

Abstract
Background
Opioid agonist therapy (OAT) is the standard of care for pregnant women with opioid use disorder (OUD). Medicaid coverage policies may strongly influence OAT use in this group.
Objective
To examine the association between Medicaid coverage of methadone maintenance and planned use of OAT in the publicly-funded treatment system.
Research Design
Retrospective cross-sectional analysis of treatment admissions in 30 states extracted from the Treatment Episode Data Set (2013 and 2014).
Subjects
Medicaid-insured pregnant women with OUD (n=3,354 treatment admissions).
Measures
The main outcome measure was planned use of OAT on admission. The main exposure was state Medicaid coverage of methadone maintenance. Using multivariable logistic regression models adjusting for sociodemographic, substance use, and treatment characteristics, we compared the probability of planned OAT use in states with Medicaid coverage of methadone maintenance versus states without coverage.
Results
71% of pregnant women admitted to OUD treatment were 18 to 29 years old, 85% were White non-Hispanic, and 56% used heroin. Overall, 74% of admissions occurred in the 18 states with Medicaid coverage of methadone maintenance and 53% of admissions involved planned use of OAT. Compared to states without Medicaid coverage of methadone maintenance, admissions in states with coverage were significantly more likely to involve planned OAT use (adjusted difference: 32.9 percentage points, 95% CI: 19.2, 46.7).
Conclusions
Including methadone maintenance in the Medicaid benefit is essential to increasing OAT among pregnant women with OUD and should be considered a key policy strategy to enhance outcomes for mothers and newborns.
MeSH key words: pregnancy, heroin dependence, opioid use disorder, opioid substitution therapy, methadone maintenance, Medicaid, insurance, access to care
Introduction
Pregnant women with untreated opioid use disorder (OUD) are at high risk for poor maternal outcomes including infections, overdose, and pregnancy-associated death, as well as poor fetal and perinatal outcomes such as fetal growth restriction, intrauterine fetal demise, placental abruption, and preterm delivery.(1–5) Opioid agonist therapy (OAT), consisting of methadone or buprenorphine in addition to counseling, is associated with reduced illicit opioid use and reduced craving, reduced HIV and viral hepatitis seroconversion, and lower relapse rates compared to counseling alone.(6–10) For pregnant women specifically, OAT prevents complications associated with illicit opioid use and withdrawal, encourages adherence to prenatal care, and reduces criminal activity and high-risk sexual behaviors.(1,3,4,11–13) Because of these benefits, current clinical guidelines recommend OAT as the standard of care for pregnant women with OUD.(1,3,12,14,15)
While the increasing availability of buprenorphine in office-based settings has expanded access to OAT,(16,17) public and private substance use disorder treatment facilities that receive public funding (i.e., the publicly-funded treatment system) remain an important source of care. Admitting over 8,000 pregnant women with OUD annually, this treatment system consists of specialty opioid treatment programs, which provide OAT (overwhelmingly methadone) along with counseling and supportive services, as well as programs that provide counseling and supportive services without OAT.(18–21) Despite being the recommended standard of care, only 46% of admissions of pregnant women to the publicly-funded treatment system in 2013 included OAT in the treatment plan.(22)
State Medicaid programs can elect to provide or deny coverage of methadone maintenance in their benefit package. Because Medicaid covers half of all pregnancies and OUD disproportionately affects low-income individuals, such coverage policies could have a profound impact on OUD treatment.(23–27) In a recent study, Medicaid coverage of methadone maintenance was associated with a 27 percentage point higher probability of OAT being included in the treatment plan (42.4% in states with coverage versus 15.8% in states without coverage).(28) The impact of Medicaid coverage of methadone maintenance on pregnant women is unclear and, to our knowledge, has not been the focus of any previous studies.
Given the substantial risk of untreated OUD and potential changes to Medicaid under consideration, an understanding of the impact of Medicaid coverage policies on OAT use among pregnant women is critical. Focusing on the publicly-funded treatment system, the goal of the current study is to estimate the association between state Medicaid coverage of methadone maintenance and use of OAT among pregnant women.
