

Abstract
Purpose
Secondary primary cancers (SPCs) commonly arise in patients with renal cell carcinoma (RCC). We designed the present study to estimate the SPC incidence in Korean patients with RCC.
Materials and Methods
The study cohort was population-based and consisted of 40,347 individuals from the Korean Central Cancer Registry who were diagnosed with primary renal cancer between 1993 and 2013. Standardized incidence ratios (SIRs) for SPCs were estimated for different ages at diagnosis, latencies, diagnostic periods, and treatments.
Results
For patients with primary RCC, the risk of developing a SPC was higher than the risk of developing cancer in the general population (SIR, 1.13; 95% confidence interval, 1.08 to 1.18). Most cancer types showed higher incidences in patients with RCC than in the general population. However, the relative incidence of gastric cancer as an SPC varied by age. Gastric cancer incidence was elevated in young patients (< 30 years) with RCC, but reduced in older (≥ 30) patients with RCC. Patients with advanced RCC died prematurely, regardless of SPC development. In contrast, those with early-stage RCC survived for longer periods, although SPC development affected their post-RCC survival. After SPC development, women had better survival than men.
Conclusion
In Korean patients with primary RCC, the incidence of SPC was 13% higher than the incidence of cancer in the general population. These findings may play important roles in the conduct of follow-up evaluations and education for patients with RCC.
Keywords: Renal cell carcinoma, Second primary neoplasms, Prognosis, Incidence, Survival
Introduction
The number of cancer survivors continues to increase because of earlier diagnosis, improvements in treatment, and supportive care [1,2]. As advancements are made in medical diagnostic imaging, a growing number of renal cell carcinoma (RCC) cases are being discovered incidentally because small RCC tumors tend to be asymptomatic [3]. According to the Korea Central Cancer Registry (KCCR), 4,333 new RCC cases were diagnosed in 2013 (male, 2,992; female, 1,341), amounting to an incidence of 5.7 cases per 100,000 individuals (male, 8.3; female, 3.4). Additionally, in Korea, the 5-year survival rates of men and women with RCC have increased gradually, rising from 60.8% and 64.5% in 1993-1995 to 80.5% and 81.6% in 2009-2013, respectively [4].
Previous studies have reported that the risk of developing second primary cancers (SPCs) in RCC survivors is higher than the risk of developing primary cancers in comparable members of the general population. RCC survivors have been observed to have elevated risks of bladder, prostate, colorectal, lung, and nervous system SPCs, as well as second primary melanoma and non-Hodgkin’s lymphoma [5,6]. The elevated incidences of SPCs might be attributable to the application of more intensive medical surveillance following the development of primary cancer, genetic or non-genetic factors that are shared between the primary cancer and SPCs, or interactions between the primary cancer and SPCs [7,8].
Novel treatment modalities are improving the survival rate of patients with RCC [9,10], and understanding the incidence and prognostic importance of SPC has become a concern for treatment providers and RCC survivors, particularly in relation to quality of life. In this context, the objective of the present study of Korean patients with RCC was to calculate the SPC incidence and evaluate the effects of SPC on survival. The ultimate goal of our analysis was to produce data that would be useful for the management of patients with RCC.
Materials and Methods
1. Study population and data collection
We evaluated 40,347 patients who were diagnosed with primary RCC between 1993 and 2013, as recorded in the KCCR (Fig. 1). The Korean Ministry of Health and Welfare began accumulating data via the KCCR in 1980 [11]. Until 1998, cancer cases were collected and registered annually from > 180 Korean hospitals, which are believed to have included 80%-90% of all cancer cases in Korea [11]. Since 1999, population-based cancer incidence data have been produced systematically, and the KCCR data from 1999 to 2002 have been published in the Cancer Incidence in Five Continents. Vol. 9, which reflects the completeness and validity of the dataset [12]. The cancers recorded in the KCCR were classified based on the International Classification of Disease for Oncology, 3rd edition (ICD-O-3) [13]. RCC was defined as being present for cases with ICD-O-3 code C64.9. The KCCR data includes patient information (sex and age at the time of diagnosis), cancer information (date of diagnosis, tumor site, histology type, and Surveillance, Epidemiology, and End Results [SEER] summary stage), and first-line treatment information (surgery, chemotherapy, radiothereapy [RT], immunotherapy, and hormone therapy). The details of the KCCR are widely published [4,11,14]. For the multiple primary rules, we used the definition from the International Agency for Research on Cancer [15].
