

Abstract
Objectives
Previous research has suggested that sexually aggressive behavior and sexual HIV risk behavior are associated. Childhood sexual abuse (CSA) is a well-established risk factor for both types problematic sexual behavior. Negative affect (i.e., anxiety, depression, and anger) is a less well-studied risk factor, but it has been theorized to relate to both sexual aggression and HIV risk behavior. Thus, this study sought to (1) confirm the relationship between sexual aggression and HIV risk behavior, (2) establish CSA and negative affect as shared risk factors for sexual aggression and HIV risk behavior, and (3) evaluate whether negative affect mediates the relationship between CSA and sexual aggression and between CSA and HIV sexual risk in a sample of heterosexual men.
Methods
We recruited young (ages 18–30), heterosexual men (N=377) from urban sexually transmitted infection clinics. Men completed measures of sexual HIV risk history (number of partners and condom use), sexual aggression history, CSA history, and trait negative affect (anger, anxiety, and depression). Structural equation modeling was used to examine hypothesized direct and indirect relationships.
Results
In the final SEM model, sexual aggression history and sexual HIV risk behavior were correlated. CSA was associated with both types of problematic sexual behavior. Anxiety significantly mediated the relationship between CSA and sexual aggression and between CSA and sexual HIV risk behavior (χ2[1300]= 2121.779, p<.000; CFI=0.905; RMSEA[90% CI]=.044 [.041–.047]).
Conclusions
Sexual aggression appears to be part of a constellation of sexual risk behaviors; thus, it may be possible to develop prevention programs that target both sexual HIV risk and sexual aggression. CSA is a shared risk factor for sexual aggression and HIV risk behavior through the pathway of anxiety. Thus, anxiety might be one promising target for intervention.
There is a movement in public health to broaden prevention approaches so that they simultaneously address multiple risky behaviors by targeting the shared underlying determinants of those behaviors (e.g., Prochaska, Spring, & Nigg, 2008). Sexual aggression (engaging in sex with an unwilling partner through use of verbal coercion, incapacitation, or force) and sexual HIV risk behavior (behavior, such as engaging in unprotected sex with multiple sexual partners, that increases the risk of contracting or spreading HIV or other sexually transmitted infections [STIs]) are two potential threats to public health that seem to overlap in occurrence and share some underlying risk factors. Thus, research on the shared correlates of these two risky sexual behaviors could be an initial step in the development of primary prevention programs that are designed to simultaneously target both behaviors. To that end, this study sought to examine the relationship between heterosexual men’s sexual aggression and HIV risk behavior and to evaluate child sexual abuse and negative affect as possible shared risk factors for these problematic sexual behaviors.
The Association between Sexual Aggression and HIV Risk
Sexual aggression (i.e., use of coercion, incapacitation, threats, or force to obtain sexual acts from an unwilling partner) has been theorized to be an important factor in the spread of HIV worldwide (e.g., Amaro, Raj, & Reed, 2001; Martin & Curtis, 2004). There is a large body of literature that demonstrates that sexual victimization—particularly childhood sexual abuse—is associated with HIV risk behavior (e.g., see Arriola, Louden, Doldren, & Fortenberry, 2005, for a meta-analysis, and see below for further discussion); however, there is limited empirical research on the relationship between adult sexual aggression perpetration and HIV risk. A few international studies have addressed the association between perpetration of sexual aggression and HIV risk. For example, in a study of South African students, researchers found that inconsistent condom use was more frequent in relationships in which the man used threat or force to obtain sex from the woman (Hoffman, O’Sullivan, Harrison, Dolezal, & Monroe-Wise, 2006). In one of the few U.S. studies on this topic, Blythe, Fortenberry, Temkit, Tu, and Orr (2006) found that, compared to other adolescent dating relationships, adolescent relationships in which the women experienced unwanted sex had higher proportions of intercourse without condom use.
Peterson, Janssen, and Heiman (2010) directly investigated the association between sexual aggression and HIV risk behavior. They found that men who had a history of sexual aggression (specifically those who had engaged in multiple acts of sexual aggression) reported (1) more sexual partners in the last year, (2) a larger number of lifetime “one-night stands,” and (3) a larger number of partners with whom they had not used a condom during the last three years as compared to men with no sexual aggression history. Men who had perpetrated multiple acts of sexual aggression also were more likely to have been diagnosed with a sexually transmitted infection (STI) in their lifetime than non-aggressive men. Peterson et al. (2010) also found that, at an event level, almost half of the discrete incidents of sexual aggression perpetrated by their sample involved no condom use, and in cases of physically forced sex in particular, no condom was worn during 97% of incidents. Thus, not only is it the case sexual aggression may be part of a larger pattern of sexual risk-taking, it also is the case that sometimes sexual aggression and HIV risk behavior co-occur within a single incident (see also Davis et al., 2012). Relatedly, Casey et al. (2016) found that young men who had perpetrated sexual coercion against an intimate partner reported higher numbers of lifetime sexual partners, high rates of non-monogamy, and less frequent condom use than young men who reported no history of physical abuse or sexual coercion against an intimate partner.
Although there is limited research looking directly at the association between sexual aggression and HIV risk, there is research to suggest that there are several factors that are likely to place men at risk for engaging in both sexual aggression and HIV risk behaviors. Identifying shared risk factors for sexual aggression and HIV risk could contribute to primary prevention interventions that simultaneously target both behaviors. By reviewing the literature on the correlates of men’s sexual aggression and HIV/STI risk, some shared predictors can already be identified—for example, alcohol use (Abbey, Zawacki, Buck, Clinton & McAuslan, 2004; Leigh and Stall, 1993) and hypermasculine gender roles (Murnen, Wright, Kaluzny, 2002; Shearer, Hosterman, Gillen, & Lefkowitz, 2005). One other empirically-supported risk factor for both sexual aggression and HIV risk is a history of child sexual abuse (CSA).
CSA and Risky Sexual Behavior
CSA is one of the most well-established correlates of risky sexual behavior in adulthood. This relationship has been demonstrated in a wide range of participant populations including women (e.g., Arriola et al., 2005), adolescent boys (e.g., Homma, Wang, Saewyc, & Kishor, 2012), men who have sex with men (e.g., Lloyd & Operario, 2012; Paul, Catania, Pollack, & Stall, 2001), and HIV positive men (e.g., O’Leary, Purcell, Remien, & Gomez, 2003). Senn, Carey, Vanable, Coury-Doniger, and Urban (2006) found very high rates of CSA among both men and women recruited at a STI clinic. In that study, patients with a history of CSA also reported more sexual risk than patients without a history of CSA, including more sexual partners, more unprotected sex, and a higher likelihood of having engaged in sex trading.
CSA and Sexual Aggression
CSA is also a well-documented correlate of later sexual aggression perpetration against others (e.g., Lambie, Seymour, Lee, & Adams, 2002; Merrill, Thomsen, Gold, & Milner, 2001). For example, in a nationally representative sample of young men, men with a history of CSA combined with a history of physical abuse were 450% more likely to perpetrate sexual coercion than men without a history of physical or sexual abuse (Casey, Beadnell, & Lindhorst, 2009). Loh and Gidycz (2006) found that history of CSA was related to sexual aggression perpetration at an initial retrospective assessment, such that men with a history of CSA were six times more likely to report sexual aggression than men without a history of CSA. However, history of CSA at the initial assessment did not predict perpetration during a three-month follow-up period when entered into a model with multiple other predictors; instead, sexual aggression in the follow-up was predicted by prior history of sexual aggression perpetration, family conflict resolution strategies, and dating conflict resolution strategies. Relatedly, White and Smith (2004) found that CSA predicted adolescent sexual aggression, which in turn, predicted adult sexual aggression. Using mediation analyses, Casey et al. (2017) found both a direct and indirect relationship between CSA and sexual aggression perpetration. Other researchers, though, have failed to find a direct path between CSA and adult sexual aggression perpetration, instead finding that the relationship is mediated by a variety of different variables (e.g., Krahe & Berger, 2017; Parkhill & Pickett, 2016). Identifying factors that mediate the relationship between CSA and sexual aggression is important—especially if those factors are amenable to change—because they provide a potential avenue for prevention.
CSA has been shown to be related to negative affect, including depression, anxiety, and anger (e.g., Browne & Finkelhor, 1986; Romano & De Luca, 2001). Compared to CSA, negative affect has been less studied as a predictor of sexual risk and sexual aggression, but there is reason to think that it might be associated with both sexual risk behaviors. Thus, negative affect represents one potential mediator in the relationship between CSA and negative sexual health outcomes.
Negative Affect and Sexual HIV Risk Behavior
Trait negative affect underlies a range of psychopathology, including major depressive disorder, social phobia, generalized anxiety disorder, obsessive-compulsive disorder, and panic disorder with agoraphobia (Brown, Chorpita, & Barlow, 1998). Trait negative affect represents a broad dimension comprised of proneness to several separate but interrelated emotions, including anxiety, depression, and anger (Watson & Clark, 1992; Watson & Tellegen, 1985). There is value in investigating negative emotions separately as well as in combination with each other. Much of the literature evaluating the impact of trait negative emotions on sexual aggression and sexual risk (see below) has investigated the impact of anxiety, depression, and anger separately, and indeed, the relationship between negative affect and any given outcome variable is sometimes found to differ across different types of negative affect.
Negative affect may be a risk factor for HIV/STI risk behavior, although the evidence for this is mixed. Several researchers have found support for a relationship between negative affect and sexual risk-taking. For example, Brown et al. (2006) found that, among African American adolescents, depressive symptoms at an initial time point were positively associated with inconsistent condom use at a six month follow-up. Ramrakha, Caspi, Dickson, Moffitt, and Paul (2000) also found a positive association between depressive disorders and sexual risk in young adults. Among men who have sex with men in a daily diary study, Mustanksi (2007) found no relationship between state or trait negative affect and HIV risk behavior. However, Perkins, Lesserman, Murphy, and Evans (1993) found a positive association between risk and both depression and anger, and Rotheram-Borus, Rosario, Reid, & Koopman (1995) found a positive association between risk and both depression and anxiety among men who have sex with men. Cooper, Agocha, and Sheldon’s (2000) research provided a potential theoretical explanation for the relationship between negative affect and sexual risk; they found that for some individuals, risky sexual behaviors function as a maladaptive strategy for coping with negative emotional states.
Yet, in a meta-analytic review, Crepaz and Marks (2001) concluded that there was not strong empirical support for a relationship between negative affect and sexual risk, although the authors acknowledged that effect sizes varied widely in the studies that they reviewed, with some studies showing a moderate positive relationship between negative affect and risk, some studies showing a moderate negative relationship, and some showing no relationship.
