

Abstract
Aims and Objectives:
Many situations in the dental office can provoke medical emergencies. Lack of training and inability to overcome the medical emergencies can lead to serious consequences and legal actions. The aim of the study is to investigate and assess the knowledge, attitude, and perceived confidence of dental students and interns in the management of medical emergency.
Materials and Methods:
A self-administered structured questionnaire was distributed to 153 of the undergraduate dental students and interns in Qassim province. Questionnaire consisted of nineteen questions pertaining to knowledge and awareness regarding syncope, cardiopulmonary resuscitation (CPR), intravenous drugs, measuring vital signs, and handling situation of aspiration of a foreign body, bleeding, and choking. Data were analyzed by Statistical Package for Social Sciences (SPSS) version 21.0.
Results:
Fifty-seven percent was the response rate received from the questionnaire. Eighty-nine percent and 30% of the participants inquired about the medical history and vital signs before dental treatment, respectively. Only 37% of participants were confident to handle any medical emergency in the dental office. Seventy percent knew the correct location of chest compression and 67% were familiar about the right compression ventilation ratio showing significant difference between academic years and interns (P = 0.003). Females were significantly more aware about the management of bleeding after extraction than the males (65%, and 47%, respectively; P = 0.035). Thirty-five percent and 53% chose the correct management to relieve choking in responsive and unresponsive adult or child, respectively. A total of 28% of the participants reported syncope as the most common emergency situation.
Conclusion:
Participants were lacking confidence in handling medical emergencies even though the majority of them inquired the medical history. Most of them have a good knowledge regarding CPR, but regarding airway obstruction, the knowledge was not at an acceptable level. Annual basic life support and emergency courses should be mandatory in dental teaching curriculum.
KEYWORDS: Angina, cardiopulmonary resuscitation, choking, dental students, emergency, obstruction, syncope
INTRODUCTION
Many situations in the dental office can provoke medical emergencies. The frequent administration of local anesthetics and other drugs, dental materials, the dental care of medically compromised patients, and the fear of surgical operations in many patients are frequent causes of emergency situations such as syncope, hyperventilation, and cardiac arrest.[1] Most of the dentists did not follow stress reduction protocol while treating their patients. It is reported that three-quarters of all medical emergencies develop because dentists often fail to recognize patient's anxiety.[2] Hence, it is imperative to follow stress reduction protocol in the dental office.[3] One of the method is to schedule the patients in morning with appointments of shorter duration. This can be achieved by scheduling the patients for short morning appointment.[4,5]
A medical history of the patient is helpful in preventing or minimizing medical emergencies in the dental office. The information is helpful during the patient examination and formulating comprehensive treatment plan with suitable alternatives in the dental treatment plan.[6,7] However, despite efforts to minimize any untoward incidence, emergency situations may arise on the dental chair.[8]
Lack of training and inability to manage the medical emergencies can lead to serious consequences and legal actions.[9] Therefore, dental students must have appropriate knowledge of potential interactions with medical conditions and the ability to diagnose medical problems. The fundamental principles of emergency conditions and a consideration of the management must be objects of the dental education and training. The aim of this study is to investigate and assess the knowledge, attitude, and perceived confidence of dental students and interns in the management of medical emergency.
MATERIALS AND METHODS
A cross-sectional study was performed at three dental schools in Qassim Province; Qassim University, Qassim Private Colleges, and Buraydah Private Colleges. The study was conducted during the academic year in March 2017 among both female and male dental students and interns.
The study received the approval of the dental ethics committee; process code: EA/202/2017, and the approval of scientific research and presentation skills supervision committee; code: F-5002-17. After the approval, the directors of the dental universities were informed about the aim of this research; then, they authorized the study. A self-administered questionnaire was administered among dental students and interns. The questionnaire was pretested to check its validity. Questionnaire consisted of two parts; the first contained general information about the demographic data including age, gender, level of education, and the name of the university. The second part contained seventeen questions pertaining to knowledge, attitude, and perceived confidence of dental students in handling medical emergencies in the dental clinic. Their knowledge and awareness regarding the management of syncope and their confidence in administering cardiopulmonary resuscitation (CPR), drugs, measuring vital signs, and handling situation of aspiration of a foreign body, bleeding, or choking were also assessed.
A total of 153 questionnaires (76 female and 77 male) were completed and returned by participants. The inclusion criteria were students in their clinical practice years or interns and agreement to participate in the research. Questionnaires that were filled by doctors or students who were not in their clinical courses were excluded.