Methods
We obtained data on pregnant women entering OUD treatment from the 2013 and 2014 Treatment Episode Data Set (TEDS). Maintained by the Substance Abuse and Mental Health Services Administration of the U.S. Department of Health and Human Services, TEDS contains information on approximately 1.6 million annual admissions to the publicly-funded treatment system.(19) Each observation in TEDS represents a treatment admission or transfer from another facility and cannot be linked to unique individuals; therefore, individual patients may appear more than once. Because methadone is the medication used in 98.6% of patients receiving OAT in the publicly-funded treatment system, we focused on state Medicaid program coverage of methadone maintenance, obtained from a survey with data through 2013.(18,29) For states with missing information from this survey (CO, IA, KS, ND, NH), we used information from a 2013 survey from the American Society of Addiction Medicine.(30)
From TEDS, we identified all pregnant women age 18–44 who reported primarily using either heroin or opioid analgesics, were admitted to residential or outpatient treatment (i.e., excluding short-term detoxification), and had Medicaid insurance; health insurance is an optional variable reported for >75% of admissions by 30 states. Our main outcome measure was planned use of OAT (i.e., whether methadone or buprenorphine was part of the treatment plan documented on admission). TEDS includes a variable indicating planned OAT use, but does not identify the specific medication planned, although it is overwhelmingly methadone.(18) Our main exposure of interest was state Medicaid coverage of methadone maintenance, a state-level variable which we linked to admissions data. We also included several covariates in our analyses: sociodemographic (age, race/ethnicity, education), substance use (e.g., heroin use), and treatment characteristics (e.g., referral source and service setting). Service setting was classified as residential, intensive outpatient (defined as ≥2 hours of service per day for ≥3 days per week), and non-intensive outpatient.(31) To account for differences in Medicaid-eligible populations in each state, we also included the 2013 state Medicaid income eligibility limit as a covariate.(32)
Complete information was available for 92.2% of relevant admissions. To account for missing data, we performed a multiple imputation procedure with chained equations.(33) We assumed data were missing at random and created 10 imputed datasets using the main outcome, main exposure, Census division of residence (the procedure did not converge with state of residence), and all covariates. Standard errors were adjusted to account for the additional uncertainty associated with imputed estimates.
Statistical analysis
First, we calculated descriptive statistics of sociodemographic, substance use, and treatment characteristics for our study population. Next, we used multivariable logistic regression models to estimate the association between state Medicaid coverage of methadone maintenance and planned use of OAT. For this model, the dependent variable was planned use of OAT and the main independent variable was state coverage of methadone maintenance. We included all sociodemographic, substance use, and treatment characteristic variables that were different between admissions in states with and without Medicaid coverage of methadone maintenance with a P value ≤ 0.2.(34) We also created models stratified by service setting. To account for clustering of data at the state level, we used cluster-robust standard errors to calculate 95% confidence intervals in all models. Finally, to calculate the predicted probabilities of OAT use, adjusting for covariates, we used predictive margins. All analyses were performed using Stata 13.1 (StataCorp, College Station, TX) with a two-tailed P value ≤ 0.05 considered statistically significant.
Sensitivity analyses
First, to determine the impact of our multiple imputation procedure on study findings, we repeated our main analyses using unimputed data. Next, as Medicaid coverage of methadone maintenance may be associated with other factors that could encourage OAT use more broadly, we conducted a sensitivity analysis to determine if differences in planned OAT use were observed among Medicaid-insured pregnant women only or also among non-Medicaid-insured pregnant women (who should not be directly affected by Medicaid coverage policies). Overall and by service setting, we first calculated the regression-adjusted difference in OAT use between coverage states versus no coverage states for Medicaid-insured pregnant women. Next, we calculated the regression-adjusted difference in planned OAT use between coverage states versus no coverage states for non-Medicaid pregnant women. Finally, we subtracted those two differences (i.e., a differences-in-differences analysis). A result that is positive and significantly different than 0 indicates a higher rate of planned OAT use associated with state Medicaid coverage of methadone maintenance over and above the difference seen for non-Medicaid pregnant women, suggesting a specific effect of coverage on Medicaid-insured pregnant women.
Results
Of 3,354 admissions to OUD treatment among Medicaid-insured pregnant women, 71.2% were 18 to 29 years old and 84.9% were White non-Hispanic (Table 1). About half used heroin (55.9%) and had daily opioid use prior to treatment (57.5%). Compared to states without Medicaid coverage of methadone maintenance, admissions in states with coverage were more likely to involve heroin use and daily use of opioids prior to treatment, and were less likely to be the first treatment episode or to be referred from the criminal justice system.
Table 1.