In their response to Crepaz and Marks (2001), Kalichman and Weinhardt (2001) argued against dismissing the relationship between negative affect and sexual risk, and they called particularly for research on the relationship between negative affect and sexual risk in at-risk populations (p. 301). Indeed, the relationship between negative affect and sexual risk does seem to differ depending on the population studied, suggesting that there are likely multiple different pathways to sexual risk. For example, in the Crepaz and Marks (2001) review, some of the largest effect sizes showing a positive relationship between negative affect and sexual risk (weighted r = .30–.55) were found in studies of high risk groups such as female injection drug users (Nemoto, Foster, & Brown, 1991), men who have sex with men (Perkins et al., 1993; Rotheram-Borus et al., 1995), and HIV positive participants (Clement, 1992; Kelly et al., 1993).
Negative Affect and Sexual Aggression
Although trait negative affect is a well-documented correlate of aggressive behavior across a variety of contexts (e.g., Douglas & Martinko, 2001; Mammen, Kolko, & Pilkonis, 2002; Margolin, John, & Gleberman, 1988), there is relatively little research on negative affect as a correlate of sexual aggression specifically. Nevertheless, negative affect has frequently been hypothesized to be one risk factor for sexual aggression (e.g., Hall & Hirschman, 1991; Howells, Day, & Wright, 2004). For example, Malamuth and colleagues identified “hostile masculinity” as a central characteristic of sexually aggressive men (Malamuth, Linz, Heavey, Barnes, & Acker, 1995; Malamuth, Sockloskie, Koss, & Tanaka, 1991). According to the researchers, hostile masculinity is driven, in part, by negative affect. For example, Malamuth et al. (1995) described the hostile masculine man as “afraid of rejection and anxious about relationships with women,” “feeling stress as a result of failure to live up to rigid masculine expectations,” and prone to “irritability” and “high negative affect” (p. 354). Indeed, Malamuth et al. (1995) found that a composite measure of hostile masculinity, which included measures of affective intensity and irritability, was significantly associated with men’s sexually aggressive behavior.
A few older studies have explored the role of anger in predicting sexual aggression. Anger has been found to be correlated with sexual aggression based on self-report studies of community men (Scott, Owens, & Stecker, 1993) and incarcerated men (Lyn & Burton, 2005). Yates, Barbaree, and Marshall (1983) found that anger inductions in a laboratory increased college men’s sexual arousal in response to a sexually violent video clip. More recently, Davis, Danube, Stappenbeck, Norris, and George (2015) found that trait anger at an initial assessment predicted sexual aggression perpetration at a three month follow-up in a sample of young community men.
Although anger has been shown to be a correlate of sexual aggression, there is limited research on the association between sexual aggression and other negative affective states (e.g., anxiety, sadness), especially among community samples of men. However, Lyn and Burton (2005) did find an association between anxiety and rape in their sample of incarcerated men, and depressive symptoms have been shown in several studies to be associated with sexual offending in juveniles (Becker, Kaplan, Tenke, & Tartaglini, 1991; Cooper, Murphy, & Haynes, 1996). Miner, Swinburne Romine, Robinson, Berg, and Knight (2014) also found that anxious attachment was associated with child sexual abuse perpetration among adolescent boys; however, the mechanisms underlying child sexual abuse perpetration and adult sexual aggression may be quite distinct.
A Potential Mediation Model
CSA has been well-established as a risk factor for both sexual HIV risk behavior and sexual aggression. Understanding the pathway through which CSA leads to these risk behaviors could help in the development of interventions to reduce risk among individuals with a history of CSA.
A history of CSA has been clearly demonstrated to be associated with high levels of trait negative affect, including depression, anxiety, and anger (e.g., Browne & Finkelhor, 1986; Romano & De Luca, 2001). Given (1) the established relationship between CSA and negative affect and (2) the potential relationship between negative affect and HIV risk and sexual aggression, negative affect may help to explain the link between CSA and later sexual risk in the form of HIV risk behaviors and sexual aggression. Further, negative affect is a promising direction for prevention programs, as there are already effective psychological interventions to address negative affect.
The Current Study
In the current study, we used structural equation modeling (SEM) to examine the following four interconnected hypotheses:
Consistent with Peterson et al. (2010), we predicted that sexual aggression would be associated with HIV/STI risk behavior. Specifically, we predicted that men with a history of sexual aggression would have a higher likelihood of engaging in sexual behavior that places them at risk for HIV and STIs as compared to men without a history of sexual aggression.
Based on past research (e.g., Lambie et al., 2002; Lloyd & Operario, 2012), we predicted that a history of child sexual abuse would be associated with both HIV risk behavior and sexual aggression.
Based on past theory (e.g., Cooper et al., 2000; Hall & Hirschman, 1991) and research (e.g., Brown et al., 2006; Malamuth et al., 1995), we predicted that trait negative affect (anger, anxiety, and depression) would be associated with both HIV risk behavior and sexual aggression.
Based on prior research demonstrating a relationship between CSA and negative affect (e.g., Browne & Finkelhor, 1986; Romano & De Luca, 2001), we predicted that negative affect would mediate the relationship between CSA and HIV risk behavior and between CSA and sexual aggression.
The hypothesized interrelationships among all variables are depicted in Figure 1.
Figure 1.
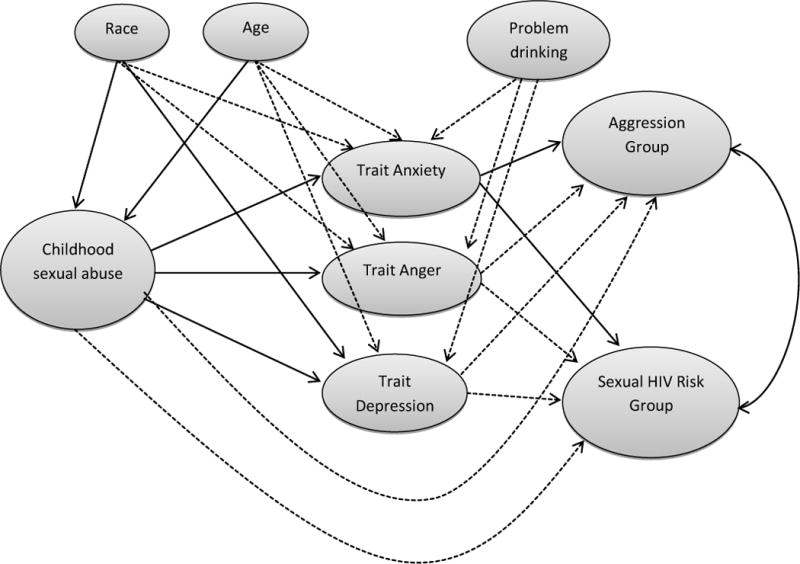
Hypothesized relationships among the variables. Based on final structural equation model testing, statistically significant pathways are depicted with solid lines and non-significant pathways are depicted with dotted lines.
We examined these hypotheses in a sample of young male patients at urban STI clinics in two Midwestern U.S. cities. We selected the STI clinic sample because we expected high rates of HIV risk behavior and high rates of sexual aggression (given the expected association between HIV risk behavior and sexual aggression) in that sample; based on past research (Senn et al., 2006), we also expected high rates of CSA among that sample.
METHODS
Participants
We recruited male patients at two urban STI clinics—one in St. Louis, Missouri and one in Indianapolis, Indiana—to complete a paper-and-pencil survey onsite in the waiting room of the clinic. Participants were eligible if they (1) were between the ages of 18 and 30, inclusive; (2) self-identified as heterosexual; and (3) were unmarried. A total of 523 men started the survey. Sixty-six were ineligible based on one or more eligibility criterion. An additional 31 failed to complete the questionnaire packet, 13 provided inconsistent or random responses, and 36 men were removed from the dataset because they were missing data on more than 75% of the items on one or more of the CSA and negative affect scales that were central to the research questions for this study. The final sample consisted of 377 men (Mage = 23.6; SD = 3.57); 161 were recruited in St. Louis and 216 were recruited in Indianapolis. Thus, the completion rate for eligible participants was 82%.
The STI clinics where participants were recruited provided low-cost or free STI testing and treatment. The clinics served primarily low-income, African American patients, and the demographics of our sample reflected that population. Racially, the sample predominantly identified as Black/African American (294; 78%). The remaining men were White/European American (60; 16%), American Indian/Native American/Alaskan Native (2; 0.5%); or Asian/Asian American (1; 0.3%). Six men (2%) reported that they were bi- or multi-racial. The remaining men (15; 4%) did not report their race or identified their race as “other.” Thirteen men (3%) identified their ethnicity as Hispanic or Latino. The modal household income reported by 42% of participants was $15,000 or less per year, and the majority of participants (78%) reported an annual household income of less than $30,000. Participants in our sample reported completing a mean of 12.05 years of education (SD = 2.17), equivalent to a high school diploma or successful completion of the General Education Development (GED) test.
Participants described their current relationship status as “not in a relationship, but I am dating” (110; 29%), “in an exclusive/monogamous relationship” (108; 29%), “in a nonexclusive/nonmonogamous relationship (one or both of us has, or has had, sex with others but WITHOUT the other’s knowledge or permission)” (75; 20%), “not in a relationship, and I am not dating” (42; 11%), or “in an open relationship (one or both of us has or may have sex with other partners, WITH the other’s knowledge or permission)” (34; 9%). The remaining men did not report their relationship status. Over a fourth of the men (27%) reported that they were living with a partner at the time they participated in the study.
Measures
Participants completed a questionnaire packet that included measures of demographics, sexual aggression history, sexual risk-taking history, CSA history, and negative affect proneness. As a measure of problematic alcohol consumption, we also asked participants to “think of the occasion you drank the most this past month,” and to indicate how many alcoholic drinks they consumed on that occasion. The findings presented here were part of a larger research project, so the participants also completed additional attitudinal and behavioral measures (e.g., measures of sexual sensation-seeking, hypermasculinity, sexual excitation and inhibition, etc.) that are not reported here.
Sexual aggression history
Sexual aggression history was measured using the Sexual Strategies Scale (SSS; Strang, Peterson, Hill, & Heiman, 2014). The SSS is a revision and extension of the Postrefusal Persistence Scale developed by Struckman-Johnson, Struckman-Johnson, & Anderson (2003). The SSS asks participants, “In the past, which if any of the following strategies have you used to convince a woman to have sex (oral, anal, or vaginal intercourse) after she initially said ‘no’?” Participants can then check any of 22 sexually coercive strategies that they had used for obtaining sex. The strategies listed in the scale reflect varying types of sexual aggression; for the purposes of this study, the four types of strategies included the following: Enticement, Coercion, Intoxication, and Threats/Force. The items from the SSS are listed in Table 1. Prior research (Strang et al., 2014) found that the SSS was significantly correlated with other measures of sexual aggression, including the Revised Sexual Experiences Survey (SES; Koss et al., 2007); however, in that study, men reported higher rates of sexual aggression on the SSS as compared to the SES, suggesting that the SSS may identify some sexually aggressive men who are missed by the SES. Additionally, in a prior study, the SSS was not significantly correlated with measures of socially desirable responding (Strang et al., 2014). Testa, Hoffman, Lucke, & Pagnan (2015) concluded that the SSS may be a preferable to the SES as a measure of sexual aggression due to its better Rasch properties and simpler wording.
