

Abstract
Background
The social determinants of health have a disproportionate impact on mortality in men. A study into the state of health of the male population in Leeds was undertaken to guide public health commissioning decisions. This paper reports on the data relating to the social lives of men.
Methods
A cross-sectional study was undertaken, comprising descriptive analysis of data relating to educational attainment, housing, employment (including benefit claimants), marital status and relationships. Data was considered for the whole city and localised at the Middle Super Output Area (MSOA) level and mapped against the Index of Deprivation.
Results
Boys’ educational attainment was found to be lagging behind girls’ from their earliest assessments (Early Years Foundation Stage Profile, 46% vs. 60%, P = 0.00) to GCSEs (53% vs. 63%, P = 0.00), leaving many men with no qualifications. There were 68% more men than women identified as being unemployed, with more men claiming benefits. Men living in social housing are more likely to be housed in high-rise flats. Almost 50% of men aged 16–64 are single, with 2254 lone fathers.
Conclusions
There appears to be a lack of sex/gender analysis of current cross city data. In areas of deprivation a complex picture of multiple social problems emerges, with marked gender differences in the social determinants of health, with males seeming to be more negatively affected. There is a need for more focused planning for reaching out and targeting boys and men in the most deprived inner city areas, so that greater efficiency in service delivery can be obtained.
Keywords: Men’s health, Social determinants, Education, Housing, Employment, Relationships
Background
There is a growing recognition that the health of the male population is heavily affected by their social situation, with increasing poverty linked to a widening gap in life expectancy [1, 2]. This is a global phenomenon, with such differences reported across the European Union [3], Asia [4], Australia [5], and within countries such as Ireland [6], Denmark [7], and Germany [8]. This study explores the social situation of men within a substantial metropolitan city in the UK, however the findings should have a resonance with men in other large conurbations.
The opportunities for improving public health through local action has been recognised [9, 10] and with an increasing agenda for targeting activity within the most challenging areas. Leeds is the third largest city in the United Kingdom; since 2010, there has been a 47% reduction in the money that Leeds City Council gets from Government to run local services. To ensure tendered contracts are fit for purpose, Leeds Council’s Joint Strategic Needs Assessment [11] noted that there was a dearth of information on the 400,000 male population across the city. This acted as a stimulant to instigate a study into the State of Men’s Health in Leeds, to act as a guide to future public health planning.
The findings of that study [12–14] highlighted that there were large differences in both morbidity and mortality for men across different areas of Leeds, suggesting that the health challenges the men were facing were more than a biological issue specific to being male.
There is strong evidence across a wide range of studies and reports on the impact of the wider determinants of health on a population’s wellbeing [15–21]. What has been less well-researched is how being sex is affected by these social factors [22–30]. There has been a sustained campaign for the disaggregation of data by sex in both research and routinely collected data within public health [3, 31–35], with the recent report on women’s health in Europe calling for improved availability and use of sex-disaggregated data that can be cross-linked to social factors [36]. With the push for gender mainstreaming [37] and also the legal requirements for gender to be recognised as a protected group within health policy strategy and service provision [38] the need for such scrutiny is further supported.
Through the more detailed examination of how sex maps onto intersectional factors (such as age, ethnicity, disabilities and sexuality) and the wider social determinants of health a more efficient targeting of resources may be achieved. By making more explicit how social and environmental factors differentially impact on both men and women we can help guide the development of more gender sensitive policies and practices to ensure equity in provision of services as opposed to the blunter push for equality.
The aim of this paper is to provide an overview of the findings from the Leeds study to highlight the wide disparities that exist within our municipalities with regard to some of the key social determinants of men’s health: educational attainment, housing, employment, poverty and living arrangements.
Methods
A cross-sectional study was adopted, which was based on an examination of routinely collected and available data relating to the social determinants of health.
Data sources
Educational attainment included the proportion of girls and boys in Leeds achieving: 1) a good level of development in the Early Years Foundation Stage Profile (EYFSP) [39]; 2) level 2 key stage 1 reading; 3) level 2 key stage 1 writing [40]; and 4) three or more higher grade General Certificate of Secondary Education (GCSE) passes including English and Maths [41]. Educational attainment data relating to looked after children was obtained directly from Leeds Children’s Services. Demographic data for those living in Council-owned high-rise flats was obtained directly from the Environments and Housing department within Leeds City Council (obtained April 2015). Benefits data for job seekers allowance and employment and support allowance were obtained from Leeds City Council Public Health intelligence team. Data showing underlying conditions for Employment and Support Allowance (ESA) claimants were obtained from nomisweb.co.uk. Data on divorces were obtained from the Office for National Statistics (ONS) [42].
