

Abstract
BACKGROUND AND OBJECTIVE:
The objective of this systematic review was to determine from published data the prevalence of Vitamin D deficiency in the Saudi population.
METHODS:
An extensive and meticulous search was conducted for studies published in MEDLINE, EMBASE the Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews (2008–2015), and the Science Citation Index published data from the Annals of Saudi Medicine and Saudi Medical Journal with the key words: Vitamin D deficiency, insufficiency, and Saudi Arabians. The inclusion criterion was studies published during 2008 to 2015, and studies involving healthy individuals between the age of 18 and 80 years. Binary random- effect model was used to estimate pooled Vitamin D deficiency. Prevalence rates along with overall estimate were presented by forest plot. Heterogeneity test was used to assess the significance of heterogeneity among studies.
RESULTS:
The authors identified 26 potentially relevant articles, 16 of which met the inclusion criteria. A total of 20,787 patients were analyzed. Sixty-two percent (12,959) were females, and the rest were males. The overall Vitamin D deficiency was 63.5% (95% CI: 53.3, 73.7).
CONCLUSIONS:
The currently available literature on the Saudi Arabian population suggests that the Vitamin D deficiency is around 60% and not 100% as indicated in some studies. The relatively small number of studies on the population and the different modes of diagnostic methodology used make the issue of correct figures of Vitamin D deficiency contentious.
Keywords: Deficiency, insufficiency, meta-analysis, Saudi Arabia, Vitamin D
Introduction
Vitamin D is a fat-soluble vitamin produced endogenously when the skin is exposed to the ultraviolet light and is also present in some foods and other dietary supplements. Initially, it was believed that Vitamin D was important for musculoskeletal health; however, recent studies indicate that it is also important in the maintenance of health other systems and the prevention of certain malignancies.[1,2,3,4,5] In Saudi Arabia, studies in Vitamin D conducted as early as 1983–1984 indicated a deficiency of 30% in the general population.[6,7] In the recent past, there has been a burgeoning of reports on Vitamin D in the world, and Saudi Arabia was not immune to it. Published data reveal that in the Saudi Arabian population, Vitamin D deficiency is as high as 100%[8,9,10,11,12,13,14,15,16,17,18,19,20,21,22] even though the major cities in the country lie in the tropics: Riyadh at 24°42’N, 46° 43’ E, Jeddah: 21°32’N, 39° 10’ E, and Dammam 26.3927° N, 49.9777° E. The question is why should a population whose diet is adequate and live in the sunny climate have very low Vitamin D levels? Many reasons have been put forward, including inactivity of the individuals at risk, chronic diseases, diabetes mellitus, obesity all of which are thought to be causative factors of low Vitamin D levels.[23,24] Other factors which could also influence low levels of Vitamin D could be genetic, different methods of assessment, and screening criteria. This could have varied the reported deficiency between 50% and 100%.
To find the average levels of Vitamin D deficiency in Saudi Arabian population, this meta-analysis was conducted between 2008 and 2015 with clear inclusion and exclusion criteria.
Methods
An extensive and meticulous search was conducted for studies published between January 2008 and December 2015 in MEDLINE, EMBASE the Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews (2008–2015) and the Science Citation Index published data from the Annals of Saudi Medicine and Saudi Medical Journal. The search was conducted with the key words: Vitamin D, deficiency, insufficiency, and Saudi Arabians. Institutional Review Board approval was obtained from the Imam Abdul Rahman Bin Faisal University, Dammam. The inclusion criteria were studies published in English only and conducted on at least 100 healthy Saudi Arabian individuals between the ages of ≥18 and ≤80 years. Prospective and retrospective studies and those with questionnaires that avoided other metabolic diseases were included to reduce the chance of confounding and limit bias. Three broad issues with 11-point questions were considered during appraisal for inclusion: the results, the validity of the results of the study and finally, the impact of the results and analysis locally. Only 16 out of 26 published studies were selected.
