

Abstract
Background:
Recently we have upgraded our Varian Clinac 2100CD with a 6MV FFF beam, this upgrade being the first of its kind in our country. Even though the dosimetric characteristics of FFF beams have been reported both in experimental and Monte Carlo studies, application in planning and delivery is complex. The aim of this study was to validate the commissioning of upgraded FFF beams dosimetrically using AAPM TG-119 bench mark plans for VMAT and to make a comparison with IMRT plans for both flattened filtered and FFF beams.
Materials and Methods:
AAPM TG-119 proposes a set of test clinical cases for testing the accuracy of IMRT planning and delivery systems. For these clinical cases we generated four treatment plans using IMRT FF, IMRT FFF, VMAT FF and VMAT FFF on a Varian Clinac 2100CD machine equipped with a millennium 120 MLC in Eclipse treatment planning system. Dose prescription and planning objectives were set according to the TG-119 goals and plans were scored based on planning objectives. Plans were compared using dose coverage, the conformity index and the homogeneity index. Point doses were measured at points recommended by TG-119 using a CC13 ion chamber. Planar dosimetry was accomplished using Imatrix and gamma evaluation was conducted using Omnipro IMRT software.
Results:
Dose distributions of FFF beam based plans were comparable to FF plans for both IMRT and VMAT. Our planning results matched TG-119 planning results. Measured point doses were within ±2% of planned doses and planar dosimetry gamma values were <1 for >95% of data points for all plans.
Conclusion:
We found a reduction of 40% treatment time for FFF against FF beams for sliding window IMRT. Upgraded FFF beams were in good agreement with TG-119 benchmark plans and goals.
Keywords: FF, FFF, VMAT, TG-119, patient specific QA
Introduction
Volumetric-modulated arc therapy (VMAT) has shown a promising delivery method resulting in plan quality of equal or better than that of IMRT for several sites. It has gained widespread adoption in the recent years by treating various sites, including prostate, spine, head and neck. The dynamic features of VMAT and corresponding optimization constraints are significantly different from the dynamic MLC delivery technique in IMRT (Eugenio et al., 2009; Wiehle et al., 2011; Subramanian et al., 2012).
VMAT uses dynamic MLCs, variable dose rate and gantry speed to generate quality dose distributions in a single optimized arc around the patient. VMAT can now continuously modulate the dose to the entire tumor volume while sparing of normal and healthy tissue. VMAT dose optimization employs an aperture-based method that incorporates MLC leaf positions and Monitor Unit (MU) weights as optimization parameters (Otto, 2008).
The Flattening Filter Free beam (FFF) has been introduced to increase dose rate and reduce leaf transmission, head scatter, and leakage radiation. The treatment time can be reduced significantly for stereotactic body radiation therapy (SBRT) delivery. A sharper penumbra can also be generated from FFF beams. There is a noticeable dose reduction outside the field in FFF beams compared to Flattening Filtered (FF) beams, which can improve the target conformity and sharper dose fall-off to limit radiation dose to distant organs (Thirumalai et al., 2015; Hansen et al., 1972).
Our Varian Clinac 2100CD linear accelerator was upgraded with 6MV FFF beam which had only conventional 6MV FF and 15MV FF beam before. This upgrade was first of its kind in our country. This 6 MV FFF beam has a maximum dose rate of 1400MU/min (140, 280, 420, 560, 700, 840, 980, 1120, 1260, 1400 MU/min) with the multiples of 140. Even though the dosimetric characteristics of FFF beam have been reported both in experimental and Monte Carlo studies, the applications of FFF beam in the planning and delivery is complicated and it requires validation in preclinical situation.
In year 2009 AAPM (American Association of Physicists in Medicine) Task Group 119 (TG119) has developed a set of test cases to assess the overall accuracy of planning and delivery of IMRT treatments to produce quantitative confidence limits as baseline expectation values for IMRT commissioning (Ezzell et al., 2009). Dinesh Kumar et al., (2012) used TG 119 as a metric to determine the capability of VMAT plan delivery with 6MV FF beam.
Aim of this study is to validate the commissioning of upgraded 6MV FFF beam dosimetrically using AAPM TG-119 benchmark plans for VMAT and to compare with IMRT plans for both FF and FFF beams.