Census data were used for the following:
The number of men and women in Leeds with no qualifications [43].
The number of men and women living alone [44]
Tenure [45]
Homelessness [46]
Unemployment [47]
Long-term unemployment and ‘never worked’ [48]
Employment data including status and hours worked [47]
The number of men and women economically inactive due to a long-term health problem or disability [49]
Marital status [50]
Lone fathers [51]
Data analysis
A descriptive analysis was undertaken. Where possible, data were disaggregated by age group, and sex at a city level and by area of residence within Leeds [at the level of the Middle Super Output Area (MSOA)]. Data were calculated as a proportion of the male or female age-specific population in Leeds or within an MSOA where appropriate. Data for each variable were ranked by MSOA with the greatest occurrence within the male population of that area. Mean ± SD sex differences in prevalence of socio-economic factor were analysed using an independent t-test or Mann Whitney U-test where appropriate, with significance set at p < 0.05. Analysis and presentation of data was completed using Microsoft Excel 2013 and SPSS (version 22).
Results
Educational attainment
The proportion of boys in Leeds (of all those eligible to be assessed) in 2013 achieving a good level of development in the Early Years Foundation Stage Profile [EYFSP] was significantly lower than for girls (45.6% ± 13.4% as compared to 60.2% ± 13.0%, P = 0.00) (Table 1). For both sexes, this was below the national average (boys 52.0%, girls 69.0%). In 3 MSOAs in Leeds the proportion of boys achieving a good level of development was at, or below, 20%.
Table 1.
Percentage of males and females, for Leeds and national, for Education, housing, employment and marital status and relationships
| Leeds | National | |||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| Mean ± SD (%) | Mean ± SD (%) | % | % | |
| Education | ||||
| Achieving a good level of development in the Early Years Foundation Stage Profile [EYFSP] * | 45.6 ± 13.4 | 60.2 ± 13.0 | 52.0 | 69.0 |
| Achieve level 2+ key stage 1 reading * | 80.1 ± 6.35 | 88.0 ± 6.87 | 86.0 | 92.0 |
| Achieve level 2+ key stage 1 writing * | 75.1 ± 7.31 | 85.5 ± 7.30 | 80.0 | 90.0 |
| Pupils at the End of KS4 Achieving 5+ A*-C Including English and Mathematics * | 52.4 ± 15.9 | 62.9 ± 15.2 | 55.7 | 65.7 |
| Adults (16–64) with no qualifications | 16.1 ± 8.38 | 16.9 ± 8.82 | ||
| Housing | ||||
| Aged 16+ living alone | 17.2 ± 6.30 | 17.6 ± 3.76 | ||
| Living in council-owned high-rise flats* | 62.4 ± 10.1 | 37.6 ± 10.1 | ||
| Living in social housing (aged 16+) | 17.7 ± 14.5 | 19.9 ± 15.2 | ||
| Employment | ||||
| Unemployed (aged 16+ exc FT students) * | 5.80 ± 3.12 | 3.30 ± 1.92 | 4.9 | 3.1 |
| Long term unemployed (aged 16–64) * | 2.70 ± 1.66 | 1.69 ± 1.05 | 2.2 | 1.7 |
| Never worked (aged 25+) * | 2.48 ± 1.96 | 6.23 ± 5.94 | 2.1 | 5.7 |
| Employees and self-employed (aged 16+ years) working long hours - over 49 h * | 9.87 ± 3.58 | 3.14 ± 1.46 | 8.5 | 2.2 |
| claiming Job Seekers Allowance * | 4.19 ± 3.51 | 2.18 ± 1.92 | 2.7 | 1.6 |
| Economically inactive due to long-term disability or illness (aged 16+) | 4.18 ± 2.32 | 3.69 ± 1.89 | 4.1 | 3.7 |
| Employment and Support Allowance (ESA) | 5.88 ± 3.30 | 5.01 ± 2.67 | 5.4 | 4.6 |
| Attendance allowance (aged 65+ years) * | 10.5 ± 3.65 | 16.8 ± 5.86 | 10.8 | 18.0 |
| Marital status and relationships | ||||
| Single (aged 16–64 years) * | 48.4 ± 13.5 | 42.8 ± 14.7 | 45.4 | 38.5 |
| Single (aged 30–49 years) * | 39.1 ± 11.3 | 27.0 ± 7.82 | 35.4 | 27.6 |
| Lone parents (aged 16–74) * | 0.85 ± 0.43 | 8.16 ± 4.32 | 0.8 | 7.2 |
| Divorced (aged 30–59 years) * | 10.5 ± 2.28 | 13.7 ± 2.70 | 8.4 | 11.9 |
* P < 0.01
Boys (aged 5–7 years) were also significantly less likely to achieve level 2+ key stage 1 reading (boys 80.1% ± 6.35%, girls 88.0% ± 6.87%, P = 0.00) and writing (boys 75.1% ± 7.31%, girls 85.5% ± 7.30%, P = 0.00) (Table 1). In 6 MSOAs in Leeds less than 60% of boys achieved level 2+ in writing, and in 11 MSOAs less than 70% of boys achieved level 2+ reading, with 1 MSOA having only 58% of their boys achieve this level. For girls, all MSOAs had more than 60% of girls reaching this level for writing, with only 6 of the 107 MSOAs in Leeds having less than 70% of girls reach this level for reading.
