

Abstract
BACKGROUND:
Falls among the elderly are one of the major causes of morbidity and mortality worldwide. They constitute the second leading cause of unintentional deaths after road-traffic accidents. The aim of the study was to estimate the prevalence of falls among the elderly and to investigate the factors that contribute to this phenomenon.
MATERIALS AND METHODS:
A cross-sectional analytical study was conducted in the elderly, over the age of 60, in Riyadh. The sample under scrutiny was estimated to be 357 in total. A pilot study was conducted among 15 subjects. Two questionnaires were used for the interviews which were translated into Arabic using the “Morse Fall Scale.” The questionnaires assessed: the participants’ previous history of falls, whether a secondary diagnosis had been obtained, whether any ambulatory aids had been used or whether an IV connection had been fitted during convalescence. They also inquired if any gait/transferring device had been used to assist the patient at any time.
RESULTS:
Out of 357 participants, 206 (57.7%) had a history of falls. Study found an association between the number of falls recorded, the age of the participants, and whether the participant was female. Furthermore, there were statistically significant associations between the history of falls and a condition of impaired health. The results also showed that environmental hazards play a significant role in the occurrence of falls with P ≤ 0.001, in which 103 (81.7%) of the individuals who were exposed to environmental hazards revealed a history of falls.
CONCLUSION:
Falls among the elderly are common. Significantly, if the health of the individuals is impaired, and there are contiguous environmental risk factors, these elements combine to play a part in the occurrence of such falls. There is, therefore, a need to design and develop a health awareness program to prevent such problems in the elderly.
Keywords: Elderly, falls, Saudi Arabia
Introduction
Falls are one of the most common problems in the elderly around the world. A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or at another lower level.[1] Currently, there is no numerical criterion that classifies people as “elderly.” However, the United Nations has determined that the age of 60+ should be used to refer to people as being “elderly.”[2] This is in spite of the fact that most developed countries take the chronological age of 65 years to define the ‘elderly.[2] In the United States, falls are a leading cause of morbidity and mortality among mature adults.[3] It is the second leading cause of accidental or unintentional injury/death after road traffic injuries.[4] For example, of the 11 million adults aged 65 years and over living in the UK, around 30% of community-dwelling mature adults fall at least once in their lifetime.[5] It was found in a study conducted in the Eastern Mediterranean Region that 30%–40% of adults older than 65 years residing in the community fall each year. The rates were higher in hospitalized patients and nursing home residents. Moreover, the incidence of falls rose steadily from middle-age onward peaking in persons older than 80 years.[6]
In Qatar, the prevalence of falls among the elderly in 2008 was 34% (119 of 355 attendees); out of this figure, 47% of elderly individuals suffered a fall while 53% experienced recurrent falls.[7] Each year, emergency departments treat millions of people aged 65 and older for falls. Significantly, over 700,000 patients a year are hospitalized because of a fall injury.[8] Treating fall injuries among elderly patients is proving to be extremely costly. In the United States, national estimates of the incidence and direct medical costs associated with fall-related injuries in mature patients aged ≥65 in 2000, showed that 10,300 were fatal. Furthermore, an additional 2.6 million nonfatal fall-related injuries were reported. The estimated total cost of medical treatment for these injuries was $0.2 billion for fatal falls and $19 billion for nonfatal falls.[9] Even though the majority of falls do not cause injuries, about 20% of them lead to a serious injury (such as a fracture or a head injury). These injuries can greatly restrict a person in their everyday activities, or prevent them from living on their own as they need to be cared for after the fall.[10]
Falls may be associated with various contiguous environmental hazards such as carpets and rugs. Most falls (72.8%) occur at home. Women represented 80.2% of fall injury victims. Not surprisingly, perhaps, the most common location for fall injuries in the home is the bathroom (35.7%).[11] Other environmental hazards include poor stairway design and disrepair, inadequate lighting, clutter, slippery floors, unsecured mats, and the lack of nonskid surfaces in bathtubs.[12] There is a paucity of literature on the important topic of falls amongst the elderly in the Kingdom of Saudi Arabia. However, our study will focus on estimating the true extent of falls among the elderly within the community in Riyadh alone and examine the relationship between the health status of elderly people as well as the impact of the environment on their propensity to experience falls.
