

Abstract
Background
Pazopanib is an oral tyrosine kinase inhibitor registered for metastatic renal cell carcinoma and soft tissue sarcoma. Liver toxicity is a common side effect for this class of agents. The current opinion is that in case of severe liver toxicity pazopanib should be interrupted and restarted at a lower dose after returning to Common Terminology Criteria for Adverse Events (CTCAE) grade 1. After recurrence of liver toxicity at the lower dose it is advised to permanently stop pazopanib. We describe a patient with an YWHAE-FAM22 translocated endometrial stromal sarcoma with a remarkable response to pazopanib despite recurrent liver toxicity.
Case Presentation
A 40 year old woman was diagnosed with metastatic YWHAE-FAM22 translocated endometrial stromal sarcoma. She was treated successively with doxorubicin, megestrol acetate and anastrozole, before pazopanib was initiated. Several dose interruptions and reductions were necessary due to liver toxicity, but nevertheless she had a good partial response. Seven months after the start, pazopanib was permanently stopped because of a bilateral pneumothorax. Nine months later it was reinitiated because of progression and was continued for another 8 months until final disease progression.
Conclusion
In contrast to the current summary of product characteristics of pazopanib, the drug was successfully continued despite recurrent liver toxicity, and no further liver function deterioration was found. This case suggests that further dose reductions are good practice when liver toxicity limits treatment in responding patients.
Secondly, this patient with rare YWHAE-FAM22 translocated endometrial stromal sarcoma showed a remarkable response to VEGFR/KIT inhibitor pazopanib. Recently, it was reported that this specific subtype of endometrial stromal sarcoma overexpresses CD117, but has no KIT mutations.
This case illustrates that (a) pazopanib can be continued in patients with recurrent liver toxicity after dose reductions under strict surveillance and that (b) pazopanib shows good efficacy in YWHAE-FAM22 translocated endometrial stromal sarcoma.
Keywords: Pazopanib, Endometrial stromal sarcoma, Liver function, Adverse events, Response
Background
The oral anti-angiogenic tyrosine kinase inhibitor (TKI) pazopanib is a multi-target TKI [1]. Its main activity is against vascular endothelial growth factor receptors (VEGFR) 1, 2 and 3, platelet derived growth factor receptors (PDGFR) and KIT [1]. The phase III PALETTE study showed an increase in the progression free survival (PFS) from 1.6 months with placebo to 4.6 months with pazopanib (Votrient®, GlaxoSmithKline) in patients with metastatic soft tissue sarcoma [2, 3]. Pazopanib is also effective in renal-cell carcinoma (RCC), with an increase in PFS from 4.2 months with placebo to 9.2 months with pazopanib [4]. Overall survival (OS) was also significantly increased with pazopanib despite cross-over from placebo treatment to pazopanib treatment [5].
Liver toxicity is a well-known side effect of pazopanib, with an incidence in the PALETTE study of a grade ≥ 2 elevated alanine aminotransferase (ALAT) of 10% (placebo 3%) and aspartate aminotransferase (ASAT) of 8% (placebo 2%) [2]. An increase in total bilirubin was not seen in this study. In the RCC study, a National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) grade ≥ 3 increase in ALAT was found in 12% (placebo 1%), ASAT 7% (< 1%) and total bilirubin 3% (1%) [4]. Two patients in this RCC study were assessed as having died due to abnormal hepatic function. The current opinion is that physicians should be careful prescribing pazopanib in patients with abnormal ASAT, ALAT and total bilirubin levels and that treatment should be discontinued at least temporarily when grade 3 or more elevations occur during treatment. In case of recurrence of liver function abnormalities after restarting treatment pazopanib should be stopped permanently [6].
