

Abstract
Objectives:
The aim of the present prospective study is to determine the effect of an intellectual colored game (ICG) on the severity of gag reflex (GR) and anxiety in children during dental alginate impression.
Materials and Methods:
Forty-one children, aging between 5 and 11 years, having a GR varying from normal to moderate had upper alginate impressions. The children's anxiety was evaluated with a facial image scale (FIS) before (T0) and after first failed impression (T1), then, after playing an intellectual colored game (ICG) at T2, while taking an upper alginate impression.
Results:
42.9 % of the children had a gag reflex of stage 2 and 31.0 % a facial scale of 3. Initial GR was not significantly associated with the final success of the impression (P =0.260) whereas final impression success was strongly associated with FIS (P <0.001). There was a statistically significant reduction in median GR score from T0 to T2 (P < 0.001) and FIS dropped significantly at T2 with ICG (P < 0.001).
Conclusion:
This study highlights the clinical performance of the intellectual distraction approach in GR management
KEYWORDS: Anxiety, behavioral management, children, distraction, gag reflex
INTRODUCTION
The gag reflex (GR) is an innate healthy defense mechanism that helps prevent foreign bodies from entering the trachea.[1] Psychological, anatomic, iatrogenic, local and systemic factors influence the GR.[2] The pharyngeal reflex that prevents choking involves five triggering zones in the oral cavity: the palatoglossal and palatopharyngeal folds, the postpharyngeal wall, the uvula, the palate, and the base of the tongue.[2,3] Stimulation of these zones generates afferent impulses to the medulla oblongata leading to efferent impulses that create the spasmodic and uncoordinated movements of gagging.[1] Psychological factors such as fear and anxiety, which cause approximately 20% of patients to avoid dental treatments, have also been implicated in gagging.[3] Decreasing the rate of dental avoidance in children is essential if we are to improve overall dental care.[4] Relaxation, desensitization, and distraction have been suggested for anxiety management in children.[5,6,7] Peripherally and centrally acting drugs have been used for the management of the GR.[8] Gagging can also be decreased in direct proportion to the reduction of awareness of the stimulus. For example, intraoral procedures can be accomplished successfully while the patient is distracted by audiovisual or intellectual games.
The aim of this pilot study is to determine the effect of mental distraction using the intellectual colored game (ICG) on the severity of GR and anxiety in children during dental impression.
MATERIALS AND METHODS
In this prospective pilot study, 41 children (20 boys and 21 girls) aged between 5 and 11 years, needing upper alginate impressions for space loss management, were recruited from a pediatric dentistry center in Beirut. The procedure was explained to the parents, and written informed consent was obtained, as well as the approval of the scientific board and the ethical committee.
Inclusion criteria included children with no special needs. The assessment of GR was performed in a calm environment by one pediatric dentist having >10 years of experience.
The patient was with the unknown history of GR for the practitioner.
The GR grade was evaluated before the impression procedure using the classification of gagging problem index as proposed by Saita et al.:[3]
G1: Normal gagging but not desensitized (the child tolerates a basic periodontal examination with a probe)
G2: Mild gagging (the child does not tolerate the basic periodontal examination with a probe)
G3: Moderate gagging (the child does not tolerate molar region examination with a dental mirror)
G4: Severe gagging (the child does not tolerate anterior teeth examination with a dental mirror)
G5: Very severe gagging (the child does not tolerate momentary insertion of dental mirror).
All children presenting with a G4 or G5 GR were excluded from the study for advanced technical difficulties.
Children's baseline anxiety was evaluated according to the Buchanan's Facial Image Scale (FIS)[9] [Figure 1] before any impression attempt (point T0). The FIS consists of a row of five faces ranging from very happy to very unhappy, and subjects are asked to select the one that best reflects their state of mind. The upper impression was attempted with unflavored alginate (Tropicalgin Zhermack®, Italy) without playing the ICG invented for the study purpose, and which consists of counting different geometrical shapes and colors [Figure 2]. If a patient failed the first attempt to obtain an upper impression, the FIS was administered again (T1). A second impression was then obtained at T2 while the patient played the ICG. The psychological state was again assessed at T2 using FIS [Figure 1].
Figure 1.