Fig. 1.
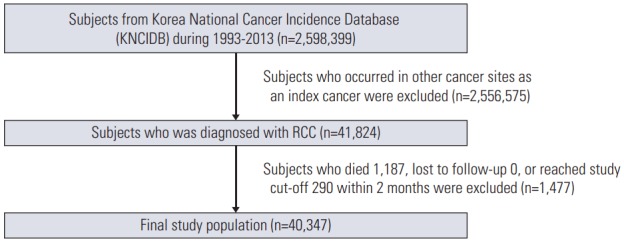
Flow chart of selection of the study population. RCC, renal cell carcinoma.
If an SPC was identified within the first 2 months after the diagnosis of the first primary cancer, it was considered to be a synchronous cancer, and was therefore excluded from our study [16]. Additionally, to avoid potential confusion, secondary kidney cases were also excluded.
The reasons for exit from the present study were death during follow-up (n=12,262, 30.39%) and the end of the study period (n=28,085, 69.61%). The National Cancer Center Institutional Review Board approved this study (NCC2016-0230).
2. Statistical analyses
To provide a quantitative comparison of the cancer risks faced by patients with RCC and the general population, we calculated standardized incidence ratios (SIRs) and corresponding 95% confidence intervals (95% CIs). We chose to use the SIR because it is a measure of relative risk that compares the incidence rate of the subsequent cancer of interest to the baseline incidence rate in the general population. Cancer incidence rates were calculated for each type of cancer, by sex, age and calendar year, and were multiplied by the accumulated person years at risk to estimate the expected number of subsequent cancers for each stratum. SIRs were obtained by dividing the observed number of second cancers in patients with RCC by the expected number, if the patients in the cohort experienced the same cancer rates as members of in the general population. We calculated the person-years at risk from 2 months after the date of the initial RCC diagnosis to the date of the last known survival status, death, or study completion (December 31, 2013). For analysis, the subjects were stratified by age at RCC diagnosis (< 30, 30-59, and ≥ 60 years), latency (< 1 year, 1-5 years, 5-10 years, and ≥ 10 years), and the period of RCC diagnosis (1993-2000 and 2001-2013).
Data were also analyzed based on the treatment modalities that had been used for RCC. Treatment given within 4 months of the initial RCC diagnosis was considered to be first-line treatment. Survival probabilities were calculated using the Kaplan-Meier method [17], based on the presence of an SPC. Intergroup differences were evaluated using the log-rank test. All statistical tests were two-sided, and a p-value of < 0.05 was considered statistically significant. SEER*Stat software (ver. 8.3.2, http://seer.cancer.gov/seerstat) was used to calculate the SIRs and 95% CIs. Survival curves and log-rank tests were generated using STATA ver. 11 (StataCorp LP, College Station, TX).
Results
The characteristics of the 40,347 patients with primary RCC are shown in Table 1. Those with primary RCC had an elevated overall risk of developing an SPC. For the following cancers, the incidences of SPC were higher in patients with RCC than in comparable members of the general population: lung cancer, female breast cancer, thyroid cancer, soft tissue tumor, acute lymphocytic leukemia, skin melanoma, prostate cancer, bladder cancer, and renal pelvis tumor (Table 2). On the other hand, the risks of gastric, and esophagus cancer in RCC patients were significantly decreased (SIR, 0.68 and 0.60, respectively).
Table 1.