Endometrial stromal neoplasms of the uterus are divided into four categories based on the 2014 WHO classification, i.e. endometrial stromal nodule, low-grade endometrial stromal sarcoma (ESS), high grade ESS and undifferentiated uterine sarcoma [7, 8]. ESS is very rare, representing 0.2% of all genital tract malignancies and the patients are generally younger than in other uterine malignancies. Low grade ESS is usually CD10 positive and Cyclin D1 negative [9]. Fifty to 60 % of the ESS harbour translocations involving JAZF1. Recently, it was found that high grade ESS (negative for CD10, positive for Cyclin D1) are characterised by a t(10;17)(q22;p13) translocation resulting in a YWHAE-FAM22 (also known as YWHAE-NUTM2A/B) gene fusion [10, 11]. It is suggested that these tumours have a poor response to therapy compared to the lower grade ESS, which has a 5 year disease specific survival rate for FIGO stage III-IV of 50.3% [12]. Current treatment for metastatic or locally advanced disease consists of hormonal therapy and chemotherapy, i.e. doxorubicin or ifosfamide monotherapy or gemcitabine/docetaxel combination therapy [9]. Pazopanib is also registered for this soft tissue sarcoma subtype, but specific studies are not available and will not be run because of the rarity of this histologic subtype.
This case report describes a patient successfully treated with pazopanib for an ESS developing abnormal liver chemistry, which continued treatment with adapted dosing of pazopanib under careful surveillance of liver function. She had a remarkable response on pazopanib.
Case Presentation
A 40 year old female presented with a 4 months history of recurrent right sided lower thoracic pain during sports. Medical history consisted of a hysterectomy for symptomatic uterine myomatosis four years previously, after giving birth to her second child. This was a non-radical non-oncological resection. The original pathology report revealed a 15 cm low grade ESS. Now, four years after the hysterectomy, a CT scan showed a large mediastinal mass with expansion in the upper abdomen and compression of the left atrium and multiple lesions in both lungs. A bronchoscopic biopsy showed cells similar to the earlier diagnosed ESS. Treatment with six courses of doxorubicin resulted in a very good partial response. Maintenance therapy with megestrol acetate 160 mg was started hoping to prolong the time to progression. Two years later, an increase in size and number of the lung metastases was observed, so megestrol acetate was stopped and anastrozole 1 mg started. Further disease progression was noticed 4 months later (Fig. 1a). Pazopanib 800 mg orally once daily was started in the named patient program in collaboration with the Leiden University Medical Centre, one of the Dutch sarcoma reference centres. At the same time, pathology review was performed, confirming the diagnosis of low grade ESS, but also noticing a CyclinD1 positive and CD10 negative higher grade component suggesting a YWHAE-FAM22 translocated ESS. (Fig. 2a-d) Fluorescent in situ hybridisation confirmed the diagnosis. The tumour showed high expression of KIT in the high grade component of the tumour.
Fig. 1.
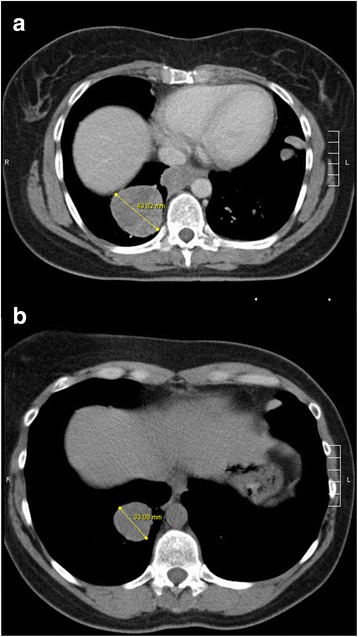
CT scans. Evaluation CT scans before start of pazopanib (a) and 12 weeks after start of pazopanib (so 6 weeks on pazopanib and 6 weeks off because of liver toxicity) (b) showing a shrinking pulmonary metastasis measured by largest diameter at both times
Fig. 2.