The data was entered into Statistical Package for Social Sciences (SPSS) version 21 (IBM Corp., Armonk, N.Y., USA). 0 and were utilized for data analysis. The data were analyzed for frequency distributions. The Chi-square test was used for comparisons among male and female students. The significance level (P value) was set at 0.05.
RESULTS
Out of 350 questionnaires that were distributed among dental students in their clinical practice years (3rd, 4th, and 5th year) and dental interns. Two hundred and one questionnaires were received, and the response rate was 57%. The number of valid cases for analysis was 153 (76 female and 77 male). Valid cases were those who answered the questionnaire completely. The questionnaires that were incompletely filled were excluded from the final analysis. The respondents’ age range was between 20 and 30 years with the mean age of 23 years.
Eighty-nine percent of the participants inquired about the medical history including medications and allergy history before dental treatment [Table 1]. Among these participants, 29.4% of them obtained vital signs before commencing any treatment, while 20.3% did not. Moreover, 50.3% obtained the vital signs when the patient's condition requires. Only 37% of participants were actually very confident to handle any medical emergency in the dental office. Almost 60% of the participants know about the availability of emergency kits in their dental office showing a significant difference between female and male participants (50% and 69%, respectively; P = 0.021).
Table 1.
Response rate of the participants on different parameters evaluated
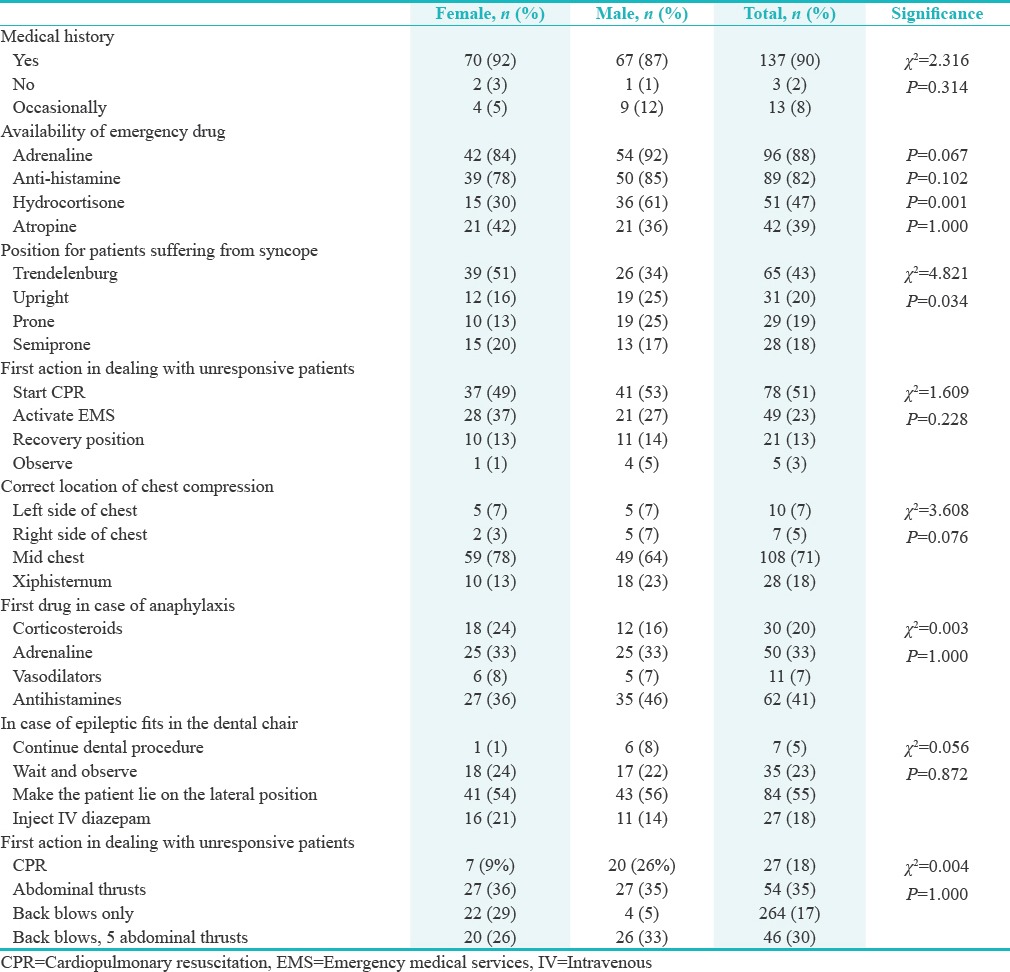
Regarding the availability of emergency drugs, adrenaline followed by antihistamine were the most available drugs (88% and 82, respectively) [Table 1]. Fifty-one percent of the female and 34% of male participants knew the correct position for patients suffering from syncope with a significant difference between the two genders (P = 0.034). On the participant's knowledge regarding aspiration of foreign body, 24% were aware about the management of airway obstruction showing significant difference between 3rd, 4th, 5th year, and interns (6%, 25%, 30%, and 59% respectively; P = 0.000) [Table 2].