In 2013, the proportion of boys in Leeds achieving five or more higher grade GCSE passes including English and Maths was significantly lower compared to girls (52.4% ± 15.9% vs. 62.9% ± 15.2%, P = 0.00) and was lower compared to boys nationally (55.7%) (Table 1). In 9 MSOAs across Leeds less than 30% of boys are achieving this standard, with all MSOAs seeing more than 30% of girls getting those grades.
Approximately 69% of Looked After Children (LAC) accessing alternative education provision were boys, and the proportion of male LAC achieving a good level of development in the early Years Foundation Stage profile (23%) was similar to that observed in the lowest five ranked MSOAs in Leeds (19–26%). The proportion of male LAC achieving five or more A-C grades at GCSE including English and maths (14%) was less than observed in the lowest ranked MSOA in Leeds (21% for boys).
Across Leeds, 16.1% ± 8.38% of males (16–64) had no qualifications in 2011, however the top ten ranked MSOAs with the highest proportion ranged from 30% to 37% of males with no qualifications.
Housing
Approximately 17% of men aged 16+ lived alone in Leeds in 2011, which was similar to the number of women (Table 1). In the top ten ranked MSOAs with the highest proportion this was as high as 26.2% to 42.0% of men. Across Leeds as a whole approximately 16% of men in Leeds aged 16+ lived in social housing (rented from the local council or a not-for-profit housing association approved and regulated by Government) in 2011, however in the top ten ranked MSOAs this was as high as 39.4% to 59.1%.
In April 2015 there were blocks of council-owned high-rise flats in Leeds where 75–85% of residents were males and overall, there was a significantly higher proportion of male residents in this type of housing (62.4% ± 10.1% vs. 37.6% ± 10.1%, P = 0.00). The highest proportion of residents within these complexes were aged between 31 and 60 years of age (Fig. 1).
Fig. 1.
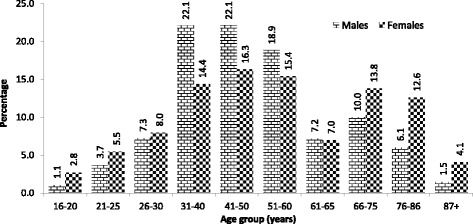
Percentage of men and women living in council owned high-rise flats in Leeds by age group (from Seims & White 5)
The 2011 census data for Leeds showed that 127 men (aged 16+) were living in a privately owned hostel or temporary shelter for the homeless which is almost double the number of females (64).
Employment
The number of unemployed men in Leeds, in 2011 was 68% higher compared to females, a gender difference much higher than for England & Wales, where 48% more men were unemployed compared to women. Unemployment was significantly greater among men than women (5.80% ± 3.12% vs. 3.30% ± 1.92%, P = 0.00) (Table 1), and the top ten ranked MSOAs with the highest proportion ranged from 10.9%–15.7%.
In 2011, significantly more men were classed as long-term unemployed than women (2.70% ± 1.66% vs. 1.69% ± 1.05%, P = 0.00), which was greater than observed for England & Wales (2.2%) (Table 1). The gender gap was also greater in Leeds compared to the data for England & Wales with 60% more men in Leeds classed as long-term unemployed compared to women verses a gap of 32% nationally. The top ten ranked MSOAs with the highest proportion of men (16–64 years) who were long-term unemployed ranged from 5.1% to 7.5%.
In 2011, 2.48% ± 1.96% % of men in Leeds aged 25+ had never worked which was higher than men in England & Wales (2.1%) (Table 1). In the ten highest ranked MSOAs this was as high as 5.2% to 8.2%.
In 2011, those men in work (employed and self-employed) were significantly more likely to be working full time, with nearly 9.87% ± 3.58% of men in Leeds over the age of 16 years working over 49 h a week compared to 3.14% ± 1.46% of women (P = 0.00, (Fig. 2 and Fig. 3). The top ten ranked MSOAs with the highest proportion of male employees (aged 16+ years) working long hours (over 49 h a week) ranged from 10.4% to 13.3% of men.