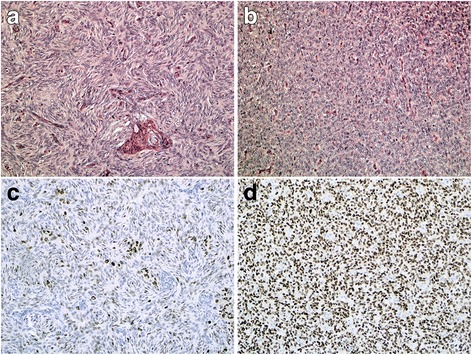
Histology. a: Normal HE slides of the lower grade component of ESS, showing spindled cells in a storiform pattern. b: HE slides of the high grade component of ESS, showing round cells and open nuclei. c: Cyclin D1 expression of the lower grade component is weak and more heterogeneous. d: Diffuse and strong Cyclin D1 expression in the high grade areas
Six weeks after start of pazopanib 800 mg once daily an increase in ALAT to > 10 times the upper limit of normal (ULN) was observed. (Figure 3) Hepatitis serology, liver ultrasound and liver biopsy were not performed because of the clear relationship of the increased liver enzymes with the start of pazopanib. She had no history of liver disease, no liver metastases and no liver function abnormalities before start of pazopanib. During the previous treatment with doxorubicin, y-glutamyl transferase increased to 20× ULN and ALAT to 6× ULN, no other liver function abnormalities occurred. The CT scan showed a decrease in the sum of the largest diameters of the target lesions of 23%. Pazopanib was put on hold immediately until the liver enzymes returned to normal. (Figure 3) After six weeks without pazopanib the CT scan showed a further decrease of the target lesions of 38% compared to baseline (19% compared to the previous CT scan) indicating a partial response. Figure 1b) At the time the liver toxicity had almost recovered, a re-challenge with pazopanib 200 mg once daily was performed, but after one week liver function abnormalities recurred and pazopanib was stopped again. After liver function recoverage, pazopanib 200 mg once every other day was initiated, but again after 2 weeks liver enzymes increased to > 3× ULN. Another week later pazopanib 200 mg every third day was given for 2 weeks, until a CT scan showed progression (six months after the start of pazopanib). She was still in very good clinical condition and besides the remarkable inclination of liver enzymes at the beginning of treatment and lesser rises thereafter she had had little other toxicity with pazopanib. She consented to another challenge with pazopanib 200 mg every day under further strict surveillance of liver enzymes. The liver enzymes remained < 3 times ULN, but 3 weeks later she was admitted with a bilateral pneumothorax and pazopanib was stopped. On the right side a pleurodesis was performed and on the left side it was drained. Anastrozole and leuproreline were prescribed, hoping to slow down progression. Two months later, a CT scan again showed progressive disease, and ifosfamide chemotherapy (5 g/m2 in a 24-h continuous infusion every 3 weeks) was initiated. CT scans after 3 and 6 cycles showed stable disease. During ifosfamide treatment only a slight increase in y-glutamyl transferase was noticed (increase to < 2× ULN). Two months after the last ifosfamide administration, radiological progression was observed again and pazopanib 400 mg daily was prescribed again under strict weekly surveillance of the liver enzymes. This dose was chosen because patient had a pleural effusion due to the progression and thereby a lot of complaints. To be sure of a therapeutic dose of pazopanib we started with 400 mg daily. Two weeks after reinitiating pazopanib the pneumothorax on the left side recurred and persisted. Pazopanib was held for two weeks, but was then reinitiated after discussion of the risks with the patient. CT scans 6 weeks and 3.5 months after the restart of pazopanib showed stable disease. Pazopanib was stopped permanently 6 months after the restart because of progressive disease, and she died 2 weeks later. In the second period of pazopanib treatment, no liver toxicity occurred. No differences between co-medication were found between the first period of pazopanib treatment and the second. A summary of the patients’ history is given in Fig. 4.
Fig. 3.
