

Abstract
Introduction: Non-ablative fractional erbium-doped glass 1540 nm and fractional ablative 10600 nm carbon dioxide lasers are regarded as effective modalities for treating acne atrophic scars. In this study, we aimed to compare the effectiveness of fractional CO2 laser and fractional nonablative 1540 nm erbium doped glass laser in treating post acne atrophic scars in Egyptian patients.
Methods: Fifty-eight patients complaining of moderate and severe acne atrophic scars were randomly divided into 2 groups of 29 patients each. Both groups were subjected to 4 treatment sessions with 3 weeks interval and were followed up for 3 months. In group A, enrolled patient sreceived C2 laser, while in group B, patients were treated with 1540 nm erbium glass fractional laser.
Results: Clinical assessment revealed that the mean grades of progress and improvement were higher with fractional 10600 nm CO2 laser but with non-significant difference between both treatments (P = 0.1). The overall patients’ satisfaction with both lasers were not significantly different (P = 0.44).
Conclusion: Both fractional ablative CO2 and fractional non-ablative erbium glass lasers are good modalities for treating acne scars with a high efficacy and safety profile and good patient satisfaction. The fractional ablative laser showed higher efficacy while non-ablative laser offered less pain and shorter downtime.
Keywords: Acne scars, Ablative laser, Fractional laser
Introduction
Acne is a multifactoral condition that affects 80% of people during their second to fourth decades, moreover, 5% of old people can still experience acne.1 Comedone formation and hyperkeratinization remain to be the principal culprits in acne illicitation.2 Depressed atrophic scars develop due to collagen breakdown following skin conditions such as cystic acne and varicella. Trying to hide these scars with cosmetics frequently exacerbate their appearance by amplifying the textural variety of the skin. A number of treatments to improve the appearance of atrophic scars were employed in literature with different degrees of satisfaction.3
Safety and efficacy of fractional photothermolysis had been established since its introduction in 2003 in a number of skin conditions including but not only acne, scars, pigmentations and wrinkles.4
Fractional technology thermolysis was introduced to decrease the side effects and downtime of the ablative laser technologies, and at the same time improve on the comparatively less effective non-ablative lasers. The energy columns introduced to the skin creates columns of injury called microthermal zones (MTZs). Healthy untreated skin fractions provide a source of rapid healing and repair to the coagulated zones removing the necrotic debris.5
The distinctive recovery mechanism following fractional photothermolysis ensures an early patient recovery with less adverse events. Multiple treatments are usually required since the coverage area of skin ranges from 5% to 40%.6
The non-ablative erbium doped fractional lasers are used in many skin conditions owing to its tendency to preserve the epidermal functions and reduce the side effects, resulting in faster recovery.1–4 Nevertheless, more than one session is required to provide a satisfactory outcome.7
Studies on the safety and efficacy of this technology among Egyptians are limited. Our study design aimed at comparing the effectiveness of ablative fractional CO2 and non-ablative 1540 nm erbium doped glass fractional technologies in improving and treating atrophic scars in Egyptian skin tone.
Methods
Fifty-eight patients (39 females, 19 males, of skin types II-IV, aged 18-45) who had to fulfill the criteria of presenting with moderate to severe atrophic facial acne scars were recruited as of June 2011 to October 2013. Scar grading system was used to determine the degree of post acne scars. Approval of the ethical committee of Al-Azhar University was first obtained. All recruited participants were advised to sign a consent form before they were enrolled into the study and before starting any laser sessions. Exclusion criteria included those less than 18 years of age, patients with active viral or bacterial infections, pregnant females and anyone with a scar history. Randomization divided the patients into 2 groups of 29 patients each. In group A, enrolled participants received sessions with fractional 10 600 nm carbon dioxide laser while in group B, patients were treated with 1540 nm Erbium glass fractional laser.
Treatment
Treatment in one group of the enrolled patients was carried out with the ablative fractional CO2 laser (SmartXide DOT, Deka, Firenze, Italy), while the other half of patients received treatment with the non-ablative fractional erbium-doped glass 1540 nm laser (Icon, Cynosure, USA). Gentle face cleansing was followed by application of topical EMLA cream (AstraZeneca AB, Sodertalje, Sweden) for 60 minutes before starting the laser session. Those with history of herpes infection received prophylactic antiviral medication for 3 days prior to the laser procedure.
The 2 groups received 4 treatment sessions with a 3 weeks free interval between every session. The energy settings of the fractional 10 600 nm CO2 laser ranged from 10-15 W, with 500-1000 µs dwell time, stack 2 and spacing of 700 µm. The erbium group treatment settings consisted of 4 passes with pulse energy of 50-60 mJ⁄cm2 with XD Microlens and 15 ms pulse duration. After treatment, patients applied a moisturizer and sunscreen (SPF 50+). Patients were remotely followed up through phone call on the same and next day after treatment to document any side effect or adverse event.