Materials and Methods
Computed tomography (CT) datasets of the test cases were downloaded directly from the AAPM website (www.aapm.org) and imported into our treatment planning system. Figure 1 shows the test structures of these CT’s superimposed upon a set of water-equivalent slab phantom. TG 119 problem set consists of four structure sets namely test prostate, head-and-neck (H and N), C-shaped and Multi Target. Prostate structure set consists of prostate GTV, prostate PTV, rectum and bladder. One-third of rectum is overlapped with prostate PTV. In test head and neck case with PTV, we have OARs left (LT) and right (RT) parotids and spinal cord. There is 1.5cm gap between spinal cord and PTV. The C-shape structure set consists of C-shape PTV with 1.5cm inner and 3.7cm outer radius. OAR core is a cylindrical structure of 1cm radius and with a gap of 0.5 cm between C-shape PTV and core. Multi-target structure set has three cylindrical structures of 4cm diameter and 4cm length stacked along the coronal axis. Full description of all the structure sets is available, with dimensions, and goals in AAPM TG 119 report. AAPM TG 119 defines the beam arrangement, IMRT goals, and methods for analyzing the dosimetric results.
Figure 1.
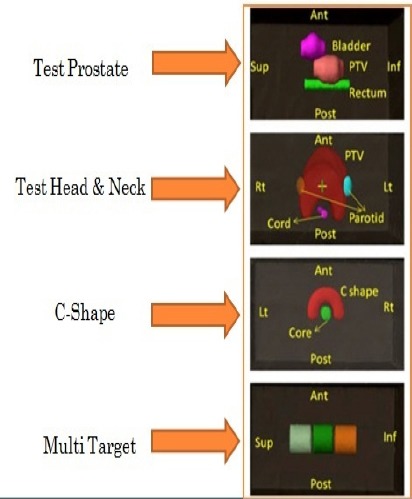
AAPM TG-119 Test Structure Set
For these test cases, we generated four treatment plans (namely IMRT FF, IMRT FFF, VMAT FF and VMAT FFF) on Varian Clinac 2100CD machine equipped with millennium 120 MLC (Varian Medical Systems, Palo Alto, CA) in Eclipse treatment planning system version 11.0. The IMRT plan was done using static 7-9 dynamic Multi-Leaf Collimator (dMLC) and a VMAT plan utilizing one- or two-arc. For prostate and Multi Target cases, seven static gantry angles 50° apart (0°, 50°, 100°, 150°, 310°, 260° and 210°) and one full arc (175° to 185°) were chosen for IMRT and VMAT plans respectively. For head-and-neck and C-shaped tests, nine static gantry angles 40° apart (0°, 40°, 80°, 120°, 160°, 320°, 280°, 240° and 200°) for IMRT and two complimentary full arcs were used for VMAT. For all VMAT plans we maintained the collimator angle at ± 10° while for IMRT plans 0° collimator angle was applied throughout.
All IMRT plan optimizations were done with dose volume optimization (DVO) algorithm and for VMAT plan optimizations were done using progressive resolution optimizer (PRO-III) algorithm. Dose calculations for all plans were performed using analytical anisotropic algorithm (AAA) with a dose calculation grid size of 2.5 mm and heterogeneity corrections were applied. All plans were normalized to an isodose line that ensured coverage of the volume to meet TG 119 requirements. Dose prescription and planning objectives were set according to the TG-119 goals and planning objectives as shown in Table 1. Treatment plans were compared using dose coverage, conformity index (CI) for reference dose (D95), homogeneity index (HID5–D95) and treatment time.
Table 1.
AAPM TG 119 Goals and Results with Standard Deviation (SD) for Test Cases
| Test Case | Planning Parameter | Plan goal (cGy) | Mean (cGy) | Standard Deviation (cGy) | Coefficient of variation |
|---|---|---|---|---|---|
| Prostate | Prostate D95 | > 7,560 | 7,566 | 21 | 0.003 |
| Prostate D5 | < 8,300 | 8,143 | 156 | 0.019 | |
| Rectum D30 | < 7,000 | 6,536 | 297 | 0.045 | |
| Rectum D10 | < 7,500 | 7,303 | 150 | 0.02 | |
| Bladder D30 | < 7,000 | 4,394 | 878 | 0.2 | |
| Bladder D10 | < 7,500 | 6,269 | 815 | 0.13 | |
| Head and Neck | PTV D90 | 5,000 | 5,028 | 58 | 0.013 |
| PTV D99 | > 4,650 | 4,704 | 52 | 0.011 | |
| PTV D20 | < 5,500 | 5,299 | 93 | 0.018 | |
| Cord maximum | < 4,000 | 3,741 | 250 | 0.067 | |
| Parotid | < 2,000 | 1,798 | 184 | 0.102 | |
| C-shape | PTV D95 | < 5,000 | 5,011 | 16.5 | 0.003 |
| PTV D10 | < 5,500 | 5,702 | 220 | 0.039 | |
| Core | 1,000 | 1,630 | 307 | 0.188 | |
| Multi Target | Central target D99 | > 5,000 | 4,955 | 162 | 0.033 |
| Central target D10 | < 5,300 | 5,455 | 173 | 0.032 | |
| Superior target D99 | > 2,500 | 2,516 | 85 | 0.034 | |
| Superior target D10 | < 3,500 | 3,412 | 304 | 0.089 | |
| Inferior target D99 | > 1,250 | 1,407 | 185 | 0.132 | |
| Inferior target D10 | < 2,500 | 2,418 | 272 | 0.112 |
For all the IMRT and VMAT plans verification plans were created to measure point dose and planar dose. These measurements were done in a plane recommended by TG-119. Point doses were measured using ion chamber CC13. Planar Dosimetry was done using I matrix with Multicube phantom (iba dosimetry, Germany) and gamma evaluation was done using Omnipro IMRT software (Xin et al., 2012).