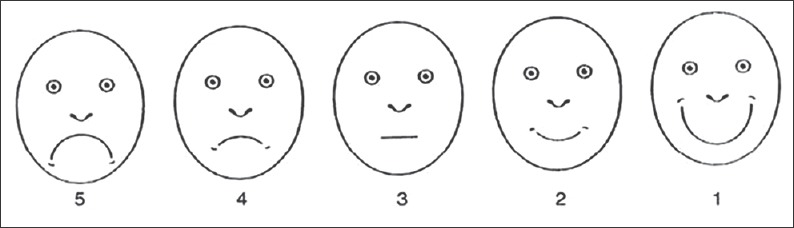
Buchanan Facial Image Scale with images scores from 1 to 5
Figure 2.
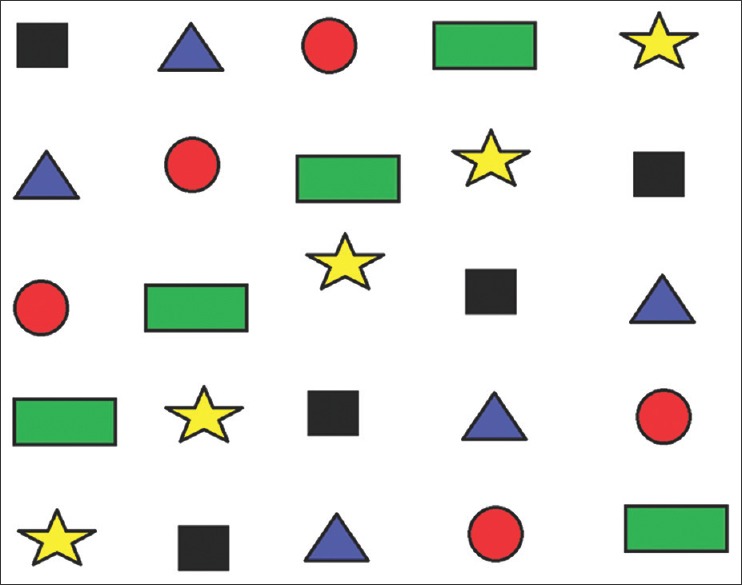
Chart of the intellectual colored game
STATISTICAL ANALYSIS
Frequencies were generated for the variables GR stage (T0 and T2), FIS (T0, T1 and T2), and impression success (T1 and T2). Descriptive statistics were also generated for the variables GR stage (T0 and T2) and FIS (T0, T1, and T2), considered as continuous variables. The variables GR stage and FIS were not normally distributed (Shapiro–Wilk's P < 0.05).
Fisher's exact test was used to test the association between baseline child characteristics (GR stage and FIS) and impression success with the ICG, and to test the association between FIS at T1 and T2 and impression success with the ICG. The Wilcoxon signed ranks test was used to assess the change in GR stage after the impression attempt with the ICG (T2 compared to T0). The Friedman test was used to compare FIS across the 3 time points (T0, T1, and T2). Kruskal–Wallis tests were used to compare the difference in FIS (T2-T1) across the different GR stages at T0 and T2.
The IBM® SPSS® statistics 20.0 (SPSS, Chicago, IL, USA)statistical package was used to carry out all statistical analyses. Statistical significance was set at 0.05.
RESULTS
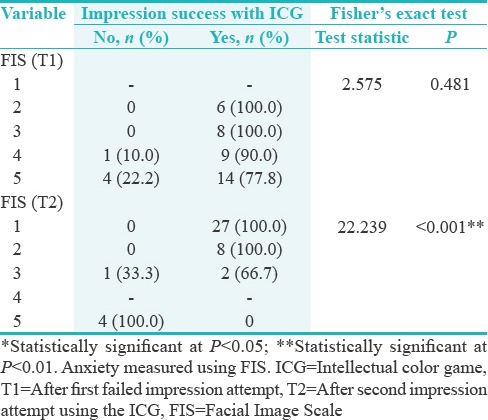
Before any impression taking, none of the children had a GR more severe than Stage 3 whereas 5 children (11.9%) had high anxiety as assessed by FIS scores of 5 [Table 1]. The majority had GR of Stage 2 severity (18; 42.9%) and a FIS of 3 (13; 31.0%). Initial GR was not significantly associated with the final success of the impression process with the ICG (P = 0.260) whereas initial facial scale did predict impression success (P = 0.039). FIS scores after the first failed impression attempt were not associated with final impression success with the ICG (P = 0.481), whereas final impression success was strongly associated with final FIS score (T2, P < 0.001) [Table 2].