Characteristics of patients with initial kidney cancer, 1993-2013
| No. (%) | |
|---|---|
| Patients with kidney cancer | 40,347 (100) |
| Time period kidney cancer diagnosis | |
| 1993-1997 | 3,938 (9.76) |
| 1998-2002 | 6,684 (16.57) |
| 2003-2007 | 10,569 (26.20) |
| 2008-2013 | 19,156 (47.48) |
| Age at diagnosis with kidney cancer, mean±SD (yr) | 56.36±15.18 |
| Age at diagnosis with kidney cancer, median (range, yr) | 57.00 (0.00-100.00) |
| Patients by age at 1st primary kidney cancer diagnosis (yr) | |
| 0-29 | 1,532 (3.80) |
| 30-59 | 20,927 (51.87) |
| ≥ 60 | 17,888 (44.34) |
| Primary treatment for kidney cancer | |
| Surgery | 32,688 (81.02) |
| Radiation | 1,343 (3.33) |
| Chemotherapy | 3,545 (8.79) |
| Follow-up after kidney cancer diagnosis, mean±SD (yr) | 5.14±4.82 |
| Follow-up after kidney cancer diagnosis, median (range, yr) | 3.63 (0.00-20.80) |
| Patients who developed subsequent primary cancers | 2,111 (5.23) |
| Patients by number of subsequent primary cancer | |
| 1 | 1,977 (4.90) |
| 2 | 126 (0.31) |
| ≥ 3 | 8 (0.02) |
| Age at diagnosis of 2nd primary cancer, mean±SD (yr) | 64.15±11.61 |
| Letency between 1st and 2nd cancers, mean±SD (yr) | 4.97±4.26 |
| Letency between 1st and 2nd cancers, median (range, yr) | 3.83 (0.17-20.00) |
| Patients by latency group between 1st and 2nd cancers (mo) | |
| < 12 | 354 (16.77) |
| 12-59 | 912 (43.2) |
| 60-119 | 543 (25.72) |
| ≥ 120 | 302 (14.31) |
| Patients by age at 2nd primary cancer diagnosis (yr) | |
| 0-29 | 15 (0.71) |
| 30-59 | 639 (30.27) |
| ≥ 60 | 1,457 (69.02) |
| Follow-up after 2nd primary cancer diagnosis, mean±SD (yr) | 3.08±3.06 |
| Follow-up after 2nd primary cancer diagnosis, median (range, yr) | 2.17 (0.00-19.42) |
SD, standard deviation.
Table 2.
Risk of subsequent primary cancers after diagnosis of kidney cancer by follow-up, age, period, and treatment, 1993-2013
| SIR |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total SIR (O/E) | Latency (mo) |
Age (yr) |
Period |
Treatment |
|||||||||
| < 12 | 12-59 | 60-119 | ≥ 120 | 0-29 | 30-59 | ≥ 60 | 1993-2000 | 2001-2013 | RT | Surgery | Chemotherapy | ||
| All subsequent cancers | 1.13a) (2,269/2,007.01) | 1.44a) | 1.10a) | 1.05 | 1.07 | 4.63a) | 1.29a) | 1.01 | 1.13a) | 1.13a) | 1.13 | 1.15a) | 1.26a) |
| All excluding kidney | 1.14a) (2,253/1,970.16) | 1.42a) | 1.13a) | 1.07 | 1.09 | 4.38a) | 1.31a) | 1.02 | 1.14a) | 1.14a) | 1.15 | 1.16a) | 1.26a) |
| Buccal cavity, pharynx | 1 (33/32.9) | 0.45 | 1.11 | 0.98 | 1.24 | 0.00 | 1.57 | 0.55 | 1.41 | 0.79 | 0.00 | 1.06 | 0.63 |
| Digestive system | 0.88a) (915/1,043.64) | 0.98 | 0.80a) | 0.90 | 0.95 | 3.84a) | 0.93 | 0.83a) | 0.94 | 0.84a) | 1.06 | 0.88a) | 0.94 |
| Esophagus | 0.60a) (24/39.82) | 0.75 | 0.46a) | 0.63 | 0.84 | 0.00 | 0.74 | 0.53a) | 0.75 | 0.52a) | 0.00 | 0.54a) | 1.03 |
| Stomach | 0.68a) (257/377.73) | 0.68a) | 0.62a) | 0.72a) | 0.79 | 2.19 | 0.74a) | 0.64a) | 0.75a) | 0.64a) | 0.53 | 0.72a) | 0.79 |