Table 2.
Response rate of the participants (based on the academic level) on different parameters evaluated
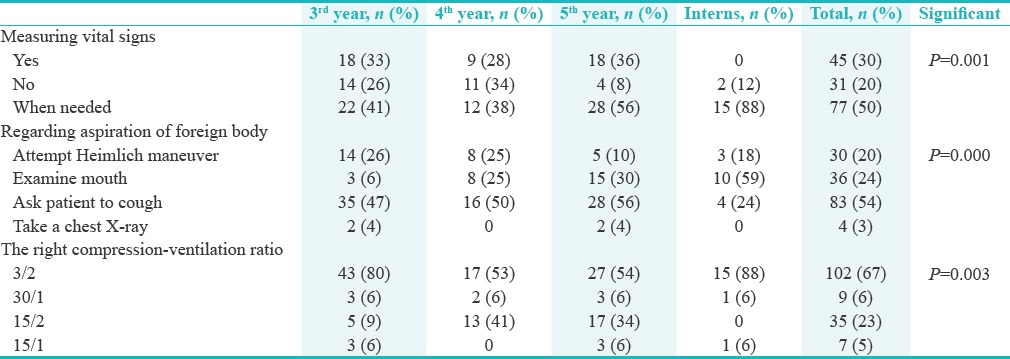
Regarding the knowledge about the first action in dealing with unresponsive patients, 32% of the participants chose to activate emergency medical services (EMS) first. The majority of participants (71%) knew the correct location of chest compression showing similar percentage between female and male participants (77.6% and 64%, respectively) [Table 1]. A total of 67% of the participants were familiar about the right compression-ventilation ratio that should be given in CPR in case of a single rescuer, showing significant difference between 3rd, 4th, 5th year, and interns (80%, 53%, 54%, and 88%, respectively; P = 0.003) [Table 2]. Female participants were significantly more aware about the primary management of spontaneous bleeding after extraction than the male participants (65% and 47%, respectively; P = 0.035). Forty percent of the participants chose antihistamine as the first drug in case of anaphylaxis, while only 33% chose adrenaline as the first drug of choice [Table 1]. The knowledge about the primary management in case of epileptic fits in the dental chair was similar between female and male participants (54% and 56%, respectively).
Sublingual nitrates were the most chosen answer regarding the management of patient suffering from angina pain, showing significant difference between the academic years (46% of third, 60% of forth, 56% of 5th year, and 94% of the interns; P = 0.007). Only 35% chose to perform abdominal thrusts (also known as the Heimlich maneuver) to relieve choking in responsive adult or child. Moreover, regarding choking in unresponsive adult or child, a total of 53% chose CPR as the first management with a significant difference between female and male participants (62% and 44%, respectively; P = 0.035). When we asked the participant about the emergency situation that was faced during their practice, 28% of the participants reported syncope as the most common emergency situation; others reported hemorrhage, hyperglycemia, and seizures.