Fig. 2.
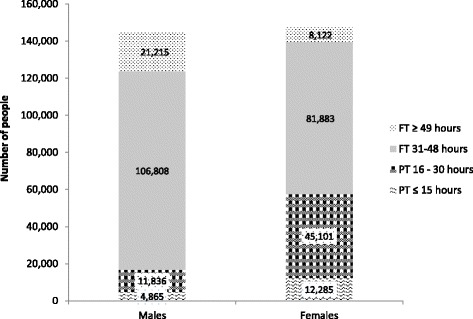
Hours worked by male and female employees (from Seims & White5)
Fig. 3.
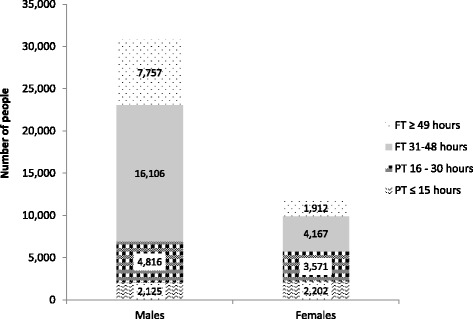
Hours worked by self-employed males and females (from Seims & White5)
There were 4.19% ± 3.51% of men claiming Job Seekers Allowance in Leeds in 2014, as compared to 2.18% ± 1.92% of women (P = 0.00), but in 3 MSOAs over 14% of the male population were claimants.
In 2011, 4.18% ± 2.32% of men (3.69% ± 1.89% of women) (aged 16+) were economically inactive due to long-term disability or illness (P = 0.23), however the top ten ranked MSOAs with the highest proportion ranged from 7.4% to 10.1%. In 2014, 5.88% ± 3.30% of men (aged 16–64) in Leeds claimed Employment and Support Allowance (ESA) as compared to 5.01% ± 2.67% of women (P = 0.09), with the top ten ranked MSOAs with the highest proportion of male claimants ranging from 10.9 to 13.0%. The most prominent underlying condition was mental and behavioural disorders, accounting for almost 50% of males claiming ESA. In 2014, 10.5% ± 3.65% of men aged over 65 claimed attendance allowance in Leeds (16.8% ± 5.86% of women, P = 0.00), however in the top ten ranked MSOAs this ranged from 14.7 to 25.8% of men in those areas.
Marital status and relationships
In 2011, 48.4% ± 13.5% of men aged 16–64 years were single, which was significantly higher than for women (42.8% ± 14.7%, P = 0.00) (Table 1). Significantly more men within the middle-aged (30–49 year) population of Leeds, were also single men compared to women (39.1% ± 11.3% vs. 27.0% ± 7.82%, P = 0.00).
The data from the 2011 Census for Leeds shows that divorced men are typically aged 30–59 years and that approximately 11% of this age group are divorced, however in the ten MSOAs ranked with the highest proportion of divorced men this ranged from 13.2% to 15.9%.
In 2011 there were 2254 lone fathers (aged 16–74) with dependent children in Leeds (0.85% ± 0.43% of men aged 16–74 in Leeds). This was proportionally similar to data for England and Wales (0.8% and 7.2% of the male and female 16–74 year population were lone fathers and mothers respectively).
Discussion
Main findings from this study
This is the first study to explore the social determinants of health from a male perspective across an entire city. Our study suggests that there is a clustering of known social determinants that are detrimental to health around deprived areas of Leeds and that there are marked gender differences evident. Although the current analysis did not allow for individual’s experiences to the mapped, it is notable that there was a common group of MSOAs which saw the highest proportion of men struggling with the social determinants of health. Those areas of Leeds that showed poor educational attainment also had a high proportion of long-term unemployed men, a higher proportion of men claiming benefits, more problematic housing and divorced men.
Comparison with the literature
There are well-established links between poverty and health [52–56], with the Marmot report highlighting that men generally have higher rates of premature death when experiencing social and economic hardship [1]. The health implications for men and boys with regard to worsening socio-economic hardship has also been noted both nationally [57] and internationally [2, 3, 58].
Implications of the findings
With the move of Public Health into local government, the link between targeting the social determinants of health as a means of improving the health of the local population has been acknowledged, but fiscal constraints mean more focused provision may prove more cost effective.
Planning services for effective public health requires targeting of resources to achieve maximal effect. What has become apparent through the study is the impact of the social determinants on men have been generally under-reported in the literature and this has perhaps left a cohort of vulnerable men hidden from Commissioners’ eyes. The clustering of factors that influence men and their health suggests they need to be recognised and tackled as a whole; focusing on single items negates the complexity of the broader picture.