Table 1.
Percentages of men reporting use of each sexually aggressive strategy on the Sexual Strategies Scale (SSS)
| SSS items | % (n) |
|---|---|
| Enticement items | |
| 1. Continuing to touch and kiss her in the hopes that she will give in to sex. | 59.2% (223) |
| 13. Taking of your clothes in the hopes that she will give in to sex. | 28.1% (106) |
| 12. Taking off her clothes in the hopes that she will give in to sex. | 25.5% (96) |
| Endorsement of one or more enticement items | 63.9% (241) |
| Verbal Coercion items | |
| 2. Telling her lies (e.g., saying “I love you” when you don’t). | 33.2% (125) |
| 6. Asking her repeatedly to have sex. | 27.3% (103) |
| 21. Accusing her of “leading you on” or being “a tease.” | 16.7% (63) |
| 3. Using your older age to convince her. | 13.5% (51) |
| 20. Questioning her commitment to the relationship (e.g., saying “if you loved me, you would.”). | 13.3% (50) |
| 16. Questioning her sexuality (e.g., calling her a lesbian). | 11.1% (42) |
| 5. Threatening to tell others a secret or lie about her if she doesn’t have sex (i.e., blackmail). | 4.8% (18) |
| 15. Threatening to break up with her if she doesn’t have sex. | 4.5% (17) |
| 17. Using your authority to convince her (e.g., if you were her boss, her supervisor, her camp counseling, etc.). | 3.7% (14) |
| 10. Threatening to harm yourself if she doesn’t have sex. | 2.1% (8) |
| Endorsement of one or more verbal coercion items | 57.6% (217) |
| Intoxication items | |
| 4. Getting her drunk/high in order to convince her to have sex. | 20.7% (78) |
| 9. Taking advantage of the fact that she is drunk/high. | 10.9% (41) |
| 22. Slipping her drugs (e.g., GHB or “Roofies”) so that you can take advantage of her. | 1.1% (4) |
| Endorsement of one or more intoxication items | 25.5% (96) |
| Threat/Physical Force items | |
| 7. Blocking her if she tries to leave the room. | 4.5% (17) |
| 14. Using physical restraint. | 4.0% (15) |
| 11. Using a weapon to frighten her into having sex. | 3.2% (12) |
| 18. Harming her physically. | 2.1% (8) |
| 19. Tying her up. | 1.9% (7) |
| 8. Threatening to harm her physically if she doesn’t have sex. | 1.9% (7) |
| Endorsement of one or more threat/physical force items | 10.6% (40) |
Note. Instructions for the SSS read, “In the past, which if any of the following strategies have you used to convince a woman to have sex (oral, anal, or vaginal intercourse) after she initially said ‘no’?” Participants were instructed to check all strategies that applied to them.
STI risk history
Sexual risk was measured with questions about participants’ number of sexual partners and their use of condoms. To assess number of partners, participants were asked “In the past 6 months, with how many people have you had vaginal intercourse (penis in vagina sex)?” and “In the past 6 month, with how many people have you had anal sex (penis in anus/butt/rectum)?” For the anal sex question, participants were asked to indicate their number of male and their number of female partners. To assess condom use, participants were asked, “The last time you had vaginal intercourse, did you use a condom?” and “The last time you had anal sex, did you use a condom.” Response options were No, Yes, Unsure, and Not applicable (I’ve never had vaginal [anal] sex). Responses to these items were used to calculate an HIV risk index as described in the results section below. Our index is consistent with recommendations to assess multiple aspects of risk-taking (i.e., number of partners and condom use) and to use items that assess risk behaviors in a relatively short time period (Metzler, Noell, & Biglan, 1992).
Childhood sexual abuse
Experiences with child sexual abuse were measured with the five-item sexual abuse subscale of the Childhood Trauma Questionnaire (CTQ; Berstein, Ahluvalia, Pogge, & Handelsman, 1997; Berstein et al., 2003). Items on the scale (e.g., “When I was growing up, someone tried to make me do sexual things or watch sexual things.”) were rated on a scale from 1 (Never true) to 5 (Very often true). Thus, scores on the subscale could range from 5 (meaning that the participant had never experienced sexual abuse) to 25. The CTQ and its subscales have demonstrated strong psychometric properties across diverse populations. In the current study, the five items of the sexual abuse subscale demonstrated good internal consistency (α = .89)
Negative affect
Negative affect can be conceptualized as both a state and a trait (Watson, Clark, & Tellegen, 1988). Because for this study we were interested in the relationship between negative affect and long-term sexual aggression and HIV risk history, we wanted to evaluate trait-level negative affect, or a general proneness to experiencing anger, anxiety, and depression.
Anxiety was assessed using the Trait subscale of the State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, & Lushene, 1970), a 20-item measure of proneness to anxiety symptoms. Sample items on the STAI include, “I feel nervous and restless” and “I feel secure” (reverse scored). Participants rate each item using the following scale: 1 (almost never), 2 (sometimes), 3 (often), and 4 (almost always). Scores on the trait scale of the STAI range from 20 to 80, with higher scores indicating greater trait anxiety. The trait portion of the STAI has shown good test-retest reliability (α = .97), and discriminant validity (Metzger, 1976). For the current sample, internal consistency was good (α = .85).
Depression was assessed using the Zemore Depression Proneness Ratings (ZDPR; Zemore, Fischer, Garratt, & Miller, 1990). The ZDPR is a 13-item measure of the propensity of individuals to experience depressive symptoms. Items such as, “Compared to most people you know, how often do you get depressed?” are rated on a scale from 1 (much less) to 5 (about the same) to 9 (much more). Scores on the ZDPR range from 13 to 117, with higher scores indicating greater depression proneness. The ZDPR has shown good internal consistency (α=.90), and good test-retest reliability (r=.82). It also has proven to be a better predictor of past depressive episodes than the Beck Depression Inventory (Zemore et al., 1990). In the current sample, the ZDPR demonstrated similarly strong internal consistency (α = .94).
Anger was assessed using the Trait Anger Scale from the State-Trait Anger Expression Inventory (STAXI; Spielberger, 1988). This is a 10-item scale that measures the tendency to experience and express anger. It includes items such as, “I have a fiery temper,” which are rated on the following scale: 1 (almost never), 2 (sometimes), 3 (often), 4 (almost always). Scores range from 10 to 40, with higher scores indicating greater anger proneness. The STAXI has shown good internal consistency (α =.73–.85), has been shown to correlate positively with other anger measures, and has successfully discriminated between high and low anger groups (Eckhardt, Norlander, & Deffenbacher, 2004). The scale demonstrated good internal consistency in the current sample (α = .90).
Procedure
Participants were approached by researchers in the waiting room of the clinic, invited to participate in a study of “men’s sexual decision-making,” and told the eligibility criteria for the study. A consent statement was reviewed with interested and eligible men. Then, the men were given a paper-and-pencil questionnaire packet to complete in the waiting room. They were told to sit in a quiet place and not to consult with anyone about the questions or their answers. If they came to the clinic with someone, they were asked to sit separately from that person while filling out the packet. The entire packet took approximately 45 minutes to complete; most men were able to complete the packet during the time that they were waiting for their appointment. Participants were paid $15 cash for their participation. Participants were not required to provide identifying information; however, participants had the option to provide their name and contact information if they were interested in being contacted for future paid studies. The methods of this study were approved by the institutional review boards at Indiana University Medical School and University of Missouri-St. Louis. Data for this study were collected in 2008 and 2009.
Data Analytic Approach
The hypotheses of this study were tested using structural equation modeling (SEM). SEM is a flexible methodology that allows for examination of several empirical relationships simultaneously while also assessing the factor structure of the items. In doing so, the analyses account for measurement error while estimating the significance of the paths between variables (Byrne, 2009).
The choice of ordering variables is not a straight forward process (Bollen, 1989; Kenny, 1979; Loehlin, 1992; Pearl, 2000). Without assuming causality, we tested the predictive relationship between variables to provide an overall picture of how childhood sexual abuse and the components of negative affect each directly impact risk and aggression, as well as to understand how childhood sexual abuse works through different types of negative affect to indirectly impact risk and aggression while controlling for age, race, and problem drinking.
We grouped the nine variables in the model (age, race, problem drinking, childhood sexual abuse, anger, depression, anxiety, HIV risk, and aggression) into subsets with respect to their likely predictive order. Age, race and problem drinking were treated as exogenous control variables. Age seemed relevant as a control variable because we were measuring lifetime experiences of sexual aggression; thus, older age would be associated with greater opportunity to engage in aggression. We controlled for race, because race has been shown in prior studies to be related to some of the variables in our model, including CSA history (Kenny & McEachern, 2000) and trait depression (Breslau et al., 2006; William et al., 2007). Problem drinking also was included as a control variable because problematic alcohol use has been shown to be correlated with CSA (e.g., Bensley, Van Eenwyk, & Simmons, 2000), negative affect (e.g., Caldwell et al., 2002), HIV risk behavior (e.g., Leigh & Stall, 1993), and sexual aggression (e.g., Abbey et al., 2004). Childhood sexual abuse, anger, depression, anxiety were modeled as both exogenous and endogenous variables, and risk and aggression were considered as endogenous (Figure 1).
Model fit was assessed in several ways. Global goodness of fit was assessed via the chi-square statistic (Bollen, 1989). However, because the chi-square test can be significant with larger sample sizes (e.g. N≈400), it is often paired with local fit indices to fully assess model integrity (Bollen & Pearl, 2013). Our local goodness of fit measures were the comparative fit index (CFI), for which ideal values range between 0.90 and 1.0, as well as the root mean square error of approximation (RMSEA; Brown & Cudeck, 1993), for which values of .08 or below indicate reasonable fit of the model to the data. A more exhaustive review of fit indices can be found in previous literature (e.g. Bollen, 1989; Bollen & Pearl, 2013; Brown & Cudeck, 1993; Byrne, 2009; Pearl, 2000). All analyses were conducted in AMOS, 24.0, using full information maximum likelihood estimation.
