

Abstract
This study was aimed at assessing any association between smoking and health-related quality of life (HRQoL) among adults aged 18 years and above living in Kermanshah city, western Iran. A cross-sectional study was conducted on a total sample of 1,543 participants obtained by convenient sampling during the period from February 1st to May 30th, 2017. Data were collected using a self-administrated questionnaire. The HRQoL of the study participants was assessed with reference to the EuroQol 5-dimensions-3-level (EQ-5D-3L). The impact of smoking behavior of the participants on HRQoL with controls for potential confounders was examined by multiple regression. Out of the total of 1,543 participants, current smokers, past smokers, and never smokers accounted for 19.7%, 4.2% and 76.1%, respectively. The mean EQ-5D indices were 0.69 ±SD 0.20, 0.70 ± SD 0.22, and 0.78 ± SD 0.16. The highest proportion of self-reported problems (including both ‘some’ and ‘severe’) were related to current, heavy smokers, with high nicotine dependence. Regression analysis indicated that current smokers had a significantly lower HRQoL compared to past smokers and never smokers (p < 0.05). The heavy smokers also had a significantly lower HRQoL score than moderate and light smokers (p < 0.05) and there was an inverse relationship between the HRQoL score and nicotine dependence (p<0.05). The current smokers, heavy smokers, and high nicotine dependent smokers had lower HRQoL scores. These findings provide inputs for better understanding and for devising interventions for smoking cessation, reducing the number of cigarettes smoked per day and nicotine dependency.
Keywords: Health-related quality of life, smoking, adult, EQ-5D, Iran
Introduction
Cigarette smoking is one of the major public health concerns globally. Each year, more than five million adults die from condition related to smoking. The annual death rate is expected to rise to about 8 million people by the year 2030. More than 80 % of these deaths will be in low- and middle-income countries (Max et al., 2004). Despite interventions to decrease smoking, the prevalence of smoking in Iran remained very high. The prevalence of male and female smokers were estimated at 23.4% and 1.4% respectively (Meysamie et al., 2010). Evidence from Iran and elsewhere indicated a negative impact of smoking including death, length of hospital stay (LHS) and costs of hospitalization (Rezaei et al., 2015; Rezaei et al., 2016a; Rezaei et al., 2016b; Akbari Sari et al., 2016).
The adverse effects of smoking on the health of individuals are commonly understood. While the impact of smoking on health-related quality of life (HRQoL) in the developed countries are well document, the association between smoking behavior and HRQoL of individuals in the developing world is rarely reported (Coste et al., 2014; Strine et al., 2005; Vogl et al., 2012). An inverse association between HRQoL and the number of cigarettes smoked has been reported. However, there is no such an evidence from Iran in general and the western region of Iran in particular. The HRQoL, as a physical well-being of a person, is an important concept in health systems research (HSR) to inform decisions for improving the prevention and treatment of disorders (Stewart et al., 1995).
Determining the relationship between HRQoL and a particular lifestyle such as cigarette smoking needs inputs from economic evaluation studies for better informed decisions concerning the allocation of the limited resources in health systems. The knowledge on the lost utility due to smoking can also help design cost-effectiveness studies about smoking reduction and smoking cessation interventions among populations. Thus, the knowledge on the utility is an important input for the economic evaluation studies such as cost-utility analysis (Jia and Lubetkin, 2010; Stewart et al., 1995; Vogl et al., 2012; Tillmann and Silcock, 1997). Despite well-established risk of poor health, to the best of our knowledge, there is no evidence showing the association between smoking and HRQoL among the general population in Iran. This study aims to identify the association between smoking and HRQoL and to examine the impact of smoking on health-related quality of life using the EQ-5D among 18 year old and above individuals living in Kermanshah city, western Iran.
Materials and Methods
Study population and sampling method
A cross-sectional study was carried out from February one to May 30, 2017 to examine the association between smoking and HRQoL among 18 year old and above individuals living in Kermanshah city, western Iran. A convenience sampling technique was used to select the study participants.