Materials and Methods
This cross-sectional analytical study was conducted among the elderly in the community in Riyadh from August 2015 to April 2016. The Institutional Review Board at King Saud University (College of Medicine) approved the study protocol. The study was carried out in several different locations in Riyadh. The investigators divided Riyadh into five sections, namely, the North of the city, the South, Riyadh Central, the East, and the West. Then, the biggest mosques, malls, hospitals, and health centers in these sections were selected. People who went to these mosques, malls, hospitals, and health centers were invited to complete the questionnaires as was convenient. The participants in the study were both men and women (60-year-old or above) living in Riyadh. Informed consent was obtained before the start of the study and participation in the study was voluntary. Sociodemographic variables included in the questionnaire were age, gender, residence, marital status, level of education, and nature of work.
The investigators used two well-standardized and validated tools. First, the participants completed the “Morse Fall Scale” questionnaire which consists of six variables (relating to their previous history of falls, whether a secondary diagnosis had been obtained) this meant that if a participant had more than one diagnosis such as diabetes mellitus, hypertension, asthma, cerebrovascular accident (CVA), rheumatoid arthritis, cancer, and cataract/refractive errors are all examples of chronic conditions he or she would be scored as 15; if the participant had <2 diseases the score would be (0), the type of ambulatory aids used. This was scored as 0 if the patient walked without a walking aid (even if assisted by a nurse), used a wheelchair, or was on a bed rest and was completely bedridden. If the patient used crutches, a cane, or a walker, this item scored 15; if the patient ambulated holding onto furniture for support, the score for this item was (30), if an IV connection or gait/transferring device had been used and their mental status). The risk of falls was divided into three categories: no risk [0–24], low or moderate risk [25–45], and high risk (i.e., >45 on the scale).[13]
Second, elderly participants completed the Missouri Alliance for Home Care (MAHC-10) fall risk assessment tool. The MAHC-10 consists of ten variables are age, medical diagnoses, history of falls within the last 3 months, incontinence, vision impairment, problems in movement, medication, mental status, and environmental hazards. These included poor illumination, equipment tubing, inappropriate footwear, pets, hard to reach items, floor surfaces that are uneven or cluttered, outdoor entry and exits, as well as any pain suffered that would affect their level of function. Each of these variables was recorded at one point. Four points or more suggests that the person has a risk of falling.[14] Permission from the copyright owner was received before embarking on the study to translate the questions into Arabic and use the “Morse Fall Scale.” Furthermore, the (MAHC-10) fall risk assessment tool is available free of cost.
The original English versions of both questionnaires were translated following the recommendations outlined in the “Process of translation and adaptation of instruments” set forth by the World Health Organization.[15] Two experienced bilingual English teachers from King Saud University who were fluent in English (and whose mother tongue was Arabic) independently translated the questionnaires from English to Arabic. The resulting versions were then translated back into English by a professional translator who had never seen the original English questionnaires. This was done to reduce bias in translation. The translated versions were first corrected for any errors and were then culturally adapted with the help of the translators, to eliminate any ambiguities between the original and back-translated versions. A pilot study was conducted on 15 Arabic-speaking participants using the final Arabic version of the questionnaires, and the questions which were deemed clear took just (3–4) minutes to answer.
The study sample size was estimated according to the formula: N = Z2 P (1-P)/d2. Where N = sample size, Z = the Z statistic for a level of confidence. Notably, a 95% level of confidence was used; therefore, the Z value was 1.96. Moreover, P = the percentage of falls of the elderly (approximate 28%) according to a global report on “The Prevention of Falls” published in the Epidemiology of Falls,[16] d = the degree of precision (0.05). The sample size was estimated to be 310 in total, but 357 elderly adults were studied. The data collection was done by interviews.