This study has been bifurcated for convenience. The first section compares the plan parameters achieved with TG-119 results and in the second section TG-119 point dose and planar dose, measurement results were compared.
Results
A. Plan comparison
Figure 2(a) shows the prostate plan results where PTV D95 and D5 of IMRT and VMAT plans with both 6FF and FFF are comparable to TG 119 plans, where the dose prescription is 75.6 Gy to D95. All criteria were achieved or exceed the requirements of TG 119. Figure 3 shows prostate case IMRT and VMAT plan DVHs for PTV, rectum and bladder. For prostate case IMRT and VMAT plans have comparable DVH.
Figure 2.
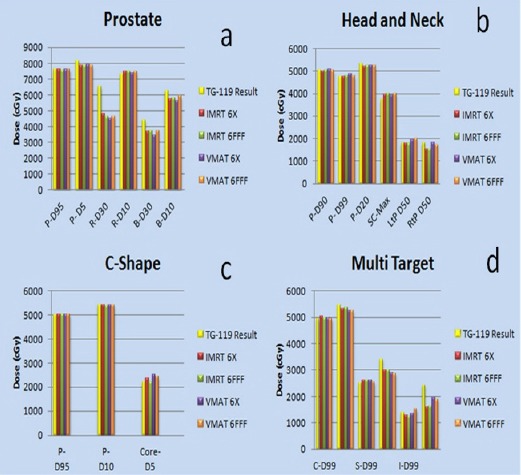
Results Achieved for AAPM TG-119 Test Clinical Cases
Figure 3.

Prostate Plan Comparison DVH
Figure 4 shows Head and Neck case IMRT and VMAT DVHs for PTV, cord, right and left parotids. The maximum cord doses for IMRT and VMAT for 6FF plans were 39.49 Gy and 39.30 Gy and for 6FFF were 39.89 Gy and 39.90 Gy respectively, but they are greater than the given constraint (< 38.50 Gy). However, AAPM TG 119 cord maximum standard deviation is 2.50 Gy and our results are within one standard deviation. The dose constraint for parotid is D50 less than 20 Gy, IMRT plans with both 6 FF and FFF achieved less dose to both the parotids compared to the VMAT plans as shown in Figure 2(b).
Figure 4.

Head and Neck Plan Comparison DVH
Figure 2(c) shows C-shaped plan results for IMRT and VMAT plans for both 6FF and 6FFF. The target and core dose goals are achieved. PTV plan prescription is 50 Gy to outer target, both IMRT and VMAT plans achieved PTV D10 very close to the planning goal of 55 Gy. All the plans achieved D5 constraint of OAR core, and results are comparable to TG 119 plan results. Figure 5 shows the C-shaped plan DVHs of IMRT and VMAT plans for 6FF and 6FFF beams the results shows core and target DVHs are comparable.
Figure 5.

C-Shape Plan Comparison DVH
Figure 2(d) shows for Multi Target plan results for IMRT and VMAT plans with 6FF and 6FFF achieved the planning goals. When compared to the benchmark TG 119 results, our IMRT and VMAT plans have more homogenous coverage to superior and inferior targets and similar results for the center target. Figure 6 shows IMRT and VMAT dose volume histograms of superior, inferior, and center target are comparable.
Figure 6.

Multi Target Plan Comparison DVH
Figure 7 shows frontal plane VMAT dose distribution comparison between 6FF and 6FFF for Test prostate, head and neck, C-shape and Multi Target. All the plans dose coverage is comparable to each other. The conformity index ranged 1.006 to 1.182 and the homogeneity index ranged from 1.03 to 1.078.
Figure 7.