| Gallbladder | 0.66 (17/25.67) | 0.93 | 0.84 | 0.41 | 0.46 | 0.00 | 0.14a) | 0.87 | 0.76 | 0.61 | 0.00 | 0.64 | 0.93 |
| Respiratory system | 1.05 (349/330.94) | 0.73 | 1.19a) | 0.99 | 1.07 | 7.47 | 1.36a) | 0.93 | 1.21a) | 0.97 | 0.41 | 1.08 | 1.06 |
| Nose, nasal cavity, ear | 1.9 (7/3.68) | 2.00 | 2.49 | 1.95 | 0.00 | 0.00 | 1.31 | 2.33 | 1.51 | 2.13 | 17.94 | 1.86 | 5.77 |
| Larynx | 0.83 (17/20.37) | 0.36 | 1.22 | 0.18a) | 1.37 | 0.00 | 0.79 | 0.86 | 1.03 | 0.71 | 0.00 | 0.78 | 0.00 |
| Lung, bronchus | 1.05 (320/305.26) | 0.74 | 1.16 | 1.01 | 1.05 | 10.41 | 1.39a) | 0.91 | 1.18 | 0.97 | 0.23 | 1.08 | 1.09 |
| Female breast | 1.34a) (69/51.59) | 0.74 | 1.57a) | 1.24 | 1.34 | 0.00 | 1.45a) | 1.10 | 1.42 | 1.31 | 0.00 | 1.33a) | 1.04 |
| Female genital system | 0.9 (34/37.57) | 0.97 | 1.19 | 0.48 | 0.77 | 0.00 | 0.99 | 0.82 | 0.78 | 0.98 | 4.41 | 0.94 | 1.37 |
| Cervix | 0.67 (13/19.29) | 0.36 | 1.02 | 0.19 | 0.81 | 0.00 | 0.77 | 0.58 | 0.62 | 0.72 | 4.09 | 0.66 | 1.29 |
| Male genital system | 1.75a) (237/135.4) | 2.61a) | 1.85a) | 1.60a) | 1.24 | 15.20 | 2.07a) | 1.64a) | 1.66a) | 1.78a) | 1.12 | 1.81a) | 0.67 |
| Prostate | 1.76a) (233/132.72) | 2.55a) | 1.87a) | 1.60a) | 1.26 | 0.00 | 2.07a) | 1.65a) | 1.62a) | 1.81a) | 1.15 | 1.83a) | 0.69 |
| Testis | 3.66 (2/0.55) | 11.44 | 0.00 | 7.34 | 0.00 | 16.96 | 2.90 | 0.00 | 6.29 | 2.58 | 0.00 | 4.04 | 0.00 |
| Urinary system | 1.50a) (153/102.23) | 5.27a) | 1.18 | 0.79 | 0.60 | 27.08a) | 1.43a) | 1.48a) | 1.48a) | 1.51a) | 2.04 | 1.40a) | 3.89a) |
| Urinary bladder | 1.66a) (90/54.28) | 3.16a) | 1.66a) | 1.29 | 1.12 | 72.74a) | 1.91a) | 1.50a) | 1.92a) | 1.52a) | 1.25 | 1.64a) | 2.85a) |
| Kidney parenchyma | 0.43a) (16/36.86) | 2.73a) | 0.19a) | 0.00 | 0.00 | 17.20a) | 0.34a) | 0.41a) | 0.46 | 0.43a) | 0.00 | 0.46a) | 1.19 |
| Renal pelvis, other urinary | 4.24a) (47/11.09) | 24.99a) | 2.18a) | 0.94 | 0.00 | 0.00 | 4.76a) | 4.01a) | 2.26 | 5.17a) | 13.24a) | 3.40a) | 18.51a) |
| Ureter | 0.74 (4/5.38) | 3.09 | 0.45 | 0.64 | 0.00 | 0.00 | 0.00 | 1.03 | 0.00 | 1.08 | 0.00 | 0.43 | 0.00 |
| Bone, joints | 2.48 (6/2.42) | 0.00 | 3.75a) | 3.01 | 0.00 | 21.59a) | 2.61 | 0.85 | 1.12 | 3.26a) | 0.00 | 1.88 | 6.62 |
| Soft tissue including heart | 2.03a) (14/6.9) | 1.11 | 1.35 | 3.10a) | 2.74 | 22.21a) | 2.35 | 1.30 | 1.79 | 2.15a) | 0.00 | 1.81 | 6.01 |
| Melanoma of skin | 2.71a) (12/4.42) | 0.00 | 1.07 | 4.75a) | 5.43a) | 0.00 | 4.11a) | 1.85 | 2.80 | 2.67a) | 0.00 | 3.10a) | 5.23 |
| Thyroid | 2.70a) (311/115.02) | 4.29a) | 2.85a) | 2.09a) | 2.10a) | 3.13a) | 2.64a) | 2.86a) | 2.40a) | 2.79a) | 2.42 | 2.80a) | 2.24a) |
| Acute lymphocytic leukemia | 3.25a) (5/1.54) | 0.00 | 2.87 | 4.81 | 4.82 | 5.06 | 3.90 | 1.75 | 3.69 | 3.01 | 46.40a) | 2.94 | 5.43 |
RT, radiotherapy; SIR, standardized incidence ratio; O/E, observed/expected.
