone to rule out possible learning or behavior problems (i.e. a diagnosed learning disability or need for special education services, as per parent report). Parents subsequently completed the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997), which confirmed that all control participants scored at “low risk” for emotional, behavioral, or hyperactivity/concentration problems. To screen for autistic traits, parents completed the Social Communications Questionnaire (SCQ) (Rutter, 2003), with all control participants scoring well below the study-imposed, stringent cut-off score of 10 (mean score 2.9, range 0–7). Parents of participants from both groups completed the Vineland Adaptive Behaviors Scales (2nd edition) (Sparrow, Cicchetti, & Balla, 2005) and, as expected, participants with ASD scored significantly lower on overall adaptive functioning (t = 5.2, p < 0.001), and on each of the individual subscales: social (t = 7.8, p < 0.001), communication (t = 4.4, p < 0.001), and daily living (t = 3.3, p < 0.005) (Table 1).
Table 1.
Demographic and Behavioral Characteristics of ASD and Control Participants
| Control | ASD | |||
|---|---|---|---|---|
|
| ||||
|
M ± SD (n = 16) |
Range |
M ± SD (n = 16) |
Range | |
| Participant age on first visit (years) | 13.2 ± 3.2 | 9.2 – 19.6 | 12.8 ± 3.4 | 8.2 – 19.0 |
| Race, N (%) | ||||
| White | 9 (56.3%) | 9 (56.3%) | ||
| Non-White | 7 (43.7%) | 7 (43.7%) | ||
| Hollingshead Socioeconomic Status | 49.3 ± 12.0 | 29.0 – 66.0 | 42.3 ± 14.5 | 9.0 – 63.5 |
| Psychiatric Comorbidity* | ||||
| ADHD | 0 | 6 (37.5%) | ||
| Anxiety/depression | 0 | 4 (25%) | ||
| Mood instability | 0 | 4 (25%) | ||
| Reported annual household income, n (%) | ||||
| Not reported | 3 (18.8%) | 2 (12.5%) | ||
| < $65,000 | 4 (25%) | 7 (43.8%) | ||
| $66,000–$100,000 | 4 (25%) | 2 (12.5%) | ||
| > $100,000 | 5 (31.2%) | 5 (31.3%) | ||
| Vineland Composite Score | 104.3 ± 12.3 (n = 15) |
84 – 126 | 74.5 ± 16.3 (n =10) |
39 – 90 |
| Communication | 102.9 ± 13.8 (n = 16) |
82 – 134 | 75.2 ± 19.0 (n = 11) |
38 – 101 |
| Daily Living | 108.0 ± 19.6 (n = 15) |
78 – 146 | 81.2 ± 20.7 (n = 10) |
38 – 109 |
| Social | 103.1 ± 10.0 (n = 16) |
87 – 119 | 67.8 ± 13.6 (n = 11) |
46 – 87 |
based on medication prescription
Two participants with ASD did not return for their second visit, and two others were excluded from further analyses; one had been started on a psychotropic medication between visits, and the other had poor-quality eye-tracking data. Thus, a total of 16 participants with ASD and 16 corresponding control participants were included in the final analysis. Of those with ASD, 11 (69%) were taking psychotropic medications at the time of the study visits, including stimulant medications for Attention Deficit Hyperactivity Disorder (n = 6), medication for depression or anxiety (n = 4), and mood stabilizers (n = 4). None of the control participants were on psychotropic medications or had comorbid conditions, as assessed using the SDQ. Additional participant characteristics are described in Table 1.
The Institutional Review Board at Baylor College of Medicine approved the research protocol, and the participants’ parents provided written informed consent and certified child assent. The Food and Drug Administration (FDA) approved the use of oxytocin in this study as part of an Investigational New Drug (IND) application.
Apparatus and Stimuli
Eye tracker
Real-time eye movements and visual fixations were recorded using the Tobii T120 automated eye tracker (Tobii Technology, Sweden). The eye tracker consists of two infrared light sources and a camera (frame rate 640 × 480 @ 30 frames per second) integrated into a 17-inch computer monitor, on which the visual stimuli were displayed. Using corneal reflection techniques to track both bright and dark pupils, x and y coordinates of eye gaze position were recorded at a rate of 60 Hz, with an estimated accuracy between 0.4° and 0.6° (i.e. difference between measured and actual gaze direction) (Tobii, 2011). Spatial resolution was estimated to be 0.3° and drift due to change in lighting 0.1°.
Visual stimuli: The Systemizing Picture Task
In order to test gaze preferences in ASD, we developed the Systemizing Picture Task (SPT), using real-life images of people, animals, scenes, and objects (Figure 1). Each slide consisted of 4 related images, positioned in each quadrant of the slide, that were equivalent in terms of social relevance but which varied systematically in terms of organization or structure (“systemizing”).
Figure 1.

Systemizing Picture Task. Representative slides displayed on the Tobii eye-tracker, showing four levels of picture systemizing. The position of each picture was pseudo-randomized across 4 versions of the task, and the position of the most and least systemized pictures varied between slides. The 3 primary factors in the model included ASD vs. control group, treatment (oxytocin vs. placebo), and level of picture systemizing. Comparable but not actual images used in the task are shown, due to copyright constraints.
Upon initial selection of 22 slides, we sampled 8 individuals to rate each picture on level of systemizing. Systemizing was defined for participants as the level of organization indicated by the picture. Across the participants, this initial rating yielded a median concordance (Kendall’s W) of .911. We selected 70% agreement on the rank ordering as the minimum criteria (W=.84). On this basis, 7 slides were eliminated. We eliminated an additional slide which appeared to distract participants. The remaining 14 slides were re-rated on systemizing by a further group of 39 individuals, which yielded a median Kendall’s W coefficient of .871. These final systemizing ratings were used to assign rank orders to the four pictures within each slide.
Each picture in this final set of slides was also rated for valence (9-point scale), humanness (5-point scale), aliveness (5-point scale), and movement (5-point scale). These ratings yielded high reliability as indicated by Cronbach’s alphas of .858, .961, .837, and .828, respectively. The averaged humanness, aliveness, and movement scores were later entered into statistical models to control for potential confounding effects.
Four different versions of the experiment were created, varying the positions of the four pictures within each slide, in order to minimize possible gaze bias based on picture location. The different versions were consistent between matched subjects.