Data collection tools
The data was collected using a self-administrated questionnaire consisting of three parts. The first part was related to socio-demographic characteristics, socio-economic status, and life style of the study participants. The second part was related to the smoking behavior (smoking status, smoking intensity and nicotine dependence) of the respondents. The Fagerstrom test with 6 questions was used to identify the level of nicotine dependence of the participants (Heatherton et al., 1991). The third part was administered the validated Iranian version of the EuroQol 5-dimensions-3-level (EQ-5D-3L) questionnaire that consisted of five dimensions (mobility, self-care, usual activity, pain/discomfort, and anxiety/depression) with three response levels (no problem, some problem and extreme problem) for each dimension (Rabin and Charro, 2001). We used the Iranian value set for the EQ-5D-3L health states, which was calculated by the visual analog score to compute the HRQoL of the study participants. This method was suggested for use in a recent study conducted by Goudarzi et al. (Goudarzi et al., 2016).
Statistical analysis
Based on their smoking status, we classified the participants into current smokers (those who smoke at least one piece of cigarette per day), never smokers (those who have never had smoked or smoked less than 100 pieces of cigarettes in their lifetime), and past smokers (those who have had smoked regularly or occasionally in the past). Again, based on the frequency of cigarette smoking per day, the current smokers were further classified into light smokers (those who smoke less than 10 pieces of cigarettes per day), moderate smokers (those who smoke between 10 and 19 pieces of cigarettes per day), and heavy smokers (those who smoke 20 or more pieces of cigarette per day). The nicotine dependence of the smokers was also classified as low dependence (score 1-2), medium dependence (score 3-7), and high dependence (score 8+). The never smokers and past smokers were considered as having no nicotine dependence. To explore the association between smoking and HRQoL, we applied a series of multiple linear regression models. First, we included all the study participants in the model and investigated the association between smoking status (considering never smokers as the baseline group) and HRQoL. Second, we modeled the relationship between the number of cigarettes smoked per day (heavy smokers were the reference group) and HRQoL among the current smokers only. Third, we included all the study participants in the model and analyzed using the nicotine dependence (no dependence) as the predicator of the HRQoL. The analyses were run in separate models because of a high collinearity. All the models were adjusted for age, gender, marital status, educational level, body-mass index (BMI), physical activity, health insurance coverage, having chronic diseases and monthly household income per capita. The analyses were done using Stata version 14.2 and the p-value less than 0.05 was considered statistically significant.
Ethical statement
The study protocol was reviewed and approved by the Ethics Committee of the Deputy of Research, Kermanshah University of Medical Sciences (KUMS). Furthermore, each eligible study participant was involved in the study in accordance to the ethical code of conduct recommendation of the World Medical Association Declaration of Helsinki. The verbal consent was obtained from each study participant after explaining the details about the study. The data was collected and analysis anonymously.
Results
A total of 1534 adults whose age was 18 year and above participated in the study. The mean age of the participants was 35.9 years with standard deviation (SD) of 13.4 years. Eight-hundred-seventy-three (56.9%) of the participants were males and the rest was females. Furthermore, those participants in the low-income (monthly household income per capita less than 10 million Iranian Rials), physically active, and normal body weight categories accounted for 54.8%, 57.4%, and 55.2% respectively (Table 1). Those participants in the overweight or obese category accounted for 44.8%. Based on the smoking status of the participants, those current smokers, past smokers and never smokers accounted for 19.7%, 4.2% and 76.1%, respectively. Beside, those with chronic diseases, who had health insurance, and illiterate respectively accounted for 11.9%, 84.8% and 5.7%.
Table 1.