Evaluation
Two blinded dermatologists determined the patients improvement using a 4-grade evaluation scale in which grade 1 would show less than 25% improvement; grade 2 showing 26% to 50% improvement; with grade 3 showing 51% to 75% improvement; while grade 4, with more than 75% improvement denoted near to full recovery. The 2 dermatologists did the assessment using pretreatment photographs and post treatment photographs
Subjective assessment was determined using a 4-grade satisfaction scale, patients were classified into very satisfied, only satisfied, slightly satisfied or completely unsatisfied. Moreover side effects were followed and recorded for up to 3 months after the last laser session. Pain that accompanied the laser sessions was evaluated using a 10-point score with 0 denoting “absent pain” and 10 denoting “severe pain.”
Statistical Analysis
Statistical evaluation for this study was completed using SPSS for Windows software (SPSS Inc., Chicago, IL, USA, version 20). P < 0.05 was considered by investigators to be statistically significant.
Results
All patients recruited successfully completed the full length of the study of 4 laser treatments and were followed up afterwards for 3 more months. Three months after the last laser procedure with fractional 10 600 nm CO2 laser (group A), 6 of 29 patients showed excellent improvement (>75%), 12 of the recruited patients demonstrated marked improvement (51%-75%), 8 of the patients demonstrated moderate improvement (25%-50%), and 3 of the patients showed poor improvement (<25%). On the other hand, for group B patients with fractional 1540 nm erbium doped glass, 2 of 29 patients showed excellent improvement (>75%), 11 demonstrated marked improvement (51%–75%), 11 showed moderate improvement (25%-50%), while 5 patients showed poor improvement (<25%). (Table 1; Figures 1 and 2).
Table 1. Clinical Improvement Based on the Quartile Grading Scale .
| Improvement | 10 600 nm (n = 29) | 1540 nm (n = 29) |
| <25% | 3 (10.3%) | 5 (17.2%) |
| 25%–50% | 8 (27.5%) | 11 (37.9%) |
| 51%–75% | 12 (41.3%) | 11 (37.9%) |
| >75% | 6 (20.6%) | 2 (6.8%) |
χ = 3.172, P = 0.38
Figure 1.
A 27-Year-Old Female Patient With Post-acne Scar, Before and After 3 Sessions of Fractional CO2 Laser.
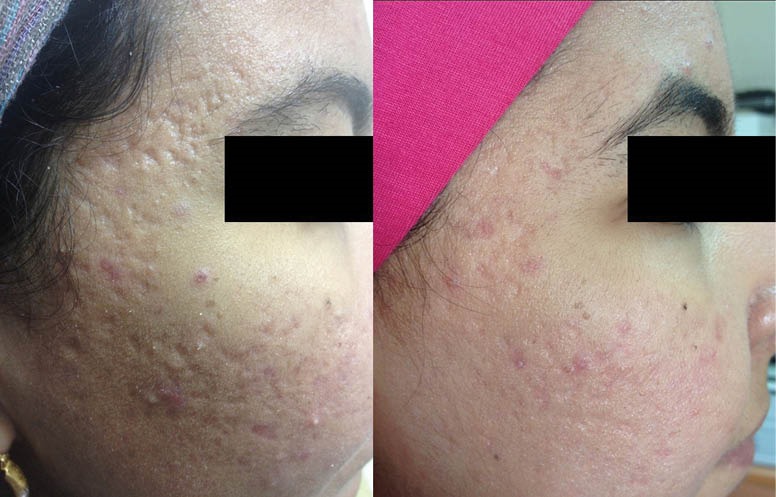
Figure 2.

A 24-Year-Old Male Patient With Post-acne Scar, Before and After 3 Sessions of Fractional Erbium Glass 1540 nm Laser.
After clinically assessing the patients following the sessions and during the follow-ups, the mean grades of improvements were 2.7 ± 0.9 for group A and 2.3 ± 0.8 for group B. Although CO2 laser achieved higher clinical improvement than erbium glass, clinical improvement scores between both laser treatments did not show any significance statistically (P = 0.1). The overall patients’ satisfaction was 48.1 % for ablative fractional CO2 group and 41 % for non-ablative laser group with a non-significant difference (P = 0.44) (Table 2). For clinical improvement, the investigator and subject assessments at 3 months did not differ significantly between the investigator and subjects.