IMRT and VMAT Dose Distribution Comparison for Test Prostate, Head and Neck, C-Shape and Multi Target
Discussion
B. TG-119 measurements
B.1. Point measurement results
Table 2 shows the point dose results in high dose and low gradient region (PTV region) and low dose and high gradient region (organ at risk region). The dose deviations were within ±2 % of planned values in PTV region and within ±5% in organ at risk region, but in case of prostate when the point dose were measured at rectum region the percentage of deviation is up to 5.39% but the absolute dose deviation is 0.6 Gy only.
Table 2.
Point Dosimetry Results in High and Low Dose Regions
| High Dose Region Point Dose (Gy) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IMRT 6FF | IMRT 6FFF | VMAT 6FF | VMAT 6FFF | |||||||||
| Case | Measured | Planned | Deviation | Measured | Planned | Deviation | Measured | Planned | Deviation (%) | Measured | Planned | Deviation (%) |
| (%) | (%) | |||||||||||
| Test Prostate | 2.3 | 2.33 | -1.29 | 2.34 | 2.31 | 1.3 | 2.28 | 2.31 | -1.3 | 2.33 | 2.3 | 1.3 |
| Test H&N | 1.95 | 1.98 | -1.52 | 2.45 | 2.41 | 1.66 | 2 | 2.03 | -1.48 | 2.38 | 2.36 | 0.85 |
| C-Shape | 0.41 | 0.43 | -4.65 | 0.428 | 0.427 | 0.23 | 0.453 | 0.454 | -0.22 | 0.374 | 0.367 | 1.91 |
| Multi Target | 1.97 | 2.01 | -1.99 | 1.98 | 2.02 | -1.98 | 2.03 | 2 | 1.5 | 2.03 | 2 | 1.5 |
| Low Dose Region Point Dose (Gy) | ||||||||||||
| IMRT 6FF | IMRT 6FFF | VMAT 6FF | VMAT 6FFF | |||||||||
| Case | Measured | Planned | Deviation | Measured | Planned | Deviation | Measured | Planned | Deviation (%) | Measured | Planned | Deviation (%) |
| (%) | (%) | |||||||||||
| Test Prostate | 1.02 | 1.08 | -5.56 | 2.34 | 2.31 | 1.3 | 0.83 | 0.85 | -2.35 | 0.97 | 0.99 | -2.02 |
| Test H&N | 1.38 | 1.39 | -0.72 | 2.47 | 2.41 | 2.49 | 1.59 | 1.56 | 1.92 | 1.67 | 1.64 | 1.83 |
| C-Shape | 2.08 | 2.12 | -1.89 | 0.428 | 0.427 | 0.23 | 1.99 | 2 | -0.5 | 2.04 | 1.99 | 2.51 |
B.2 Planar dose Measurements
Planar dose measurements were measured in a plane recommended by TG-119. The gamma analysis work space of C-shape target is shown in the Figure 8. In high dose and low gradient region, the passing criteria is 3% dose difference (DD) and 3mm distance to agreement (DTA) is accepted and in low dose and high gradient region the criteria is 5% DD and 5mm DTA were accepted (Palta et al., 2008) and the gamma analysis results are tabulated in table 3. All gamma evaluation results show gamma less than one for more than 97% data points with the given criteria.
Figure 8.

Planned Axial Dose Distribution (a) at central core level (i.e., low-dose region) of 6X FFF C-shape plan using VMAT technique; (b) Measured in detractor array at the same level; (c) the corresponding X and Y profiles for planned and delivered doses. (d) Gamma analysis results with 3%/3 mm criteria (98.63% of pixels passed)
Figure 9.
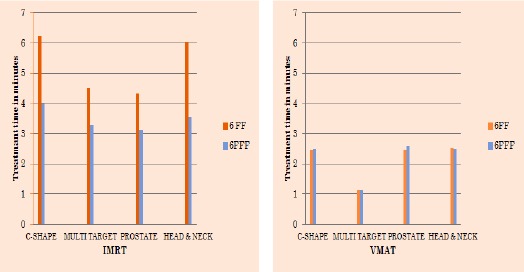
Treatment Time Comparison for TG-119 Test Clinical Cases
Table 3.