Demographic and substance use characteristics of Medicaid-insured pregnant women admitted to specialty opioid use disorder treatment in 30 states (n=3,354)a
| Characteristic | Overall, % (95% CI) | State Medicaid coverage of methadone maintenance
|
P | |
|---|---|---|---|---|
| No (n=863), % (95% CI)b | Yes (n=2,491), % (95% CI)c | |||
| Demographics | ||||
| Age | 0.20 | |||
| 18 to 29 | 71.2 (69.7, 72.7) | 72.9 (69.9, 75.9) | 70.6 (68.8, 72.4) | |
| 30 to 44 | 28.8 (27.3, 30.3) | 27.1 (24.1, 30.1) | 29.4 (27.6, 31.2) | |
| Race/ethnicity | ||||
| White, non-Hispanic | 84.9 (83.7, 86.2) | 89.2 (87.1, 91.3) | 83.5 (82.0, 84.9) | <0.001 |
| Black, non-Hispanic | 6.0 (5.2, 6.8) | 5.8 (4.2, 7.4) | 6.1 (5.2, 7.1) | |
| Hispanic/Latina, of any race | 5.5 (4.7, 6.2) | 2.0 (1.0, 2.9) | 6.7 (5.7, 7.6) | |
| Another race or multiple races | 3.6 (2.9, 4.2) | 3.0 (1.9, 4.2) | 3.8 (3.0, 4.5) | |
| Education | 0.29 | |||
| Some high school | 31.9 (30.3, 33.6) | 32.7 (29.1, 36.2) | 31.7 (29.8, 33.5) | |
| High school graduate | 46.2 (44.5, 47.9) | 43.9 (40.5, 47.3) | 47.0 (45.1, 49.0) | |
| Some college or more | 21.8 (20.4, 23.3) | 23.4 (20.3, 26.6) | 21.3 (19.7, 22.9) | |
| Substance use and treatment | ||||
| Daily opioid use prior to treatment | 57.5 (55.8, 59.2) | 42.8 (39.5, 46.1) | 62.5 (60.7, 64.5) | <0.001 |
| Heroin as primary substance used | 55.9 (54.2, 57.6) | 36.5 (33.3, 39.7) | 62.6 (60.7, 64.5) | <0.001 |
| First episode of treatment | 25.7 (24.2, 27.3) | 35.0 (31.8, 38.2) | 22.5 (20.8, 24.2) | <0.001 |
| Referral to treatment from the criminal justice system | 12.8 (11.6, 13.9) | 17.0 (14.5, 19.5) | 11.3 (10.0, 12.6) | <0.001 |
| Service setting | 0.007 | |||
| Residential | 19.9 (18.5, 21.2) | 16.2 (13.8, 18.7) | 21.2 (19.6, 22.8) | |
| Intensive outpatientd | 15.0 (13.8, 16.2) | 15.1 (12.7, 17.5) | 14.9 (13.5, 16.3) | |
| Non-intensive outpatient | 65.1 (63.5, 66.8) | 68.7 (65.6, 71.8) | 63.9 (62.0, 65.8) | |
Data are unique at the level of the treatment admission; therefore, individual patients may be included more than once
The 12 states that do not cover methadone maintenance in Medicaid are: AR, IA, IL, KS, KY, LA, MS, MT, SC, SD, TN, WV
The 18 states that cover methadone maintenance in Medicaid are: AK, AL, CO, DE, HI, MA, MD, ME, MO, ND, NH, NJ, NM, OR, PA, TX, UT, WY
Intensive outpatient treatment is defined as ≥2 hours of service per day for ≥3 days per week
Overall, OAT use was planned in 52.9% of admissions but varied by service setting (Table 2, Figure). Compared to states without Medicaid coverage of methadone maintenance, admissions in states with coverage were more likely to involve planned OAT use (adjusted difference: 32.9 percentage points, 95% CI: 19.2, 46.7). By setting, this relationship persisted in intensive and non-intensive outpatient settings but was not significant in residential settings (adjusted difference: 14.3 percentage points, 95% CI: −0.7, 29.2).
Table 2.
Use of opioid agonist therapy among Medicaid-insured pregnant women admitted to specialty opioid use disorder treatment in states with Medicaid coverage of methadone maintenance versus no coverage (n=3,354)a
| Service setting | Unadjusted | Regression-adjustedb | ||||
|---|---|---|---|---|---|---|
|
| ||||||
| Opioid agonist treatment use, % (95% CI) | State Medicaid coverage of methadone maintenance | State Medicaid coverage of methadone maintenance | ||||
| Noc, % (95% CI) | Yesd, % (95% CI) | No, % (95% CI) | Yes, % (95% CI) | Adjusted difference, % (95% CI) | ||
| All settings | 52.9 (51.2, 54.6) | 22.7 (19.9, 25.6) | 63.4 (61.5, 65.3) | 28.1 (19.7, 36.4) | 61.0 (51.4, 70.5) | 32.9 (19.2, 46.7) |
| Residential | 30.7 (27.2, 34.3) | 15.4 (9.3, 21.4) | 34.8 (30.7, 38.9) | 19.1 (9.1, 29.0) | 33.3 (21.7, 45.0) | 14.3 (-0.7, 29.2) |
| Intensive outpatiente | 36.3 (32.0, 40.6) | 4.8 (1.0, 8.5) | 47.3 (42.1, 52.5) | 5.3 (0, 11.7) | 45.4 (24.2, 66.6) | 40.2 (15.5, 64.8) |
| Non-intensive outpatient | 63.5 (61.4, 65.5) | 28.4 (24.7, 32.1) | 76.6 (74.5, 78.7) | 36.0 (27.6, 44.4) | 73.9 (65.1, 82.7) | 37.9 (25.1, 50.7) |
Data are unique at the level of the treatment admission; therefore, individual patients may be included more than once
Estimates adjusted for age, race/ethnicity, daily use prior to treatment, heroin as primary substance used, first episode of treatment, referral to treatment from the criminal justice system, and state Medicaid income eligibility limit
The 12 states that do not cover methadone maintenance in Medicaid are: AR, IA, IL, KS, KY, LA, MS, MT, SC, SD, TN, WV
The 18 states that cover methadone maintenance in Medicaid are: AK, AL, CO, DE, HI, MA, MD, ME, MO, ND, NH, NJ, NM, OR, PA, TX, UT, WY
Intensive outpatient treatment is defined as ≥2 hours of service per day for ≥3 days per week
Figure.