Two authors independently reviewed the articles and abstracted the data and a whole team of authors agreed on the extraction results. Normal Vitamin D level was defined as ≥30 ng/mL, insufficiency between 21 and 29 ng/mL and deficiency as ≤20 ng/mL. The authors called the hospitals to be used in the meta-analysis study to find out the methodology, they used to assess Vitamin D levels. The data were entered in the database and analyzed using software package for statistical analysis Version 19. SPSS Inc. Chicago, Illinois, USA. The data were expressed as mean and standard deviation (±SD). Statistically significant differences between groups were determined by using Student t-test and P < 0.05 was held as statistically significant. Binary random-effect model is used to estimate pooled Vitamin D deficiency. Prevalence rates along with overall estimate are presented by forest plot. Heterogeneity test is used to assess the significance of heterogeneity among studies.[25,26]
Results
Twenty-six studies were identified and 16 fulfilled the inclusion and exclusion criteria in men and women who were apparently healthy. A total of 20787 patients were analyzed. The baseline characteristics of the studies analyzed with all cohorts included men and women and age groups between 18 and 80 years. Sixty-two percent (12959) were females and the rest were males. The average age was 34.5±8.5 years.
Table 1 gives the Vitamin D prevalence estimates by different studies. Majority of the studies were cross sectional and one was random selection. Five studies were reported from Central region, six from Eastern Region, 2 from Western Province, 2 from Qassim region and one was from Taif [Figure 1]. The technique used for assessment of vitamin D levels in all the hospitals was Chemiluminescence immunoassay. Only one hospital used HPLC-LC MS as well as Chemiluminescence immunoassay. Table 2 shows the Binary Random-Effects Model pooled estimates. The over all Vitamin D deficiency was 63.6% (95% CI: 53.3% - 73.7%) [Table 2]. Vitamin D deficiency prevalence for each study, and the overall summary estimate for Vitamin D deficiency are presented by Forest Plot [Figure 2].
Table 1.
Vitamin D prevalence estimates by studies
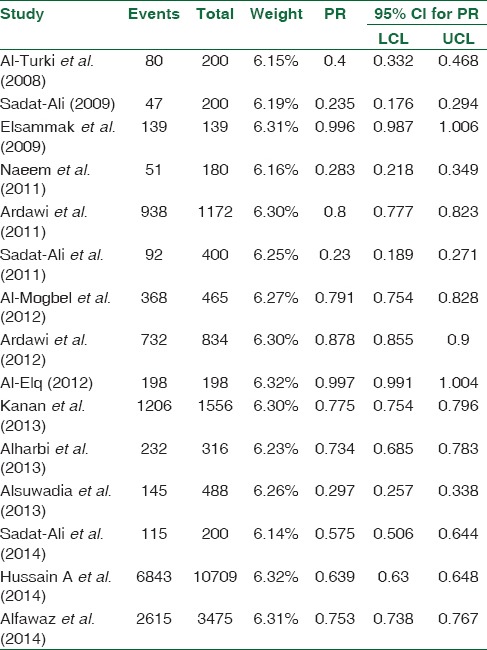
Figure 1.

Regions of Saudi Arabia from where studies were published
Table 2.
Binary random-effects model pooled estimates

Figure 2.