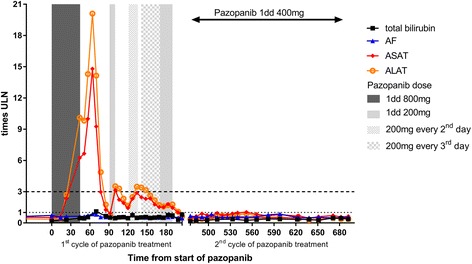
Course of pazopanib dose and laboratory parameters in time. ULN: upper limit of normal
Fig. 4.

Timeline. Description of treatment in time
The DNA of the patient was analyzed for single nucleotide polymorphisms (SNPs) in enzymes known to be involved in the absorption, distribution, metabolism and elimination of pazopanib [13]. The genes analyzed were CYP3A4, CYP1A2, CYP2C8, ABCB1 and SLCO1B1. The main metabolizing enzyme for pazopanib, CYP3A4 did not have SNPs associated with a decreased metabolic function. Two SNP variants in CYP1A2 (rs762551 and rs2470890) and one in SLCO1B1 (rs4149057) were detected, but no evidence exists that these polymorphisms cause elevated levels of pazopanib. So, this analysis did not result in the elucidation of a cause for the liver toxicity in this patient.
Discussion and conclusion
This case report has 2 new learning messages: we present a patient with an ESS with a remarkable response on pazopanib and we describe clinical management of pazopanib induced recurrent liver toxicity.
Liver function test abnormalities, mainly elevations in ASAT and ALAT, are a common side effect of pazopanib and more in general of TKIs [14]. The exact pathophysiologic mechanism is unknown. A distinctive class effect seems to be unlikely, because pharmacologically different TKIs are known to be hepatotoxic and the substances are also very different chemical compounds. In a case series of two patients with liver toxicity of pazopanib liver histology showed mild active cholestatic hepatitis with inflammation that predominantly involved portal tracts [15]. Recently, it was reported that treatment with pazopanib in combination with prednisolone in case of liver function abnormalities prevented recurrence of liver function abnormalities in two patients [16]. UDP-glucuronosyltransferase isoform 1A1 has been related to bilirubin elevations during pazopanib treatment. These are probably patients with latent Gilbert syndrome becoming evident due to the inhibitory effect of pazopanib [14]. More recently, an association between HLA-B*57:01 and pazopanib induced liver toxicity was found [17]. Whether other germline genetic causes of pazopanib induced liver toxicity exist is unclear. The summary of product characteristics (SmPC) of pazopanib contains guidelines on handling liver toxicity [6]. If the elevation of ASAT and ALAT between 3 and 8× ULN it is safe to continue pazopanib with strict control of ASAT and ALAT until grade 1 toxicity. If ASAT and/or ALAT is more than 8× ULN then pazopanib should be stopped until recovery till grade I or less and if reinitiated restart with pazopanib once daily 400 mg. It should be stopped permanently if ASAT and/or ALAT rise again to > 3× ULN. Pazopanib should also be stopped if ASAT and/or ALAT are elevated > 3× ULN concurrently with a bilirubin elevated > 2× ULN. In our case, despite these recommendations, pazopanib was reintroduced at further reduced dose and no progressive liver insufficiency developed. Ultimately this strategy seemed to be effective until a dose reduction to 200 mg once every second day. Another possible solution for toxicity management would be therapeutic drug monitoring, which is possible for pazopanib with a dried blood spot assay [18]. However, because the intrapatient variability of pazopanib levels is high, a recent study could not show an effect of therapeutic drug monitoring on the interpatient variation [19]. A SNP analysis of genes for enzymes known to be involved in the metabolism of pazopanib did not provide an explanation for elevated pazopanib levels or liver toxicity in our patient. In case of further dose reductions after reduction to once daily 400 mg, we suggest that patients should be monitored closely with once weekly liver function testing.