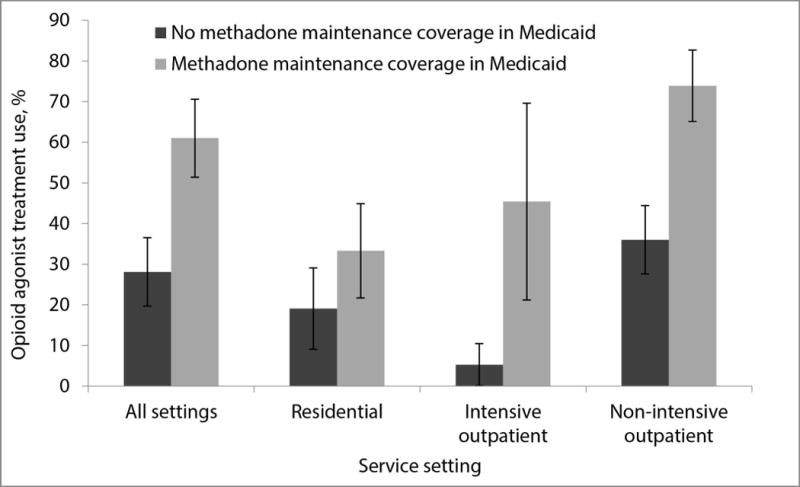
Use of opioid agonist therapy among Medicaid-insured pregnant women admitted to specialty opioid use disorder treatment in states with Medicaid coverage of methadone maintenance versus no coverage, overall and by service setting (n=3,354)a
aEstimates adjusted for age, race, daily use prior to treatment, heroin as primary substance used, first episode of treatment, referral to treatment from the criminal justice system, and state Medicaid income eligibility limit
In sensitivity analyses, estimates using unimputed data were similar in direction and magnitude to estimates using multiply-imputed data (see Table 1 and 2, Supplemental Digital Content). The overall adjusted difference between Medicaid-insured pregnant women and non-Medicaid pregnant women was 21.2 percentage points (95% CI: 4.6, 37.9), indicating that Medicaid-insured pregnant women experienced higher rates of planned OAT use in coverage states versus no coverage states, which was over and above the higher rate experienced by non-Medicaid pregnant women (Table 3). However, these results varied by setting, with a significant adjusted difference in residential and intensive outpatient settings but not in non-intensive outpatient settings (13.2 percentage points, 95% CI: −1.1, 27.4).
Table 3.