Breaking the data down by MSOA gives a more detailed view of where services should be targeted and also gives visibility to the social problems that men are facing and a possible explanation for some of the health challenges they face. This is most starkly seen with regard to the high level of suicide in men within Leeds, with over 5 times more men dying as a result of taking their own life as compared to women, with living in the high rise flats, creating the most notable risky setting [13, 59, 60].
The analysis of educational attainment across the City showed that there is a need to consider not just how to get young boys better engaged with schooling, but that support may be needed for men throughout their lifespan. With some areas of Leeds having nearly a third of their male population with no educational qualifications this adds greatly to their risk of unhealthy lifestyles and risk of premature death [55, 61–63]. By targeting boys early in their school life they can be helped to overcome some of their deficits and this has long term benefits with regard to their cognitive skills and achievement, behaviour, mental health, other school related outcomes, and adult outcomes [64].
In support for the need for sex-specific data on the social determinants [32, 36] a key observation made in the Leeds study [13] was that although there were comprehensive locality maps of deprivation produced by the Leeds public health observatory, they rarely offered sex-specific data, leaving the possibility that those most at risk (either male or female) to be missed within any subsequent planning decisions. By making explicit the data on men and women it can also help inform health policies relating to the potential impact of the social world they live in.
The Leeds Report was initiated by the Health and Wellbeing Board and the Director for Public Health, and is now being considered by the Scrutiny Board of the Council, with view to stimulating a City-wide response to the report’s findings. This will be the first time that a whole city has instigated a review of services for men and offers up a model for how other cities can tackle men’s health.
There has already been some response, with, for instance, a new service being introduced into the high rise flats in Leeds. The introduction of the bedroom tax and the system of housing allocation has impacted on where young single unemployed men are being housed, with more now being located in the high rise blocks of flats than previously. The Commissioners have noted that this is creating a new problem, where these mostly white young men are suffering from low self-esteem, depression and social isolation. By offering support on their doorsteps has started to create a safer environment for them and an opportunity to identify physical and emotional problems earlier than previously.
Further research is needed with those living in the high risk areas to determine if they are affected by multiples of the factors identified in this paper, in the same way that are now being identified through the clustering of lifestyle factors such as smoking, drinking and sedentary behaviour [65]. This might enable a much more nuanced level of care planning for those individuals who are the most vulnerable.
Limitations of this study
The data that has been presented gives an overview of some of the key aspects of the social determinants that could be seen to affect the health of men, however the study was based on available data and was part of a bigger study, and therefore should not be seen as comprehensive.
This is not a longitudinal study and therefore the current data cannot be directly matched. There is a growing realisation of the clustering effect of factors that impact on health and wellbeing [66], however the health data available through the public health observatory does not allow for grouping of social factors at the individual level.
There may well be other levels of difference based on the intersectional factors, such as age, ethnicity, sexuality, and disability; this would need to be incorporated into future studies.
Conclusion
Although data collected across the city is disaggregated by sex there appears to be a lack of a gendered analysis of its implications for both men and for women. There is great variance in the social worlds of men across a city, which has implications for their health and wellbeing. In areas of deprivation a complex picture of multiple social problems emerges, with marked gender differences in the social determinants of health, with males seeming to be more negatively affected. By targeting men and boys more effectively greater efficiency in service delivery could be obtained. This examination of men’s social circumstances within a city could act as a model for undertaking similar studies both in the UK and elsewhere.
Acknowledgements
We thank the Leeds Observatory and Public Health team for their support during the study.
Funding
The study was funded by the Leeds City Council.
Availability of data and materials
Raw data are not publically available but were obtained as part of a contractual agreement with Leeds City Council.
Abbreviations
- ESA
Employment and support allowance
- EYFSP
Early years foundation stage profile
- GCSE
General Certificate of Secondary Education
- LAC
Looked after Children
- MSOA
Middle super output area
- ONS
Office for National Statistics
Authors’ contributions
All authors contributed to the study. AW was the principal investigator, AS conducted data collection and analysis, IC and TT helped interpret the data analysis and reviewed the manuscript critically for content. AW will act as guarantor. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The study was given ethical approval by Leeds Beckett University.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Alan White, Email: a.white@leedsbeckett.ac.uk.
Amanda Seims, Email: A.Seims@leedsbeckett.ac.uk.
Ian Cameron, Email: Ian.Cameron@leeds.gov.uk.
Tim Taylor, Email: Tim.Taylor@leeds.gov.uk.