Socio-Demographic Characteristics, Socioeconomic Status and Life Style Factors of The Study Participants in Kermanshah, Western Iran, 2017
| Variables | Frequency | Percent |
|---|---|---|
| Age group | ||
| 18-44 years | 1,066 | 69.5 |
| ≥45 years | 468 | 30.5 |
| Sex | ||
| Male | 873 | 56.9 |
| Female | 661 | 43.1 |
| Marital status | ||
| Never married | 70 | 4.6 |
| Married | 835 | 54.4 |
| Divorced and widowed | 629 | 41 |
| Monthly household income per capita (Iranian Rialsa) | ||
| Low (<10 million) | 840 | 54.8 |
| Middle (10 - 20 million) | 606 | 39.5 |
| High (>2 million) | 88 | 5.7 |
| Educational level | ||
| Illiterate | 88 | 5.7 |
| Primary and secondary | 641 | 41.8 |
| Post-secondary | 805 | 52.5 |
| Health insurance | ||
| Yes | 1,301 | 84.8 |
| No | 233 | 15.2 |
| Smoking behavior | ||
| Current smoker | 303 | 19.7 |
| Past smoker | 64 | 4.2 |
| Never smoker | 1167 | 76.1 |
| Smoking intensity | ||
| Light smoker | 83 | 27.4 |
| Moderate smoker | 146 | 48.2 |
| Heavy smoker | 74 | 24.4 |
| Nicotine dependence | ||
| No dependence (non-smoker) | 1,231 | 80.2 |
| Low dependence | 160 | 10.4 |
| Middle dependence | 100 | 6.5 |
| High dependence | 43 | 2.8 |
| Physical activity | ||
| Active | 878 | 57.4 |
| Moderately active | 443 | 28.9 |
| Inactive | 210 | 13.7 |
| Body mass index (BMI) | ||
| Normal | 846 | 55.2 |
| Overweight /obese | 688 | 44.8 |
| Chronic diseases | ||
| Yes | 182 | 11.9 |
| No | 1,352 | 88.1 |
a, One US Dollar, 35,000 Iranian Rials (IR) in 2017.
The descriptive statistics based on the five dimensions of the EQ-5D for the different smoking behaviors of the participants are presented in Table 2 and Figure 1. Among the current smokers, anxiety/depression (51.6%), pain/discomfort (51.6%), usual-activities (28.7%), mobility problems (19.5%) and problems of self-care (17.2%) were the highest proportions of the reported problems (both ‘some’ and ‘severe’) across the five dimensions of the EQ-5D. Compared to the never smokers, those who reported having the problems were higher in proportion than those of the current and past smokers. Based on the intensity of smoking, anxiety/depression (40.5%), pain/discomfort (39.2%), usual-activities (37.8%), problems of self-care (39.2%) and mobility problems (33.8%) were the highest percentages reported among the heavy smokers. The proportions of those who reported ‘some’ or ‘severe’ problems across the five dimensions were higher for the light smokers than that of the heavy and moderate smokers. However, in none of the participants were ‘severe’ mobility, problem of self-care and usual activities problems reported (see Table 2).
Table 2.
Responses of Participants to the Five Dimensions of the EQ-5D by Smoking Behavior of the Study Participants in Kermanshah, Western Iran, 2017
| EQ-5D dimensions | Level (problem) | Smoking status | Smoking intensity | Nicotine dependence | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Never | Past | Current | Light | Moderate | Heavy | No | low | Middle | High | ||
| No | 89.2 | 93.7 | 80.5 | 86.8 | 84.3 | 66.2 | 89.4 | 88.8 | 79 | 53.5 | |
| Mobility | Some | 10.8 | 6.3 | 19.5 | 13.2 | 15.7 | 33.8 | 10.6 | 11.2 | 21 | 46.5 |
| Severe | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| No | 96.2 | 89 | 82.8 | 91.8 | 86.7 | 60.8 | 95.9 | 90.6 | 86 | 46.5 | |
| Self-care | Some | 3.8 | 11 | 17.2 | 8.2 | 13.3 | 39.2 | 4.1 | 9.4 | 14 | 53.5 |
| Severe | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| No | 88.3 | 71.9 | 71.3 | 79.5 | 71.2 | 62.2 | 87.5 | 81.2 | 68 | 41.9 | |
| Usual activities | Some | 11.7 | 28.1 | 28.7 | 20.5 | 28.8 | 37.8 | 12.5 | 18.8 | 32 | 58.1 |
| Severe | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| No | 71.9 | 64.4 | 48.4 | 67.1 | 62.7 | 60.8 | 70.1 | 70.2 | 63 | 48 | |
| Pain/discomfort | Some | 27.4 | 34.6 | 50 | 31.5 | 36.1 | 39.2 | 28.7 | 28.8 | 37 | 51 |
| Severe | 0.7 | 1 | 1.6 | 1.4 | 1.2 | 0 | 0 | 0 | 0 | 0 | |
| No | 69.2 | 61.1 | 48.4 | 63.7 | 57.8 | 59.5 | 68.1 | 65 | 61 | 46.5 | |
| Anxiety/depression | Some | 29.7 | 36.3 | 45.3 | 33.6 | 39.8 | 37.8 | 30.5 | 31.9 | 37 | 51.2 |
| Severe | 1.1 | 2.7 | 6.3 | 2.7 | 2.4 | 2.7 | 1.4 | 3.1 | 2 | 2.3 | |
All numbers are in percentage.