RESULTS
Data Preparation and Descriptive Statistics
See Table 1 for the frequencies with which men endorsed each item on the SSS. The SSS is a behavioral sampling measure, and items cannot be summed to create a meaningful total score because the total number of times that an individual engaged in each specific behavior is not assessed by the scale; thus, a dichotomous score was used. For the purposes of our analyses, men were classified as sexually aggressive (n = 233; 61.8%) if they reported ever obtaining oral, anal, or vaginal sex through coercion, incapacitation through drugs or alcohol, or physical force. All other men were classified as non-aggressive.
Men who reported using enticement (e.g., continuing to touch or kiss their partner, removing their clothes or their partner’s clothes) but no other forms of coercion or aggression were not included in our sexually aggressive group because it was not clear whether enticement should be considered a coercive strategy or an acceptable form of seduction and because the majority of men in our sample reported engaging in enticement, suggesting that it was a relatively normative behavior. Notably, although we did not include enticement as part of our definition of sexual aggression, a significantly larger percentage of our aggressive group (84.1%) reported having used enticement as compared to our non-aggressive group (31.3%), X2 (1, N = 377) = 107.88, p < .001, ɸ = .54. Thus, although enticement may be relatively less severe or coercive than other forms of pressure, this does suggest that enticement likely falls on the very low end of a continuum of sexually coercive and aggressive behavior (see also Testa et al, 2015).
For our analyses, men were classified as high HIV risk (n = 122; 32.4%) if they reported one or both of the following: (1) They had three or more vaginal sex partners in the last 6 months, and they did not use or did not know if they had used a condom during the last vaginal sex. (2) They had three or more anal sex partners (including both men and women) in the last 6 months, and they did not use or did not know if they had used a condom during the last anal sex. All other men were classified as low HIV risk. The use of a dichotomous index of risk allowed for the simultaneous consideration of both number of partners and consistency of condom use, and use of three or more sexual partners as a criterion for risk is consistent with risk indices used by other researchers with a variety of research population (e.g., Guttmacher et al., 1997; Koblin et al, 2015; Reisner, Hughto, Pardee, & Sevelius, 2016).
For the measures of negative affect (STAXI, STAI, and ZDPR) and CSA (CTQ), as described above, participants were eliminated if they completed less than 75% of items on at least one of the measures. For the remaining participants, missing values were replaced using mean imputations for descriptive statistics; for the SEM analyses, missing data were handled using full information maximum likelihood estimation. Our sample’s mean score on the STAI was 43.80 (SD = 8.90; range = 20–75), which is significantly higher than in a prior study of undergraduate men and women (M = 39.63; SD = 9.27; Plehn & Peterson, 2002), t (877) = 6.71, p < .001. Our sample’s mean score on the STAXI was 20.18 (SD = 6.47; range = 10–40), which is significantly higher than in a prior study with a sample of nonclinical young men (ages 18–21 years; M = 18.30; SD = 4.49; Meyer et al., 2005), t (500) = 3.02, p < .001. Finally, the mean scores for our sample on the ZDPR was 46.94 (SD = 21.72; range = 13–117), which is significantly lower than in a prior study of undergraduate men (M = 54.3, SD = 16.7; Lykins, Janssen, & Graham, 2006), t (774) = 5.31, p < .001.
The mean score on the CTQ sexual abuse subscale was 8.97 (SD = 4.68; range = 5–25), with 197 men (52.3%) reporting at least some CSA history (CTQ > 5.0). Skewness and kurtosis values for all measures of negative affect and CSA were within an acceptable range (−.33 – .77 for skewness and −.70 – .70 for kurtosis).
When asked about the most alcohol they had consumed at a time during the prior month (a measure of problem drinking), participants reported consuming an average of 7.02 drinks (SD = 5.26), with a range of 0 to 16 drinks.
Correlations among all of the variables in our model are included in Table 2. Based on a chi-square test, aggressive men were classified as high HIV risk at significantly greater rates (40.9%) than non-aggressive men (25.6%), X2 (1, N = 348) = 8.52, p = .004, ɸ = .16
Table 2.
Bivariate correlations among all variables included in the SEM model
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Racea (0 = Black; 1 = White) | ||||||||
| 2. Age (years) | .12* | |||||||
| 3. Problem drinking (largest number of drinks consumed at one time in the prior month) | .30*** | .14** | ||||||
| 4. Childhood sexual abuse (CTQ) | −.20*** | −.04 | .01 | |||||
| 5. Trait anxiety (STAI) | −.06 | −.02 | .06 | .48*** | ||||
| 6. Trait anger (STAXI) | −.12* | −.13* | .05 | .30*** | .36*** | |||
| 7. Trait depression (ZDPR) | .08 | −.03 | .07 | .39*** | .56*** | .34*** | ||
| 8. Sexual aggressionb (0 = no aggression; 1 = any aggression) | −.24*** | .05 | .14** | .25*** | .33*** | .28*** | .24*** | |
| 9. Sexual riskc (0 = low risk; 1 = high risk) | −.07 | .08 | .15** | .16** | .16** | .09 | .11* | .16** |
Note. CTQ = Childhood Trauma Questionnaire. STAI = Trait subscale of the State-Trait Anxiety Inventory. STAXI = Trait Anger subscale from the State-Trait Anger Expression Inventory. ZDPR = Zenmore Depression Proneness Ratings.
For correlations with race, n = 353; individuals who identified with racial categories other than Black or White were excluded.
“Any sexual aggression” includes all men who reported engaging in oral, anal, or vaginal sex through verbal coercion, intoxication, and/or threats or force on the Sexual Strategies Scale.
“High HIV risk” includes all men (1) who reported 3 or more vaginal sex partners in the last six months and who reported not using a condom or not knowing whether they used a condom during last vaginal sex and/or (2) who reported 3 or more anal sex partners in the last six months and who reported not using or not knowing whether they used a condom during last anal sex.
Model Fitting and Hypothesis Testing
As described earlier, we began analyses with a preliminary model (Figure 1) in which age, race and problem drinking were used as exogenous control variables, childhood sexual abuse, anger, depression, and anxiety were modeled as both exogenous and endogenous variables, and sexual HIV risk and aggression were considered as endogenous variables. In this original model, all three control variables were correlated, error terms between anxiety, depression and anger were correlated, and error terms between risk and aggression were correlated. Model fit indices for this preliminary model were not good (χ2[1356]= 3720.721, p<.000; CFI=0.745 and RMSEA[90% CI]=0.065 [.061–.088]). Based on model modification indices, we added several error covariances within our three dimensions of affect (not shown), while retaining all proposed paths. Additions were made one at a time and were based on several criteria, taking into account the theoretical, statistical, and practical impact of each change. We examined all path coefficients and fit statistics after each addition, arriving at our final model when all remaining proposed changes no longer reasonably fit within our criteria. Compared to the preliminary model, our revised model (χ2[1300]= 2121.779, p<.000) had significantly better global fit (Δχ2[59] = 1598.342 p<.001) and substantially better local fit indices (CFI=0.905 and RMSEA[90% CI]=.044 [.041–.047]). Direct standardized path estimates are presented in Table 3.
Table 3.
Standardized direct path coefficients among all variables in the final SEM model
| Parameter | Beta | 95% CI | p |
|---|---|---|---|
| Age to CSA | .06 | 0.02 – 0.1 | .001 |
| Race to CSA | −.40 | −0.62 – −0.24 | .002 |
| CSA to Anger | .33 | 0.24 – 0.47 | .002 |
| CSA to Anxiety | .30 | 0.20 – .43 | .005 |
| CSA to Depression | .95 | 0.74 – 1.21 | .002 |
| Age to Anxiety | .02 | −0.01 – 0.03 | .16 |
| Age to Anger | −.01 | −0.04 – 0.03 | .76 |
| Age to Depression | .02 | −0.06 – .011 | .55 |
| Race to Depression | .61 | 0.18 – 1.12 | .009 |
| Race to Anxiety | .05 | −0.06 – 0.18 | .49 |
| Race to Anger | −.13 | −0.33 – 0.07 | .16 |
| Problem Drinking to Anger | .01 | −0.01 – 0.02 | .19 |
| Problem Drinking to Anxiety | .00 | −0.01 – 0.01 | .97 |
| Problem Drinking to Depression | .01 | −0.03 – 0.05 | .55 |
| Anger to Aggression | .08 | −0.11 – 0.22 | .46 |
| Anxiety to Aggression | .54 | −0.08 – 2.78 | .02 |
| Depression to Aggression | .00 | −0.35 – 0.10 | .91 |
| CSA to Aggression | .08 | −0.09 – 0.30 | .38 |
| Anger to HIV Risk | −.03 | −0.12 – 0.08 | .51 |
| Anxiety to HIV Risk | .22 | −0.09 – 0.82 | .02 |
| Depression to HIV Risk | −.01 | −0.07 – 0.06 | .92 |
| CSA to HIV Risk | .08 | −0.06 – 0.18 | .22 |
| Aggression to HIV Risk | .11 | −0.03 – 0.22 | .02 |
Note. Significant paths are bolded. For race, 0 = Black and 1 = White.
Consistent with Hypothesis 1, sexual aggression and sexual HIV risk were significantly associated based on a chi square test as well as in our final SEM model (β = .11, p = .02). Consistent with Hypothesis 2, CSA was significantly associated with sexual aggression and sexual HIV risk based on point biserial correlations (see Table 2); however, the direct pathways between CSA and sexual aggression (β = .08, p = .38) and CSA and sexual HIV risk (β = .08, p = .22) were not significant in our final SEM model. Hypothesis 3 predicted that trait negative affect would be associated with sexual aggression and sexual risk; this hypothesis received partial support. Sexual aggression demonstrated significant point biserial correlations with anxiety, anger, and depression, and sexual HIV risk demonstrated significant correlations with anxiety and depression. However, in the final SEM model only trait anxiety demonstrated a significant direct path to sexual aggression (β = .54, p = .02) and to sexual risk (β = .22, p = .02). Finally, Hypothesis 4 predicted that trait negative affect would mediate the relationship between CSA and sexual aggression and sexual HIV risk. This hypothesis was supported; there was a significant indirect effect of CSA on sexual HIV risk, β = .13 (95% CI = 0.02 – 0.39), p = .02, and a significant indirect effect of CSA on sexual aggression, β = 0.28 (95% CI = .09 – 1.16), p = .01.
DISCUSSION
In this study, we examined the association between two types of sexual risk behavior—sexual aggression and sexual HIV risk. Consistent with prior research (Peterson et al., 2010), we found that sexual aggression and HIV risk behaviors were related in our sample of heterosexual men from urban STI clinics, providing further evidence that sexual aggression can be conceptualized as one form of sexual risk-taking. This suggests that, if researchers are able to identify the shared risk factors for both HIV risk behavior and sexual aggression, primary prevention could potentially target both behaviors simultaneously.