Use of opioid agonist therapy among Medicaid-insured pregnant women admitted to specialty opioid use disorder treatment, compared with other pregnant women, in states with Medicaid coverage of methadone maintenance versus no coverage (n=6,532)a,b
| State Medicaid coverage of methadone maintenance | P | ||
|---|---|---|---|
| No, % (95% CI) | Yes, % (95% CI) | ||
| All settings | |||
| Medicaid | 28.4 (19.9, 37.0) | 60.6 (50.9, 70.4) | |
| All othersc | 36.5 (28.2, 44.8) | 47.6 (34.8, 60.4) | |
| Adjusted differenced | 21.2 (4.6, 37.9) | 0.01 | |
| Residential | |||
| Medicaid | 18.7 (9.5, 27.9) | 32.0 (20.5, 43.5) | |
| All others | 16.8 (6.3, 27.3) | 14.1 (5.3, 23.0) | |
| Adjusted difference | 16.1 (0.8, 31.4) | 0.04 | |
| Intensive outpatiente | |||
| Medicaid | 6.8 (0, 14.5) | 39.6 (14.8, 64.5) | |
| All others | 17.4 (0, 38.7) | 21.8 (6.8, 36.7) | |
| Adjusted difference | 37.0 (8.1, 66.0) | 0.01 | |
| Non-intensive outpatient | |||
| Medicaid | 38.0 (30.4, 45.6) | 73.9 (64.8, 83.0) | |
| All others | 48.6 (41.4, 55.6) | 69.5 (59.4, 79.7) | |
| Adjusted difference | 13.2 (−1.1, 27.4) | 0.07 | |
Data are unique at the level of the treatment admission; therefore, individual patients may be included more than once
Estimates adjusted for age, race/ethnicity, daily use prior to treatment, heroin as primary substance used, first episode of treatment, referral to treatment from the criminal justice system, and state Medicaid income eligibility limit
Includes those with private insurance, non-Medicaid public insurance, and no insurance
Adjusted difference is calculated by subtracting predicted probabilities in Medicaid row (Difference 1), subtracting same predicted probabilities in All others row (Difference 2), and then subtracting Difference 2 from Difference 1 (e.g. [60.6 − 28.4] − [47.6 − 36.5] = 21.2)
Intensive outpatient treatment is defined as ≥2 hours of service per day for ≥3 days per week
Discussion
In a study of admissions to OUD treatment among Medicaid-insured pregnant women in 30 states, we found that Medicaid coverage of methadone maintenance was associated with a 33 percentage point higher probability of planned OAT use. Our findings extend, and are similar to, previous work showing that Medicaid coverage of methadone maintenance is associated with OAT use in the general adult population entering OUD treatment.(28)
Overall, only about half of admissions of pregnant women to specialty OUD treatment had OAT as part of the treatment plan. While we found evidence that Medicaid coverage policies play a role, several other patient, provider, and policy factors likely contribute to low rates of OAT. Pregnant women with OUD may experience stigma and have negative perceptions of OAT, both of which serve as barriers to treatment and retention.(35–38) Pregnant women may also be treated by providers who prefer non-OAT approaches, lack information about OAT, or doubt the clinical effectiveness of OAT.(39–41) Furthermore, pregnant women may not receive OAT or may be given sub-therapeutic doses because of concerns about neonatal abstinence syndrome, a postnatal withdrawal syndrome characterized by central nervous system hyperirritability and autonomic nervous system dysfunction, which is an expected and treatable outcome of maternal OAT.(3,14,42,43) Finally, as of 2015, at least 18 states had laws considering substance use during pregnancy to be child abuse and 1 considered it assault.(44,45) Research suggests such laws are linked with lower use of OAT, potentially because pregnant women fear that these laws apply to OAT.(45)
Despite their status as a more intensive level of care, we found that admissions to residential and intensive outpatient programs were much less likely to have OAT as part of their treatment plan than admissions to non-intensive outpatient programs (many of which are specialized opioid treatment programs). However, in both our primary and sensitivity analyses, we found Medicaid coverage of methadone maintenance to be associated with higher rates of planned OAT use in residential and intensive outpatient settings. This finding suggests that Medicaid coverage policies could play a critical role in promoting access to OAT in settings that traditionally have not offered it.
Although state Medicaid programs more commonly cover buprenorphine than methadone maintenance, there is rationale for coverage of both treatment options. In pregnant women, there is growing evidence that buprenorphine causes less severe neonatal abstinence syndrome, potentially leading to less costly hospitalizations for neonates.(14) However, methadone maintenance is superior to buprenorphine in retaining patients in treatment, although data in pregnant women are limited.(10,14) Furthermore, methadone maintenance is delivered in opioid treatment programs which provide on-site counseling and often other supportive services such as psychiatric services.(1,20,21) In contrast, office-based buprenorphine treatment usually consists of less frequent patient-provider contact and counseling is not necessarily required. Therefore, beyond retention differences in clinical trials, methadone maintenance may also be more appropriate for the subset of pregnant women who could benefit from a more structured treatment setting.
This study has several limitations. First, TEDS only contains data from specialty treatment facilities that receive public funding, therefore we could not determine the impact of Medicaid coverage policies on OAT use in private facilities that do not receive public funding or in office-based care (stand-alone or embedded into prenatal care). If Medicaid-insured pregnant women in states without Medicaid coverage of methadone maintenance preferentially access or are referred to private facilities or office-based settings for OAT (i.e., outside the scope of our data source), our estimates of OAT use in these states may be conservative. Second, as our study relies on cross-sectional data, we could not determine the causal impact of changing Medicaid coverage policies on OAT use. In sensitivity analyses, we found higher rates of OAT use among non-Medicaid-insured pregnant women in states with Medicaid coverage of methadone maintenance versus no coverage in non-intensive outpatient settings, suggesting that our findings may be due, at least in part, to differences between states other than Medicaid coverage of methadone maintenance. Third, pregnant women in residential treatment facilities may receive OAT outside of the treatment facility (e.g., through a prenatal provider or an opioid treatment program) which may have resulted in an underestimate of planned OAT use in residential settings. Finally, as our data source only contains data from treatment admissions, we cannot determine treatment received over time (e.g., planned taper versus maintenance) or the impact of Medicaid coverage policies on maternal, fetal, or perinatal outcomes. Moreover, the postpartum period is a high-risk time for overdose death; however, Medicaid coverage through the pregnancy eligibility pathway ends 60 days postpartum.(5,46,47) Changes in coverage status postpartum may disrupt access to OAT, particularly in states where Medicaid expansion did not occur. Further research is needed to assess the impact of OAT coverage policies on a broad range of outcomes in pregnant women.