Figure 1.
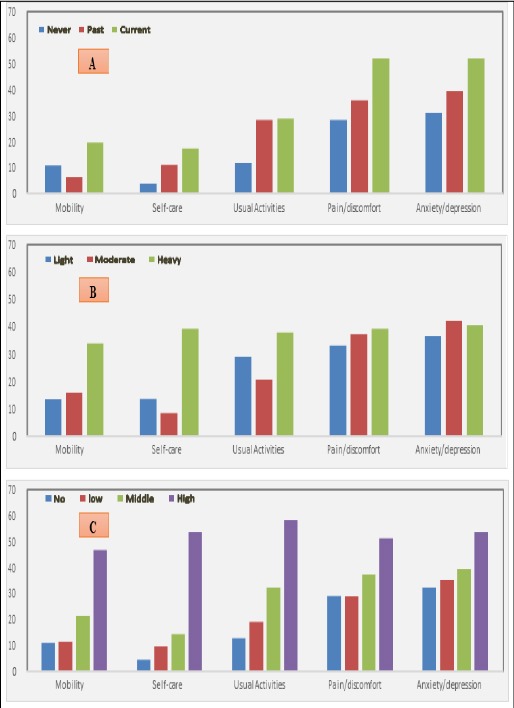
Percentage Distribution of Reported Problems (‘some’ or ‘severe’) among Adult Population by Smoking Status: (A) smoking intensity, (B) nicotine dependence and (C) the study participants in Kermanshah, western Iran, 2017
The means of the EQ-5D index for the different smoking behavior and the multiple linear regression results are shown in Table 3. The overall mean of the EQ-5D was 0.76 ±SD 0.18. The mean EQ-5D index for the current, past smokers, and never smokers were 0.69 ± 0.20, 0.70 ± 0.22 and 0.78 ± 0.16, respectively. The multiple regression analysis indicated that the current smokers had significantly lower HRQoL compared to the past and never smokers. Again, the past smokers had better HRQoL compared to the current smokers. Among the current smokers, the heavy smokers (those who smoke 20 and over pieces of cigarettes per day) had significantly lower HRQoL scores than those of the moderate smokers (those who smoke 11-20 pieces of cigarettes per day) and the light smokers (those who smoke 0-10 pieces of cigarettes per day). The HRQoL score for light smokers was significantly higher when compared to the HRQoL score of the moderate smokers. However, the regression analysis revealed an inverse relationship between the HRQoL scores and the nicotine dependence of the smokers. The smokers with high nicotine dependence had lower HRQoL score compared to those with medium, low and no nicotine dependence.
Table 3.
Multiple Linear Regression of the Association between Different Smoking Behavior and EQ-5D Index Study Participants in Kermanshah, Western Iran, 2017
| Mean EQ-5D index±SD | EQ-5D index | |||
|---|---|---|---|---|
| Coefficient | P-value | 95 %confidence interval | ||
| Smoking statusa | ||||
| Never smoker | 0.78 ±0.16 | Reference | - | - |
| Past smoker | 0.70 ±0.22 | -0.057 | 0 | -0.079 to -0.035 |
| Current smoker | 0.69 ±0.20 | -0.065 | 0.001 | -0.105 to -0.025 |
| Smoking intensityb | ||||
| Heavy smoker | 0.62 ±0.28 | Reference | - | - |
| Moderate smoker | 0.72 ±0.20 | 0.067 | 0.031 | 0.006 to 0.127 |
| Slight smoker | 0.73 ±0.20 | 0.074 | 0.005 | 0.022 to 0.127 |
| Nicotine dependencec | ||||
| No dependence | 0.77 ±0.16 | Reference | - | - |
| Low | 0.75 ±0.19 | -0.027 | 0.05 | -0.053 to 0.0004 |
| Middle | 0.70 ±0.22 | -0.047 | 0.006 | -0.079 to -0.014 |
| High | 0.52 ±0.26 | -0.17 | 0 | -0.221 to -0.121 |
Adjusted for age, gender, physical activity, marital status, chronic diseases, income, health insurance, educational level, BMI. a, Adj R-squared is 0.29; b, Adj R-squared is 0.39; c, Adj R-squared is 0.30.