Data analysis was conducted using SPSS 21 (IBM, NY, USA) to determine certain objectives as follows: (1) To estimate the prevalence of falls of the elderly within a segment of the Saudi population in Riyadh city by the use of descriptive statistics, (2) To investigate the relationship between the health status of mature adults and the severity of the falls they have experienced through cross-tabulation and Chi-square testing, and (3) To investigate further the relationship between the falls suffered by the elderly and contiguous environmental factors using cross-tabulation and Chi-square statistical testing.[17]
Results
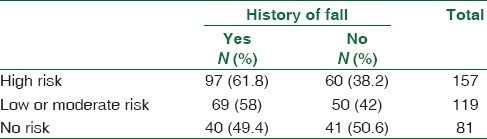
A total of 357 eldery participated in the study; 47 % were male, and 46.5% were older than 70 years [Table 1]. Fifty seven percent of the elderly gave a history of a fall. Significantly, the prevalence of falls was higher in females than in males by 14%. Furthermore, age was strongly correlated with the occurrence of falls, and the prevalence of these falls gradually increased with age up to the age of 90 years after which there was a decrease in the number of falls. Table 2 shows the link between the Morse scale and its association with age. The risk of suffering a fall progressively increases with age in the following manner: 60–69 years (34%), 70–79 years (49%), 80–89 years (65.5%), and above 90 years (63%). Using the (MAHC-10) fall risk assessment tool, the risk of suffering a fall also increased with advancing age as shown in Table 3 The results for each age group are as follows: 60–69 years (67.9%), 70–79 years (81%), 80–89 years (93%), and above 90 years (100%). To investigate the relationship between the health status of the elderly and the incidence of falls, several variables have been analyzed using the Morse Fall Scale [Table 4]. From the data obtained, the authors of this paper found that 64% of the individuals had obtained a secondary diagnosis, 44.4% had normal gait, 71.1% of the individuals had weak gait, and 83.3% of the individuals who had an impaired gait had a history of falls with a P < 0.001. This finding indicates that as the impairment in gait increased in severity, there was a marked increase in the incidence of falls. Table 5 explains that the percentage of individuals who demonstrated a high risk of falls (risk score + 45) is 44.5%, whereas those with a low- or moderate-risk of falls (risk score 25–45) is 32.8%. Finally, those individuals who demonstrated no risk (risk score 0–24) is 22.7%. On the other hand, in relation to the second scale: (MAHC-10) fall risk assessment tool, [Table 6], the variables were analyzed according to age, incontinence, vision, problems in movement, medication, mental status, and environmental hazards in relation to the incidence of falls. The results showed that there was a significant association with the number of falls documented and all associated factors with (P < 0.001) with the exception of visual impairment. This resulted in a value of P = 0.01. Moreover, according to the data, there was no significant association between mental status and the occurrence of falls (P = 0.02) (3). Finally, there was a strong association between the occurrence of falls and environmental hazards, resulting in a P < 0.001 where 103 (81.7%) of the individuals who were exposed to environmental hazards had a history of falls [Table 7]. Showed that the higher the Morse risk score the higher the possibility of the older falls. About 62% of the individuals with high Morse risk score suffered from falls compared with 49.4% among individuals with no risk on Morse score.
Table 1.
The prevalence of falls in relation to the age and gender of the study participants (n=357)
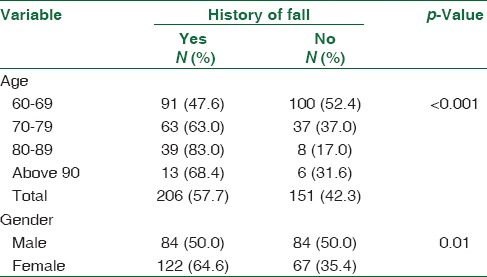
Table 2.
The relationship between the classifications of the Morse fall scale and age and gender of study participants (n=357)
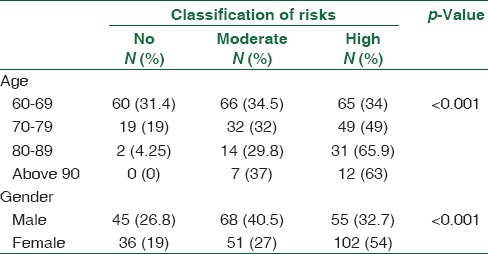
Table 3.