The second message of this case report regards the pazopanib response related to the tumour type. When feasible ESS is treated with radical surgery. Treatment of metastatic or locally progressive ESS consists of endocrine therapy as first line and when progressive on endocrine therapy chemotherapy. No specific data on the use of pazopanib in ESS is available, but this case report shows that pazopanib induced a partial response and prolonged PFS of 9 months which is more than the median PFS in the PALETTE study. Although in general ESS does not overexpress KIT, it was recently shown that ESS harbouring the YWHAE-FAM22 fusion gene frequently overexpress KIT (without a mutation in the KIT oncogene) in the high grade component of the tumour, as was the case in our patient [11, 20]. This could explain the good response, in this rare histologic subtype, to pazopanib, which is an inhibitor of VEGFRs, PDGFRs and KIT. Based on these findings there may also be a potential role for imatinib, which was already reported in two cases [21, 22]. Most probably the evidence for treatments in ESS will be not better than small case series due to the rarity of this disease.
The 3rd teaching point of this case report regarding the occurrence and clinical development of a pneumothorax during pazopanib treatment in (responding) patients with pleurally located metastatic lesions was addressed in a previous case series [23].
In conclusion this case illustrates two important new points:
First, reversible severe liver toxicity with pazopanib treatment is a known rare side effect of pazopanib and low dose personalized rechallenge in responding patients is a therapeutic option in experienced hands. This low dose personalized rechallenge is in conflict with the current SmPC of pazopanib and patients should be closely monitored for liver function abnormalities with for example weekly testing of the liver functions.
Second, pazopanib was found to result in a good response in this patient with a YWHAE-FAM22A/B translocated ESS which may be related to the KIT overexpression in these tumours.
Acknowledgements
We would like to thank Marissa Nucci for reviewing the histological slides and confirming the diagnosis and we would like to thank Djoeke de Wit for helping us with the interpretation of the drug metabolism array.
Funding
No funding was received for this case report.
Availability of data and materials
The patients information used for this study is not publicly available due to privacy regulations.
Abbreviations
- ALAT
Alanine aminotransferase
- ASAT
Aspartate aminotransferase
- CTCAE
Common Terminology Criteria for Adverse Events
- ESS
Endometrial stromal sarcoma
- NCI
National Cancer Institute
- OS
Overall survival
- PDGFR
Platelet derived growth factor receptors
- PFS
Progression free survival
- RCC
Renal-cell carcinoma
- SmPC
Summary of product characteristics
- SNP
Single nucleotide polymorphism
- TKI
Tyrosine kinase inhibitor
- VEGFR
Vascular endothelial growth factor receptors
Authors’ contributions
AV and HG did the conception and design of the case report, did a review of the literature and wrote the case report. FW provided the patient information. JB and TB reviewed the histopathological specimens. FW, JB and TB revised the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Because no experimental treatment was used ethics approval is not necessary. Patient consented to be part of the pazopanib compassionate use program and thereby consented for use of medical data for scientific purposes. Consent to publish was given by her family, because the patient has passed away. A copy of the written informed consent is available for review by the Editor-in-Chief of this journal. Because no experimental treatment was used, ethics approval is not necessary.
Consent for publication
Consent to publish was given by her family, because the patient has passed away. A copy of the written informed consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Arie J. Verschoor, Email: a.j.verschoor@lumc.nl
Fabiënne A. R. M. Warmerdam, Email: f.warmerdam@atriummc.nl
Tjalling Bosse, Email: t.bosse@lumc.nl.
Judith V. M. G. Bovée, Email: j.v.m.g.bovee@lumc.nl
Hans Gelderblom, Email: a.j.gelderblom@lumc.nl.