Discussion
This study attempted to investigate the HRQoL of smokers and non-smokers and the relationship between smoking behavior (never, current and past smoker), smoking intensity (light, moderate and heavy smoker), nicotine dependence (no, low, medium and high dependence) and HRQoL of adult smokers among the people living in west Iran. The findings showed negative association between smoking behavior and HRQoL. Those never smokers had higher scores of HRQoL and reported lower problems in the EQ-5D dimensions. In contrast, the heavy smokers had lower HRQoL than the light and moderate smokers. The higher nicotine dependency of the smokers was correlated with a lower HRQoL scores.
Previous study in Iran reported that smokers had significantly lower quality of life in the physical, psychological, social and environmental dimensions of health (Khalilzad Behrozian and Ahmadi, 2013). Similarly, our findings indicated that anxiety/depression was more prevalent among the current smokers than the never and past smokers. Others also found that psychological problems such as depression were more prevalent among current smokers than former smokers and never smokers (Brown et al., 1996; Rathnayaka et al., 2014; Talati et al., 2016). Evidence from a systematic review and meta-analysis also indicated that smoking cessation improved mental health and quality of life of the quitters. Beside, smoking cessation was correlated with reduction in depression, stress and anxiety problems (Taylor et al., 2014). Despite the higher rate of smoking among people with mental illness, providing appropriate treatment for mentally ill smokers can increase their chance of smoking cessation (Lê Cook et al., 2014).
Our findings indicated an association between smoking and lower HRQoL among adult individuals living in Kermanshah province. An earlier study in the same province reported the absence of a significant effect of smoking on quality of life among patients with hemodialysis (Omrani et al., 2013). However, evidence showed that patients undergoing hemodialysis are more likely to have poor quality of life compare to the general population (Fukuhara et al., 2003; Pakpour et al., 2010). A study on HRQoL among water pipe smokers in south Iran found that smoking decreases the physical and mental dimensions of quality of life. Beside, smoking water pipe, being female, older age, and lower education level were associated with increased risk of poor HRQoL (Tavafian et al., 2009). Another study in Iraq also reported that water pipe smokers were in a poorer physical and mental quality of life than the non-smokers. The age, education status, cigarette smoking status, disease status and water pipe use were correlated with the physical and mental health scores among the water pipe smokers (Al-Easawi et al., 2014).
The mean score of the EQ-5D in our study (0.76) is consistent with the report of a similar study in Tehran (0.74). Pain/discomfort and anxiety/depression were the most prevalent problems reported and smoking was negatively associated with HRQoL (Kazemi Karyani et al., 2016). The most frequently reported problems “both some and extreme” among the Iranian population were pain/discomfort and anxiety/depression dimensions of the EQ-5D (Javanbakht et al., 2012). These EQ-5D dimensions exert most of the weights on the Iranian value-set (Goudarzi et al., 2016). Thus, paying attention to the HRQoL dimensions can lead to improved HRQoL. The mean values of the HRQoL reported from developed countries such as Sweden (Burström et al., 2001a), U.S. (Luo et al., 2005), Italy (Scalone et al., 2015) and Japan (Shiroiwa et al., 2015) were higher than that reported from Iran. Nevertheless, the problems of mobility, self-care, and usual activity were the least prevalent problems both in the developed and developing countries including Iran (Burström et al., 2001a; Kazemi Karyani et al., 2016; McCaffrey et al., 2016; Scalone et al., 2015).
Several studies reported that socio-demographic characteristics, socioeconomic status and health status [chronic diseases) of the study participants were among the main determinants of the HRQoL in different populations (Burström et al., 2001b; Kazemi Karyani et al., 2016; Luo et al., 2005). Our analysis adjusted for these determinants to identify the pure effect of smoking on HRQoL. By controlling for the socio-economic differences of the study participants, our analysis revealed that smoking and nicotine dependency significantly decreased the HRQoL. Evidence from a related study that adjusted the study participants for socioeconomic status also reported the negative effect of nicotine dependency on HRQoL and the smokers with nicotine dependence had a higher risk of developing mental disorders (Schmitz et al., 2003). Nonetheless, the difference in socio-demographic characteristics might be explained by the high rate of mental disorders and poor health status among the smokers than the non-smokers (Son et al., 1997), and the improvement in quality of life after smoking cessation could also be explained by the socio-economic status of the people (Tillmann and Silcock, 1997).