DISCUSSION
Although the occurrence of life-threatening emergencies in dental offices is infrequent, many factors can increase the likelihood of such incidents. These include (1) the increasing number of older persons seeking dental care, (2) therapeutic advances in the medical and pharmaceutical professions, (3) the growing trend toward longer dental appointments, and (4) the increasing use and administration of drugs in dentistry.[10] The results of a postal questionnaire undertaken in Australia reported that 1 in 7 out of the 1250 general dental practitioners had to perform resuscitation.[11] A similar study done in Great Britain over a period of 10 years found that an emergency event was reported, on average, for every 4.5 practice years in England and Wales and 3.6 years in Scotland. The study also found that there were 1.9 cases of syncope reported per dentist per year.[12] Completed questionnaire received from 199 dental practitioners in New Zealand showed that 65% respondents had experienced at least one medical emergency in their practice in the last 10 years.[13]
All attempts must be made to prevent the occurrence of a medical emergency, and this prevention begins as soon as the patient is asked about his/her medical history.[14] According to the present study, higher number of the participants (89.5%) recorded the medical history of their patients, including medications and allergy before dental treatment, showing a significant difference between the academic years. As per the protocol, all dentists need to record the medical history as it may help them to recognize the possible complication/s and modify the treatment plan when required.[14,15]
Obtaining vital signs provide a baseline measurement from which alterations in the patient's condition can be determined. This is a practice not frequently seen in all dental offices. Vital signs including blood pressure, pulse, respiratory rate, and temperature should be measured before each treatment.[16] In our study, 29.4% of the participants mentioned that obtaining vital signs before commencing any treatment, while 20.3% of them did not. Moreover, the majority of them (50.3%) believed that the vital signs are important when the patient's condition requires such as hypertension, diabetes, asthma, and heart diseases in general. In addition, some of them reported that the need to obtain the vital signs depends on the procedure to be done such as scaling, extraction, and oral surgeries.
The knowledge about the availability of emergency drugs is mandate. It seems prudent to prepare an emergency drug kit consisting of drugs, which are considered to be essential. The guidelines differ in recommended drug and equipments.[17] We found that respondents in our study had a good knowledge in the availability of adrenaline followed by antihistamine (88.1% and 81.7%, respectively). The knowledge was not at an acceptable level, particularly with drugs such as hydrocortisone and atropine (46.8% and 3.5%, respectively).
Every dental practitioner must be able to diagnose and treat common emergent problems such as syncope. The basic principles of emergency situations and a consideration of the management must be objects of the dental education.[18] In our study, 51.3% of females and 33.8% of male participants knew the correct position for patients suffering from syncope with a significant difference between the two genders. Many reports describe accidental ingestion or aspiration of dental instruments, restorations, and prosthesis during dental treatment.[19] Twenty-three percent of the participants were aware about the management of airway obstruction by examining the mouth and local area to locate and remove any object that might cause acute upper airway obstruction, which showed a significant difference between 3rd, 4th, 5th year, and interns.
Optimizing EMS dispatch is likely to be one of the most cost-effective solutions to improving outcomes from cardiac arrest, as recommended by both Saudi and American heart associations. Only 32% of the participants chose to activate EMS as their immediate action. Saudi heart association recommendation regarding chest compression in CPR is to place the hand in on the lower half of the sternum, place the heels of the hand 2–3 fingers above the xiphisternal angel, and also placing the hands below an imaginary line between the two nipples.[20] Seventy percent of the participants have chosen midchest as the right location for chest compression with similar percentage between females and males participants. Compression ventilation ratio is the number of compression per rescue breath and vice versa. As recommended by both Saudi Heart Association and American Heart Association, the single rescuer should begin CPR with 30 chest compressions followed by two breaths.[21,22] Although 66.7% of the participants knew the correct compression-ventilation ratio, a significant difference between the academic years has been recorded giving a higher prevalence among interns then followed by 3rd, 5th, and 4th year.
Postoperative bleeding is a common complication in oral surgery and may occur during a simple tooth extraction or during any other surgical procedure. The primary management of bleeding is compression, which aims at causing vasoconstriction and decreasing the permeability of the capillaries, and is achieved by placing gauze over the bleeding site with pressure. Placing pressure by biting on gauze for 10–30 min over the postextraction wound or other superficial bleeding areas is usually sufficient.[23] Only 55.6% of the participants had the knowledge about the primary management of spontaneous bleeding after extraction.
Anaphylaxis requires immediate medical attention including administration of epinephrine. When symptoms of anaphylaxis do not resolve with an initial dose of epinephrine, and EMS arrival will exceed 5–10 min, a second dose of epinephrine may be considered.[24] Forty percent of the participants chose antihistamine as the first drug in case of anaphylaxis, while only 32.7% chose adrenaline as the first drug of choice.
Epilepsy is a disease that involves seizures, which are characterized by an alteration of perception, behavior, and mental activities, as well as by involuntary muscle contractions, temporary loss of consciousness, and chronic changes in neurological functions that result from abnormal electrical activity in the brain.[20] If a seizure occurs while a patient is in the dental chair, a dentist should be able to manage the situation by knowing the primary steps including discontinuing the procedure immediately and placing the patient on his/her side to decrease the chance of aspiration of secretions or dental materials in the patient's mouth.[25] In our study, the knowledge about the primary management in case of epileptic fits in the dental chair was similar between female and male participants (53.9% and 55.8%, respectively).