Table 1.
Association between gag reflex severity and child reported anxiety at baselines with the ability to complete impression with the aid of the intellectual color game (n=42)
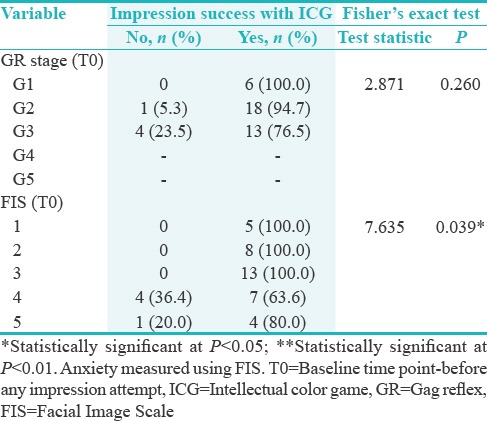
Table 2.
Association between child reported anxiety after impression attempts and the ability to complete impression with the aid of the intellectual color game (n=42)
PARAMETER CHANGES THROUGHOUT STUDY PERIOD
There was a statistically significant reduction in median GR score from T0 to T2 (P < 0.001) [Table 3]. There was a reduction in GR score for 29 children (69%) and no change for 13 children. None of the children experienced an increase in GR severity. FIS scores also exhibited an overall improvement between initial and final scores (P < 0.001) [Table 4]. Although median FIS score increased after the first failed impression attempt (from 3.0 to 4.0, P = 0.012), it dropped significantly after the final impression attempt with the ICG (median = 1.0, P < 0.001 compared to T0 and T1).
Table 3.
Change in gag reflex stage throughout the study period (n=42)

Table 4.
Change in child reported anxiety level throughout study period (n=42)

ASSOCIATION BETWEEN GAG REFLEX SEVERITY AND ANXIETY REDUCTION WITH INTELLECTUAL COLORED GAME
Initial GR severity was not significantly associated with the reduction in anxiety (T2-T1) as a result of the ICG (P = 0.758) [Table 5]. Final GR severity (T2), on the other hand, showed a statistically significant association with anxiety reduction as measured by the FIS [P = 0.010; Table 6]. Children with a final FIS score of G1 had the most reduction in FIS score (median reduction of 3.0 points) compared to those with a final score of G3 who had a median reduction of 0.0 (P = 0.010).
Table 5.
Association between baseline gag reflex severity and reduction in anxiety following the use of the intellectual color game (n=42)

Table 6.
Association between reduction in anxiety following the use of the intellectual color game and final gag reflex severity (n=42)

DISCUSSION
The GR is a subjective sensation that helps prevent foreign bodies from entering the mouth and pharynx.[1,10] Bassi et al. observed that there are two main categories of gagging patients based on somatogenic and psychogenic origins. However, it may be difficult to differentiate between them, as a physical stimulus may provoke gagging of psychogenic origin.[11] Exaggerated reflex during maxillary alginate impression may complicate the procedure, and in some cases, render impression taking impossible. Since the feeling or act of gagging can be embarrassing to children, knowledge regarding its management can play an important role in addressing patients’ psychological state.
This study aimed to explore a potential association between child-reported anxiety at (T0) and after impression attempts at T1 and T2, and the ability to complete alginate impression.
Dental fear is one of the most common phobias. It could be described in different intensities. Buchanan's FIS, used in the present study, is a simple and valid way to measure pediatric subjects’ anxiety state in a dental context.[9] At T0, children exhibited differences in anxiety strength varying from very happy (FIS 1) to very unhappy (FIS 5) [Figure 1 and Table 1]. Dental care-related fear, fear of pain, and negative beliefs about dental care could explain children's anxiety at baseline.
After the failed first alginate impression (T1), 14 out of 18 (77.8%) of children reported being very unhappy (FIS level 5) [Table 2], and the median FIS increased from 3 to 4 [Table 4]. This could be related to the child's fear of vomiting or choking. According to Gao et al. the prevalence of dental fear anxiety in children and adolescents ranges from 5% to 20%.[12] In fact, fearful children may try every possible means to avoid dental treatment such as alginate impressions.