Table 2. Overall Patients’ Satisfaction .
| Improvement | 10 600 nm (n = 29) | 1540 nm (n = 29) |
| Not satisfied | 7 (24.1%) | 7 (24.1%) |
| Slightly satisfied | 8 (27.5%) | 13 (44.8%) |
| Satisfied | 11 (37.9%) | 8 (27.5%) |
| Very satisfied | 3 (10.3%) | 1 (3.4%) |
χ = 2.664, P = 0.44.
In group A, post laser treatment downtime mean (crusting, scaling and erythema) was 5.2 ± 1.05 days. In group B, post-laser session downtime (erythema) mean was 2.1 ± 0.81 days. This difference in the downtime duration following laser sessions was statistically significant (P < 0.001).
The mean VAS pain score associated with the procedures was 5.93 ± 1.39 for group A and 4.41 ± 1.30 for group B (P < 0.001). In group A, 3 patients showed post-inflammatory hyperpigmentation, 2 patients showed acneiform eruption and one patient showed herpes simplex outbreaks after laser treatment, while in group B, only acneiform eruption was noticed with one patient after the laser sessions.
Discussion
Fractional ablative resurfacing (AFR) technology using 10 600 nm carbon dioxide laser relies on the formation of ablated, vaporized columns of tissue surrounded by annular zones of coagulation and dermal remodelling.8 On the other hand the erbium-doped glass laser is a fractional laser that utilizes a non-ablative technology inducing columns of MTZs with much less downtime and with reported high efficacy in treating acne scars.9,10
In high energies, the 1540 nm, non-ablative, erbium glass laser can reach depths exceeding 1000 μm, while the mean penetration depth stands at 679 μm with moderate energy modes.11 At this wavelength, the main chromophores absorbing laser energy are the sebaceous glands, water and adjacent dermal tissues while melanin remains to be spared. Minimal side effects, downtime and superior results were all demonstrated in multiple previous studies.12,13
This study was designed to assess and compare the effectiveness of fractional CO2 laser and fractional non-ablative 1540 nm erbium doped glass laser in the treatment of atrophic acne scars in Egyptian patients. We aimed to investigate the safety of the treatments as well as patients satisfaction following treatment as well.
Ninety days after the final laser treatment session, a significant improvement was seen in both groups. Objective clinical assessment by quartile grading scale revealed a significant improvement in both. Sixty-two percent of patients treated with fractional CO2 laser attained more than 50% improvement while 44.8% of the patients treated with fractional erbium doped glass attained more than 50% improvement. At the 3 months post laser follow up, patients treated with CO2 laser showed a higher improvement that was not statistically significant (P = 0.38). Treatment with fractional CO2 laser was associated with a significant higher downtime than with fractional non-ablative 1540 nm erbium glass, including post-treatment crust formation, scaling and erythema. Pain assessment scores were relatively high using the ablative carbon dioxide in comparison to the non-ablative erbium glass.
In consistence with our study, Hedelund et al14 showed a statistically significant improvement in atrophic post acne scar in comparison with placebo after 3 monthly laser sessions with fractional CO2 device. The study was conducted on 13 patients and the patients were also quoted as being ‘satisfied’ following the laser session treatments.
Three months after the last laser session in a study conducted by Cho et al,15 the clinical assessment of the participants in the study showed mean improvements in all groups of both lasers, treatments did not show statistically significant differences between fractional non-ablative 1550-nm erbium glass laser and fractional ablative CO2 laser (P = 0.249).
In consistence with our study, Cho et al7 demonstrated that the mean improvements were higher with fractional 10 600 nm CO2 laser than fractional non-ablative 1550-nm erbium-glass but with a non-significant difference between both treatments (P = 0.158). The overall patients’ satisfaction levels of fractional 1550-nm glass and fractional 10 600 nm CO2 laser sessions did not reveal any difference of significance (P = 0.105).
Conclusion
According to both the subjective and investigators assessment, it is possible to consider that both fractional ablative CO2 and fractional non-ablative erbium glass lasers represent a useful tool to treat acne scars. Moreover both types of laser represent a modality with a safe profile and that can achieve good patient satisfaction. Additionally, the fractional ablative laser might offer a higher efficacy for acne scars, while the fractional non-ablative might offer a less painful treatment with a shorter downtime.
Conflict of Interests
None.
Ethical Considerations
All subjects gave an informed consent to join this study. The study has been approved by the ethical committee review board.