Gamma Analysis Results of Planar Dosimetry in High Dose and Low Dose Regions
| Gamma criteria | Test | IMRT | VMAT | ||
|---|---|---|---|---|---|
| FF | FFF | FF | FFF | ||
| 3% DD and 3mm DTA (High dose region) | Multi target | 98.37 | 97.6 | 97.65 | 97.57 |
| C-Shape | 98.48 | 97.98 | 95.15 | 98.06 | |
| Head and Neck | 98.72 | 98.24 | 97.78 | 97.09 | |
| Prostate | 97.45 | 96.84 | 98.17 | 99.19 | |
| 5% DD and 5mm DTA (Low dose region) | C-Shape | 98.04 | 96.8 | 96.02 | 98.63 |
| Head and Neck | 96.78 | 97.64 | 97.84 | 97.39 | |
| Prostate | 98.55 | 97.59 | 98.88 | 98.75 | |
B.3 Treatment Time comparison
The beam ‘ON’ time comparison for 6 MV FF and FFF were done for TG-119 test clinical cases. The beam ‘ON’ time was defined as the time elapsed between the beam ‘ON’ of the first Arc/Field and the beam ‘OFF’ of the last Arc/Field of the treatment. Study found that Sliding window IMRT with FFF beam shows significant reduction in treatment time as compare to conventional FF beam the as shown in figure 10. However, in case of VMAT, the reduction in treatment time was not significant as the dose per fraction is low and the gantry speed cannot be increased beyond 4.8º/sec.
In conclusion, upgraded FFF beams were in good agreement with TG-119 Bench mark plans and goals. It is helpful to gain confidence in new modalities like FFF based VMAT and to test its capabilities at preclinical implementation stage. Interestingly the study reveals that the sliding window IMRT with 6 MV FFF beam shows 40% reduction in the treatment time as compared to FF beam. We require multi-institutional and multiple-vendor study for true benchmarking of VMAT programs, as done in TG 119.
Statement conflict of Interest
Authors have no conflict of Interest.
References
- Dinesh Kumar M, Ravindra Y, Linda H, Hsiang-Chi K, Dennis M. Application of AAPM TG 119 to volumetric arc therapy (VMAT) J Appl Clin Med Phys. 2012;13:108–16. doi: 10.1120/jacmp.v13i5.3382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eugenio V, Alessandro C, Giorgia N, et al. Volumetric modulated arc radiotherapy for carcinomas of the oro-pharynx, hypo-pharynx and larynx: A treatment planning comparison with fixed field IMRT. Radiother Oncol. 2009;92:111–17. doi: 10.1016/j.radonc.2008.12.008. [DOI] [PubMed] [Google Scholar]
- Ezzell GA, Burmeister JW, Dogan N, et al. IMRT commissioning: multiple institution planning and dosimetry comparisons, a report from AAPM Task Group 119. Med Phys. 2009;36:5359–73. doi: 10.1118/1.3238104. [DOI] [PubMed] [Google Scholar]
- Hansen HH, Connor WG, Doppke K, Boone MML. A new field flattening filter for the clinac-4. Radiology. 1972;103:443–6. doi: 10.1148/103.2.443. [DOI] [PubMed] [Google Scholar]
- Jatinder R, Palta Liu C, Li JG. Quality assurance of intensity-modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2008;71:108–12. doi: 10.1016/j.ijrobp.2007.05.092. [DOI] [PubMed] [Google Scholar]
- Otto K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med Phys. 2008;35:310–7. doi: 10.1118/1.2818738. [DOI] [PubMed] [Google Scholar]
- Subramanian S, Srinivas C, Ramalingam K, et al. Volumetric modulated arc-based hypofractionated stereotactic radiotherapy for the treatment of selected intracranial arteriovenous malformations, Dosimetric report and early clinical experience. Int J Radiat Oncol Bio Phys. 2012;82:1278–84. doi: 10.1016/j.ijrobp.2011.02.005. [DOI] [PubMed] [Google Scholar]
- Shanmugam TS, Chandrasekaran AR, Gandhi A, Murugesan K, Sai S. Planning and dosimetric study of volumetric modulated arc based hypofractionated stereotactic radiotherapy for acoustic schwannoma - 6MV flattening filter free photon beam. Asian Pac J Cancer Prev. 2015;16:5019–23. doi: 10.7314/apjcp.2015.16.12.5019. [DOI] [PubMed] [Google Scholar]
- Wiehle R, Knippen S, Grosu AL, Bruggmoser G, Hodapp N. VMAT and step-and-shoot IMRT in head and neck cancer: a comparative plan analysis. Strahlenther Onkol. 2011;187:820–5. doi: 10.1007/s00066-011-2267-x. [DOI] [PubMed] [Google Scholar]
- Xin Y, Wang JY, Li L, et al. Dosimetric verification for primary focal hyper metabolism of nasopharyngeal carcinoma patients treated with dynamic intensity-modulated radiation therapy. Asian Pac J Cancer Prev. 2012;13:985–9. doi: 10.7314/apjcp.2012.13.3.985. [DOI] [PubMed] [Google Scholar]