References
- 1.Marmot Review Team . Marmot indicators 2014 a preliminary summary with graphs - strategic review of health inequalities post 2010. London: Institiute of Health Equity; 2014. [Google Scholar]
- 2.Cullen MR, Baiocchi M, Eggleston K, Loftus P, Fuchs V. The weaker sex? Vulnerable men and women’s resilience to socio-economic disadvantage. SSM - Popul Heal. 2016;2:512–524. doi: 10.1016/j.ssmph.2016.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.EC . The state of Men’s health in Europe: extended report. Luxembourg: European Commission; 2011. [Google Scholar]
- 4.Tan HM, Ng CJ, HCK C, Hai, Teo CH. Asian Men’s health report. Kuala Lumpur: Malaysian Men’s Health Initiative; 2013. [Google Scholar]
- 5.AIHW. The health of Australia’s males: 25 years and over. Canberra: Australian Institute of Health & Welfare; 2013.
- 6.McEvoy R, Richardson N. Men’s health in Ireland: a report from the Men’s health forum in Ireland. Belfast; 2004. http://www.mhfi.org/fullreport.pd. Accessed 26 Jan 2014.
- 7.Danish National Board of Health . Mænds sundhed - en oversigt overmænds sundhedstilstand og en gennemgang af effektive forebyggelsesmetoder. [Men’s health: An overview of men’s health and review of effective prevention methods] Copenhagen: Danish National Board of Health; 2010. [Google Scholar]
- 8.Starker A, Rommel A, Saß A-C. Bericht zur gesundheitlichen Lage der Männer in Deutschland – Fazit und Herausforderungen für eine gendersensible Gesundheitsberichterstattung. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2016;59:979–985. doi: 10.1007/s00103-016-2383-y. [DOI] [PubMed] [Google Scholar]
- 9.Storm I, den Hertog F, van Oers H, Schuit AJ. How to improve collaboration between the public health sector and other policy sectors to reduce health inequalities? – a study in sixteen municipalities in the Netherlands. Int J Equity Health. 2016;15:97. doi: 10.1186/s12939-016-0384-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.La Placa V, Knight A. Well-being: its influence and local impact on public health. Public Health. 2014;128:38–42. doi: 10.1016/j.puhe.2013.09.017. [DOI] [PubMed] [Google Scholar]
- 11.Leeds City Council and NHS Leeds . Leeds joint strategic needs assessment 2012: executive summary. Leeds: Leeds City Council and NHS Leeds; 2012. [Google Scholar]
- 12.Seims A, White A. The state of Men’s health in Leeds: data. Leeds: Leeds Beckett University, Leeds City Council; 2016. [Google Scholar]
- 13.White A, Seims A, Newton R. The state of Men’s health in Leeds: main report. Leeds: Leeds Beckett University, Leeds City Council; 2016. [Google Scholar]
- 14.White A, Seims A, Newton R. The state of Men’s health in Leeds: a summary. Leeds: Leeds Beckett University, Leeds City Council; 2016. [Google Scholar]
- 15.Wilkinson R, Marmot M. Social determinants of health. The solid facts (2nd edition) Copenhagen: World Health Organization; 2003. [Google Scholar]
- 16.Marmot Review Team . Fair society, healthy lives (the marmot review) London: The Marmot Review Team; 2010. [Google Scholar]
- 17.Feeney A, North F, Head J, Canner R, Marmot M. Socioeconomic and sex differentials in reason for sickness absence from the Whitehall II study. Occup Environ Med. 1998;55:91–98. doi: 10.1136/oem.55.2.91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.CSDH . A conceptual framework for action on the social determinants of health discussion. 2007. [Google Scholar]
- 19.Deaton A. Policy implications of the gradient of health and wealth. Health Aff. 2002;21:13–30. doi: 10.1377/hlthaff.21.2.13. [DOI] [PubMed] [Google Scholar]
- 20.Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav. 2010;51(Suppl Spring):S28–S40. doi: 10.1177/0022146510383498. [DOI] [PubMed] [Google Scholar]
- 21.Braveman P, Egerter S, Williams DR. The social determinants of health: coming of age. Annu Rev Public Health. 2011;32:381–398. doi: 10.1146/annurev-publhealth-031210-101218. [DOI] [PubMed] [Google Scholar]
- 22.Macdonald J. Shifting paradigms: a social determinants approach to solving problems in men’s health policy and practice. Med J Aust. 2006;185:456–458. doi: 10.5694/j.1326-5377.2006.tb00648.x. [DOI] [PubMed] [Google Scholar]
- 23.Griffith DM, Metzl JM, Gunter K. Considering intersections of race and gender in interventions that address US men’s health disparities. Public Health. 2011;125:417–423. doi: 10.1016/j.puhe.2011.04.014. [DOI] [PubMed] [Google Scholar]
- 24.Hosseinpoor AR, Stewart Williams J, Amin A, Araujo de Carvalho I, Beard J, Boerma T, et al. Social determinants of self-reported health in women and men: understanding the role of gender in population health. PLoS One. 2012;7:e34799. doi: 10.1371/journal.pone.0034799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bates LM, Hankivsky O, Springer KW. Gender and health inequities: a comment on the final report of the WHO Commission on the social determinants of health. Soc Sci Med. 2009;69:1002–1004. doi: 10.1016/j.socscimed.2009.07.021. [DOI] [PubMed] [Google Scholar]