At T2, the child was asked to concentrate on the ICG to divert his or her attention from the dental procedure. The counting of multiple colors and geometric shapes [Figure 2] seems to have avoided the discomfort of alginate impression. The present results are statistically significant (P < 0.001) when appraising facial scale throughout the study at T0, T1, and T2 [Table 4]. In fact, a considerable amelioration was noticed: 37 children had a FIS between 1 and 3 at T2 [Table 2]. This is consistent with Nuvvula's findings that audiovisual distraction is a key strategy for GR management.[13] Similarly, Richmond and Sato reported that the perception of pain is directly linked to the degree of attention a patient pays to the unpleasant stimulus.[14] Several studies suggest the importance of distraction in decreasing children's dental visit distress.[15,16] The ICG could, therefore, be considered a distraction technique useful for controlling dental fear and anxiety in pediatric patients.[17] The patient's attentiveness was diverted by the ICG chart, which played an important role in alginate impression success. The present findings are also consistent with the results by Al-Khotani et al. who demonstrated that audiovisual distraction can help decrease anxiety during dental procedures.[18] Similarly, Prabhakar et al. showed that audiovisual presentation and multi-sensory distraction helped in managing anxious children.[19]
THE SECOND PURPOSE WAS TO DETERMINE WHETHER GAG REFLEX SCORES AT T0 AND T2 WERE ASSOCIATED WITH THE SUCCESS OF THE IMPRESSIONS WHILE PLAYING WITH INTELLECTUAL COLORED GAME
Table 1 shows that baseline GR was not statistically significantly associated with the final success of the impression process while using the ICG (P = 0.260). An improvement in GR from T0 to T2 while playing the ICG was noticed [Table 3] (P = 0.001). The present findings showed that ICG could be considered an important element in reducing GR regardless of the reflex's state. Occasionally, dental gagging could not be considered as a sign of the child's anxiety, rather, the child's fear of choking.[2] The fact that children in this study experienced the first failed impression without any choking accident could have played a role in reducing their GR. However, the child's unwillingness to get the second alginate impression was overcome due to several reasons, including implementation of the ICG, a comfortable environment, appropriate selection of impression trays without alginate overloading, the use of fast setting unflavored alginate, and correct upright positioning of the patient.
On the other hand, many authors agree on the psychological factors involved in gagging.[20,21] In some cases, children may express their apprehension by an increased tendency to gag. This is considered a conscious self-defense against the invasion of the oral cavity.[22,23] Randall et al. suggested that a type of gagging during dental procedures could be a behavioral response determined by psychological variables.[4] Moreover, according to Armfield et al., GR is provoked by emotional factors that may be related to the child's past dental experiences.[24] Emotional gagging is thought to be due to the stimulation of the gag center located at the level of the diencephalon, limbic system, and sympathetic nervous system.[10,11]
THE THIRD TARGET WAS TO SHOW ANY ASSOCIATION BETWEEN GAG REFLEX AND FACIAL IMAGE SCALE THROUGHOUT THE STUDY AT T0, T1, AND T2
No statistically significant association was observed between GR severity at baseline and child's anxiety at T2 and T1 (P = 0.758) [Table 5]. These results could be explained by the presence of anatomic variations in the soft palate. Indeed, atypical anatomy; a relatively long soft palate; a larger angle between the hard and soft palates; an atonic or relaxed soft palate; and hypersensitivity of the soft palate, uvula, fauces, posterior pharyngeal wall, and tongue have been implicated.[25]
On the other hand, a statistically significant association between GR severity at (T2) and anxiety reduction using FIS was found (P = 0.010) [Table 6]. Accordingly, Randall et al. reported a direct correlation between levels of anxiety and frequency of gagging.[4]
Occasionally, psychological gagging can be induced without direct contact. Sight, sound, smell, or even the thought of dental treatment can be sufficient to induce the GR in some individuals.[26,27]
For the G3 group, touching a triggering area could have induced a higher gagging reflex than the G1 (P = 0.010) [Table 6]. Bassi et al. implicated vagal nerve sensitivity in GR development.[11] Psychogenic effect showed a greater amelioration in FIS due to the children's better cooperation in G1 group while playing ICG in the present study.
It would be difficult to make a clear-cut distinction between the general or local causes of GR and the psychological component. The dental practitioner's skills and patience are greatly responsible for controlling such a situation to carry out the respective treatment with satisfactory results for the patient.