Procedure
Oxytocin administration
As part of a randomized, double-blinded crossover study, participants were randomly assigned one nasal solution on Visit 1 and the alternate solution on Visit 2. The intranasal oxytocin (Syntocinon Spray, Novartis, Switzerland) was purchased from a Swiss pharmacy, and a local compounding pharmacy prepared the placebo sprays using identical base ingredients (for 5 ml of placebo solution: 12.5 mg chlorobutanol hemihydrate, 2 mg methyl-4-hydroxybenzoate, 1 mg propyl-4-hydroxybenzoate, 14 mg citric acid monohydrate, 125 mg glycerine 85%, and 4.85 g purified water; for active drug: 24 IU oxytocin per ml). The oxytocin solution and the placebo (base alone) were stored in identical glass metered pump spray bottles (0.1 ml per spray) and labeled to ensure that both participants and experimenters were blind to the drug treatment.
Trained research assistants administered either the oxytocin or the placebo spray intranasally. Children 16 years and older received the usual adult dose of 24 IU oxytocin (10 puffs alternating between nostrils with the head in the upright position, each spray containing 2.4 IU), while doses for younger children were titrated downward, similar to Guastella et al. (2010). Those aged 12–15 years received 7 puffs (16.8 IU), while children aged 8–11 years received 5 puffs (12 IU total).
After oxytocin administration, participants rested while watching an animated film or reading quietly. A similar activity was provided during the second visit, to standardize the environment across visits. Approximately 30 minutes after oxytocin administration, the participants commenced the eye-tracking experiment.
Eye-tracking experiment
After performing a 9-point eye-tracking calibration using the Tobii Studio software (Tobii Technology, Sweden), an instruction slide appeared that was read aloud to the participant, followed by a practice slide. A crosshair was shown for 1 second between each slide, and participants were instructed to gaze directly at the crosshair when present. During the experiment, the monitor displayed each SPT slide for 12 seconds (except for 3 participants who viewed the slides for 8 seconds each; sensitivity analysis revealed no difference in the pattern of findings and therefore these 3 participants were included in all of the analyses). After the entire eye-tracking computer task was completed, participants received compensation, were presented with a certificate of completion, and scheduled to return in approximately 1–2 weeks’ time for the corresponding study visit.
Data Analysis
Eye-gaze data were extracted from the four pictures/regions of interest (ROI) on each slide, which depicted the theme at four different levels of organization or structure (i.e., least systemized, less systemized, more systemized, most systemized) (Figure 1). We exported and analyzed, as our outcome measures: a) fixation time (total duration of fixation) and b) fixation count (total number of fixations) in each ROI. Fixation was defined as an eye gaze that remained stationary (within 1° radius, or approximately 35 pixels) for a minimum of 80 msec. Proportion variables were calculated by dividing the fixation values (time or count) recorded for each quadrant by the respective total value obtained for the entire slide. As the proportions were not distributed normally, a range of transformations was performed. Intercept-adjusted logarithmic transforms offered the closest approximation to normality. The random-effect models controlled for ROI location on the slide and visit order, as we probed for significance of the group × treatment × systemizing interaction. Participants’ performance across four levels of systemizing was represented by random effects parameters. Three additional variables (participant age, picture “humanness”, and picture “aliveness”) were added to the model individually, to test for any confounding influence. Analyses were performed in STATA/SE 13.1 and IBM SPSS Statistics (version 21).
Results
Means and standard errors of fixation variables are presented in Table 2. Consistent with our hypothesis, the ASD group showed a visual preference for more highly systemized images in the standard placebo (PL) condition (Figure 2). There was a significant linear trend of increase in the fixation time of ASD participants with increasing levels of picture systemizing (ASDPL βsystemizing = 0.0041 ± 0.002 [standard error], z = 2.00, p = 0.045), while no such effect was seen in the control group (CTLPL βsystemizing = 0.0006 ± 0.0018, z = 0.32, p = 0.748).
Table 2.
Visual Systemizing Preferences Based on Fixation Time and Count, in Control and ASD Groups as a Function of Oxytocin and Level of Picture Systemizing
| Fixation time | Fixation count | |||
|---|---|---|---|---|
|
| ||||
| Placebo | Oxytocin | Placebo | Oxytocin | |
| Control (n =16) | ||||
|
| ||||
| Least systemized | 0.212 ± 0.008 | 0.198 ± 0.008 | 0.215 ± 0.007 | 0.204 ± 0.007 |
| Less systemized | 0.214 ± 0.005 | 0.210 ± 0.005 | 0.216 ± 0.004 | 0.213± 0.004 |
| More systemized | 0.216 ± 0.005 | 0.222 ± 0.005 | 0.217 ± 0.004 | 0.223 ± 0.004 |
| Most systemized | 0.218 ± 0.008 | 0.234 ± 0.008 | 0.219 ± 0.007 | 0.232 ± 0.007 |
|
| ||||
| Wald χ2 | 32.01 | 25.10 | ||
| p | 0.0004 | 0.005 | ||
|
| ||||
| ASD (n =16) | ||||
|
| ||||
| Least systemized | 0.201 ± 0.008 | 0.220 ± 0.008 | 0.203 ± 0.007 | 0.220 ± 0.007 |
| Less systemized | 0.209 ± 0.005 | 0.215 ± 0.005 | 0.211 ± 0.004 | 0.216 ± 0.004 |
| More systemized | 0.217 ± 0.005 | 0.209 ± 0.005 | 0.219 ± 0.004 | 0.212 ± 0.004 |
| Most systemized | 0.226 ± 0.008 | 0.204 ± 0.008 | 0.227 ± 0.007 | 0.208 ± 0.007 |
|
| ||||
| Wald χ2 | 32.97 | 35.81 | ||
| p | 0.0003 | 0.0001 | ||
Note. Duration and frequency values (estimated marginal means ± SE) shown are log-transformed proportion values, adjusted for the total duration and number of fixations recorded for each slide. Wald χ2 and p-values are those obtained for the best-fitting mixed-effects models for the respective outcome variables, including a subject-level random intercept and a random coefficient for level of picture systemizing. df = 10 for all models.
Figure 2.