Generally, several studies highlighted that smokers have lower quality of life than non-smokers. Heavy smokers have lower level of HRQoL than the light smokers, ex-smokers and never smokers (Strine et al., 2005; Wilson et al., 1999). The smokers are more likely to drink alcohol and to report sleep disorders, symptoms of anxiety and depression than the non-smokers. Besides, smokers are more likely to be inactive, have pain and unhealthy diet than the non-smokers (Strine et al., 2005). A cohort study demonstrated that never-smokers had the highest scores on health status and they have longer life than the smokers. There was a big difference between never smokers and heavy smokers in their health status and longevity (Strandberg et al., 2008).
The consideration of smoking alone in the investigation of the effect of smoking on health may provide misleading results concerning the evaluation of tobacco and smoking cessation programs (Breslau et al., 2001; Schmitz et al., 2003). Our study included nicotine dependence to declare the association between HRQoL and nicotine dependence. A high nicotine dependence could resulted in low HRQoL, while decreasing the nicotine dependence can be consider successful in the smoking cessation programs. The EQ-5D value-set for the Iranian population was used to increase the validity of the study. The different categories of smoking status were considered to better understand about the association between smoking and HRQoL among the participants. Nevertheless, our study has several limitations. First, the fact that our study was based on convenience sampling, the interpretation of the findings should be with caution. Second, the cross-sectional design study could not let the authors to investigate causal relationship between smoking and HRQoL of the participants. Third, the study participants were included only from only one province in Iran, Kermanshah. Hence, the findings cannot be generalizable to other provinces in Iran. Fourth, this study measured the smoking behavior, smoking intensity and nicotine dependence of the participants. Therefore, there could be a possible of recall bias in measuring the items. Taking into account the differences in socio-demographic and smoking behaviors of the people living different in the different provinces of Iran, future studies can provide useful understanding about the HRQoL and smoking in the different provinces in Iran.
In conclusion, the findings indicated that current smokers had lower HRQoL than past and never smokers. The nicotine dependence was inversely associated with HRQoL of the study participants. Thus, smoking cessation programs should emphasize on individuals with high nicotine dependence and decreasing the nicotine dependence can be considered as a part of an effective smoking cessation intervention of the programs. Improving the HRQoL of smokers can encourage the development of public smoking cessation programs.
Conflict of Interest
The authors declare that they have no conflict of interest associated with the material presented in this paper.
Acknowledgements
This study was extracted from a project approved by the Kermanshah University of Medical Sciences. The study was funded and supported by the Research Deputy of Kermanshah University of Medical Sciences (Grant Number: 96404).
References
- Al-Easawi NA RF, Almashhadani SAKA, Alrekabi AANG. Health related quality of life variation among water pipe (Argihla) smokers in Baghdad, Iraq. J Al-Nahrain Uni Sci. 2016;17:128–36. [Google Scholar]
- Akbari Sari A, Rezaei S, Arab M, et al. Effects of smoking on cost of hospitalization and length of stay among patients with lung cancer in Iran: a hospital-based study. Asian Pac J Cancer Prev. 2016;17:4421–6. [PubMed] [Google Scholar]
- Brown RA, Lewinsohn PM, Seeley JR, Wagner EF. Cigarette smoking, major depression, and other psychiatric disorders among adolescents. J Am Acad Child Adolesc Psychiatry. 1996;35:1602–10. doi: 10.1097/00004583-199612000-00011. [DOI] [PubMed] [Google Scholar]
- Burstrom K, Johannesson M, Diderichsen F. Health-related quality of life by disease and socio-economic group in the general population in Sweden. Health Policy. 2001;55:51–69. doi: 10.1016/s0168-8510(00)00111-1. [DOI] [PubMed] [Google Scholar]