Table 6 shows a statistically significant association between GR severity at (T2) and anxiety reduction. These results could highlight the role of ICG distraction in temporarily diverting the children's attention and allowing a fast alginate impression. In fact, the child's participation in ICG may help enhancing his or her self-confidence, possibly by increasing endorphin release. According to Donaldson, the serotonin 1A receptor (5-HT1A) plays a major role in modulating mood and behavior, and previous studies have shown that knocking out 5-HT1A selectively in the raphe leads to higher levels of anxiety in adulthood.[28] Behavioral issues in children are due to multiple elements such as immature reasoning and restricted skills to deal with anxiety. Singh et al. state that behavioral techniques are the most successful long-term methods in gagging management. It reduces anxiety and helps “unlearn” the behavior that provokes gagging.[21] In the present study, the ICG enhanced the child's compliance and gained his attention allowing a successful alginate impression by decreasing his GR and anxiety.
Finally, some factors limit our study and conclusions. They include the small sample size. Larger studies would yield more accurate results. In addition, our sample concerns only children, making the results not directly applicable to adults. Another limitation of our study is that we did not test other potentially more effective behavioral interventions.
CONCLUSION
Intellectual distraction is a safe, potentially effective, and cost-saving method of GR management in pediatric dentistry. The clinical effectiveness of the distraction approach is of significant interest since parents often prefer nonpharmacological interventions. The ICG diverted the child's attention during the stressful alginate impression and should be considered to further advance behavior management techniques.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Kumar S, Satheesh P, Savadi RC. Gagging. N Y State Dent J. 2011;77:22–7. [PubMed] [Google Scholar]
- 2.van Linden van den Heuvell GF, de Boer B, Ter Pelkwijk BJ, Bildt MM, Stegenga B. Gagging problem assessment: A re-evaluation. J Oral Rehabil. 2015;42:495–502. doi: 10.1111/joor.12280. [DOI] [PubMed] [Google Scholar]
- 3.Saita N, Fukuda K, Koukita Y, Ichinohe T, Yamashita S. Relationship between gagging severity and its management in dentistry. J Oral Rehabil. 2013;40:106–11. doi: 10.1111/joor.12014. [DOI] [PubMed] [Google Scholar]
- 4.Randall CL, Shulman GP, Crout RJ, McNeil DW. Gagging and its associations with dental care-related fear, fear of pain and beliefs about treatment. J Am Dent Assoc. 2014;145:452–8. doi: 10.14219/jada.2013.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gera A, Kaur G, Kalra T, Gupta N. Pharangeal reflex during orthodontic impressions: A problem and its solutions. Indian J Dent Sci. 2010;2:29–31. [Google Scholar]
- 6.Aartman IH, Van Everdingen TA, Hoogstraten J, Schuurs AH. Appraisal of behavioural measurement techniques for assessing dental anxiety and fear in children: A review. J Psychopathol Behav Assess. 1996;18:153–71. [Google Scholar]
- 7.Aartman IH, van Everdingen T, Hoogstraten J, Schuurs AH. Self-report measurements of dental anxiety and fear in children: A critical assessment. ASDC J Dent Child. 1998;65:252–8. 229-30. [PubMed] [Google Scholar]
- 8.Klingberg G. Dental anxiety and behavior management problems in paediatric dentistry: A review of background factors and diagnostics. Eur Arch Paediatr Dent. 2007;8:11–5. doi: 10.1007/BF03262650. [DOI] [PubMed] [Google Scholar]
- 9.Buchanan H, Niven N. Validation of a facial image scale to assess child dental anxiety. Int J Paediatr Dent. 2002;12:47–52. [PubMed] [Google Scholar]
- 10.Dickinson CM, Fiske J. A review of gagging problems in dentistry: I. Aetiology and classification. Dent Update. 2005;32:26–8. doi: 10.12968/denu.2005.32.1.26. 31-2. [DOI] [PubMed] [Google Scholar]