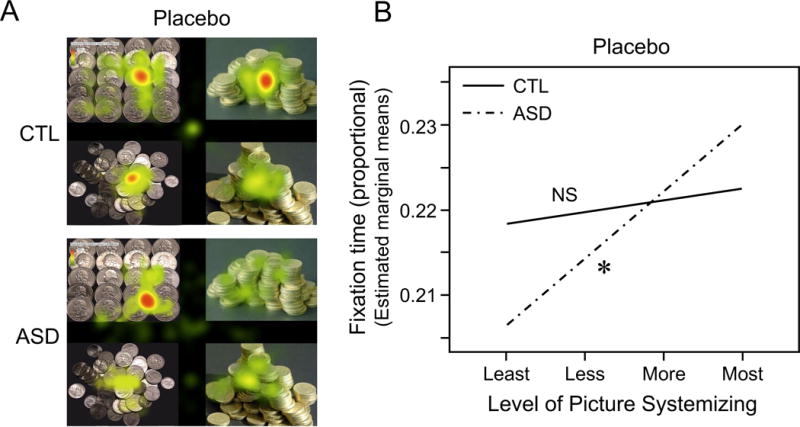
Visual systemizing preferences in ASD versus control groups, in the placebo condition. A. Representative heat maps visualizing differences in relative gaze duration between ASD and control groups for all participants in one version of the Systemizing Picture Task (n = 8) on the coin slide. Participants with ASD showed a gaze preference for the most systemized image. Relative duration was calculated from the sum of individual fixation times relative to the total fixation time for that slide. B. Participants with ASD showed a linear trend of increase in the fixation time with increasing levels of picture systemizing. This trend was absent in the control group. The interaction effect was not significant. The y-axis represents log-transformed proportion variable. The statistical significance of the linear trend of increase is noted: NS, not significant; * p < .05
Oxytocin, however, reversed the overall patterns of fixation observed under placebo, as reflected in a significant 3-way interaction (βgroup × treatment × systemizing = −0.0119 ± 0.0039, z = −3.04, p = 0.002) (Figure 3). For the ASD group, oxytocin eliminated the tendency to fixate on more highly systemized pictures, as seen in a significant two-way interaction (ASD βtreatment × systemizing = −0.0070 ± 0.0030, z = −2.33, p = 0.020) (Figure 3A). In particular, after receiving intranasal oxytocin compared with placebo, ASD participants showed significantly less fixation on the “most systemized” pictures (ASD βtreatment = −0.0215 ± 0.0104, z = −2.07, p = 0.038). The ASD group showed no persisting gaze preference after receiving intranasal oxytocin (OT) (ASDOT βsystemizing = −0.0030 ± 0.0022, z = −1.38, p = 0.169), similar to what was seen in the control group under placebo conditions (CTLPL βsystemizing = 0.0006 ± 0.0018, z = 0.32, p = 0.748; Figure 3B).
Figure 3.
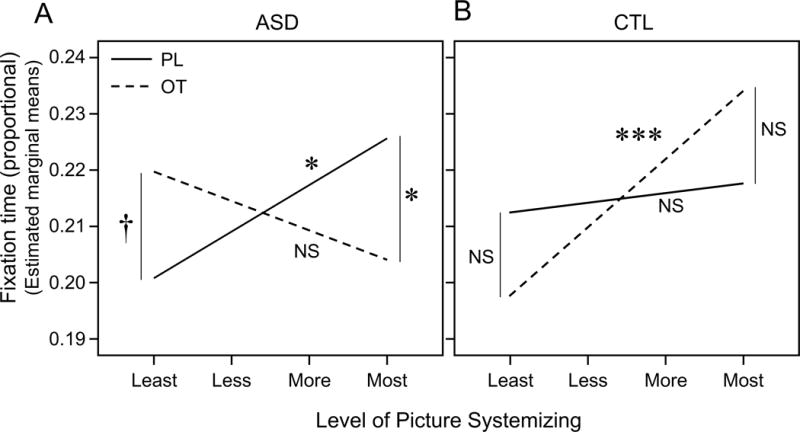
Visual systemizing preferences as a function of drug treatment and level of picture systemizing in ASD (A) versus control (CTL) (B) groups. Oxytocin significantly reversed the overall patterns of fixation time observed under placebo. A. Oxytocin (OT) compared with placebo (PL) significantly reduced the tendency for participants with ASD to fixate on the most systemized stimuli, while increasing their fixation on the least systemized stimuli, with marginal significance. After oxytocin, participants with ASD did not demonstrate a significant gaze preference. B. In the control group, oxytocin produced a significant preference to view more highly systemized pictures. The y-axis represents log-transformed proportion variables. The statistical significance of the linear trend of increase or differences between oxytocin and placebo at specific levels of systemizing is noted: NS, not significant; † p < .1; * p < .05; ** p < .01; *** p < .001
In contrast, the control group became more likely to fixate on more systemized pictures after oxytocin administration (CTLOT βsystemizing = −0.0065 ± 0.0018, z = 3.60, p < 0.001), with a significant 2-way interaction observed (CTL βtreatment × systemizing = 0.0054 ± 0.0026, z = 2.13, p = 0.033) (Figure 3B). However, the difference in fixation time after oxytocin vs. placebo was not statistically significant for either “most systemized” or “least systemized” pictures (CTL βtreatment = 0.0164 ± 0.0104, z = 1.57, p = 0.116; βtreatment = −0.0147 ± 0.0104, z = −1.41, p = 0.158, respectively).
Overall, oxytocin resulted in a decrease in systemizing preference (βsystemizing) in ASD participants (Figure 3A), but an increase in systemizing preference for control participants (Figure 3B), resulting is a highly significant 2-way interaction effect (OT βgroup × systemizing = −0.0087 ± 0.0028, z = −3.07, p = 0.002). Figure 4A illustrates the change in slope after oxytocin administration comparing ASD and CTL groups.
Figure 4.