Significant at alpha=0.05.
Following a diagnosis of RCC, the risk of thyroid cancer as an SPC tended to decrease over time. For patients examined within 1 year after diagnosis of RCC, there was an increased risk of thyroid cancer (SIR, 4.29). For patients followed for 1-5 years, the risk decreased to an SIR of 2.85. Finally, the SIR decreased to 2.09 in patients after an even longer follow-up period (≥ 5 years). Similar findings were seen for prostate and bladder cancer. The early-onset group had higher relative risks for all SPCs than the mid or late-onset groups (SIR, 4.38). Patients who developed RCC at < 30 years of age had elevated incidences of gastric cancer as an SPC (SIR, 2.19), but those who developed RCC at 30-59 and ≥ 60 years of age had reduced incidences (SIR, 0.74 and 0.64, respectively). To investigate the potential effects of changes in the techniques and methods that were used for diagnosis and treatment, we considered two separate analysis periods (1993-2000 and 2001-2013). However, there were no significant differences in the incidence of SPCs between these periods (Table 2).
To investigate the effects of first-line treatment for RCC on the risk of SPC, we calculated SIRs according to RT, surgery, and chemotherapy. For all treatment modalities except RT, the risk of SPC was significantly higher in RCC patients than the risk of cancer in comparable members of the general population. Similarly, for all therapies, the risks of urological cancers were higher in RCC patients than in the general population. Among the 32,688 patients (81.02%) who underwent surgery as the initial therapy for RCC, the incidences of gall-bladder and cervical cancers appeared to be lower than the incidences of these cancers in the general population (SIR, 0.64 and 0.66, respectively), but did not reach statistical significance (Table 2).
During 21 years of follow-up, 12,241 of the 40,347 patients with RCC died. The 10-year overall survival (OS) rates were 60.9% and 63.1% in the SPC and non-SPC groups, respectively (p > 0.05). The 5- and 15-year OS rates in the SPC group were 81.3% and 44.7%, respectively, whereas those in the non-SPC group were 71.8% and 55.9%, respectively. The curves intersected over time. The SPC group had a higher OS rate than the non-SPC group prior to 8 years, but the rate began to decrease thereafter (Fig. 2). Among patients who developed SPC, the OS rate following SPC onset was higher for women than for men (Fig. 3).
Fig. 2.
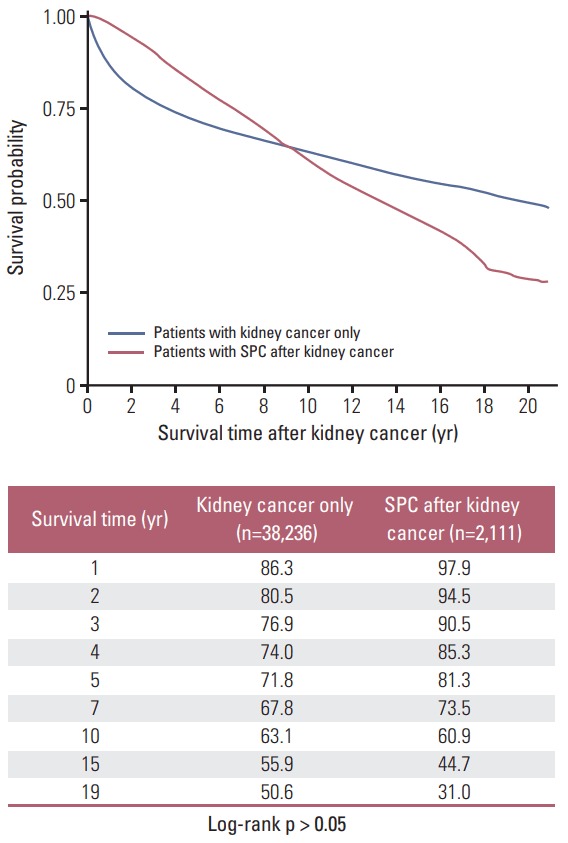
Kaplan-Meier curve: survival after kidney cancer according to whether secondary primary cancer (SPC).