We had hypothesized that CSA history and high levels of trait negative affect might represent two such shared risk factors. We found some support for these variables as shared correlates of sexual aggression and HIV risk. As in numerous past studies, CSA was associated with both sexual HIV risk and sexual aggression. Anxiety, anger, and depression were independent correlates of sexual aggression, and anxiety and depression were independent correlates of sexual HIV risk behavior. However, in the SEM model, anxiety was the only type of trait negative affect that was directly predictive of aggression and sexual HIV risk. Thus, anxiety, in particular, seems to be a risk factor for both types of sexual risk behavior. Indeed, in our model, trait anxiety helped to explain the relationship between CSA and sexual aggression and between CSA and sexual HIV risk.
Limitations
Before discussing possible implications of our results, several limitations should be noted. Results of this study were based entirely on self-report, and thus are prone to recall and social desirability biases. This may especially be true given that participants were completing the questionnaires in a public waiting room; although we instructed them to sit alone, they may have worried that others would see their responses. We attempted to minimize the impact of these biases through our choice of measures—for example, by choosing well-validated measures of negative affect, and by choosing a measure of sexual aggression that has been shown to be only weakly related to measures of social desirability.
Defining and measuring HIV/STI risk is challenging (e.g., see Jaccard, McDonald, Wan, Dittus, & Quinlan, 2002; Noar, Coyle, & Carlyle, 2000; Weinhardt, Forsyth, Carey, Jaworski, & Durant, 1998, for discussions), and thus our measure of HIV risk is inevitability imperfect. A strength of our HIV risk index is that it considers both number of partners and condom use, as neither unprotected sex with a single partner nor protected sex with multiple partners is likely to place men at high risk for HIV or other STIs. For our measure of condom use, we asked about condom use during last intercourse because there is evidence that participants have difficulty remembering condom use over longer time periods (Noar et al., 2000); however, because we only asked about condom use during last intercourse, it is possible that some men typically use condoms but did not use one at last intercourse and thus were wrongly classified as “high risk,” and it is possible that some men typically do not use condoms but did use one at last intercourse and thus were wrongly classified as “low risk.” It is also worth noting that these data were collected prior to the introduction of pharmacological Pre-Exposure Prophylaxis (PrEP). The use of PrEP renders condom-less sex less risky. However, participants in our study were largely low-income Black men, who were seeking services from free a STI clinic. Thus, it is quite possible that, even today, most of our participants would not have access to PrEP due to disparities in access related to income (Mansergh, Koblin, & Sullivan, 2012) and race (Calabrese, Earnshaw, Underhill, Hansen, & Dovidio, 2014).
Additionally, an important limitation of this study is its cross-sectional design. We examined the global associations among CSA, trait levels of negative affect proneness, and sexual risk and aggression. This design poses multiple problems with interpretation. First, it is not clear whether negative affect proceeds and contributes to sexual risk and aggression or whether it follows as a consequence of risky and aggressive behavior. Second, our design did not allow us to examine event-level associations between negative affect and the two kinds of sexual risk. Kalichman and Weinhardt (2001) particularly noted the need for event-level analyses of the association between negative affect and sexual risk among at-risk populations. Sexual risk and aggression may be influenced more by emotional states that occur immediately before the sexual acts than by trait levels of negative affect. Nevertheless, even at a global level, identifying a relationship between negative affect proneness and sexual risk and aggression may contribute to better identification of the men who are vulnerable to engaging in these sexual risk behaviors and may be a first step in pointing researchers and clinicians in the direction of effective prevention.
Because we recruited this sample from STI clinics in low-income urban neighborhoods, this was a high risk sample—high risk for STIs and, based on prior findings by Senn et al. (2006), high risk for CSA. The patterns of relationships among our variables of interest may have looked a bit different if we have examined them in a lower risk sample. Indeed, in the Crepaz and Marks (2001) meta-analysis, there was a stronger relationship between negative affect and sexual risk in high risk samples than in lower risk samples.
Our sample also was predominantly Black. In our final SEM model, race was significantly associated with CSA, with Black participants reporting more CSA than White participants, which is consistent with some prior research findings but not others (see Kenny & McEachern, 2000, for a review and discussion). Also, in our final model, race was significantly associated with depression, with White participants reporting greater trait depression than Black participants; this finding is consistent with a number of prior research findings (e.g., Breslau et al., 2006; Williams et al., 2007). Thus, relationships among the variables in our model may differ somewhat as a function of race and other demographic variables. Future research could explore this possibility.
This study also focused on the association between sexual aggression and sexual HIV risk behavior specifically among men who have sex with women. It is not clear whether these sexual risk behaviors also co-occur among men who have sex with men—a group at higher risk for HIV (Centers for Disease Control, 2017). In future studies, it would be beneficial to examine the association between sexual aggression and HIV risk among men who have sex with men.
Finally, it is important to note that the effect sizes for our significant results are fairly small. This highlights the fact that sexual risk behavior is complicated and likely multi-determined. Even CSA, which is a well-established risk factor for both sexual aggression and HIV risk behavior, was only weakly related to the sexual risk outcomes in the current study. On the one hand, this is good news, as it is a reminder that CSA does not inevitably or invariably lead to later sexual risk behavior. On the other hand, this means that additional research is needed to identify other important developmental risk factors for sexual aggression and HIV risk behavior in order to effectively target primary prevention at the highest risk groups of men.
Clinical and Research Implications
This study, along with prior research (Peterson et al., 2010) provides evidence of a relationship between sexual HIV risk behavior and sexual aggression. This suggests that men who sexually aggress against women are likely at high risk for HIV and other STIs; thus, they place their female victims at risk as well. Therefore, prevention interventions are particularly needed to target these doubly-risky men. Further, the association between sexual aggression and HIV risk behavior suggests that primary prevention programs potentially could be developed to simultaneously address both risk behaviors. However, before such dual-purpose interventions can be developed, a better understanding of the shared risk factors for sexual HIV risk and sexual aggression is needed.
In this and other studies, a history of CSA has emerged as one such shared risk factor. This points to the possible benefits of creating dual-purpose invention programs particularly targeting men who have experienced CSA. However, given that a history of CSA is not something that can, itself, be changed through intervention, more research is needed to address the mediators in the relationship between CSA history and adult sexual risk behaviors.
To that end, we found evidence that negative affect—particularly anxiety—helps to explain the relationship between CSA and sexual aggression and between CSA and sexual risk. Contrary to our hypotheses, in our SEM model, we did not find evidence for the mediating impact of other types of negative affect—namely depression or anger. Notably, though, several studies suggest that the STAI, which we used to measure anxiety in this study, may actually measure—not only anxiety—but more generalized negative affect, including depressed mood (Bados, Gomez-Benito, & Balaguer, 2010; Balsamo et al., 2013; Caci, Bayle, Dossios, Robert, & Boyer, 2003). Thus, in future studies, it may be useful to further examine the role of different types of negative affect on sexual aggression and sexual HIV risk.
The finding that anxiety is the strongest predictor of sexual aggression and sexual HIV risk is, perhaps, counterintuitive. For example, anxiety is often thought to inhibit sexual response specifically among individuals with sexual dysfunction, including erectile dysfunction (e.g., Barlow, 1986). To the extent that anxiety inhibits sexual response, it also might be expected to reduce or inhibit risky sexual behavior such as engaging in sex with multiple partners. Nevertheless, there is prior research to support the association between anxiety and sexual risk behaviors. Several researchers (Hoyle, Fejfar, & Miller, 2000; Rotheram-Borus et al., 1995) have suggested that anxiety and neuroticism are sometimes associated with sexual risk. And research (Bancroft, Janssen, Strong, Vakadinovic, & Long, 2003) has found that some men experience an increased drive for sexual activity during negative mood states—perhaps because they seek out sex as a way to relieve tension.
Similarly, the relationship between anxiety and sexual aggression may seem unexpected, given that there is research suggesting that men who engage in sexually aggressive behavior are high in antisocial or psychopathic personality traits, such as callousness (Kosson, Kelly, & White, 1997; Lalumiere & Quinsey, 1996; Zinzow & Thompson, 2014), which traditionally have been conceptualized as involving pathologically low levels of anxiety (Hare, 1996). From this perspective, sexually aggressive behavior might be expected to be “cold-blooded,” instrumental, or proactive rather than driven by strong emotion (see Dodge, 1991). However, anxiety has been shown to be associated with physical aggression—especially “hot-blooded” or reactive aggression—in prior studies (e.g., Fite, Raine, Stouthamer-Loeber, Loeber, & Pardini, 2009). Anxious attachment also has been shown to be associated with child sexual abuse perpetration among adolescent boys (Miner et al., 2014). Although the relationship between anxiety and sexual aggression in adult men has received limited research attention, it has been theorized that sexually aggressive men may be insecure and anxious about their relationships with women (Malamuth et al., 1995) and/or about their sexual performance (Peterson et al. 2010). This anxious, emotionally-aroused state may lead the men to respond impulsively and aggressively to perceived or feared sexual rejection. It also is possible, given the significant, but only moderately strong, association between anxiety and sexual aggression in this study, that there are at least two types of sexually aggressive men: (1) an anxious or reactive type and (2) a callous or proactive type (see also Peterson, Janssen, Goodrich, & Heiman, 2014). Future research could investigate these possibilities further. Understanding these pathways could be important for developing effective primary prevention strategies.
Finally, it is important to note that, in general, the relationship between anxiety and sexual response is quite complicated and may differ for different individuals. Anxiety—and related emotions such as worry and fear—seem to interfere with sexual arousal among those who are prone to sexual dysfunction, possibly because worry and rumination lead to distraction (e.g., Beck & Barlow, 1986; Hale & Strassberg, 1990; Nobre & Pinto-Gouveia, 2007). However, among those without sexual dysfunction, anxiety may facilitate sexual arousal, possibly because physiological anxiety responses are incorrectly perceived as sexual arousal (Dutton & Aaron, 1974) or because anxiety leads to a generalized physiological activation associated sympathetic arousal (e.g., Barlow, Sakheim, & Beck, 1983; Meston & Gorzalka, 1996; Peterson & Janssen, 2007). To further complicate current understandings, a recent study provided some preliminary evidence that, when exposed to an anxiety-inducing stimulus followed by an erotic stimulus in the laboratory, men with a history of sexual aggression exhibited greater sexual arousal than men without a history of sexual aggression (Craig, Peterson, Janssen, Goodrich, & Heiman, 2017), further illustrating that not all individuals’ sexual response is impacted by anxiety in the same way. Therefore, it is perhaps not surprising that the relationship between anxiety and sexual risk behaviors—sexual aggression and HIV risk—is similarly complicated. More research on the interrelationships among anxiety, sexual arousal, sexual aggression, and sexual HIV risk could be valuable.