- Burstrom K, Johannesson M, Diderichsen F. Swedish population health-related quality of life results using the EQ-5D. Qual Life Res. 2001;10:621–35. doi: 10.1023/a:1013171831202. [DOI] [PubMed] [Google Scholar]
- Breslau N, Johnson EO, Hiripi E, Kessler R. Nicotine dependence in the United States: prevalence, trends, and smoking persistence. Arch Gen Psychiatry. 2001;58:810–6. doi: 10.1001/archpsyc.58.9.810. [DOI] [PubMed] [Google Scholar]
- Coste J, Quinquis L, D'Almeida S, Audureau E. Smoking and health-related quality of life in the general population Independent relationships and large differences according to patterns and quantity of smoking and to gender. PLoS One. 2014;9:e91562. doi: 10.1371/journal.pone.0091562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fukuhara S, Lopes AA, Bragg-Gresham JL, et al. Health-related quality of life among dialysis patients on three continents: the dialysis outcomes and practice patterns study. Kidney Int. 2003;64:1903–10. doi: 10.1046/j.1523-1755.2003.00289.x. [DOI] [PubMed] [Google Scholar]
- Goudarzi R, Zeraati H, Akbari Sari A, Rashidian A, Mohammad K. Population-based preference weights for the EQ-5D health states using the visual analogue scale (VAS) in Iran. Iran Red Crescent Med J. 2016;18:e21584. doi: 10.5812/ircmj.21584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heatherton TF, Kozlowski LT, Frecker RC, fagerstrom KO. The Fagerström test for nicotine dependence: a revision of the fagerstrom tolerance questionnaire. Addic. 1991;86:1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- Javanbakht M, Abolhasani F, Mashayekhi A, Baradaran HR, Jahangiri noudeh Y. Health related quality of life in patients with type 2 diabetes mellitus in Iran: a national survey. PLoS One. 2012;7:e44526. doi: 10.1371/journal.pone.0044526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jia H, Lubetkin EI. Trends in quality-adjusted life-years lost contributed by smoking and obesity. Am J Prev Med. 2012;38:138–44. doi: 10.1016/j.amepre.2009.09.043. [DOI] [PubMed] [Google Scholar]
- Kazemi Karyani A, Rashidian A, Sefiddashti SE, Akbari Sari A. Self-reported health-related quality of life (HRQoL) and factors affecting HRQoL among individuals with health insurance in Iran. Epidemiol Health. 2016;38:e2016046. doi: 10.4178/epih.e2016046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khalilzad Behrozian S, Ahmadi E. The assessment of self efficacy and the dimensions of quality of life on smokers and nonsmokers. Urmia Med J. 2013;24:257–62. [Google Scholar]
- LêCook B, Wayne GF, Kafali EN, et al. Trends in smoking among adults with mental illness and association between mental health treatment and smoking cessation. JAMA. 2014;311:172–82. doi: 10.1001/jama.2013.284985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo N, Johnson JA, Shaw JW, Feeny D, Coons SJ. Self-reported health status of the general adult U.S. population as assessed by the EQ-5D and Health Utilities Index. Med Care. 2005;43:1078–86. doi: 10.1097/01.mlr.0000182493.57090.c1. [DOI] [PubMed] [Google Scholar]
- Max W, Rice D, Sung H, Zhang X, Miller L. The economic burden of smoking in California. Tob Control. 2004;13:264–7. doi: 10.1136/tc.2003.006023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCaffrey N, Kaambwa B, Currow DC, Ratcliffe J. Health-related quality of life measured using the EQ-5D–5L: South Australian population norms. Health Qual Life Outcomes. 2016;14:133. doi: 10.1186/s12955-016-0537-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meysamie A, Ghaletaki R, Haghazali M, et al. Pattern of tobacco use among the Iranian adult population: results of the national survey of risk factors of non-communicable diseases (SuRFNCD-2007) Tob Control. 2010;19:125–8. doi: 10.1136/tc.2009.030759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Omrani HR, Raeisi D, Seyedzadeh A, et al. Quality of life and it's determinant in hemodialysis patients in Kermanshah in 2010. J Kermanshah Univ Med Sci. 2013;16:657–64. [Google Scholar]