Fig. 3.
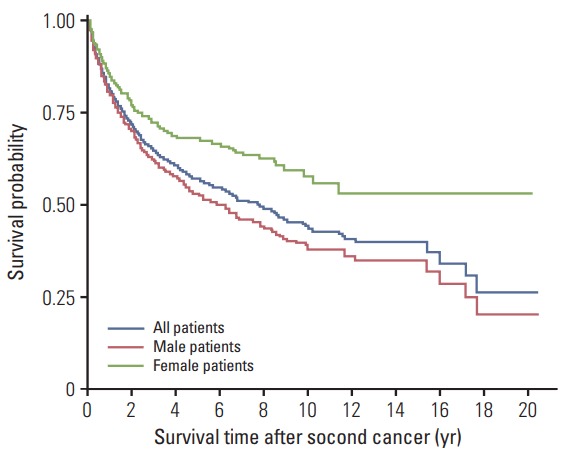
Kaplan-Meier curve: survival after second cancer according to sex in patients with second cancer.
To analyze the associations between SPC incidence and OS according to RCC stage, we performed a subgroup analysis on patients from 2006-2013. The OS curves of those with an SPC and those with RCC only (i.e., the non-SPC group) intersected 5.25 years after RCC diagnosis (S1 Fig.). Distant stage disease was present in 4.17% and 12.52% of cases in the SPC and non-SPC groups, respectively. Before 5.25 years after RCC diagnosis, the proportion of patients with distant stage disease at the time of diagnosis was 16.41%, but this value decreased to 2.47% thereafter (p < 0.05). Regarding the presence of SPC, before 5.25 years, 16.66% of cases in the non-SPC group and 6.65% of cases in the SPC group were distant stage (p < 0.05) (S2 Fig.). However, there were no differences in stage between the 2 groups after 5.25 years of follow-up (p=0.39). After 5.25 years, the survival rate of the SPC group decreased over time and was lower than that in the non-SPC group.
Discussion
Our results show that the risk of SPC in patients with a diagnosis of primary RCC was higher than the risk of cancer in the general population, a finding that is consistent with previous reports. Our results also show that—unlike other types of SPCs—the risk of developing gastrointestinal SPC was age-dependent. Patients who had RCC onset before the age of 30 years showed an elevated risk of gastric SPC, while those who developed RCC at older ages showed reduced risks of gastric SPC. In RCC survivors who undergo nephrectomy, lifestyle changes (e.g., limiting excessive dietary salt, spice food and high calorie intake, quitting smoking) are recommended to maintain the residual kidney function and prevent cancer recurrence. Such adaptations have prophylactic effects for gastric cancer [18,19], which might explain the reduced incidence of gastric cancers in those who develop RCC after the age of 30.
In the present study, we observed that patients with RCC had higher incidences of the following cancers than did comparable members of the general population: lung, breast, prostate, bladder, and renal pelvis tumor, as well as melanoma.
We observed that about 13% of all patients with RCC had one or more new primary tumors. Across previous studies, the incidence of SPC among RCC patients has been quite diverse. For instance, in a study of the SEER database during 1973-2006, Chakraborty et al. [20] found a 10% incidence of SPC in RCC. On the other hand, in a study set in Norway, Beisland et al. [21] a 47% incidence of SPC in RCC. Other studies have reported incidences of 16% and 18.5% [22,23]. The diverse incidences of SPC in the investigated registries might be explained by differences in intrinsic factors (such as genetic backgrounds and ethnic groups) and extrinsic factors (such as life styles and environment).
The immune system has been implicated in both RCC and melanoma. Interferon-α (IFN-α) and high-dose interleukin 2 (IL-2) were reported to be effective for RCC, prior to therapy using a targeted agent against metastatic RCC [24]. IL-2 stimulates T-cell proliferation and differentiation, whereas IFN-αhas antiangiogenic effects [25]. Recently, immunotherapy based on the close association between melanoma and immunity has had a profound impact on the treatment of metastatic melanoma [26]. Many studies that are currently underway use agents that target programmed death-1 (PD1) [27,28]. And these agents have been reported to have impressive antitumor effects in several malignancies, including melanoma and urologic cancer [29,30].