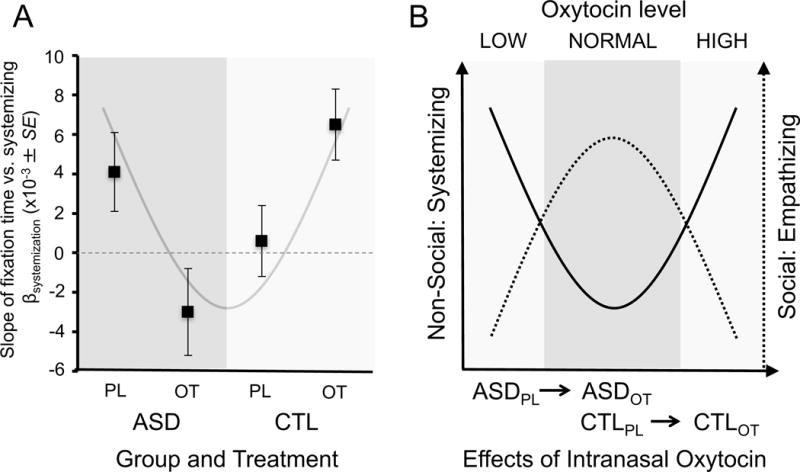
A. Contrasting effect of intranasal oxytocin on visual systemizing preference, based on the slope of fixation time vs. systemizing, in ASD vs. control participants. Oxytocin decreased the systemizing preference in ASD participants, but increased systemizing preference in control participants. B. Model of how oxytocin levels may be associated with systemizing and empathizing characteristics in ASD and typically developing individuals. Effects of systemizing are based on results displayed in (A). We propose that intranasal oxytocin may increase oxytocin levels in ASD participants from the low to normal range, while shifting the level in typically developing participants from normal to a high range. An inverted pattern may represent the effect of oxytocin on empathizing abilities, based on other studies of intranasal oxytocin in ASD and typically developing populations (see text).
Similar gaze patterns were seen after examining the total number of fixations in each region of interest (fixation count) (Table 2), except that the interaction effect between drug treatment and level of systemizing in the control group was no longer statistically significant (CTL βtreatment × systemizing = 0.0041 ± 0.0022, z = 1.86, p = 0.063).
None of the independent ratings of picture “humanness” or “aliveness” were associated with fixation time or count, and these variables did not alter any of the significant main or interaction effects. The age variable was also not associated with either of the outcome variables and did not significantly alter any of the observed effects.
Discussion
This study is the first to examine the effects of intranasal oxytocin, in both ASD and non-ASD groups, on what we have termed “visual systemizing preference,” a non-social manifestation of ASD. Firstly, we confirmed that our novel eye-tracking task was able to distinguish children/adolescents with ASD from non-ASD controls. Secondly, we showed that when intranasal oxytocin was administered to ASD participants, it effectively eliminated the difference between ASD and control participants. Surprisingly, however, oxytocin also increased systemizing preference when administered to control participants. Understanding how oxytocin affects both social and non-social aspects of ASD, in affected and unaffected individuals, may provide clues for understanding its potential role in the etiology and treatment of autism.
Oxytocin in ASD
There are no currently approved pharmacotherapies available to treat the core social or non-social manifestations of ASD. As noted above, early studies provided preliminary evidence for the beneficial effects of single dose intranasal oxytocin in adolescents and adults with autism, with regard to both social communication (Andari et al., 2010; Guastella et al., 2010) and repetitive behavior (Anagnostou et al., 2012; Hollander et al., 2003). Subsequent studies of repeated administrations of oxytocin have shown variable effects on behavioral outcomes, ranging from no significant effects on social skills or repetitive behavior (Dadds et al., 2014; Guastella et al., 2015), to improved social reciprocity and clinical ratings of behavior (Watanabe et al., 2015; Yatawara et al., 2015). Other human studies in non-clinical populations have shown improvements in a range of responses relevant to autism, including emotional empathy (Hurlemann et al., 2010), eye gaze (Guastella et al., 2008), trust (Baumgartner, Heinrichs, Vonlanthen, Fischbacher, & Fehr, 2008), and the ability to read the affective state of others (Domes et al., 2007).
Despite an abundance of media attention on the promises of oxytocin therapy in conditions such as ASD, concerns remain about anomalous effects or even unanticipated adverse effects (Bales & Perkeybile, 2012; Bales et al., 2012; J. Bartz et al., 2011; De Dreu et al., 2010; Miller, 2013). A number of studies have noted variations in oxytocin response depending on individual differences and other contextual factors (Bartz, Zaki, Bolger, & Ochsner, 2011). Other work has shown, for example, that plasma oxytocin response to social cues (mothers interacting with their infants) varies with adult temperament, being positively associated with sensitivity to moods, emotions and physical sensations, but negatively associated with compulsive and task oriented behavior (Strathearn et al., 2012), which parallel empathizing and systemizing traits respectively.
Systemizing and Empathizing in ASD
Baron-Cohen first hypothesized that autism may result from an extreme tendency to “systemize” or seek out regularities or predictable patterns and rules (S. Baron-Cohen, 2009). This preference for patterned over unpatterned information may help to explain some of the restricted, repetitive behaviors and interests characteristically observed in individuals with ASD. Consistent with this model, our findings, along with those of Pierce et al. (2011), show that individuals with ASD display a preference for more patterned or “systemized” visual stimuli.
According to Baron-Cohen’s theory, hyper-systemizing is also often accompanied by deficits in “empathizing,” or the ability to identify and appropriately respond to another person’s thoughts and emotions (S. Baron-Cohen & Wheelwright, 2004), with deficits in social communication characteristically seen in ASD. Individuals with ASD tend to score higher than the general population on measures of systemizing but lower on empathizing measures (Auyeung et al., 2009; S. Baron-Cohen, 2009).
Effects of Oxytocin in Non-ASD Participants
As noted, we also found that oxytocin increased visual systemizing preference in control participants, resulting in a gaze preference similar to ASD participants under placebo conditions (Figure 3A & B). Although not predicted, this result is consistent with a growing body of literature demonstrating that the effects of oxytocin are significantly modulated by individual differences. Oxytocin receptor deficient mice, which display social deficits as well as cognitive inflexibility, serve as an animal model for ASD. After intraventricular administration of oxytocin, social deficits improve and cognitive inflexibility decreases (Ring, 2011; Sala et al., 2011). However, when the same dose of oxytocin is administered to unaffected mice, the opposite effect is observed. While Hollander et al. (2003) reported that intravenous oxytocin resulted in a decrease in repetitive behaviors in adults with autism, higher oxytocin levels are associated with an increase in repetitive behavior in adults with obsessive-compulsive disorder (Leckman et al., 1994). Although intranasal oxytocin enhances emotion recognition in individuals with ASD (Bartz et al., 2010; Guastella et al., 2010), one study showed that oxytocin decreases the accuracy of emotion recognition when administered to a normative sample (Cardoso, Ellenbogen, & Linnen, 2013). Oxytocin enhances trust and cooperation in normative populations (Declerck, Boone, & Kiyonari, 2010; Kosfeld et al., 2005), but appears to have the opposite effect in individuals with borderline personality disorder (J. Bartz et al., 2011). Finally, Groppe et al. (2013) showed that the effect of oxytocin on performance in a social reward and punishment task depended on whether the individuals had high or low sociability ratings. In the low sociability group, oxytocin increased social reward while avoiding punishment, whereas reduced performance was seen in the high sociability group.