In the publicly-funded treatment system, Medicaid coverage of methadone maintenance is associated with a substantially higher rate of planned OAT use—the recommended standard of care—among Medicaid-insured pregnant women with OUD. While other barriers to OAT use persist, our findings suggest that including Medicaid coverage for methadone maintenance could significantly improve outcomes for pregnant women with OUD.
Supplementary Material
Acknowledgments
This study was supported in part by the CTSA Grant 1 UL1 TR001073 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH).
Footnotes
The authors have no potential conflicts of interest to disclose.
Contributor Information
Marcus A. Bachhuber, Division of General Internal Medicine, Department of Medicine, Montefiore Medical Center/Albert Einstein College of Medicine, 3300 Kossuth Ave, Bronx, NY 10467, Phone: 718-920-7102; Fax: 718-561-5165.
Pooja Mehta, Department of Obstetrics and Gynecology, Boston University School of Medicine, 85 East Concord Street, 6th floor, Boston MA 02118, Phone: 617-414-5184.
Laura Faherty, RAND Corporation, 20 Park Plaza, Suite 920, Boston, MA 02116, Phone: (617) 338-2059 x8693.
Brendan Saloner, Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA, 624 N Broadway Room 344, Baltimore, MD 21205, Phone: 410-502-2116.
References
- 1.Center for Substance Abuse Treatment. Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2005. (Treatment Improvement Protocol (TIP) Series, No. 43). [PubMed] [Google Scholar]
- 2.Kaltenbach K, Berghella V, Finnegan L. Opioid dependence during pregnancy. Effects and management. Obstet Gynecol Clin North Am. 1998;25:139–151. doi: 10.1016/s0889-8545(05)70362-4. [DOI] [PubMed] [Google Scholar]
- 3.ACOG Committee. Opinion No. 524: Opioid abuse, dependence, and addiction in pregnancy. Obstet Gynecol. 2012;119:1070–1076. doi: 10.1097/AOG.0b013e318256496e. [DOI] [PubMed] [Google Scholar]
- 4.Finnegan LP. Treatment issues for opioid-dependent women during the perinatal period. J Psychoactive Drugs. 1991;23:191–201. doi: 10.1080/02791072.1991.10472236. [DOI] [PubMed] [Google Scholar]
- 5.Mehta PK, Bachhuber MA, Hoffman R, et al. Deaths From Unintentional Injury, Homicide, and Suicide During or Within 1 Year of Pregnancy in Philadelphia. Am J Public Health. 2016;106:2208–2210. doi: 10.2105/AJPH.2016.303473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Joseph H, Stancliff S, Langrod J. Methadone maintenance treatment (MMT): a review of historical and clinical issues. Mt Sinai J Med. 2000;67:347–364. [PubMed] [Google Scholar]
- 7.O’Connor PG, Fiellin DA. Pharmacologic treatment of heroin-dependent patients. Ann Intern Med. 2000;133:40–54. doi: 10.7326/0003-4819-133-1-200007040-00008. [DOI] [PubMed] [Google Scholar]
- 8.Kakko J, Svanborg KD, Kreek MJ, et al. 1-year retention and social function after buprenorphine-assisted relapse prevention treatment for heroin dependence in Sweden: a randomised, placebo-controlled trial. Lancet. 2003;361:662–668. doi: 10.1016/S0140-6736(03)12600-1. [DOI] [PubMed] [Google Scholar]
- 9.Gerra G, Ferri M, Polidori E, et al. Long-term methadone maintenance effectiveness: psychosocial and pharmacological variables. J Subst Abuse Treat. 2003;25:1–8. doi: 10.1016/s0740-5472(03)00031-x. [DOI] [PubMed] [Google Scholar]
- 10.Amato L, Davoli M, Perucci CA, et al. An overview of systematic reviews of the effectiveness of opiate maintenance therapies: available evidence to inform clinical practice and research. J Subst Abuse Treat. 2005;28:321–329. doi: 10.1016/j.jsat.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 11.Jones HE, O’Grady KE, Malfi D, et al. Methadone maintenance vs. methadone taper during pregnancy: maternal and neonatal outcomes. Am J Addict. 2008;17:372–386. doi: 10.1080/10550490802266276. [DOI] [PubMed] [Google Scholar]
- 12.Goler NC, Armstrong MA, Taillac CJ, et al. Substance abuse treatment linked with prenatal visits improves perinatal outcomes: a new standard. J Perinatol. 2008;28:597–603. doi: 10.1038/jp.2008.70. [DOI] [PubMed] [Google Scholar]
- 13.Svikis DS, Golden AS, Huggins GR, et al. Cost-effectiveness of treatment for drug-abusing pregnant women. Drug Alcohol Depend. 1997;45:105–113. doi: 10.1016/s0376-8716(97)01352-5. [DOI] [PubMed] [Google Scholar]