We also found that the incidence of thyroid SPC in patients with RCC was higher than the incidence of thyroid cancer in comparable members of the general population, regardless of age, latency, or period of diagnosis (1993-2000 vs. 2001-2013). Although we predicted that incidence of thyroid cancer would have increased due to the recent popularization of thyroid examinations, the fact that thyroid cancer was even more common in RCC patients than in the general population implies an association between RCC and thyroid cancer. Some studies have reported that patients with thyroid cancer are at risk of developing a second cancer of the kidney [31-35]. Genetic correlations between RCC and thyroid cancer might contribute to a higher risk of SPCs in a given population.
The incidence of primary thyroid cancer likely increased after 2000 because of increased surveillance, as a result of changes in health insurance coverage. Another possible hypotheses for our results are as follows. First, surveillance may need to be more frequent for cancer patients than general population. Secondly, a distinct inherited tumor syndrome has been characterized as association of papillary thyroid cancer, nodular thyroid disease, and papillary renal neoplasia [36].
The survival of patients with RCC is heavily dependent on cancer stage at the time of diagnosis. Patients who are diagnosed with advanced RCC are expected to have poor survival outcomes. However, early-stage RCC is associated with a more favorable prognosis and more than 10 years of survival following complete resection, meaning that the survival rates of patients with early-stage RCC could depend substantially on the risk of developing SPC and SPC prognosis.
In the present study, we observed that survival curves of patients with and without SPCs intersected over time. More specifically, the SPC group had a high survival rate prior to 8 years following the RCC diagnosis, but the non-SPC group had a higher survival rate thereafter. SPC risk after RCC increased with time and was higher in men (Fig. 3), whereas survival rates were higher in women.
Overall, these results indicate that the non-SPC group had significantly more cases of advanced RCC at the time of diagnosis. In addition, survival was superior in the SPC group within the first 5.25 years of diagnosis, implying that the survival rate of RCC patients might be affected by the presence of SPC.
The development of RCC and gastric cancer in relatively young patients (< 30 years) is usually due to common genetic mutations. It is already widely known that RCC is associated with mutations in the von Hippel–Lindau tumor suppressor, succinate dehydrogenase B (SDHB), c-mesenchymal-epithelial transition (c-MET), and fumarate hydratase genes [37]. Fioroni et al. [38] suggested that, despite the inconclusive results that have been obtained in multiple studies, c-MET amplification is likely to be intimately associated with gastric cancer. Peng et al. [39] reported that, in gastric cancer, higher c-MET gene expression was associated with poor prognosis. Furthermore, many studies have reported that chromosome 3p translocation of SDHB is associated with gastrointestinal stromal tumors [40-42].
The main limitations of this study are its retrospective nature and the inherent limitations of publicly available registry databases, such as underreporting (e.g., surgical treatment type, tumor size, TNM stage and grade, some of kidney cancer cell types [papillary and chromophobe type], and adjuvant treatment) after nephrectomy were not available) and the lack of some variables (e.g., RT dosage, types of systemic therapy for metastatic RCC). Additionally, some specific and relevant data were not recorded, such as on environment-lifestyle factors and comorbidities other than cancers. Furthermore, the short follow-up period was a limitation of our study. The median follow-up duration was 3.63 years in the entire study cohort. This duration is relatively short in comparison with previous studies. Therefore, further studies with longer follow-up periods should be conducted to assess the risk of SPC development with improved accuracy and to overcome surveillance bias.
In conclusion, we conducted the first nationwide analysis that has estimated the risk of SPC among patients with kidney cancer in Korea. Our analysis provides basic information on the characteristics and survival rates of patients who have primary kidney cancer and SPC. The risk of developing SPC in patients with RCC was higher than the risk of developing cancer in the general population. Most cancer types showed higher incidences in patients with RCC than in the general population. However, the relative incidence of gastric cancer as an SPC varied substantially by age. From a clinical perspective, these results suggest that patients with RCC, especially those who are long-term survivors, should be monitored carefully for the development of SPC.
Acknowledgments
This work was supported by a research grant from the National Cancer Center (No. 1610201), Republic of Korea.
Footnotes
Conflict of interest relevant to this article was not reported.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (http://www.e-crt.org).