Together, these findings suggest that an optimal range may exist for oxytocin functioning, with its behavioral effects dependent on individual differences that may reflect baseline oxytocin levels, oxytocin receptor status, or interactions with other neuroendocrine factors. A similar “optimal range” model for autism was proposed by Zoghbi and Bear (2012), based on “high” vs. “low” levels of gene expression and effects on synaptic plasticity. In our study, intranasal oxytocin appears to move ASD participants toward more typical responses in the Systemizing Picture Task, while moving control participants further away (Figure 4). Studies have suggested that individuals with ASD may have lower peripheral levels of oxytocin compared to matched-controls (Feldman, Golan, Hirschler-Guttenberg, Ostfeld-Etzion, & Zagoory-Sharon, 2014; Green et al., 2001; Modahl et al., 1998), and that intranasally administered oxytocin increases plasma oxytocin levels (Andari et al., 2010). If peripheral oxytocin levels reflect central oxytocin functioning (McGregor, Callaghan, & Hunt, 2008; Strathearn et al., 2009; Valstad et al., 2017), then giving intranasal oxytocin may move individuals with ASD from the “low” to the “normal” range of functioning (Figure 4B). Likewise, giving oxytocin to neurotypical control participants may move them from the “normal” to the “high” oxytocin range, resulting in the observed behavioral differences.
We hypothesize that a similar, but inverted, pattern may also exist for the effect of oxytocin on social responses in ASD, with other studies providing evidence for a non-linear effect on behaviors more closely associated with “empathizing” (Bales et al., 2012; Bales et al., 2007; J. Bartz et al., 2011; Cardoso et al., 2013; Sala et al., 2011) (Figure 4B). Additional studies, which also collect peripheral measures of oxytocin before and after intranasal administration, are needed to explore this question more fully.
Limitations and Future Directions
Several limitations of this study need to be considered. Firstly, having created a novel eye-tracking task to examine gaze preference for more organized or structured images, the Systemizing Picture Task has not yet been validated against other measures of systemizing. The original Systemizing Quotient (S. Baron-Cohen et al., 2003) and Autism Spectrum Quotient (S. Baron-Cohen, Wheelwright, Skinner, Martin, & Clubley, 2001) were not suitable for administration in children and adolescents, and a subsequent children’s version which relied solely on parent report (Auyeung et al., 2009) was not available at the time that the study commenced. Comparing our task with other validated measures of systemizing will help to expand our understanding of its meaning and clinical significance.
Although we sought to control for variations in picture composition and meaning, such as the “humanness” and “aliveness”, other physical aspects of the pictures, such as color, intensity or background features, may have also influenced gaze preference. Our desire to use “real-world” images limited our ability to standardize many of these other features. Although “age,” when added as a covariate, did not significantly alter study findings, the enrolled groups did encompass a broad range of ages, with a relatively small number of participants. Future studies enrolling larger numbers, and including female participants, may be able to look more specifically for age and gender response differences. An additional limitation includes a lack of systematic information on psychiatric comorbidity. Further studies are warranted to investigate possible contributions of psychiatric comorbidity to the findings reported here.
Additional studies will also need to test whether intranasal oxytocin enhances functioning in real-life environments, or influences long-term outcomes in ASD. Only after more intensive studies are conducted evaluating outcome will we know whether a potential opportunity exists to combine pharmacological treatment with therapeutic/behavioral interventions.
Conclusion
Most recent prevalence estimates indicate that up to 1 in 68 children may be affected by ASD (CDC, 2016), with affected individuals and families usually requiring intensive and costly therapeutic intervention to optimize long-term developmental and behavioral outcomes. Understanding the neuroendocrine basis for this condition is an urgent imperative. This study provides preliminary evidence for a possible role of oxytocin in the etiology and/or treatment of autism by demonstrating its effect on a non-social manifestation of ASD. With oxytocinergic pathways highly sensitive to early developmental experience via epigenetic mechanisms (F. A. Champagne, 2008; F. Champagne, Diorio, Sharma, & Meaney, 2001; Kumsta, Hummel, Chen, & Heinrichs, 2013), this understanding may provide an even more important opportunity for early intervention and/or prevention.
Acknowledgments
This work was funded by the Baylor College of Medicine Junior Faculty Seed Funding Program, 2009–2010 (Grant number 2531915102) and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01 HD065819). Peter Fonagy was in part supported by the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) North Thames at Barts Health NHS Trust. He is in receipt of a National Institute for Health Research (NIHR) Senior Investigator Award (NF-SI-0514-10157). The content is solely the responsibility of the authors and does not necessarily represent the official views of the U.S. National Institutes of Health, the NHS, the NIHR or the UK Department of Health.