Regarding the management of angina during dental procedures, the result of this study shows that 57.5% of the dental students know the primary drug of choice for angina which is relatively higher than an earlier study.[26] Although angina are rare during dental treatment, there is always a possibility. Hence, it is important for the dental practitioners to have sufficient knowledge on handling such situations if they arise. Choking (upper airway obstruction) occurs when a foreign object becomes lodged in the throat or windpipe, blocking the flow of air. Choking relieve depends on the consciousness of the patient, to relieve choking in responsive adult or child and perform abdominal thrusts repeatedly (Heimlich maneuver). In our study, 35.3% and 52.9% of the participants chose the correct management to relieve choking in responsive and unresponsive adult or child, respectively.
In the United States and Canada, studies have also shown that syncope is the most common medical emergency seen by dentists.[13,27] Syncope represented approximately 50% of all emergencies reported in one particular study, with the next most common event, mild allergy, represented only 8% of all emergencies.[28]
CONCLUSION
The observations of the survey showed that most of the participants were lacking confidence in handling medical emergencies even though the majority of them inquired the medical history including medications and allergy before dental treatment. Furthermore, although syncope was the most reported medical emergency, less than half of the participants had the knowledge regarding the correct management. The study showed that there is finding dearth of knowledge among the dental students and interns in dealing medical emergencies. Annual basic life support and emergency courses should be made mandatory in dental teaching curriculum, and further hands-on training is required to update their knowledge to enhance their capability to recognize and manage a medical emergency and to become well-qualified practitioners.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Mohan M, Sharma H, Parolia A, Barua A. Knowledge, attitude and perceived confidence in handling medical emergencies among dental practitioners in Dakshina Kannada, India. Oral Health Dent Manag. 2015;14:27–31. [Google Scholar]
- 2.Malamed SF. Knowing your patients. J Am Dent Assoc. 2010;141(Suppl 1):3S–7S. doi: 10.14219/jada.archive.2010.0350. [DOI] [PubMed] [Google Scholar]
- 3.Yoo JH, Choi BH, Hong SJ, Nam W, Kim JB, Yoon JH. Stress reduction protocol for proper extraction of advanced infected teeth in medically compromised patients: Review of literature and report of cases. J Korean Assoc Oral Maxillofac Surg. 2000;26:85–92. [Google Scholar]
- 4.Shuman SK. A physician's guide to coordinating oral health and primary care. Geriatrics. 1990;45:47–51. 54, 57. [PubMed] [Google Scholar]
- 5.Fehrenbach MJ. Stress Reduction for the Oral Health Care Patient at High Risk for Medical Emergency. Access (ADHA) 2004 Jul [Google Scholar]
- 6.Southerland JH, Gill DG, Gangula PR, Halpern LR, Cardona CY, Mouton CP, et al. Dental management in patients with hypertension: Challenges and solutions. Clin Cosmet Investig Dent. 2016;8:111–20. doi: 10.2147/CCIDE.S99446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pedigo RA. Dental emergencies: Management strategies that improve outcomes. Emerg Med Pract. 2017;19:1–24. [PubMed] [Google Scholar]
- 8.Greenwood M, Meechan JG. General medicine and surgery for dental practitioners: Part 3. Management of specific medical emergencies in dental practice. Br Dent J. 2014;217:21–6. doi: 10.1038/sj.bdj.2014.549. [DOI] [PubMed] [Google Scholar]
- 9.Wood I. Medical emergencies and complications in the practice. Prim Dent J. 2014;3:6. doi: 10.1308/205016814812135896. [DOI] [PubMed] [Google Scholar]
- 10.Stafuzza TC, Carrara CF, Oliveira FV, Santos CF, Oliveira TM. Evaluation of the dentists knowledge on medical urgency and emergency. Braz Oral Res. 2014;28 doi: 10.1590/10.1590/1807-3107bor-2014.vol28.0029. pii: S1806-83242014000100240. [DOI] [PubMed] [Google Scholar]