- 26.Scott-Samuel A, Crawshaw P, Oakley A. “Men behaving badly”: patriarchy, public policy and health inequalities. Int J Mens Health. 2015;14:250–258. [Google Scholar]
- 27.Griffith DM. An intersectional approach to Men’s health. J Mens health. 2012;9:106–112. doi: 10.1016/j.jomh.2012.03.003. [DOI] [Google Scholar]
- 28.Macdonald J. A different framework for looking at Men’s health. Int J Men’s Heal. 2016;15:283–295. [Google Scholar]
- 29.Hankivsky O. Women’s health, men’s health, and gender and health: implications of intersectionality. Soc Sci Med. 2012;74:1712–1720. doi: 10.1016/j.socscimed.2011.11.029. [DOI] [PubMed] [Google Scholar]
- 30.Tolhurst R, Leach B, Price J, Robinson J, Ettore E, Scott-Samuel A, et al. Intersectionality and gender mainstreaming in international health: using a feminist participatory action research process to analyse voices and debates from the global south and north. Soc Sci Med. 2012;74:1825–1832. doi: 10.1016/j.socscimed.2011.08.025. [DOI] [PubMed] [Google Scholar]
- 31.Richardson N, Clarker N. Men’s health in Northern Ireland : tackling the root causes of Men’s [ ill ] - health. 2011. [Google Scholar]
- 32.White A, Richardson N. Gendered epidemiology: making men’s health visible in epidemiological research. Public Health. 2011;125:407–410. doi: 10.1016/j.puhe.2011.04.012. [DOI] [PubMed] [Google Scholar]
- 33.Lawrence K, Rieder A. Methodologic and ethical ramifications of sex and gender differences in public health research. Gend Med. 2007;4(Suppl B):S96–105. doi: 10.1016/S1550-8579(07)80050-7. [DOI] [PubMed] [Google Scholar]
- 34.European Commission . Gender equality and Women’s empowerment: transforming the lives of girls and women through EU external relations 2016–2020. 2015. [Google Scholar]
- 35.Sen G, Östlin P, George A. Unequal, unfair, ineffective and inefficient gender inequity in health: why it exists and how we can change it final report to the WHO Commission on social determinants of health women and gender equity knowledge network Gita sen and Piroska Östlin rev. 2007. [Google Scholar]
- 36.WHO. Women’s health and well-being in Europe: beyond the mortality advantage. Copenhagen; 2016. http://www.euro.who.int/en/publications/abstracts/womens-health-and-well-being-in-europe-beyond-the-mortality-advantage-2016. Accessed 27 June 2017.
- 37.Varanka JJ. Mainstreaming men into gender sensitive health policies. J Mens health. 2008;5:189–191. doi: 10.1016/j.jomh.2008.07.004. [DOI] [Google Scholar]
- 38.Kingdom U. Equality act. London: HMSO; 2010. [Google Scholar]
- 39.DfE . Early years foundation stage profile by gender (referenced by location of pupil residence). Data for neighbourhoods and regeneration. 2013. [Google Scholar]
- 40.DfE . Pupil attainment at key stage 1 by gender (referenced by location of pupil residence). Data for neighbourhoods and regeneration. 2013. [Google Scholar]
- 41.DfE . Pupil attainment at GCSE by location of pupil residence. Data for neighbourhoods and regeneration. 2013. [Google Scholar]
- 42.ONS . Divorces in England and Wales, 2011: number of divorces, age at divorce and marital status before marriage. Office for National Statistics. 2011. [Google Scholar]
- 43.NOMIS . DC5102EW (highest level of qualification by sex by age) - Nomis - official labour market statistics. 2013. [Google Scholar]
- 44.NOMIS . DC1109EW (household composition by age by sex) - Nomis - official labour market statistics. 2013. [Google Scholar]
- 45.NOMIS . DC3409EW (general health by tenure by sex by age) - Nomis - official labour market statistics. 2013. [Google Scholar]
- 46.NOMIS . DC4210EWLA (communal establishment management and type by sex by age) - Nomis - official labour market statistics. 2013. [Google Scholar]
- 47.NOMIS . DC6302EW (economic activity by hours worked by sex by long-term health problem or disability) - Nomis - official labour market statistics. 2013. [Google Scholar]
- 48.NOMIS . DC6114EW (NS-SeC by sex by age) - Nomis - official labour market statistics. 2013. [Google Scholar]
- 49.NOMIS . DC6107EW (economic activity by sex by age) - Nomis - official labour market statistics. 2013. [Google Scholar]
- 50.NOMIS . DC1107EW (marital and civil partnership status by sex by age). Nomis - official labour market statistics. 2011. [Google Scholar]
- 51.NOMIS . KS107EW - lone parent households with dependent children. Nomis - official labour market statistics. 2011. [Google Scholar]
- 52.Novoa AM, Ward J, Malmusi D, Díaz F, Darnell M, Trilla C, et al. How substandard dwellings and housing affordability problems are associated with poor health in a vulnerable population during the economic recession of the late 2000s. Int J Equity Health. 2015;14:120. doi: 10.1186/s12939-015-0238-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.McDaid D, Knapp M, Medeiros H, MHEEN Group. Employment and mental health: assessing the economic impact and the case for intervention. London; 2008. http://eprints.lse.ac.uk/4236/1/MHEEN_policy_briefs_5_Employment(LSERO).pdf. Accessed 12 Feb 2014.