- 14.Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320–2331. doi: 10.1056/NEJMoa1005359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Young JL, Martin PR. Treatment of opioid dependence in the setting of pregnancy. Psychiatr Clin North Am. 2012;35:441–460. doi: 10.1016/j.psc.2012.03.008. [DOI] [PubMed] [Google Scholar]
- 16.Stein BD, Pacula RL, Gordon AJ, et al. Where Is Buprenorphine Dispensed to Treat Opioid Use Disorders? The Role of Private Offices, Opioid Treatment Programs, and Substance Abuse Treatment Facilities in Urban and Rural Counties. Milbank Q. 2015;93:561–583. doi: 10.1111/1468-0009.12137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dick AW, Pacula RL, Gordon AJ, et al. Growth In Buprenorphine Waivers For Physicians Increased Potential Access To Opioid Agonist Treatment, 2002–11. Health Aff (Millwood) 2015;34:1028–1034. doi: 10.1377/hlthaff.2014.1205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Substance Abuse and Mental Health Services Administration. 2011 Opioid Treatment Program Survey: Data on Substance Abuse Treatment Facilities with OTPs. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2011. (BHSIS Series S-65, HHS Publication No. (SMA) 14–4807). [Google Scholar]
- 19.Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Treatment Episode Data Set (TEDS): 2004–2014. State Admissions to Substance Abuse Treatment Services. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2015. (BHSIS Series S-85, HHS Publication No. (SMA) 16–4987). [Google Scholar]
- 20.Bachhuber MA, Southern WN, Cunningham CO. Profiting and providing less care: comprehensive services at for-profit, nonprofit, and public opioid treatment programs in the United States. Med Care. 2014;52:428–434. doi: 10.1097/MLR.0000000000000121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bachhuber MA, Cunningham CO. Changes in testing for human immunodeficiency virus, sexually transmitted infections, and hepatitis C virus in opioid treatment programs. JAMA. 2013;310:2671–2672. doi: 10.1001/jama.2013.278456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hand DJ, Short VL, Abatemarco DJ. Substance use, treatment, and demographic characteristics of pregnant women entering treatment for opioid use disorder differ by United States census region. J Subst Abuse Treat. 2017 doi: 10.1016/j.jsat.2017.01.011. [DOI] [PubMed] [Google Scholar]
- 23.Murphy K, Kershner D. 2014 Maternal and Child Health Update: States Are Using Medicaid and CHIP to Improve Health Outcomes for Mothers and Children. Washington, DC: National Governors Association Center for Best Practices; 2015. [Google Scholar]
- 24.Jones CM, Logan J, Gladden RM, et al. Vital Signs: Demographic and Substance Use Trends Among Heroin Users - United States, 2002–2013. MMWR Morb Mortal Wkly Rep. 2015;64:719–725. [PMC free article] [PubMed] [Google Scholar]
- 25.Saha TD, Kerridge BT, Goldstein RB, et al. Nonmedical Prescription Opioid Use and DSM-5 Nonmedical Prescription Opioid Use Disorder in the United States. J Clin Psychiatry. 2016;77:772–780. doi: 10.4088/JCP.15m10386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Stein BD, Mendelsohn J, Gordon AJ, et al. Opioid analgesic and benzodiazepine prescribing among Medicaid-enrollees with opioid use disorders: The influence of provider communities. J Addict Dis. 2017;36:14–22. doi: 10.1080/10550887.2016.1211784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Saloner B, Karthikeyan S. Changes in Substance Abuse Treatment Use Among Individuals With Opioid Use Disorders in the United States, 2004–2013. Jama. 2015;314:1515–1517. doi: 10.1001/jama.2015.10345. [DOI] [PubMed] [Google Scholar]
- 28.Saloner B, Stoller KB, Barry CL. Medicaid Coverage for Methadone Maintenance and Use of Opioid Agonist Therapy in Specialty Addiction Treatment. Psychiatr Serv. 2016;67:676–679. doi: 10.1176/appi.ps.201500228. [DOI] [PubMed] [Google Scholar]