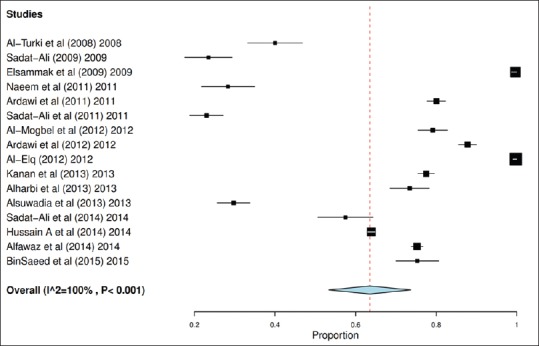
Forest plot of vitamin D deficiency prevalence
Discussion
Our meta-analysis shows that the overall Vitamin D deficiency in the healthy Saudi Arabian population is 60% and not 100% as reported in some studies. A normal level of Vitamin D (≥30 ng/mL or 75 nmol/l) was seen in 17.83% of the population. The baseline of our analysis in this study was (≥30 ng/mL or 75 nmol/l) as normal and ≤20 ng/mL as deficient. The level at which the symptoms of Vitamin D deficiency become severe enough to make an impact on the skeleton are not known, and this has led to the belief that a level of ≥20 ng/ml could be considered normal. In the United States, with the serum level of Vitamin D deficiency at ≤20 ng/mL (50 nmol/L), the overall deficiency was 41.6%, 69.2% in Hispanics and 82.1% in the Afro-American population.[27] If we label deficiency as ≤20 ng/mL, the deficiency in the Saudi Arabian population will be similar to what is found in the United States. This review highlights the reported high prevalence of low levels of Vitamin D in the Saudi population, which appears to be due to unjustified high cutoff values of serum 25 hydroxy-Vitamin D. This particular information transmitted to the social media from the medical field has created a state of near panic in the general population and some physicians are taking irrational decisions to treat Vitamin D deficiency.
There are many factors which influence the levels of Vitamin D other than diet and sunshine. Hussain et al.[21] indicated that the prevalence of hypovitaminosis D was more common and severe in Saudis than in non-Saudis living in the same areas and probably eating the same diet. Reports in the literature suggest a strong genetic influence on the circulating Vitamin D levels in different populations.[28,29] The first study in this assessment of the genetic influence in the Saudi Arabian population was reported by Sadat-Ali et al.,[30] who found that individuals who had GG allele of the three SNPs VDR rs2228570, CYP2R1 rs10741657, and GC rs4588 had significantly lower levels of 25OHD compared to the population with normal levels.
The second issue of varied Vitamin D deficiency in different parts of the Kingdom of Saudi Arabia could be due to the techniques of assessing the serum levels. In Saudi Arabia, most of the assessments of the Vitamin D is done in-house hospitals, at least, as presented in this meta-analysis. Therefore, a ± 5–10 ng/ml error can move a patient from normal to insufficiency and insufficiency to deficiency. Sadat-Ali et al,[20] found that 23% of patients had a false positive for Vitamin D deficiency when CLIA-chemiluminescence immunoassay was used. Binkley et al.,[31] in a recent review raised concerns that the wide variability in laboratory measurement of serum 25-hydroxyvitamin D is causing chaos and hindering the definition of the status of deficiency.
This meta-analysis has limitations. The reports which were analyzed had come from hospitals of different levels (Primary care or Tertiary care), where different laboratory techniques for assessment were used.
The study has definite limitations. The first is the observational study data used in the meta-analysis. In spite of the limitation of the design of observational studies and the lack of randomization and potential biases, meta-analysis on observational studies is still one of the few methods that can reveal areas that require further research.
The strength of this study is that we were able to analyze over 20,000 patients, which gave us the results of the deficiency of Vitamin D at around 60%.