References
- Anagnostou E, Soorya L, Chaplin W, Bartz J, Halpern D, Wasserman S, Hollander E. Intranasal oxytocin versus placebo in the treatment of adults with autism spectrum disorders: a randomized controlled trial. Molecular Autism. 2012;3(1):16. doi: 10.1186/2040-2392-3-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andari E, Duhamel JR, Zalla T, Herbrecht E, Leboyer M, Sirigu A. Promoting social behavior with oxytocin in high-functioning autism spectrum disorders. Proceedings of the National Academy of Sciences USA. 2010;107(9):4389–4394. doi: 10.1073/pnas.0910249107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- APA. Diagnostic and Statistical Manual of Mental Disorders (DSM-5) 5th. Washington DC: American Psychiatric Association; 2013. [Google Scholar]
- Auyeung B, Wheelwright S, Allison C, Atkinson M, Samarawickrema N, Baron-Cohen S. The children’s Empathy Quotient and Systemizing Quotient: sex differences in typical development and in autism spectrum conditions. Journal of Autism and Developmental Disorders. 2009;39(11):1509–1521. doi: 10.1007/s10803-009-0772-x. [DOI] [PubMed] [Google Scholar]
- Baker JP. Autism at 70 — Redrawing the Boundaries. New England Journal of Medicine. 2013;369(12):1089–1091. doi: 10.1056/NEJMp1306380. [DOI] [PubMed] [Google Scholar]
- Bales KL, Perkeybile AM. Developmental experiences and the oxytocin receptor system. Hormones and Behavior. 2012;61(3):313–319. doi: 10.1016/j.yhbeh.2011.12.013. dx.doi.org/10.1016/j.yhbeh.2011.12.013. [DOI] [PubMed] [Google Scholar]
- Bales KL, Perkeybile AM, Conley OG, Lee MH, Guoynes CD, Downing GM, Mendoza SP. Chronic Intranasal Oxytocin Causes Long-Term Impairments in Partner Preference Formation in Male Prairie Voles. Biological Psychiatry. 2013;74:180–188. doi: 10.1016/j.biopsych.2012.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bales KL, van Westerhuyzen JA, Lewis-Reese AD, Grotte ND, Lanter JA, Carter CS. Oxytocin has dose-dependent developmental effects on pair-bonding and alloparental care in female prairie voles. Hormones and Behavior. 2007;52(2):274–279. doi: 10.1016/j.yhbeh.2007.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron-Cohen S. Autism: the empathizing-systemizing (E-S) theory. Annals of the New York Academy of Sciences. 2009;1156:68–80. doi: 10.1111/j.1749-6632.2009.04467.x. [DOI] [PubMed] [Google Scholar]
- Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”? Cognition. 1985;21(1):37–46. doi: 10.1016/0010-0277(85)90022-8. [DOI] [PubMed] [Google Scholar]
- Baron-Cohen S, Richler J, Bisarya D, Gurunathan N, Wheelwright S. The systemizing quotient: an investigation of adults with Asperger syndrome or high-functioning autism, and normal sex differences. Philosophical Transactions of the Royal Society B: Biological Sciences. 2003;358(1430):361–374. doi: 10.1098/rstb.2002.1206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron-Cohen S, Wheelwright S. The empathy quotient: an investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. Journal of Autism and Developmental Disorders. 2004;34(2):163–175. doi: 10.1023/b:jadd.0000022607.19833.00. [DOI] [PubMed] [Google Scholar]
- Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The autism-spectrum quotient (AQ): evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders. 2001;31(1):5–17. doi: 10.1023/a:1005653411471. [DOI] [PubMed] [Google Scholar]
- Baron-Cohen Simon, Knickmeyer Rebecca C, Belmonte Matthew K. Sex Differences in the Brain: Implications for Explaining Autism. Science. 2005;310(5749):819–823. doi: 10.1126/science.1115455. [DOI] [PubMed] [Google Scholar]
- Bartz JA, Hollander E. Oxytocin and experimental therapeutics in autism spectrum disorders. In: Neumann ID, Landgraf R, editors. Progress in Brain Research. Advances in Vasopressin and Oxytocin - From Genes to Behaviour to Disease. Vol. 170. Elsevier; 2008. pp. 451–462. Reprinted from: NOT IN FILE. [DOI] [PubMed] [Google Scholar]
- Bartz JA, Zaki J, Bolger N, Hollander E, Ludwig NN, Kolevzon A, Ochsner KN. Oxytocin selectively improves empathic accuracy. Psychological Science. 2010;21(10):1426–1428. doi: 10.1177/0956797610383439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartz JA, Zaki J, Bolger N, Ochsner KN. Social effects of oxytocin in humans: context and person matter. Trends in Cognitive Sciences. 2011;15(7):301–309. doi: 10.1016/j.tics.2011.05.002. [DOI] [PubMed] [Google Scholar]
- Bartz J, Simeon D, Hamilton H, Kim S, Crystal S, Braun A, Hollander E. Oxytocin can hinder trust and cooperation in borderline personality disorder. Social Cognitive and Affective Neuroscience. 2011;6(5):556–563. doi: 10.1093/scan/nsq085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baumgartner T, Heinrichs M, Vonlanthen A, Fischbacher U, Fehr E. Oxytocin Shapes the Neural Circuitry of Trust and Trust Adaptation in Humans. Neuron. 2008;58(4):639–650. doi: 10.1016/j.neuron.2008.04.009. [DOI] [PubMed] [Google Scholar]
- Boraston Z, Blakemore SJ. The application of eye-tracking technology in the study of autism. Journal of Physiology. 2007;581(Pt 3):893–898. doi: 10.1113/jphysiol.2007.133587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cardoso C, Ellenbogen MA, Linnen AM. The Effect of Intranasal Oxytocin on Perceiving and Understanding Emotion on the Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT) Emotion. 2014;14:43–50. doi: 10.1037/a0034314. [DOI] [PubMed] [Google Scholar]
- CDC. Prevalence and Characteristics of Autism Spectrum Disorders Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2012. Morbidity and Mortality Weekly Report. 2016;65(3):1–23. doi: 10.15585/mmwr.ss6503a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Champagne FA. Epigenetic mechanisms and the transgenerational effects of maternal care. Frontiers in Neuroendocrinology. 2008;29(3):386–397. doi: 10.1016/j.yfrne.2008.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Champagne F, Diorio J, Sharma S, Meaney MJ. Naturally occurring variations in maternal behavior in the rat are associated with differences in estrogen-inducible central oxytocin receptors. Proceedings of the National Academy of Sciences USA. 2001;98(22):12736–12741. doi: 10.1073/pnas.221224598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chevallier C, Kohls G, Troiani V, Brodkin ES, Schultz RT. The social motivation theory of autism. Trends in Cognitive Sciences. 2012;16(4):231–239. doi: 10.1016/j.tics.2012.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crespi BJ. Oxytocin, testosterone, and human social cognition. Biological Reviews of the Cambridge Philosophical Society. 2016;91(2):390–408. doi: 10.1111/brv.12175. [DOI] [PubMed] [Google Scholar]