The relationship between the classifications of the Missouri Alliance for Home Care and age-gender of study participants (n=357)
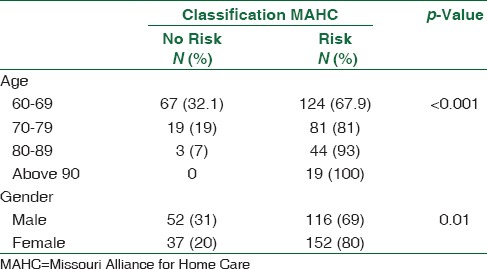
Table 4.
The association of Morse scale variables with “fall” among study participants (n=357)
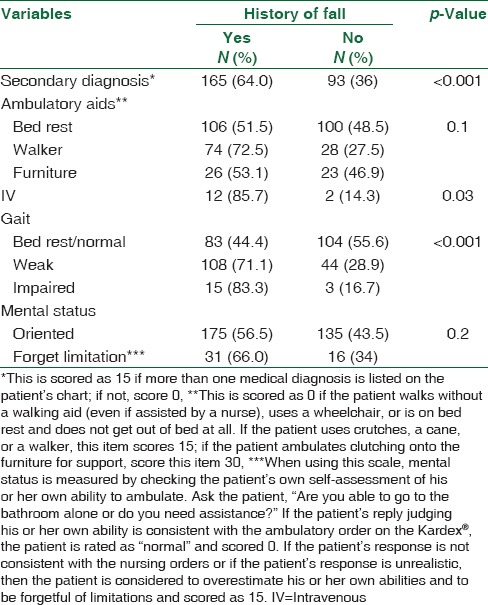
Table 5.
Study participants' risk of fall according to Morse score (n=357)

Table 6.
The association of Missouri Alliance for Home Care-10 variables with “fall” among study participants (n=357)
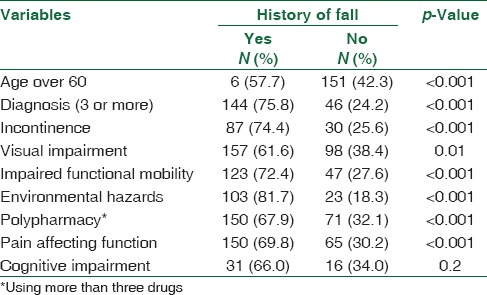
Table 7.
The percentage of individuals who were at high risk and had a history of falls according to the Morse Score (n=357)
Discussion
Older adults comprise a part of the community who require more attention and special care than the rest of society. Falls are a serious health problem that elderly people inevitably face. The study showed that among the sample of 357 elderly people surveyed in Riyadh, the history of falls was found to be 57.7%. This finding shows that more than half of the elderly participants had a history of falls, which is higher than what we expected. The prevalence of falls in Saudi Arabia/Riyadh is double the number of falls in Brazil.[18] Moreover, this number is greater than the number of falls in such countries as Japan,[19] India,[20] and Qatar which have a 34% prevalence of falls.[7] Furthermore, a study carried out in the United States shows a difference of 29% in the number of recorded falls.[21] Significantly, our study showed 14% more recorded falls in Saudi women than in Saudi men. Interestingly, a study in the US found that 30.3% of women were more likely to report a fall as opposed to 26.5% of their male counterparts who would report such an event. This shows that there is only a small difference in the incidence of falls between the two groups. This may reflect the pattern of low physical fitness demonstrated by our population, particularly the elderly. Seeing that the lives of the majority of our population are sedentary with low physical activity, this presents a serious health risk for the older generation.[22]
Our study showed that age is strongly associated with falls in that the prevalence of falls progressively increased with age. Incidentally, these findings are compatible with another study.[23] It is worth noting that the history of falls increases with age until the age of 90 when it begins to decrease. This decline in the falls may be due either to reduced mobility at this age or because the proportion of Saudi men and women who actually live to this age is small. The analysis of the risk of falls using the “Morse Fall Scale” and MAHC10-fall risk assessment tool found that there is an increased association between a rise in age and the number/incidence of falls. This increase in the risk of falls with age was found in another study.[23]
Present study showed that there is an increased risk of falling if the elderly individual happens to suffer from gait impairment. Accordingly, the more severe the gait impairment is, the higher the chances of that individual suffering a fall. This was similar to a study conducted in Brazil.[18] In addition, the highest association of falls is with those who use walkers more than all other walking aids, for 72.5% of the elderly who use it had had a history of fall. 85.7% of people using intravenous (IV) connections had a history of a fall.