Conclusion
We believe that before we label the country as having a population with a massive issue of Vitamin D deficiency, it would be prudent to clearly state the level of serum 25 OHD that should be taken as deficiency. Second, we need to study a large population at the same time of the year with same laboratory assessment technique before we can determine the correct percentage of the population with Vitamin D deficiency.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Jamil NA, Gray SR, Fraser WD, Fielding S, Macdonald HM. The relationship between Vitamin D status and muscle strength in young healthy adults from sunny climate countries currently living in the Northeast of Scotland. Osteoporos Int. 2017;28:1433–43. doi: 10.1007/s00198-016-3901-3. [DOI] [PubMed] [Google Scholar]
- 2.Bhattoa HP, Konstantynowicz J, Laszcz N, Wojcik M, Pludowski P. Vitamin D: Musculoskeletal health. Rev Endocr Metab Disord. 2017;18:363–71. doi: 10.1007/s11154-016-9404-x. [DOI] [PubMed] [Google Scholar]
- 3.Manson JE, Mayne ST, Clinton SK. Vitamin D and prevention of cancer – Ready for prime time? N Engl J Med. 2011;364:1385–7. doi: 10.1056/NEJMp1102022. [DOI] [PubMed] [Google Scholar]
- 4.Zhang X, Harbeck N, Jeschke U, Doisneau-Sixou S. Influence of Vitamin D signaling on hormone receptor status and HER2 expression in breast cancer. J Cancer Res Clin Oncol. 2017;143:1107–22. doi: 10.1007/s00432-016-2325-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Narvaez CJ, Matthews D, LaPorta E, Simmons KM, Beaudin S, Welsh J, et al. The impact of Vitamin D in breast cancer: Genomics, pathways, metabolism. Front Physiol. 2014;5:213. doi: 10.3389/fphys.2014.00213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sedrani SH, Elidrissy AW, El Arabi KM. Sunlight and Vitamin D status in normal Saudi subjects. Am J Clin Nutr. 1983;38:129–32. doi: 10.1093/ajcn/38.1.129. [DOI] [PubMed] [Google Scholar]
- 7.Sedrani SH. Vitamin D status of Saudi men. Trop Geogr Med. 1984;36:181–7. [PubMed] [Google Scholar]
- 8.Al-Turki HA, Sadat-Ali M, Al-Elq AH, Al-Mulhim FA, Al-Ali AK. 25-hydoxyvitamin D levels among healthy Saudi Arabian women. Saudi Med J. 2008;29:1765–8. [PubMed] [Google Scholar]
- 9.Sadat-Ali M, AlElq A, Al-Turki H, Al-Mulhim F, Al-Ali A. Vitamin D levels in healthy men in Eastern Saudi Arabia. Ann Saudi Med. 2009;29:378–82. doi: 10.4103/0256-4947.55168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Elsammak MY, Al-Wossaibi AA, Al-Howeish A, Alsaeed J. High prevalence of Vitamin D deficiency in the sunny Eastern region of Saudi Arabia: A hospital-based study. East Mediterr Health J. 2011;17:317–22. [PubMed] [Google Scholar]
- 11.Naeem Z, Almohaimeed A, Sharaf FK, Ismail H, Shaukat F, Inam SB, et al. Vitamin D status among population of Qassim region, Saudi Arabia. Int J Health Sci (Qassim) 2011;5:116–24. [PMC free article] [PubMed] [Google Scholar]
- 12.Ardawi MS, Qari MH, Rouzi AA, Maimani AA, Raddadi RM. Vitamin D status in relation to obesity, bone mineral density, bone turnover markers and Vitamin D receptor genotypes in healthy Saudi pre- and postmenopausal women. Osteoporos Int. 2011;22:463–75. doi: 10.1007/s00198-010-1249-7. [DOI] [PubMed] [Google Scholar]
- 13.Sadat-Ali M, Al Elq AH, Al-Turki HA, Al-Mulhim FA, Al-Ali AK. Influence of Vitamin D levels on bone mineral density and osteoporosis. Ann Saudi Med. 2011;31:602–8. doi: 10.4103/0256-4947.87097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Al-Mogbel ES. Vitamin D status among adult Saudi females visiting primary health care clinics. Int J Health Sci (Qassim) 2012;6:116–26. doi: 10.12816/0005987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ardawi MS, Sibiany AM, Bakhsh TM, Qari MH, Maimani AA. High prevalence of Vitamin D deficiency among healthy Saudi Arabian men: Relationship to bone mineral density, parathyroid hormone, bone turnover markers, and lifestyle factors. Osteoporos Int. 2012;23:675–86. doi: 10.1007/s00198-011-1606-1. [DOI] [PubMed] [Google Scholar]