- Dadds MR, MacDonald E, Cauchi A, Williams K, Levy F, Brennan J. Nasal oxytocin for social deficits in childhood autism: a randomized controlled trial. Journal of Autism and Developmental Disorders. 2014;44(3):521–531. doi: 10.1007/s10803-013-1899-3. [DOI] [PubMed] [Google Scholar]
- De Dreu CK, Greer LL, Handgraaf MJ, Shalvi S, Van Kleef GA, Baas M, Feith SW. The neuropeptide oxytocin regulates parochial altruism in intergroup conflict among humans. Science. 2010;328(5984):1408–1411. doi: 10.1126/science.1189047. [DOI] [PubMed] [Google Scholar]
- Declerck CH, Boone C, Kiyonari T. Oxytocin and cooperation under conditions of uncertainty: the modulating role of incentives and social information. Hormones and Behavior. 2010;57(3):368–374. doi: 10.1016/j.yhbeh.2010.01.006. [DOI] [PubMed] [Google Scholar]
- Domes G, Heinrichs M, Kumbier E, Grossmann A, Hauenstein K, Herpertz SC. Effects of Intranasal Oxytocin on the Neural Basis of Face Processing in Autism Spectrum Disorder. Biological Psychiatry. 2013;74(3):164–171. doi: 10.1016/j.biopsych.2013.02.007. dx.doi.org/10.1016/j.biopsych.2013.02.007. [DOI] [PubMed] [Google Scholar]
- Domes G, Heinrichs M, Michel A, Berger C, Herpertz SC. Oxytocin improves “mind-reading” in humans. Biological Psychiatry. 2007;61(6):731–733. doi: 10.1016/j.biopsych.2006.07.015. [DOI] [PubMed] [Google Scholar]
- Domes G, Kumbier E, Heinrichs M, Herpertz SC. Oxytocin Promotes Facial Emotion Recognition and Amygdala Reactivity in Adults with Asperger Syndrome. Neuropsychopharmacology. 2014;39:698–706. doi: 10.1038/npp.2013.254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Domes G, Lischke A, Berger C, Grossmann A, Hauenstein K, Heinrichs M, Herpertz SC. Effects of intranasal oxytocin on emotional face processing in women. Psychoneuroendocrinology. 2010;35(1):83–93. doi: 10.1016/j.psyneuen.2009.06.016. [DOI] [PubMed] [Google Scholar]
- Feldman R. Oxytocin and social affiliation in humans. Hormones and Behavior. 2012;61(3):380–391. doi: 10.1016/j.yhbeh.2012.01.008. [DOI] [PubMed] [Google Scholar]
- Feldman R, Golan O, Hirschler-Guttenberg Y, Ostfeld-Etzion S, Zagoory-Sharon O. Parent-child interaction and oxytocin production in pre-schoolers with autism spectrum disorder. The British Journal of Psychiatry. 2014;205(2):107–112. doi: 10.1192/bjp.bp.113.137513. [DOI] [PubMed] [Google Scholar]
- Goodman R. The Strengths and Difficulties Questionnaire: A Research Note. Journal of Child Psychology and Psychiatry. 1997;38:581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x. [DOI] [PubMed] [Google Scholar]
- Gordon I, Jack A, Pretzsch CM, Vander Wyk B, Leckman JF, Feldman R, Pelphrey KA. Intranasal Oxytocin Enhances Connectivity in the Neural Circuitry Supporting Social Motivation and Social Perception in Children with Autism. Scientific Reports. 2016;6:35054. doi: 10.1038/srep35054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gordon I, Vander Wyk BC, Bennett RH, Cordeaux C, Lucas MV, Eilbott JA, Pelphrey KA. Oxytocin enhances brain function in children with autism. Proceedings of the National Academy of Sciences USA. 2013;110:20953–20958. doi: 10.1073/pnas.1312857110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green L, Fein D, Modahl C, Feinstein C, Waterhouse L, Morris M. Oxytocin and autistic disorder: alterations in peptide forms. Biological Psychiatry. 2001;50(8):609–613. doi: 10.1016/s0006-3223(01)01139-8. [DOI] [PubMed] [Google Scholar]
- Groppe SE, Gossen A, Rademacher L, Hahn A, Westphal L, Grunder G, Spreckelmeyer KN. Oxytocin influences processing of socially relevant cues in the ventral tegmental area of the human brain. Biological Psychiatry. 2013;74(3):172–179. doi: 10.1016/j.biopsych.2012.12.023. [DOI] [PubMed] [Google Scholar]
- Grove R, Baillie A, Allison C, Baron-Cohen S, Hoekstra RA. Empathizing, systemizing, and autistic traits: latent structure in individuals with autism, their parents, and general population controls. Journal of Abnormal Psychology. 2013;122(2):600–609. doi: 10.1037/a0031919. [DOI] [PubMed] [Google Scholar]
- Guastella AJ, Einfeld SL, Gray KM, Rinehart NJ, Tonge BJ, Lambert TJ, Hickie IB. Intranasal oxytocin improves emotion recognition for youth with autism spectrum disorders. Biological Psychiatry. 2010;67(7):692–694. doi: 10.1016/j.biopsych.2009.09.020. [DOI] [PubMed] [Google Scholar]
- Guastella AJ, Gray KM, Rinehart NJ, Alvares GA, Tonge BJ, Hickie IB, Einfeld SL. The effects of a course of intranasal oxytocin on social behaviors in youth diagnosed with autism spectrum disorders: a randomized controlled trial. Journal of Child Psychology and Psychiatry. 2015;56(4):444–452. doi: 10.1111/jcpp.12305. [DOI] [PubMed] [Google Scholar]
- Guastella AJ, Mitchell PB, Dadds MR. Oxytocin increases gaze to the eye region of human faces. Biological Psychiatry. 2008;63(1):3–5. doi: 10.1016/j.biopsych.2007.06.026. [DOI] [PubMed] [Google Scholar]
- Hirosawa T, Kikuchi M, Higashida H, Okumura E, Ueno S, Shitamichi K, Minabe Y. Oxytocin attenuates feelings of hostility depending on emotional context and individuals’ characteristics. Scientific Reports. 2012;2:384. doi: 10.1038/srep00384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollander E, Novotny S, Hanratty M, Yaffe R, DeCaria CM, Aronowitz BR, Mosovich S. Oxytocin infusion reduces repetitive behaviors in adults with autistic and Asperger’s disorders. Neuropsychopharmacology. 2003;28(1):193–198. doi: 10.1038/sj.npp.1300021. [DOI] [PubMed] [Google Scholar]