References
- 1.Harris PA, Boloor A, Cheung M, Kumar R, Crosby RM, Davis-Ward RG, Epperly AH, Hinkle KW, Hunter RN, 3rd, Johnson JH, et al. Discovery of 5-[[4-[(2,3-dimethyl-2H-indazol-6-yl)methylamino]-2-pyrimidinyl]amino]-2-methyl-b enzenesulfonamide (Pazopanib), a novel and potent vascular endothelial growth factor receptor inhibitor. J Med Chem. 2008;51(15):4632–4640. doi: 10.1021/jm800566m. [DOI] [PubMed] [Google Scholar]
- 2.van der Graaf WT, Blay JY, Chawla SP, Kim DW, Bui-Nguyen B, Casali PG, Schoffski P, Aglietta M, Staddon AP, Beppu Y, et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2012;379(9829):1879–1886. doi: 10.1016/S0140-6736(12)60651-5. [DOI] [PubMed] [Google Scholar]
- 3.Van Der Graaf WTA, Blay J-Y, Chawla SP, Kim D-W, Bui Nguyen B, Casali PG, Schoffski P, Aglietta M, Staddon AP, Beppu Y, et al. PALETTE: final overall survival (OS) data and predictive factors for OS of EORTC 62072/GSK VEG110727, a randomized double-blind phase III trial of pazopanib versus placebo in advanced soft tissue sarcoma (STS) patients. ASCO Meeting Abstracts. 2012;30(15_suppl):10009. [Google Scholar]
- 4.Sternberg CN, Davis ID, Mardiak J, Szczylik C, Lee E, Wagstaff J, Barrios CH, Salman P, Gladkov OA, Kavina A, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial. J Clin Oncol. 2010;28(6):1061–1068. doi: 10.1200/JCO.2009.23.9764. [DOI] [PubMed] [Google Scholar]
- 5.Sternberg CN, Hawkins RE, Wagstaff J, Salman P, Mardiak J, Barrios CH, Zarba JJ, Gladkov OA, Lee E, Szczylik C, et al. A randomised, double-blind phase III study of pazopanib in patients with advanced and/or metastatic renal cell carcinoma: final overall survival results and safety update. European journal of cancer (Oxford, England : 1990) 2013;49(6):1287–1296. doi: 10.1016/j.ejca.2012.12.010. [DOI] [PubMed] [Google Scholar]
- 6.SmPC pazopanib (Votrient) [http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001141/WC500094272.pdf].
- 7.Oliva E, Carcangiu ML, Carinelli SG, Ip P, Loening T, Longacre TA, Nucci MR, Prat J, Zaloudek CJ. Mesenchymal tumours. In: Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. Pathology and genetics of Tumours of female reproductive organs. 4. Lyon: IARC; 2014. pp. 141–145. [Google Scholar]
- 8.Ali RH, Rouzbahman M. Endometrial stromal tumours revisited: an update based on the 2014 WHO classification. J Clin Pathol. 2015;68(5):325–332. doi: 10.1136/jclinpath-2014-202829. [DOI] [PubMed] [Google Scholar]
- 9.Rauh-Hain JA, del Carmen MG. Endometrial stromal sarcoma: a systematic review. Obstet Gynecol. 2013;122(3):676–683. doi: 10.1097/AOG.0b013e3182a189ac. [DOI] [PubMed] [Google Scholar]
- 10.Lee CH, Marino-Enriquez A, Ou W, Zhu M, Ali RH, Chiang S, Amant F, Gilks CB, van de Rijn M, Oliva E, et al. The clinicopathologic features of YWHAE-FAM22 endometrial stromal sarcomas: a histologically high-grade and clinically aggressive tumor. Am J Surg Pathol. 2012;36(5):641–653. doi: 10.1097/PAS.0b013e31824a7b1a. [DOI] [PubMed] [Google Scholar]
- 11.Lee C-H, Hoang LN, Yip S, Reyes C, Marino-Enriquez A, Eilers G, Tao D, Chiang S, Fletcher JA, Soslow RA, et al. Frequent expression of KIT in endometrial stromal sarcoma with YWHAE genetic rearrangement. Mod Pathol. 2014;27(5):751–757. doi: 10.1038/modpathol.2013.199. [DOI] [PubMed] [Google Scholar]