In the meantime, though, our results suggest that helping men with a history of CSA to cope with their negative emotions—particularly their anxiety—in more adaptive ways may prove to be a useful avenue for preventing sexual aggression and sexual HIV risk behavior. There are multiple existing and empirically-supported psychological interventions to reduce negative affect and promote adaptive emotional coping; thus, this is a promising avenue for intervention. Interventions could include cognitive behavioral therapy or Mindfulness-Based Stress Reduction (Kabat-Zinn, 2003). However, it also is possible that very brief one-time interventions could be delivered onsite at STI clinics. For example, negative affect could be address through prescriptions for physical exercise (Salmon, 2001) or on-the-spot relaxation training (Manzoni, Pagnini, Castelnuovo, & Molinari, 2008). Future research could explore potential benefits of these interventions in reducing sexual aggression and HIV risk behavior in men at high risk for both—in particular, those with a CSA history and high trait levels of anxiety.
Conclusion
The association between sexually aggressive behavior and sexual HIV risk behavior suggests that there may be shared underlying risk factors for these two behaviors that could be targeted in a single primary prevention intervention. This study revealed that anxiety is one such shared risk factor. This is a promising target for intervention efforts because there are many existing psychological and pharmacological interventions to reduce anxiety. Further research examining how anxiety contributes to sexual risk may be fruitful in advancing prevention efforts.
Acknowledgments
FUNDING
This study was supported by a grant (R21HD055831; Zoё Peterson, PI) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). This article’s contents are solely the responsibility of the authors and do not necessarily represent the views of NICHD.
Footnotes
COMPLIANCE WITH ETHICAL STANDARDS
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
References
- Abbey A, Zawacki T, Buck PO, Clinton AM, McAuslan P. Sexual assault and alcohol consumption: What do we know about their relationship and what types of research are still needed? Aggression and Violent Behavior. 2004;9:271–303. doi: 10.1016/S1359-1789(03)00011-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amaro H, Raj A, Reed E. Women’s sexual health: The need for feminist analyses in public health in the decade of behavior. Psychology of Women Quarterly. 2001;25:324–334. doi: 10.1111/1471-6402.00032. [DOI] [Google Scholar]
- Arriola KRJ, Louden T, Doldren MA, Fortenberry RM. A meta-analysis of the relationship of child sexual abuse to HIV risk behavior among women. Child Abuse & Neglect. 2005;29:725–746. doi: 10.1016/j.chiabu.2004.10.014. [DOI] [PubMed] [Google Scholar]
- Bados A, Gomez-Benito J, Balaguer G. The State-Trait Anxiety Inventory, Trait Version: Does it really measure anxiety? Journal of Personality Assessment. 2010;92:560–567. doi: 10.1080/00223891.2010.513295. [DOI] [PubMed] [Google Scholar]
- Balsamo M, Romanelli R, Innamorati M, Ciccarese G, Carlucci L, Saggino A. The State-Trait Anxiety Inventory: Shadows and lights on its construct validity. Journal of Psychopathology and Behavior Assessment. 2013;25:475–486. doi: 10.1007/s10862-013-9354-5. [DOI] [Google Scholar]
- Bancroft J, Janssen E, Strong D, Carnes L, Vukadinovic Z, Long JS. The relation between mood and sexuality in heterosexual men. Archives of Sexual Behavior. 2003;32:217–230. doi: 10.1023/A:1023409516739. [DOI] [PubMed] [Google Scholar]
- Barlow DH. Causes of sexual dysfunction: The role of anxiety and cognitive interference. Journal of Consulting and Clinical Psychology. 1986;54:140–148. doi: 10.1037/0022-006X.54.2.140. [DOI] [PubMed] [Google Scholar]
- Barlow DH, Sakheim DK, Beck JG. Anxiety increases sexual arousal. Journal of Abnormal Psychology. 1983;92:49–54. doi: 10.1037/0021-843X.92.1.49. [DOI] [PubMed] [Google Scholar]
- Beck JG, Barlow DH. The effects of anxiety and attentional focus on sexual responding I: Physiological patterns in erectile dysfunction. Behaviour Research and Therapy. 1986;24:9–17. doi: 10.1016/0005-7967(86)90144-0. [DOI] [PubMed] [Google Scholar]
- Becker JV, Kaplan MS, Tenke CE, Tartaglini A. The incidence of depressive symptomatology in juvenile sex offenders with a history of abuse. Child Abuse and Neglect. 1991;14:531–536. doi: 10.1016/0145-2134(91)90037-E. [DOI] [PubMed] [Google Scholar]
- Bensley LS, Van Eenwyk J, Simmons KW. Self-reported childhood sexual and physical abuse and adult HIV-risk behaviors and heavy drinking. American Journal of Preventative Medicine. 2000;18:151–158. doi: 10.1016/S0749-3797(99)00084-7. [DOI] [PubMed] [Google Scholar]
- Berstein, Ahluvalia T, Pogge D, Handelsman L. Validity of the Childhood Trauma Questionnaire in an adolescent psychiatric population. Journal of the American Academy of Child & Adolescent Psychiatry. 1997;36:340–348. doi: 10.1097/00004583-199703000-00012. [DOI] [PubMed] [Google Scholar]
- Berstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Zule W. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse and Neglect. 2003;27:169–190. doi: 10.1037/0893-164X.21.2.233. [DOI] [PubMed] [Google Scholar]
- Blythe MJ, Fortenberry JD, Temkit M, Tu W, Orr DP. Incidence and correlates of unwanted sex in relationships of middle and late adolescent women. Archives of Pediatric and Adolescent Medicine. 2006;160:591–595. doi: 10.1001/archpedi.160.6.591. [DOI] [PubMed] [Google Scholar]
- Bollen KA. Structural equations with latent variables. New York, NY: Wiley; 1989. [Google Scholar]
- Bollen KA, Pearl J. Eight myths about causality and structural equation models. In: Morgan SL, editor. Handbook of causal analysis for social research. Dordrecht, Netherlands: Springer; 2013. pp. 301–328. [Google Scholar]
- Breslau J, Aguilar-Gaxiola S, Kendler KS, Su M, Williams D, Kessler RC. Specifying race-ethnic differences in risk for psychiatric disorder in a US national sample. Psychological Medicine. 2006;36:57–68. doi: 10.1017/S0033291705006161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown MW, Cudeck R. Alternative ways of assessing model fit. In: Long KA, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Brown TA, Chorpita BF, Barlow DH. Structural relationships among dimensions of the DSM-IV anxiety and mood disorders and dimensions of negative affect, positive affect, and autonomic arousal. Journal of Abnormal Psychology. 1998;107:179–192. doi: 10.1037/0021-843X.107.2.179. [DOI] [PubMed] [Google Scholar]
- Brown A, Finkelhor D. Impact of child sexual abuse: A review of the research. Psychological Bulletin. 1986;99:66–77. doi: 10.1037/0033-2909.99.1.66. [DOI] [PubMed] [Google Scholar]
- Brown LK, Tolou-Shams M, Lescano C, Houck C, Zeidman J, Project SHIELD Study Group Depressive symptoms as a predictor of sexual risk among African American adolescents and young adults. Journal of Adolescent Health. 2006;39:444.e1–444.e8. doi: 10.1016/j.jadohealth.2006.01.015. [DOI] [PubMed] [Google Scholar]
- Byrne BM. Structural equation modeling with AMOS: Basic concepts, applications, and programming. New York, NY: Routledge; 2009. [Google Scholar]
- Caci H, Bayle FJ, Dossios C, Robert P, Boyer P. The Speilberger trait anxiety inventory measures more than anxiety. European Psychiatry. 2003;18:394–400. doi: 10.1016/j.eurpsy.2003.05.003. [DOI] [PubMed] [Google Scholar]
- Calabrese SK, Earnshaw VA, Underhill K, Hansen NB, Dovidio JF. The impact of patient race on clinical decisions related to prescribing HIV pre-exposure prophylaxis (PrEP): Assumptions about sexual risk compensation and implications for access. AIDS and Behavior. 2014;18:226–240. doi: 10.1007/s10461-013-0675-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldwell TM, Rodgers B, Jorm AF, Christensent H, Jacomb PA, Korten AE, Lynskey MT. Patterns of association between alcohol consumption and symptoms of depression and anxiety in young adults. Addiction. 2002;97:583–594. doi: 10.1046/j.1360-0443.2002.00092.x. [DOI] [PubMed] [Google Scholar]
- Caldwell TM, Rodgers B, Jorm AF, Christensen H, Jacomb PA, Lynskey MT. Patterns of association between alcohol consumption and symptoms of depression and anxiety in young adults. Addiction. 2002;97:583–594. doi: 10.1046/j.1360-0443.2002.00092.x. [DOI] [PubMed] [Google Scholar]
- Casey EA, Beadnell B, Lindhorst TP. Predictors of sexually coercive behavior in a nationally representative sample of adolescent males. Journal of Interpersonal Violence. 2009;24:1129–1147. doi: 10.1177/0886260508322198. [DOI] [PubMed] [Google Scholar]
- Casey EA, Masters NT, Beadnell B, Hoppe MJ, Morrison DM, Wells EA. Predicting sexual assault perpetration among heterosexually active young men. Violence Against Women. 2017;23:2–37. doi: 10.1177/1077801216634467. [DOI] [PubMed] [Google Scholar]
- Casey EA, Querna K, Masters NT, Beadnell B, Wells EA, Morrison DM. Patterns of intimate partner violence and sexual risk behavior among young heterosexually active men. Journal of Sex Research. 2016;53:239–250. doi: 10.1080/00224499.2014.1002125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control. HIV among men in the United States. 2017 Retrieved from https://www.cdc.gov/hiv/group/gender/men/
- Clement U. Psychological correlates of unprotected intercourse among HIV-positive gay men. Journal of Psychology and Human Sexuality. 1992;5:133–155. doi: 10.1300/J056v05n01_08. [DOI] [Google Scholar]
- Cooper CL, Murphy WD, Haynes MR. Characteristics of abused and nonabused adolescent sexual offenders. Sexual Abuse: A Journal of Research and Treatment. 1996;8:105–119. doi: 10.1007/BF02258004. [DOI] [Google Scholar]
- Cooper ML, Agocha VB, Sheldon MS. A motivational perspective on risky behaviors: The role of personality and affect regulatory processes. Journal of Personality. 2000;68:1059–1088. doi: 10.1111/1467-6494.00126. [DOI] [PubMed] [Google Scholar]