- 54.Peruzzi A. From childhood deprivation to adult social exclusion: evidence from the 1970 British cohort study. Soc Indic Res. 2014;120:117–135. doi: 10.1007/s11205-014-0581-2. [DOI] [Google Scholar]
- 55.Sasson I. Trends in life expectancy and lifespan variation by educational attainment: United States, 1990–2010. Demography. 2016;53:269–293. doi: 10.1007/s13524-015-0453-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Thomas B, Dorling D, Smith DG. Inequalities in premature mortality in Britain: observational study from 1921 to 2007. BMJ. 2010:341:c3639. doi:10.1136/bmj.c3639. [DOI] [PMC free article] [PubMed]
- 57.Hacking JM, Muller S, Buchan IE. Trends in mortality from 1965 to 2008 across the english north-south divide: comparative observational study. BMJ. 2011;342 10.1136/bmj.d508. Accessed 16 Feb 2011. [DOI] [PMC free article] [PubMed]
- 58.Nusselder WJ, Looman CWN, Oyen H, Robine JM, Jagger C. Gender differences in health of EU10 and EU15 populations: the double burden of EU10 men. Eur J Ageing. 2010;7:219–227. doi: 10.1007/s10433-010-0169-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Insight . Insight report into preventing male suicide in LS12: final report august 2014. Leeds: Insight; 2014. [Google Scholar]
- 60.Everitt M, Eaton V, Ward C, Sehmbi V. Audit of Suicides and Undetermined Deaths in Leeds 2011-2013. Leeds: Leeds City Council; 2016. http://observatory.leeds.gov.uk/resource/view?resourceId=4775v.
- 61.Huisman M, Kunst AE, Bopp M, Borgan J-K, Borrell C, Costa G, et al. Educational inequalities in cause-specific mortality in middle-aged and older men and women in eight western european populations. Lancet. 2005;365:493–500. doi: 10.1016/S0140-6736(05)70273-7. [DOI] [PubMed] [Google Scholar]
- 62.Ross CE, Masters RK, Hummer RA. Education and the gender gaps in health and mortality. Demography. 2012;49:1157–1183. doi: 10.1007/s13524-012-0130-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Viner RM, Ozer EM, Denny S, Marmot M, Resnick M, Fatusi A, et al. Adolescence and the social determinants of health. Lancet. 2012;379:1641–1652. doi: 10.1016/S0140-6736(12)60149-4. [DOI] [PubMed] [Google Scholar]
- 64.Magnuson KA, Kelchen R, Duncan GJ, Schindler HS, Shager H, Yoshikawa H. Do the effects of early childhood education programs differ by gender? A meta-analysis. Early Child Res Q. 2016;36:521–536. doi: 10.1016/j.ecresq.2015.12.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Zwolinsky S, Raine G, Robertson S. Prevalence, co-occurrence and clustering of lifestyle risk factors among UK men. J Mens health. 2016;12:15–24. [Google Scholar]
- 66.Watts P, Buck D, Netuveli G, Renton A. Clustering of lifestyle risk behaviours among residents of forty deprived neighbourhoods in London: lessons for targeting public health interventions. Aust J Public Health. 2016;38:308–315. doi: 10.1093/pubmed/fdv028. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Raw data are not publically available but were obtained as part of a contractual agreement with Leeds City Council.