- Pakpour AH, Saffari M, Yekaninejad MS, et al. Health-related quality of life in a sample of Iranian patients on hemodialysis. Iran J Kidney Dis. 2010;4:50–9. [PubMed] [Google Scholar]
- Rabin R, Charro Fd. EQ-SD: a measure of health status from the EuroQol Group. Ann Med. 2001;33:337–43. doi: 10.3109/07853890109002087. [DOI] [PubMed] [Google Scholar]
- Rathnayaka N, Ahmed S, Green C, Schmitz J, Vujanovik A. The association of impulsivity and distress tolerance with PTSD symptom severity: A test among trauma-exposed, cocaine-dependent adults. Drug Alcohol Depend. 2014;140:183–4. [Google Scholar]
- Rezaei S, Akbari Sari A, Arab M, Majdzadeh R, Mohammadpoorasl A. Estimating economic burden of cancer deaths attributable to smoking in Iran. J Res Health Sci. 2015;15:228–33. [PubMed] [Google Scholar]
- Rezaei S, Akbari Sari A, Arab M, et al. The association between smoking status and hospital length of stay: evidence from a hospital-based cohort. Hosp Pract. 2016;44:129–32. doi: 10.1080/21548331.2016.1178579. [DOI] [PubMed] [Google Scholar]
- Rezaei S, Akbari Sari A, Arab M, Majdzadeh R, Mohammad Poorasl A. Economic burden of smoking: a systematic review of direct and indirect costs. Med J Islam Repub Iran. 2016;30:397–405. [PMC free article] [PubMed] [Google Scholar]
- Scalone L, Cortesi PA, Ciampichini R, Cesana G, Mantovani LG. Health related quality of life norm data of the Italian general population: results using the EQ-5D-3L and EQ-5D-5L instruments. Epidemiol Biostat Public Health. 2015;12:11457–1. [Google Scholar]
- Schmitz N, Kruse J, Kugler J. Disabilities, quality of life, and mental disorders associated with smoking and nicotine dependence. Am J Psychiatry. 2003;160:1670–6. doi: 10.1176/appi.ajp.160.9.1670. [DOI] [PubMed] [Google Scholar]
- Shiroiwa T, Fukuda T, Ikeda S, et al. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual Life Res. 2016;25:707–19. doi: 10.1007/s11136-015-1108-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Son BK, Markovitz JH, Winders S, Smith D. Smoking, nicotine dependence, and depressive symptoms in the CARDIA study: Effects of educational status. Am J Epidemiol. 1997;145:110–6. doi: 10.1093/oxfordjournals.aje.a009081. [DOI] [PubMed] [Google Scholar]
- Stewart AL, King AC, Killen JD, Ritter PL. Does smoking cessation improve health-related quality-of-life? Ann Behav Med. 1995;17:331–8. doi: 10.1007/BF02888598. [DOI] [PubMed] [Google Scholar]
- Strandberg AY, Strandberg TE, Pitkälä K, et al. The effect of smoking in midlife on health-related quality of life in old age: A 26-year prospective study. Arch Iran Med. 2008;168:1968–74. doi: 10.1001/archinte.168.18.1968. [DOI] [PubMed] [Google Scholar]
- Strine TW, Okoro CA, Chapman DP, et al. Health-related quality of life and health risk behaviors among smokers. Am J Prev Med. 2005;28:182–7. doi: 10.1016/j.amepre.2004.10.002. [DOI] [PubMed] [Google Scholar]
- Talati A, Keyes K, Hasin D. Changing relationships between smoking and psychiatric disorders across twentieth century birth cohorts: clinical and research implications. Mol Psychiatry. 2016;21:464–71. doi: 10.1038/mp.2015.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tavafian SS, Aghamolaei T, Zare S. Water pipe smoking and health-related quality of life: a population-based study. Arch Iran Med. 2009;12:232–7. [PubMed] [Google Scholar]
- Taylor G, McNeill A, Girling A, et al. Change in mental health after smoking cessation: systematic review and meta-analysis. BMJ. 2014;348:1151. doi: 10.1136/bmj.g1151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tillmann M, Silcock J. A comparison of smokers'and ex-smokers'health-related quality of life. J Public Health. 1997;19:268–73. doi: 10.1093/oxfordjournals.pubmed.a024629. [DOI] [PubMed] [Google Scholar]
- Vogl M, Wenig CM, Leidl R, Pokhrel S. Smoking and health-related quality of life in English general population: implications for economic evaluations. BMC Public Health. 2012;12:203. doi: 10.1186/1471-2458-12-203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson D, Parsons J, Wakefield M. The health-related quality-of-life of never smokers, ex-smokers, and light, moderate, and heavy smokers. Prev Med. 1999;29:139–44. doi: 10.1006/pmed.1999.0523. [DOI] [PubMed] [Google Scholar]