- 29.Burns RM, Pacula RL, Bauhoff S, et al. Policies related to opioid agonist therapy for opioid use disorders: The evolution of state policies from 2004 to 2013. Subst Abus. 2016;37:63–69. doi: 10.1080/08897077.2015.1080208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gelber Rinaldo S, Rinaldo DW. Advancing Access to Addiction Medications: Implications for Opioid Addiction Treatment. Chevy Chase, MD: Medicine ASoA; 2013. Availability without accessibility? State Medicaid coverage and authorization requirements for opioid dependence medications. [Google Scholar]
- 31.Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Treatment Episode Data Set (TEDS) State Instruction Manual with State TEDS Submission System (STTS) Guide. Version 3.2. Rockville, MD: SAMHSA; 2014. [Google Scholar]
- 32.Herberlein M, Brooks T, Alker J, et al. Getting into Gear for 2014: Findings from a 50-State Survey of Eligibility, Enrollment, Renewal, and Cost-Sharing Policies in Medicaid and CHIP, 2012–2013. Washington, DC: The Henry J. Kaiser Family Foundation; 2013. [Google Scholar]
- 33.White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. 2011;30:377–399. doi: 10.1002/sim.4067. [DOI] [PubMed] [Google Scholar]
- 34.Vittinghoff E, Glidden DV, Shiboski SC, et al. Regression Methods in Biostatistics. New York, NY: Springer; 2012. [Google Scholar]
- 35.Jones HE, Deppen K, Hudak ML, et al. Clinical care for opioid-using pregnant and postpartum women: the role of obstetric providers. Am J Obstet Gynecol. 2014;210:302–310. doi: 10.1016/j.ajog.2013.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Schempf AH, Strobino DM. Drug use and limited prenatal care: an examination of responsible barriers. Am J Obstet Gynecol. 2009;200:412.e411–410. doi: 10.1016/j.ajog.2008.10.055. [DOI] [PubMed] [Google Scholar]
- 37.Roberts SC, Nuru-Jeter A. Women’s perspectives on screening for alcohol and drug use in prenatal care. Womens Health Issues. 2010;20:193–200. doi: 10.1016/j.whi.2010.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Roberts SC, Pies C. Complex calculations: how drug use during pregnancy becomes a barrier to prenatal care. Matern Child Health J. 2011;15:333–341. doi: 10.1007/s10995-010-0594-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Rieckmann T, Daley M, Fuller BE, et al. Client and counselor attitudes toward the use of medications for treatment of opioid dependence. J Subst Abuse Treat. 2007;32:207–215. doi: 10.1016/j.jsat.2006.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Knudsen HK, Abraham AJ, Oser CB. Barriers to the implementation of medication-assisted treatment for substance use disorders: the importance of funding policies and medical infrastructure. Eval Program Plann. 2011;34:375–381. doi: 10.1016/j.evalprogplan.2011.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Knudsen HK, Ducharme LJ, Roman PM. The adoption of medications in substance abuse treatment: associations with organizational characteristics and technology clusters. Drug Alcohol Depend. 2007;87:164–174. doi: 10.1016/j.drugalcdep.2006.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Jones HE, Martin PR, Heil SH, et al. Treatment of opioid-dependent pregnant women: clinical and research issues. J Subst Abuse Treat. 2008;35:245–259. doi: 10.1016/j.jsat.2007.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Calvin C, Moriarty H. A special type of ‘hard-to-reach’ patient: experiences of pregnant women on methadone. J Prim Health Care. 2010;2:61–69. [PubMed] [Google Scholar]
- 44.Guttmacher Institute. State Policies in Brief: Substance Abuse During Pregnancy. Washington, DC: Guttmacher Institute; 2015. [Google Scholar]
- 45.Angelotta C, Weiss CJ, Angelotta JW, et al. A Moral or Medical Problem? The Relationship between Legal Penalties and Treatment Practices for Opioid Use Disorders in Pregnant Women. Womens Health Issues. 2016;26:595–601. doi: 10.1016/j.whi.2016.09.002. [DOI] [PubMed] [Google Scholar]
- 46.Metz TD, Rovner P, Hoffman MC, et al. Maternal Deaths From Suicide and Overdose in Colorado, 2004–2012. Obstet Gynecol. 2016;128:1233–1240. doi: 10.1097/AOG.0000000000001695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Gifford K, Walls J, Ranji U, et al. Medicaid coverage of pregnancy and perinatal benefits: Results from a state survey. Washington, DC: The Henry J. Kaiser Family Foundation; 2017. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.