- Hurlemann R, Patin A, Onur OA, Cohen MX, Baumgartner T, Metzler S, Kendrick KM. Oxytocin enhances amygdala-dependent, socially reinforced learning and emotional empathy in humans. Journal of Neuroscience. 2010;30(14):4999–5007. doi: 10.1523/JNEUROSCI.5538-09.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Insel TR. The challenge of translation in social neuroscience: a review of oxytocin, vasopressin, and affiliative behavior. Neuron. 2010;65(6):768–779. doi: 10.1016/j.neuron.2010.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2:217–250. [PubMed] [Google Scholar]
- Kim S, Fonagy P, Koos O, Dorsett K, Strathearn L. Maternal oxytocin response predicts mother-to-infant gaze. Brain Research. 2014;1580:133–142. doi: 10.1016/j.brainres.2013.10.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, Fehr E. Oxytocin increases trust in humans. Nature. 2005;435(7042):673–676. doi: 10.1038/nature03701. [DOI] [PubMed] [Google Scholar]
- Kumsta R, Hummel E, Chen FS, Heinrichs M. Epigenetic regulation of the oxytocin receptor gene: implications for behavioral neuroscience. Frontiers in Neuroscience. 2013;7:83. doi: 10.3389/fnins.2013.00083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leckman JF, Goodman WK, North WG, Chappell PB, Price LH, Pauls DL, McDougle CJ. Elevated cerebrospinal fluid levels of oxytocin in obsessive-compulsive disorder. Comparison with Tourette’s syndrome and healthy controls. Archives of General Psychiatry. 1994;51(10):782–792. doi: 10.1001/archpsyc.1994.03950100030003. [DOI] [PubMed] [Google Scholar]
- Lord C, Rutter M, DiLavore PC, Risi S. Autism Diagnostic Observation Schedule Manual. Los Angeles, CA: Western Psychological Services; 1999. [Google Scholar]
- McGregor IS, Callaghan PD, Hunt GE. From ultrasocial to antisocial: a role for oxytocin in the acute reinforcing effects and long-term adverse consequences of drug use? British Journal of Pharmacology. 2008;154(2):358–368. doi: 10.1038/bjp.2008.132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller G. The Promise and Perils of Oxytocin. Science. 2013;339(6117):267–269. doi: 10.1126/science.339.6117.267. [DOI] [PubMed] [Google Scholar]
- Modahl C, Green L, Fein D, Morris M, Waterhouse L, Feinstein C, Levin H. Plasma oxytocin levels in autistic children. Biological Psychiatry. 1998;43(4):270–277. doi: 10.1016/s0006-3223(97)00439-3. [DOI] [PubMed] [Google Scholar]
- Modi ME, Young LJ. The oxytocin system in drug discovery for autism: animal models and novel therapeutic strategies. Hormones and Behavior. 2012;61(3):340–350. doi: 10.1016/j.yhbeh.2011.12.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pierce K, Conant D, Hazin R, Stoner R, Desmond J. Preference for geometric patterns early in life as a risk factor for autism. Archives of General Psychiatry. 2011;68(1):101–109. doi: 10.1001/archgenpsychiatry.2010.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ring RH. A Complicated Picture of Oxytocin Action in the Central Nervous System Revealed. Biological Psychiatry. 2011;69(9):818–819. doi: 10.1016/j.biopsych.2011.03.020. dx.doi.org/10.1016/j.biopsych.2011.03.020. [DOI] [PubMed] [Google Scholar]
- Rutter M, Bailey A, Lord C. SCQ: Social Communication Questionnaire. Los Angeles, CA: Western Psychological Services; 2003. [Google Scholar]
- Sala M, Braida D, Lentini D, Busnelli M, Bulgheroni E, Capurro V, Chini B. Pharmacologic rescue of impaired cognitive flexibility, social deficits, increased aggression, and seizure susceptibility in oxytocin receptor null mice: a neurobehavioral model of autism. Biological Psychiatry. 2011;69(9):875–882. doi: 10.1016/j.biopsych.2010.12.022. [DOI] [PubMed] [Google Scholar]
- Sparrow SSC, Cicchetti DV, Balla DA. Vineland Adaptive Behavior Scales, Second Edition (Vineland-II) Pearson; 2005. [Google Scholar]
- Stavropoulos KK, Carver LJ. Research Review: Social motivation and oxytocin in autism - implications for joint attention development and intervention. Journal of Child Psychology and Psychiatry. 2013;54(6):603–618. doi: 10.1111/jcpp.12061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strathearn L. The elusive etiology of autism: nature and nurture? Frontiers in Behavioral Neuroscience. 2009;3:11. doi: 10.3389/neuro.08.011.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strathearn L, Fonagy P, Amico JA, Montague PR. Adult attachment predicts mother’s brain and oxytocin response to infant cues. Neuropsychopharmacology. 2009;34(13):2655–2666. doi: 10.1038/npp.2009.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strathearn L, Iyengar U, Fonagy P, Kim S. Maternal oxytocin response during mother-infant interaction: Associations with adult temperament. Hormones and Behavior. 2012;61(3):429–435. doi: 10.1016/j.yhbeh.2012.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tobii. Accuracy and precision test report: Tobii T60 Eye tracker. Tobii Technology AB; 2011. [Google Scholar]
- Valstad M, Alvares GA, Egknud M, Matziorinis AM, Andreassen OA, Westlye LT, Quintana DS. The correlation between central and peripheral oxytocin concentrations: a systematic review and meta-analysis. Neuroscience and Biobehavioral Reviews. 2017;78:117–124. doi: 10.1016/j.neubiorev.2017.04.017. [DOI] [PubMed] [Google Scholar]
- Watanabe T, Kuroda M, Kuwabara H, Aoki Y, Iwashiro N, Tatsunobu N, Yamasue H. Clinical and neural effects of six-week administration of oxytocin on core symptoms of autism. Brain. 2015;138(Pt 11):3400–3412. doi: 10.1093/brain/awv249. [DOI] [PubMed] [Google Scholar]
- Yatawara CJ, Einfeld SL, Hickie IB, Davenport TA, Guastella AJ. The effect of oxytocin nasal spray on social interaction deficits observed in young children with autism: a randomized clinical crossover trial. Molecular Psychiatry. 2016;21:1225–1231. doi: 10.1038/mp.2015.162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zoghbi HY, Bear MF. Synaptic dysfunction in neurodevelopmental disorders associated with autism and intellectual disabilities. Cold Spring Harbor Perspectives in Biology. 2012;4(3) doi: 10.1101/cshperspect.a009886. [DOI] [PMC free article] [PubMed] [Google Scholar]