The history of falls was strongly associated with incontinence, problems pertaining to movement, medication, vision, mental impairment, environmental hazards and pain affecting the level of function in various joints. A similar finding was reported in a previous study in India.[24] In general, the strongest association with falls were with environmental hazards where 81.7% of people exposed to environmental hazards had had a fall. A study in South Korea, reported that some hazards such as, a door sill, slippery floors in the bathroom, and poor night lights were all significant factors that caused a fall.[25] It also found that about 75% of the elderly who were diagnosed with 3 or more diseases had a history of a fall. Similar findings were also reported in a study conducted in Canada, 2014;[26] the risk of suffering a fall is significantly greater in individuals with multiple chronic conditions compared to those with none.[26]
Diabetes mellitus, hypertension, asthma, CVA, rheumatoid arthritis, cancer, and cataract/refractive errors are all examples of chronic conditions found in the majority of elderly patients who had had falls in one study conducted among elderly Indian patients.[20] As much as 74.4% of elderly people with incontinence had a history of falling as they tended to use the bathroom frequently during the night and encountered various obstructions in the corridors. Moreover, visual problems too were shown to result in falls in as many as 61.6% of the elderly people surveyed. Besides, 72.4% of elderly patients with gait problems had a history of a fall.[25] Polypharmacy is another risk factor and is associated with 67.9% history of falls, a figure that is similar to the result generated in another study (Japan, 2013).[19] Thus, a fall may occur as a direct consequence of the patient's underlying disease or it may be due to the side effects of some medications, or a combination of both of these factors.
We hope this study has highlighted the grave danger that falls pose and the fact that they are a common occurrence which can very easily be prevented. The sample demographic was compiled from different parts of Riyadh using a simple strategy (see Materials and Methods section). It was difficult to recruit and interview them, and there was discrepancy in the number of participants from different sections of Riyadh. The environmental factors or hazards highlighted in this study should also be further studied to discover any additional association with falls of the elderly.
Conclusion
There is a high prevalence of falls among the elderly in the city of Riyadh. The risk of such falls increases with age and has a strong relationship with the health status of these elderly individuals. Moreover, there is a clear association with environmental factors. There is, therefore, a need to design and develop a health awareness program to prevent these problems that cause the elderly a great deal of suffering.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to thank all the people who participated in the study. Special thanks to Mr. Janice Morse and MAHC for making the Morse scale tool and MAHC-10 available for researchers. The study was supported by Research chair of health education and health promotion, the College of Medicine, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia.
References
- 1.Geneva: World Health Organization; World Health Organization. Ageing, Life Course Unit. WHO Global Report on Falls Prevention in Older Age. 2008. [Google Scholar]
- 2.World Health Organization (WHO). Proposed Working Definition of an Older Person in Africa for the MDS Project: Definition of an Older or Elderly Person. [Last accessed on 2015 Jun 09]. 2013. Available from: http://www.Who.Int/healthinfo/survey/ageingde-fnolder/en/
- 3.Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319:1701–7. doi: 10.1056/NEJM198812293192604. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization. Falls. [Last accessed on 2016 Sep 30]. Available from: http://www.who.int/mediacentre/factsheets/fs344/en/
- 5.Nazarko L. Modifiable risk factors for falls and minimizing the risk of harm. Nurse Prescribing. 2015;13:192–8. [Google Scholar]
- 6.Al-Faisal W. Geneva, Switzerland: World Health Organisation; Falls Prevention for Older Persons: Eastern Mediterranean Regional Review. 2006. [Google Scholar]
- 7.Almawlawi E, Al Ansari A, Ahmed A. Prevalence and risk factors for falls among the elderly in primary healthcare centers (PHC) in Qatar. Qatar Med J. 2011;2011:7. [Google Scholar]
- 8.Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-Based Injury Statistics Query and Reporting System (WISQARS) [Last accessed on 2013 Aug 15]. Available from: https://www.cdc.gov/injury/wisqars/index.html .