- Craig AN, Peterson ZD, Janssen E, Goodrich D, Heiman JR. Affect and sexual responsivity in men with and without a history of sexual aggression. Journal of Sex Research. 2017 doi: 10.1080/00224499.2017.1301357. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crepaz N, Marks G. Are negative affective states associated with HIV sexual risk behaviors? A meta-analytic review. Health Psychology. 2001;20:291–299. doi: 10.1037/0278-6133.20.4.291. [DOI] [PubMed] [Google Scholar]
- Davis KC, Danube CL, Stappenbeck CA, Norris J, George WH. Background predictors and event-specific characteristics of sexual aggression incidents: The roles of alcohol and other factors. Violence Against Women. 2015;21:997–1017. doi: 10.1177/1077801215589379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis KC, Kiekel PA, Schraufnagle TJ, Norris J, George WH, Kajumulo KF. Men’s alcohol intoxication and condom use during sexual assault perpetration. Journal of Interpersonal Violence. 2012;27:2790–2806. doi: 10.1177/0886260512438277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dodge KA. The structure and function of reactive and proactive aggression. In: Pepler DJ, Rubin KH, editors. The development and treatment of childhood aggression. Hillsdale, NJ: Lawrence Erlbaum Associates; 1991. pp. 201–218. [Google Scholar]
- Douglas SC, Martinko MJ. Exploring the role of individual differences in the prediction of workplace aggression. Journal of Applied Psychology. 2001;86:547–559. doi: 10.1037/0021-9010.86.4.547. [DOI] [PubMed] [Google Scholar]
- Dutton DG, Aaron AP. Some evidence for heightened sexual attraction under conditions of high anxiety. Journal of Personality and Social Psychology. 1974;30:510–517. doi: 10.1037/h0037031. [DOI] [PubMed] [Google Scholar]
- Eckhardt C, Norlander B, Deffenbacher J. The assessment of anger and hostility: A critical review. Aggression and Violent Behavior. 2004;9:17–43. doi: 10.1016/S1359-1789(02)001167. [DOI] [Google Scholar]
- Fite PJ, Raine A, Stouthamer-Loeber M, Loeber R, Pardini DA. Reactive and proactive aggression in adolescent males: Examining differential outcomes 10 years later in early adulthood. Criminal Justice Behavior. 2009;37:141–157. doi: 10.1177/0093854809353051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guttmacher S, Lieberman L, Ward D, Freudenberg N, Radosh A, Des Jarlais D. Condom availability in New York City public high schools: Relationships to condom use and sexual behavior. American Journal of Public Health. 1997;87:1427–1433. doi: 10.2105/AJPH.87.9.1427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hare RD. Psychopathy: A clinical construct whose time has come. Criminal Justice and Behavior. 1996;23(1):25–54. doi: 10.1177/0093854896023001004. [DOI] [Google Scholar]
- Hale VE, Strassberg DS. The role of anxiety on sexual arousal. Archives of Sexual Behavior. 1990;19:569–581. doi: 10.1007/BF01542466. [DOI] [PubMed] [Google Scholar]
- Hall GC, Hirschman R. Toward a theory of sexual aggression: A quadripartite model. Journal of Consulting and Clinical Psychology. 1991;59:662–669. doi: 10.1037//0022-006X.59.5.662. [DOI] [PubMed] [Google Scholar]
- Hoffman S, O’Sullivan LF, Harrison A, Dolezal C, Monroe-Wise A. HIV risk behaviors and the context of sexual coercion in young adults’ sexual interactions: Results from a diary study in rural South Africa. Sexually Transmitted Diseases. 2006;33:52–58. doi: 10.1097/01.olq.0000187198.77612.d8. [DOI] [PubMed] [Google Scholar]
- Homma Y, Wang N, Saewyc E, Kishor N. The relationship between sexual abuse and risky sexual behavior among adolescent boys: A meta-analysis. Journal of Adolescent Health. 2012;51:18–24. doi: 10.1016/j.jadohealth.2011.12.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howells K, Day A, Wright S. Affect, emotions, and sex offending. Psychology, Crime, & Law. 2004;10:179–195. doi: 10.1080/10683160310001609988. [DOI] [Google Scholar]
- Hoyle RH, Fejfar MC, Miller JD. Personality and sexual risk taking: A quantitative review. Journal of Personality. 2000;68:1203–1231. doi: 10.1111/1467-6494.00132. [DOI] [PubMed] [Google Scholar]
- Jaccard J, McDonald R, Wan CK, Bittus PJ, Quinlan S. The accuracy of self-reports of condom use and sexual behavior. Journal of Applied Social Psychology. 2002;32:1863–1905. doi: 10.1111/j.1559-1816.2002.tb00263.x. [DOI] [Google Scholar]
- Kabat-Zinn J. Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice. 2003;10:144–156. doi: 10.1093/clipsy.bpg016. [DOI] [Google Scholar]
- Kalichman SC, Weinhardt L. Negative affect and sexual risk behavior: Comment on Crepaz and Marks (2001) Health Psychology. 2001;20:300–301. doi: 10.1037/0278-6133.20.4.300. [DOI] [PubMed] [Google Scholar]
- Kelly JA, Murphy DA, Bahr GR, Koob JJ, Morgan MG, St Lawrence JS. Factors associated with severity of depression and high-risk sexual behavior among persons diagnosed with human immunodeficiency virus (HTV) infection. Health Psychology. 1993;12:215–219. doi: 10.1037/0278-6133.12.3.215. [DOI] [PubMed] [Google Scholar]
- Kenny DA. Correlation and causality. New York, NY: Wiley; 1979. [Google Scholar]
- Kenny MC, McEachern AG. Racial, ethnic, and cultural factors of childhood sexual abuse: A selected review of the literature. Clinical Psychology Review. 2000;20:905–922. doi: 10.1016/S0272-7358(99)00022-7. [DOI] [PubMed] [Google Scholar]
- Koblin BA, Grant S, Frye V, Superak H, Sanchez B, Lucy D, Frank I. HIV sexual risk and syndemics among women in three urban areas in the United States: Analysis from HVTN 906. Journal of Urban Health. 2015;92:572–583. doi: 10.1007/s11524-015-9944-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koss MP, Abbey A, Campbell R, Cook S, Norris J, White J. Revising the SES: A collaborative process to improve assessment of sexual aggression and victimization. Psychology of Women Quarterly. 2007;31:357–370. doi: 10.1111/j.1471-6402.2007.00385.x. [DOI] [Google Scholar]
- Kossen DS, Kelly JC, White JW. Psychopathy-related traits predict self-reported sexual aggression among college men. Journal of Interpersonal Violence. 1997;12:241–254. doi: 10.1177/088626097012002006. [DOI] [Google Scholar]
- Krahe B, Berger A. Gendered pathways from child sexual abuse to sexual aggression victimization and perpetration in adolescence and young adulthood. Child Abuse & Neglect. 2017;63:261–272. doi: 10.1016/j.chiabu.2016.10.004. [DOI] [PubMed] [Google Scholar]
- Lalumiere ML, Quinsey VL. Sexual deviance, antisociality, mating effort, and the use of sexually coercive behaviors. Personality and Individual Differences. 1996;21:33–48. doi: 10.1016/0191-8869(96)00059-1. [DOI] [Google Scholar]
- Lambie I, Seymour F, Lee Adams. Resiliency in the victim-offender cycle in male sexual abuse. Sexual Abuse: A Journal of Research and Treatment. 2002;14:31–48. doi: 10.1023/A:1013077426928. [DOI] [PubMed] [Google Scholar]
- Leigh BC, Stall R. Substance use and risky sexual behavior for exposure to HIV: Issues in methodology, interpretation, and prevention. American Psychologist. 1993;48:1035–1045. doi: 10.1037/0003-066X.48.10.1035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lloyd S, Operario D. HIV risk among men who have sex with men who have experienced childhood sexual abuse: Systematic review and meta-analysis. AIDS Education and Prevention. 2012;24:228–241. doi: 10.1521/aeap.2012.24.3.228. [DOI] [PubMed] [Google Scholar]
- Loehlin JC. Latent variable models: An introduction to factor, path, and structural analysis. 2nd. Hillsdale, NJ: Erlbaum; 1992. [Google Scholar]
- Loh C, Gidycz CA. A prospective analysis of the relationship between childhood sexual victimization and perpetration of dating violence and sexual assault in adulthood. Journal of Interpersonal Violence. 2006;21:732–749. doi: 10.1177/0886260506287313. [DOI] [PubMed] [Google Scholar]
- Lykins AD, Janssen E, Graham CA. The relationship between negative mood and sexuality in heterosexual college women and men. Journal of Sex Research. 2006;43:136–143. doi: 10.1080/00224490609552308. [DOI] [PubMed] [Google Scholar]
- Lyn TS, Burton DL. Attachment, anger, and anxiety of male sexual offenders. Journal of Sexual Aggression. 2005;11:127–137. doi: 10.1080/13552600500063682. [DOI] [Google Scholar]
- Malamuth NM, Linz D, Heavey CL, Barnes G, Acker M. Using the Confluence Model of sexual aggression to predict men’s conflict with women: A 10-year follow-up study. Journal of Personality and Social Psychology. 1995;69:353–369. doi: 10.1037/0022-3514.69.2.353. [DOI] [PubMed] [Google Scholar]
- Malamuth NM, Sockloskie RJ, Koss MP, Tanaka JS. Characteristics of aggressors against women: Testing a model using a national sample of college students. Journal of Consulting and Clinical Psychology. 1991;59:670–681. doi: 10.1037/0022-006X.59.5.670. [DOI] [PubMed] [Google Scholar]
- Mammen OK, Kolko DJ, Pilkonis PA. Negative affect and parental aggression in child physical abuse. Child Abuse& Neglect. 2002;26:407–424. doi: 10.1016/S0145-2134(02)00316-2. [DOI] [PubMed] [Google Scholar]
- Mansergh G, Koblin BA, Sullivan PS. Challenges for HIV pre-exposure prophylaxis among men who have sex with men in the United States. PLOS Medicine. 2012;9:e1001286. doi: 10.1371/journal.pmed.1001286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manzoni GM, Pagnini F, Castelnuovo G, Molinari E. Relaxation training for anxiety: A ten-years systematic review with meta-analysis. BMC Psychiatry. 2008;8:41. doi: 10.1186/1471-244X-8-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Margolin G, John RS, Gleberman L. Affective responses to conflictual discussions in violent and nonviolent couples. Journal of Consulting and Clinical Psychology. 1988;56:24–33. doi: 10.1037/0022-006X.56.1.24. [DOI] [PubMed] [Google Scholar]
- Martin SL, Curtis S. Gender-based violence and HIV/AIDS: Recognising links and acting on evidence. Lancet. 2004;363:1410–1411. doi: 10.1016/S0140-6736(04)16133-3. [DOI] [PubMed] [Google Scholar]
- Merrill LL, Thomsen CJ, Gold SR, Milner JS. Childhood abuse and premilitary sexual assault in navy recruits. Journal of Consulting and Clinical Psychology. 2001;69:252–261. doi: 10.1037/0022-006X.69.2.252. [DOI] [PubMed] [Google Scholar]