- 11.Bassi GS, Humphris GM, Longman LP. The etiology and management of gagging: A review of the literature. J Prosthet Dent. 2004;91:459–67. doi: 10.1016/S0022391304000939. [DOI] [PubMed] [Google Scholar]
- 12.Gao X, Hamzah SH, Yiu CK, McGrath C, King NM. Dental fear and anxiety in children and adolescents: Qualitative study using YouTube. J Med Internet Res. 2013;15:e29. doi: 10.2196/jmir.2290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nuvvula S, Alahari S, Kamatham R, Challa RR. Effect of audiovisual distraction with 3D video glasses on dental anxiety of children experiencing administration of local analgesia: A randomised clinical trial. Eur Arch Paediatr Dent. 2015;16:43–50. doi: 10.1007/s40368-014-0145-9. [DOI] [PubMed] [Google Scholar]
- 14.Richmond BJ, Sato T. Enhancement of inferior temporal neurons during visual discrimination. J Neurophysiol. 1987;58:1292–306. doi: 10.1152/jn.1987.58.6.1292. [DOI] [PubMed] [Google Scholar]
- 15.Davies AE, Kidd D, Stone SP, MacMahon J. Pharyngeal sensation and gag reflex in healthy subjects. Lancet. 1995;345:487–8. doi: 10.1016/s0140-6736(95)90584-7. [DOI] [PubMed] [Google Scholar]
- 16.Ram D, Shapira J, Holan G, Magora F, Cohen S, Davidovich E, et al. Audiovisual video eyeglass distraction during dental treatment in children. Quintessence Int. 2010;41:673–9. [PubMed] [Google Scholar]
- 17.Hamzah HS, Gao X, Yung Yiu CK, McGrath C, King NM. Managing dental fear and anxiety in pediatric patients: A qualitative study from the public's perspective. Pediatr Dent. 2014;36:29–33. [PubMed] [Google Scholar]
- 18.Al-Khotani A, Bello LA, Christidis N. Effects of audiovisual distraction on children's behaviour during dental treatment: A randomized controlled clinical trial. Acta Odontol Scand. 2016;74:494–501. doi: 10.1080/00016357.2016.1206211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Prabhakar AR, Marwah N, Raju OS. A comparison between audio and audiovisual distraction techniques in managing anxious pediatric dental patients. J Indian Soc Pedod Prev Dent. 2007;25:177–82. doi: 10.4103/0970-4388.37014. [DOI] [PubMed] [Google Scholar]
- 20.Sakamoto T, Fukuda K, Saita N, Koukita Y, Yamashita S, Koizumi J, et al. Autonomic nervous activity of patients with gagging problems during dental mirror insertion. Spec Care Dentist. 2016;36:80–4. doi: 10.1111/scd.12148. [DOI] [PubMed] [Google Scholar]
- 21.Singh S, Ali FM, Nazirkar G, Dole VK, Gaikwad B. Gag-etiology and its skillful management – A review. J Evol Med Dent Sci. 2013;2:1509–16. [Google Scholar]
- 22.Madan K, Baliga S, Thosar N, Rathi N. Recent advances in dental radiography for pediatric patients: A review. J Med Radiol Pathol Surg. 2015;1:21–5. [Google Scholar]
- 23.Londono J, Abreu A, Baker PS, Furness AR. Fabrication of a definitive obturator from a 3D cast with a chairside digital scanner for a patient with severe gag reflex: A clinical report. J Prosthet Dent. 2015;114:735–8. doi: 10.1016/j.prosdent.2015.01.019. [DOI] [PubMed] [Google Scholar]
- 24.Armfield JM, Spencer AJ, Stewart JF. Dental fear in Australia: Who's afraid of the dentist? Aust Dent J. 2006;51:78–85. doi: 10.1111/j.1834-7819.2006.tb00405.x. [DOI] [PubMed] [Google Scholar]
- 25.Conny DJ, Tedesco LA. The gagging problem in prosthodontic treatment. Part II: Patient management. J Prosthet Dent. 1983;49:757–61. doi: 10.1016/0022-3913(83)90343-8. [DOI] [PubMed] [Google Scholar]
- 26.Miles TS, Nauntofte B, Svenson P. Copenhagen: Quintessence Publishing Co., Ltd.; 2004. Clinical Oral Physiology; pp. 245–54. [Google Scholar]
- 27.Yfanti K, Kitraki E, Emmanouil D, Pandis N, Papagiannoulis L. Psychometric and biohormonal indices of dental anxiety in children. A prospective cohort study. Stress. 2014;17:296–304. doi: 10.3109/10253890.2014.918602. [DOI] [PubMed] [Google Scholar]
- 28.Donaldson ZR, Piel DA, Santos TL, Richardson-Jones J, Leonardo ED, Beck SG, et al. Developmental effects of serotonin 1A autoreceptors on anxiety and social behavior. Neuropsychopharmacology. 2014;39:291–302. doi: 10.1038/npp.2013.185. [DOI] [PMC free article] [PubMed] [Google Scholar]