- 9.Stevens JA, Corso PS, Finkelstein EA, Miller TR. The costs of fatal and non-fatal falls among older adults. Inj Prev. 2006;12:290–5. doi: 10.1136/ip.2005.011015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: Injury severity is high and disproportionate to mechanism. J Trauma Acute Care Surg. 2001;50:116–9. doi: 10.1097/00005373-200101000-00021. [DOI] [PubMed] [Google Scholar]
- 11.Rosen T, Mack KA, Noonan RK. Slipping and tripping: Fall injuries in adults associated with rugs and carpets. J Inj Violence Res. 2013;5:61–9. doi: 10.5249/jivr.v5i1.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Washington, DC: National Academy Press; 1990. MC NevittFalls in older persons: Risk factors and prevention Berg R, Cassells JS (Eds.), The second fifty years: promoting health and preventing disability; pp. 263–89. [PubMed] [Google Scholar]
- 13.Morse JM, Morse RM, Tylko SJ. Developmalet of a scale to identify the fall-prone patient. Can J Aging. 1989;8:366–77. [Google Scholar]
- 14.Calys M, Gagnon K, Jernigan S. A validation study of the Missouri alliance for home care fall risk assessment tool. Home Health Care Management Pract. 2013;25:39–44. [Google Scholar]
- 15.Geneva: WHO; 2011. World Health Organization. Management of substance abuse, process of translation and adaptation of instruments. [Google Scholar]
- 16.Yoshida-Intern S. Geneva: WHO; 2007. A Global Report on Falls Prevention Epidemiology of Falls. [Google Scholar]
- 17.Armonk, NY, USA: IBM Corp; 2011. IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. [Google Scholar]
- 18.Brito TA, Coqueiro Rda S, Fernandes MH, de Jesus CS. Determinants of falls in community-dwelling elderly: Hierarchical analysis. Public Health Nurs. 2014;31:290–7. doi: 10.1111/phn.12126. [DOI] [PubMed] [Google Scholar]
- 19.Mizukami S, Arima K, Abe Y, Kanagae M, Kusano Y, Niino N, et al. Falls are associated with stroke, arthritis and multiple medications among community-dwelling elderly persons in Japan. Tohoku J Exp Med. 2013;231:299–303. doi: 10.1620/tjem.231.299. [DOI] [PubMed] [Google Scholar]
- 20.Mane AB, Sanjana T, Patil PR, Sriniwas T. Prevalence and correlates of fear of falling among elderly population in urban area of Karnataka, India. J Midlife Health. 2014;5:150–5. doi: 10.4103/0976-7800.141224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bergen G, Stevens MR, Burns ER. Falls and fall injuries among adults aged≥65 years-United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65:993–8. doi: 10.15585/mmwr.mm6537a2. [DOI] [PubMed] [Google Scholar]
- 22.Al-Nozha MM, Al-Hazzaa HM, Arafah MR, Al-Khadra A, Al-Mazrou YY, Al-Maatouq MA, et al. Prevalence of physical activity and inactivity among Saudis aged 30-70 years. A population-based cross-sectional study. Saudi Med J. 2007;28:559–68. [PubMed] [Google Scholar]
- 23.Stevenson B, Mills EM, Welin L, Beal KG. Falls risk factors in an acute-care setting: A retrospective study. Can J Nurs Res. 1998;30:97–111. [PubMed] [Google Scholar]
- 24.Philip SA, Sengupta P, Benjamin AI. Prevalence of falls and fall risk assessment in an urban elderly population of Ludhiana. Indian J Gerontol. 2015;29:187–97. [Google Scholar]
- 25.Lim YM, Sung MH. Home environmental and health-related factors among home fallers and recurrent fallers in community dwelling older Korean women. Int J Nurs Pract. 2012;18:481–8. doi: 10.1111/j.1440-172X.2012.02060.x. [DOI] [PubMed] [Google Scholar]
- 26.Sibley KM, Voth J, Munce SE, Straus SE, Jaglal SB. Chronic disease and falls in community-dwelling Canadians over 65 years old: A population-based study exploring associations with number and pattern of chronic conditions. BMC Geriatr. 2014;14:22. doi: 10.1186/1471-2318-14-22. [DOI] [PMC free article] [PubMed] [Google Scholar]