- Meston CM, Gorzalka BB. Differential effects of sympathetic activation on sexual arousal in sexually dysfunctional and functional women. Journal of Abnormal Psychology. 1996;105:582–591. doi: 10.1037/0021-843X.105.4.582. [DOI] [PubMed] [Google Scholar]
- Metzger RL. A reliability and validity study of the State-Trait Anxiety Inventory. Journal of Clinical Psychology. 1976;32:276–278. doi: 10.1002/1097-4679(197604)32:2<276::AID-JCLP2270320215>3.0.CO;2-G. [DOI] [Google Scholar]
- Metzler CW, Noell J, Biglan A. The validation of a construct of high-risk sexual behavior in heterosexual adolescents. Journal of Adolescent Research. 1992;7:233–249. doi: 10.1177/074355489272007. [DOI] [Google Scholar]
- Meyer C, Leung N, Waller G, Perkins S, Paice N, Mitchell J. Anger and bulimic psychopathology: Gender differences in a nonclinical group. International Journal of Eating Disorders. 2005;37:69–71. doi: 10.1002/eat.20038. [DOI] [PubMed] [Google Scholar]
- Miner MH, Swinburne Romine R, Robinson BE, Berg D, Knight RA. Anxious attachment, social isolation, and indicators of sex drive and compulsivity: Predictors of child sexual abuse perpetration in adolescent males? Sexual Abuse: A Journal of Research and Treatment. 2014;28:132–153. doi: 10.1177/1079063214547585. [DOI] [PubMed] [Google Scholar]
- Murnen SK, Wright C, Kaluzny G. If “boys will be boys,” then girls will be victims? A meta-analytic review of the research that relates masculine ideology to sexual aggression. Sex Roles. 2002;46:359–375. doi: 10.1023/A:1020488928736. [DOI] [Google Scholar]
- Mustanski B. The influence of state and trait affect on HIV risk behaviors: A daily diary study of MSM. Health Psychology. 2007;26:618–626. doi: 10.1037/0278-6133.26.5.618. [DOI] [PubMed] [Google Scholar]
- Nemoto T, Foster K, Brown LS. Effect of psychological factors on risk behavior of human immunodeficiency virus (HIV) infection among intravenous drug users (IVDUs) International Journal of the Addictions. 1991;26:441–456. doi: 10.3109/10826089109058896. [DOI] [PubMed] [Google Scholar]
- Noar SM, Cole C, Carlyle K. Condom use measurement in 56 studies of sexual risk behavior: Review and recommendations. Archives of Sexual Behavior. 2006;35:327–345. doi: 10.1007/s10508-006-9028-4. [DOI] [PubMed] [Google Scholar]
- Nobre PJ, Pinto-Gouveia J. Cognitions, emotions, and sexual response: Analysis of the relationship among automatic thoughts, emotional responses, and sexual arousal. Archives of Sexual Behavior. 2007;37:652–661. doi: 10.1007/s10508-007-9258-0. [DOI] [PubMed] [Google Scholar]
- O’Leary A, Purcell D, Remien RH, Gomez C. Childhood sexual abuse and sexual transmission risk behaviour among HIV-positive men who have sex with men. AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIV. 2003;15:17–26. doi: 10.1080/0954012021000039725. [DOI] [PubMed] [Google Scholar]
- Parkhill MR, Pickett SM. Difficulties in emotion regulation as a mediator of the relationship between child sexual abuse victimization and sexual aggression perpetration in male college students. Journal of Child Sexual Abuse. 2016;25:674–685. doi: 10.1080/10538712.2016.1205161. [DOI] [PubMed] [Google Scholar]
- Paul JP, Catania J, Pollack L, Stall R. Understanding childhood sexual abuse as a predictor of sexual risk-taking among men who have sex with men: The Urban Men’s Health Study. Child Abuse & Neglect. 2001;25:557–584. doi: 10.1016/S0145-2134(01)00226-5. [DOI] [PubMed] [Google Scholar]
- Pearl J. Causality: Models, reasoning, and inference. Cambridge, UK: Cambridge University Press; 2000. [Google Scholar]
- Perkins DO, Leserman J, Murphy C, Evans DL. Psychosocial predictors of high-risk sexual behaviour among HIV-negative homosexual men. AIDS Education and Prevention. 1993;5:141–152. [PubMed] [Google Scholar]
- Peterson ZD, Janssen E. Ambivalent affect and sexual response: The impact of co-occurring positive and negative emotions on subjective and physiological sexual responses to erotic stimuli. Archives of Sexual Behavior. 2007;36:793–807. doi: 10.1007/s10508-006-9145-0. [DOI] [PubMed] [Google Scholar]
- Peterson ZD, Janssen E, Goodrich D, Heiman JR. Physiological reactivity in a community sample of sexually aggressive young men: A test of competing hypotheses. Aggressive Behavior. 2014;40:152–164. doi: 10.1002/ab.21512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson ZD, Janssen E, Heiman JR. The association between sexual aggression and HIV risk behavior in heterosexual men. Journal of Interpersonal Violence. 2010;25:538–556. doi: 10.1177/0886260509334414. [DOI] [PubMed] [Google Scholar]
- Plehn K, Peterson RA. Anxiety sensitivity as a predictor of the development of panic symptoms, panic attacks, and panic disorder: A prospective study. Anxiety Disorders. 2002;16:455–474. doi: 10.1016/S0887-6185(02)00129-9. [DOI] [PubMed] [Google Scholar]
- Prochaska JJ, Spring B, Nigg CR. Multiple health behavior change research: An introduction and overview. Prevention Medicine. 2008;46:181–188. doi: 10.1016/j.ypmed.2008.02.001. doi:10.1016%2Fj.ypmed.2008.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ramrakha S, Caspi A, Dickson N, Moffitt TE, Paul C. Psychiatric disorders and risky sexual behavior in young adulthood: Cross sectional study in birth cohort. BMJ. 2000;321:263. doi: 10.1136/bmj.321.7256.263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reisner SL, Hughto JMW, Pardee D, Sevelius J. Syndemics and gender affirmation: HIV sexual risk in female-to-male trans masculine adults reporting sexual contact with cisgender males. International Journal of STDs and AIDS. 2016;27:955–966. doi: 10.1177/0956462415602418. doi: 10.1177%2F0956462415602418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romano E, De Luca RV. Male sexual abuse: A review of effects, abuse characteristics, and links with later functioning. Aggression and Violent Behavior. 2001;6:55–78. doi: 10.1016/S1359-1789(99)00011-7. [DOI] [Google Scholar]
- Rotheram-Borus MJ, Rosario M, Reid H, Kooperman C. Predicting patterns of sexual acts among homosexual and bisexual youths. American Journal of Psychiatry. 1995;152:588–595. doi: 10.1176/ajp.152.4.588. [DOI] [PubMed] [Google Scholar]
- Salmon P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: A unifying theory. Clinical Psychology Review. 2001;21:33–61. doi: 10.1016/S0272-7358(99)00032-X. [DOI] [PubMed] [Google Scholar]
- Scott CF, Owens LA, Stecker HL. Exploring the darkside of courtship: A test of a model of male premarital sexual aggressiveness. Journal of Marriage and the Family. 1993;55:469–479. [Google Scholar]
- Senn TE, Carey MP, Vanable PA, Coury-Doniger P, Urban MA. Childhood sexual abuse and sexual risk behaviour among men and women attending a sexually transmitted disease clinic. Journal of Consulting and Clinical Psychology. 2006;74:720–731. doi: 10.1037/0022-006X.74.4.720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shearer CL, Hosterman SJ, Gillen MM, Lefkowitz ES. Are traditional gender role attitudes associated with risky sexual behavior and condom-related beliefs? Sex Roles. 2005;52:311–324. doi: 10.1007/s11199-005-2675-4. [DOI] [Google Scholar]
- Spielberger CD. Manual for the State Trait Anger Expression Inventory (STAXI) Odessa, FL: Psychological Assessment Resources; 1988. [Google Scholar]
- Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press; 1970. [Google Scholar]
- Strang ET, Peterson ZD, Hill YN, Heiman JR. Discrepant responding across self-report measures of men’s coercive and aggressive sexual strategies. Journal of Sex Research. 2013;50:458–469. doi: 10.1080/00224499.2011.646393. [DOI] [PubMed] [Google Scholar]
- Struckman-Johnson C, Struckman-Johnson D, Anderson PB. Tactics of sexual coercion: When men and women won’t take no for an answer. Journal of Sex Research. 2003;40:76–86. doi: 10.1080/00224490309552168. [DOI] [PubMed] [Google Scholar]
- Testa M, Hoffman JH, Lucke JF, Pagnan CE. Measuring sexual aggression perpetration in college men: A comparison of two measures. Psychology of Violence. 2015;5:285–293. doi: 10.1037/a0037584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson D, Clark LA. Affects separable and inseparable: On the hierarchical arrangement of the negative affects. Journal of Personality and Social Psychology. 1992;62:489–505. doi: 10.1037/0022-3514.62.3.489. [DOI] [Google Scholar]
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology. 1988;54:1063–1070. doi: 10.1037/0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- Watson D, Tellegen A. Toward a consensual structure of mood. Psychological Bulletin. 1985;98:219–235. doi: 10.1037/0033-2909.98.2.219. [DOI] [PubMed] [Google Scholar]
- Weinhardt LS, Forsyth AD, Carey MP, Jaworski BC, Durant LE. Reliability and validity of self-report measures of HIV-related sexual behaviour: Progress since 1990 and recommendations for research and practice. Archives of Sexual Behavior. 1998;27:155–180. doi: 10.1023/A:1018682530519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White JW, Smith PH. Sexual assault perpetration and reperpetration: From adolescence to young adulthood. Criminal Justice and Behavior. 2004;31:182–202. doi: 10.1177/0093854803261342. [DOI] [Google Scholar]
- Williams DR, Gonzalez HM, Neighbors H, Nesse R, Abelson JM, Sweetman J, Jackson JS. Prevalence and distribution of major depressive disorder in African Americans, Caribbean blacks, and non-Hispanic whites: Results from the National Survey of American Life. Archives of General Psychiatry. 2007;64:305–315. doi: 10.1001/archpsyc.64.3.305. [DOI] [PubMed] [Google Scholar]
- Yates E, Barbaree HE, Marshall WL. Anger and deviant sexual arousal. Behavior Therapy. 1984;15:287–294. doi: 10.1016/S0005-7894(84)80031-3. [DOI] [Google Scholar]
- Zemore R, Fischer DG, Garratt LS, Miller C. The depression proneness rating scale: Reliability, validity, and factor structure. Current Psychology. 1990;9:255–263. doi: 10.1007/BF02686863. [DOI] [Google Scholar]