- 11.Chapman PJ. Medical emergencies in dental practice and choice of emergency drugs and equipment: A survey of Australian dentists. Aust Dent J. 1997;42:103–8. doi: 10.1111/j.1834-7819.1997.tb00104.x. [DOI] [PubMed] [Google Scholar]
- 12.Atherton GJ, McCaul JA, Williams SA. Medical emergencies in general dental practice in great britain. Part 1: Their prevalence over a 10-year period. Br Dent J. 1999;186:72–9. doi: 10.1038/sj.bdj.4800023. [DOI] [PubMed] [Google Scholar]
- 13.Broadbent JM, Thomson WM. The readiness of New Zealand general dental practitioners for medical emergencies. N Z Dent J. 2001;97:82–6. [PubMed] [Google Scholar]
- 14.Rosenberg M. Preparing for medical emergencies: The essential drugs and equipment for the dental office. J Am Dent Assoc. 2010;141(Suppl 1):14S–9S. doi: 10.14219/jada.archive.2010.0351. [DOI] [PubMed] [Google Scholar]
- 15.Haas DA. Preparing dental office staff members for emergencies: Developing a basic action plan. J Am Dent Assoc. 2010;141(Suppl 1):8S–13S. doi: 10.14219/jada.archive.2010.0352. [DOI] [PubMed] [Google Scholar]
- 16.Kalladka M, Greenberg BL, Padmashree SM, Venkateshaiah NT, Yalsangi S, Raghunandan BN, et al. Screening for coronary heart disease and diabetes risk in a dental setting. Int J Public Health. 2014;59:485–92. doi: 10.1007/s00038-013-0530-x. [DOI] [PubMed] [Google Scholar]
- 17.Jodalli PS, Ankola AV. Evaluation of knowledge, experience and perceptions about medical emergencies amongst dental graduates (Interns) of belgaum city, india. J Clin Exp Dent. 2012;4:e14–8. doi: 10.4317/jced.50627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Stoeva I. The assess of dental studentsknowledge and skills in management of medical emergencies in dental officeStoeva I. Journal of IMAB. 2011;17:132–33. [Google Scholar]
- 19.Parolia A, Kamath M, Kundubala M, Manuel TS, Mohan M. Management of foreign body aspiration or ingestion in dentistry. Kathmandu Univ Med J (KUMJ) 2009;7:165–71. doi: 10.3126/kumj.v7i2.2715. [DOI] [PubMed] [Google Scholar]
- 20.Elbarbary M. International guidelines: Adoption or adaptation by the Saudi Heart Association? J Saudi Heart Assoc. 2009;21:181–6. doi: 10.1016/j.jsha.2009.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dabrowska A, Telec W. New guidelines of basic and advanced cardiopulmonary resuscitation and emergency cardiovascular care (ECC) American Heart Association (AHA) Wiad Lek. 2011;64:127–31. [PubMed] [Google Scholar]
- 22.Ewy GA. Cardiocerebral and cardiopulmonary resuscitation – 2017 update. Acute Med Surg. 2017;4:227–34. doi: 10.1002/ams2.281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.McCormick NJ, Moore UJ, Meechan JG. Haemostasis. Part 1: The management of post-extraction haemorrhage. Dent Update. 2014;41:290–2. doi: 10.12968/denu.2014.41.4.290. 294-6. [DOI] [PubMed] [Google Scholar]
- 24.Maher NG, de Looze J, Hoffman GR. Anaphylaxis: An update for dental practitioners. Aust Dent J. 2014;59:142–8. doi: 10.1111/adj.12161. [DOI] [PubMed] [Google Scholar]
- 25.Mehmet Y, Senem Ö, Sülün T, Hümeyra K. Management of epileptic patients in dentistry. Surg Sci. 2012;3:47. [Google Scholar]
- 26.Elanchezhiyan S, Elavarasu S, Vennila K, Renukadevi R, Mahabob MN, Sentilkumar B, et al. Awareness of dental office medical emergencies among dental interns in Southern India: An analytical study. J Dent Educ. 2013;77:364–9. [PubMed] [Google Scholar]
- 27.Fast TB, Martin MD, Ellis TM. Emergency preparedness: A survey of dental practitioners. J Am Dent Assoc. 1986;112:499–501. doi: 10.14219/jada.archive.1986.0043. [DOI] [PubMed] [Google Scholar]
- 28.Haas DA. Management of medical emergencies in the dental office: Conditions in each country, the extent of treatment by the dentist. Anesth Prog. 2006;53:20–4. doi: 10.2344/0003-3006(2006)53[20:MOMEIT]2.0.CO;2. [DOI] [PMC free article] [PubMed] [Google Scholar]