- 12.Chan JK, Kawar NM, Shin JY, Osann K, Lm C, Powell CB, Kapp DS. Endometrial stromal sarcoma: a population-based analysis. Br J Cancer. 2008;99(8):1210–1215. doi: 10.1038/sj.bjc.6604527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.van Geel RMJM, Beijnen JH, JHM S. Concise drug review: Pazopanib and Axitinib. Oncologist. 2012;17(8):1081–1089. doi: 10.1634/theoncologist.2012-0055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shah R, Morganroth J, Shah D. Hepatotoxicity of tyrosine Kinase inhibitors: clinical and regulatory perspectives. Drug Saf. 2013;36(7):491–503. doi: 10.1007/s40264-013-0048-4. [DOI] [PubMed] [Google Scholar]
- 15.Klempner SJ, Choueiri TK, Yee E, Doyle LA, Schuppan D, Atkins MB. Severe Pazopanib-induced Hepatotoxicity: clinical and Histologic course in two patients. J Clin Oncol. 2012;30(27):e264–e268. doi: 10.1200/JCO.2011.41.0332. [DOI] [PubMed] [Google Scholar]
- 16.Vlenterie M, van Erp NP, van der Graaf WTA. Promising management of pazopanib-induced liver toxicity. Acta Oncol. 2015;54(7):1064–1066. doi: 10.3109/0284186X.2015.1004368. [DOI] [PubMed] [Google Scholar]
- 17.Xu CF, Johnson T, Wang X, Carpenter C, Graves AP, Warren L, Xue Z, King KS, Fraser DJ, Stinnett S, et al. HLA-B*57:01 confers susceptibility to Pazopanib-associated liver injury in patients with cancer. Clin Cancer Res. 2016;22(6):1371–1377. doi: 10.1158/1078-0432.CCR-15-2044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.de Wit D, den Hartigh J, Gelderblom H, Qian Y, den Hollander M, Verheul H, Guchelaar HJ, van Erp NP. Dried blood spot analysis for therapeutic drug monitoring of pazopanib. J Clin Pharmacol. 2015;55(12):1344–50. [DOI] [PubMed]
- 19.de Wit D, van Erp NP, den Hartigh J, Wolterbeek R, den Hollander-van Deursen M, Labots M, Guchelaar HJ, Verheul HM, Gelderblom H. Therapeutic drug monitoring to individualize the dosing of pazopanib: a pharmacokinetic feasibility study. Ther Drug Monit. 2015;37(3):331–338. doi: 10.1097/FTD.0000000000000141. [DOI] [PubMed] [Google Scholar]
- 20.Sardinha R, Hernandez T, Fraile S, Tresserra F, Vidal A, Gomez MC, Astudillo A, Hernandez N, Saenz de Santamaria J, Ordi J, et al. Endometrial stromal tumors: immunohistochemical and molecular analysis of potential targets of tyrosine kinase inhibitors. Clin Sarcoma Res. 2013;3(1):3. doi: 10.1186/2045-3329-3-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Salvatierra A, Tarrats A, Gomez C, Sastre JM, Balaña C. A case of c-kit positive high-grade stromal endometrial sarcoma responding to Imatinib Mesylate. Gynecol Oncol. 2006;101(3):545–547. doi: 10.1016/j.ygyno.2006.01.024. [DOI] [PubMed] [Google Scholar]
- 22.Kalender M, Sevinc A, Yilmaz M, Ozsarac C, Camci C. Detection of complete response to imatinib mesylate (Glivec®/Gleevec®) with 18F-FDG PET/CT for low-grade endometrial stromal sarcoma. Cancer Chemother Pharmacol. 2009;63(3):555–559. doi: 10.1007/s00280-008-0786-7. [DOI] [PubMed] [Google Scholar]
- 23.Verschoor AJ, Gelderblom H. Pneumothorax as adverse event in patients with lung metastases of soft tissue sarcoma treated with pazopanib: a single reference centre case series. Clin Sarcoma Res. 2014;4:14. doi: 10.1186/2045-3329-4-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The patients information used for this study is not publicly available due to privacy regulations.