Please cite this article as follows: Elsaie ML, Ibrahim SM, Saudi W. Ablative fractional 10600 nm carbon dioxide laser versus non-ablative fractional 1540 nm erbium-glass laser in Egyptian post-acne scar patients. J Lasers Med Sci. 2018;9(1):32-35. doi:10.15171/jlm
References
- 1.Asilian A, Salimi E, Faghihi G, Dehghani F, Tajmirriahi N, Hosseini SM. Comparison of Q-Switched 1064-nm Nd: YAG laser and fractional CO2 laser efficacies on improvement of atrophic facial acne scar. J Res Med Sci. 2011;16(9):1189–1195. [PMC free article] [PubMed] [Google Scholar]
- 2.Hirsch RJ. The future of acne treatment with lasers. Cosmet Dermatol. 2002;15:73–74. [Google Scholar]
- 3.Tanzi EL, Alster TS. Comparison of a 1450-nm diode laser and a 1320-nm Nd:YAG laser in the treatment of atrophic facial scars: a prospective clinical and histologic study. Dermatol Surg. 2004;30(2 Pt 1):152–157. doi: 10.1111/j.1524-4725.2004.30078.x. [DOI] [PubMed] [Google Scholar]
- 4.Tierney EP, Kouba DJ, Hanke CW. Review of fractional photothermolysis: treatment indications and efficacy. Dermatol Surg. 2009;35(10):1445–1461. doi: 10.1111/j.1524-4725.2009.01258.x. [DOI] [PubMed] [Google Scholar]
- 5.Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004;34(5):426–438. doi: 10.1002/lsm.20048. [DOI] [PubMed] [Google Scholar]
- 6.Chan NPY, Ho SGY, Yeung CK, Shek SYN, Chan HH. The use of non-ablative fractional resurfacing in Asian acne scar patients. Lasers Surg Med. 2010;42(10):870–875. doi: 10.1002/lsm.20976. [DOI] [PubMed] [Google Scholar]
- 7.Cho SB, Lee SJ, Cho S. et al. Non-ablative 1550-nm erbium-glass and ablative 10 600-nm carbon dioxide fractional lasers for acne scars: a randomized split-face study with blinded response evaluation. J Eur Acad Dermatol Venereol. 2010;24(8):921–925. doi: 10.1111/j.1468-3083.2009.03551.x. [DOI] [PubMed] [Google Scholar]
- 8.Walgrave SE, Ortiz AE, MacFalls HT. et al. Evaluation of a novel fractional resurfacing device for treatment of acne scarring. Lasers Surg Med. 2009;41(2):122–127. doi: 10.1002/lsm.20725. [DOI] [PubMed] [Google Scholar]
- 9.Sherling M, Friedman PM, Adrian R. et al. Consensus recommendations on the use of an erbium-doped 1,550-nm fractionated laser and its applications in dermatologic laser surgery. Dermatol Surg. 2010;36(4):461–469. doi: 10.1111/j.1524-4725.2010.01483.x. [DOI] [PubMed] [Google Scholar]
- 10.Rongsaard N, Rummaneethorn P. Comparison of a fractional bipolar radiofrequency device and a fractional erbium-doped glass 1,550-nm device for the treatment of atrophic acne scars: a randomized split-face clinical study. Dermatol Surg. 2014;40(1):14–21. doi: 10.1111/dsu.12372. [DOI] [PubMed] [Google Scholar]
- 11.Lee HS, Lee JH, Ahn GY. et al. Fractional photothermolysis for the treatment of acne scars: a report of 27 Korean patients. J Dermatolog Treat. 2008;19(1):45–49. doi: 10.1080/09546630701691244. [DOI] [PubMed] [Google Scholar]
- 12.Bedi VP, Chan KF, Sink RK. et al. The effects of pulse energy variations on the dimensions of microscopic thermal treatment zones in nonablative fractional resurfacing. Lasers Surg Med. 2007;39(2):145–155. doi: 10.1002/lsm.20406. [DOI] [PubMed] [Google Scholar]
- 13.Sardana K, Garg V, Arora P, Khurana N. Histological validity and clinical evidence for use of fractional lasers for acne scars. J Cutan Aesthet Surg. 2012;5(2):75–90. doi: 10.4103/0974-2077.99431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hedelund L, Haak CS, Togsverd-Bo K, Bogh MK, Bjerring P, Haedersdal M. Fractional CO2 laser resurfacing for atrophic acne scars: a randomized controlled trial with blinded response evaluation. Lasers Surg Med. 2012;44(6):447–452. doi: 10.1002/lsm.22048. [DOI] [PubMed] [Google Scholar]
- 15.Cho S, Jung JY, Shin JU, Lee JH. Non-ablative 1550 nm erbium-glass and ablative 10,600 nm carbon dioxide fractional lasers for various types of scars in Asian people: evaluation of 100 patients. Photomed Laser Surg. 2014;32(1):42–46. doi: 10.1089/pho.2013.3608. [DOI] [PubMed] [Google Scholar]