- 16.Kanan RM, Al Saleh YM, Fakhoury HM, Adham M, Aljaser S, Tamimi W, et al. Year-round Vitamin D deficiency among Saudi female out-patients. Public Health Nutr. 2013;16:544–8. doi: 10.1017/S1368980012002947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Al-Elq AH. The status of Vitamin D in medical students in the preclerkship years of a Saudi medical school. J Family Community Med. 2012;19:100–4. doi: 10.4103/2230-8229.98293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Alharbi A, Al-Omery A, Hedaib S. Prevalence of Vitamin D deficiency in Saudi men. J Appl Med Sci. 2013;1:863–6. [Google Scholar]
- 19.Alsuwadia AO, Farag YM, Al Sayyari AA, Mousa DH, Alhejaili FF, Al-Harbi AS, et al. Prevalence of Vitamin D deficiency in Saudi adults. Saudi Med J. 2013;34:814–8. [PubMed] [Google Scholar]
- 20.Sadat-Ali M, Al-Elq AH, Al-Shaikh IH, Al-Turki HA, Al-Ali AK, Al-Othman AA, et al. Assessment of low Vitamin D among Saudi Arabians. Did we overshoot the runway? Saudi Med J. 2014;35:1243–9. [PMC free article] [PubMed] [Google Scholar]
- 21.Hussain AN, Alkhenizan AH, El Shaker M, Raef H, Gabr A. Increasing trends and significance of hypovitaminosis D: A population-based study in the Kingdom of Saudi Arabia. Arch Osteoporos. 2014;9:190. doi: 10.1007/s11657-014-0190-3. [DOI] [PubMed] [Google Scholar]
- 22.Alfawaz H, Tamim H, Alharbi S, Aljaser S, Tamimi W. Vitamin D status among patients visiting a tertiary care center in Riyadh, Saudi Arabia: A retrospective review of 3475 cases. BMC Public Health. 2014;14:159. doi: 10.1186/1471-2458-14-159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.BinSaeed AA, Torchyan AA, AlOmair BN, AlQadhib NS, AlSuwayeh FM, Monshi FM, et al. Determinants of Vitamin D deficiency among undergraduate medical students in Saudi Arabia. Eur J Clin Nutr. 2015;69:1151–5. doi: 10.1038/ejcn.2014.286. [DOI] [PubMed] [Google Scholar]
- 24.Khayyat Y, Attar S. Vitamin D deficiency in patients with irritable bowel syndrome: Does it exist? Oman Med J. 2015;30:115–8. doi: 10.5001/omj.2015.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Viechtbauer W. Conducting meta-analyses in R with the meta for package. J Stat Softw. 2010;36:1–48. [Google Scholar]
- 26.Wallace B, Dahabreh I, Trikalinos T, Lau J, Trow P, Schmid C. Closing the gap between methodologists and end-users: R as a computational back-end. J Stat Softw. 2012;49:1–15. [Google Scholar]
- 27.Forrest KY, Stuhldreher WL. Prevalence and correlates of Vitamin D deficiency in US adults. Nutr Res. 2011;31:48–54. doi: 10.1016/j.nutres.2010.12.001. [DOI] [PubMed] [Google Scholar]
- 28.Coşkun S, Şimşek Ş, Camkurt MA, Çim A, Çelik SB. Association of polymorphisms in the Vitamin D receptor gene and serum 25-hydroxyvitamin D levels in children with autism spectrum disorder. Gene. 2016;588:109–14. doi: 10.1016/j.gene.2016.05.004. [DOI] [PubMed] [Google Scholar]
- 29.Pike JW, Meyer MB, Benkusky NA, Lee SM, St. John H, Carlson A, et al. Genomic determinants of Vitamin D-regulated gene expression. Vitam Horm. 2016;100:21–44. doi: 10.1016/bs.vh.2015.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sadat-Ali M, Al-Turki HA, Azam MQ, Al-Elq AH. Genetic influence on circulating Vitamin D among Saudi Arabians. Saudi Med J. 2016;37:996–1001. doi: 10.15537/smj.2016.9.14700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Binkley N, Dawson-Hughes B, Durazo-Arvizu R, Thamm M, Tian L, Merkel JM, et al. Vitamin D measurement standardization: The way out of the chaos. J Steroid Biochem Mol Biol. 2017;173:117–21. doi: 10.1016/j.jsbmb.2016.12.002. [DOI] [PubMed] [Google Scholar]