References
- 1.Travis LB. The epidemiology of second primary cancers. Cancer Epidemiol Biomarkers Prev. 2006;15:2020–6. doi: 10.1158/1055-9965.EPI-06-0414. [DOI] [PubMed] [Google Scholar]
- 2.Wood ME, Vogel V, Ng A, Foxhall L, Goodwin P, Travis LB. Second malignant neoplasms: assessment and strategies for risk reduction. J Clin Oncol. 2012;30:3734–45. doi: 10.1200/JCO.2012.41.8681. [DOI] [PubMed] [Google Scholar]
- 3.Ljungberg B, Hanbury DC, Kuczyk MA, Merseburger AS, Mulders PF, Patard JJ, et al. Renal cell carcinoma guideline. Eur Urol. 2007;51:1502–10. doi: 10.1016/j.eururo.2007.03.035. [DOI] [PubMed] [Google Scholar]
- 4.Oh CM, Won YJ, Jung KW, Kong HJ, Cho H, Lee JK, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2013. Cancer Res Treat. 2016;48:436–50. doi: 10.4143/crt.2016.089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chen T, Fallah M, Sundquist K, Liu H, Hemminki K. Risk of subsequent cancers in renal cell carcinoma survivors with a family history. Eur J Cancer. 2014;50:2108–18. doi: 10.1016/j.ejca.2014.05.003. [DOI] [PubMed] [Google Scholar]
- 6.Liu H, Hemminki K, Sundquist J. Renal cell carcinoma as first and second primary cancer: etiological clues from the Swedish Family-Cancer Database. J Urol. 2011;185:2045–9. doi: 10.1016/j.juro.2011.02.001. [DOI] [PubMed] [Google Scholar]
- 7.Hemminki K, Boffetta P. Multiple primary cancers as clues to environmental and heritable causes of cancer and mechanisms of carcinogenesis. IARC Sci Publ. 2004;(157):289–97. [PubMed] [Google Scholar]
- 8.Travis LB, Rabkin CS, Brown LM, Allan JM, Alter BP, Ambrosone CB, et al. Cancer survivorship: genetic susceptibility and second primary cancers: research strategies and recommendations. J Natl Cancer Inst. 2006;98:15–25. doi: 10.1093/jnci/djj001. [DOI] [PubMed] [Google Scholar]
- 9.Rixe O, Rini B. Renal cell carcinoma: ten years of significant advances. Target Oncol. 2010;5:73–4. doi: 10.1007/s11523-010-0150-9. [DOI] [PubMed] [Google Scholar]
- 10.Rini BI, Campbell SC, Rathmell WK. Renal cell carcinoma. Curr Opin Oncol. 2006;18:289–96. doi: 10.1097/01.cco.0000219260.60714.c4. [DOI] [PubMed] [Google Scholar]
- 11.Shin HR, Won YJ, Jung KW, Kong HJ, Yim SH, Lee JK, et al. Nationwide cancer incidence in Korea, 1999~2001; first result using the national cancer incidence database. Cancer Res Treat. 2005;37:325–31. doi: 10.4143/crt.2005.37.6.325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, et al. Cancer incidence in five continents. Vol. 9. Lyon: IARC Press; 2007. [Google Scholar]
- 13.Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin L, Parkin DM, et al. International classification of diseases for oncology. 3rd ed. Geneva: World Health Organization; 2000. [Google Scholar]
- 14.Cho YY, Lim J, Oh CM, Ryu J, Jung KW, Chung JH, et al. Elevated risks of subsequent primary malignancies in patients with thyroid cancer: a nationwide, population-based study in Korea. Cancer. 2015;121:259–68. doi: 10.1002/cncr.29025. [DOI] [PubMed] [Google Scholar]
- 15.International Agency for Research on Cancer. World Health Organization. International Association of Cancer Registries. European Network of Cancer Registries . International rules for multiple primary cancers (ICD-O third edition) Lyon: International Agency for Research on Cancer; 2004. [Google Scholar]
- 16.Curtis RE, Freedman DM, Ron E, Ries LA, Hacker DG, Edwards BK, et al. New malignancies among cancer survivors: SEER cancer registries, 1973-2000. NIH Publ. No. 05-5302. Bethesda, MD: National Cancer Institute; 2006. [Google Scholar]
- 17.Esteve J, Benhamou E, Raymond L. Statistical methods in cancer research. Vol. IV. Descriptive epidemiology. IARC scentific publication. No. 128. Lyon: International Agency for Research on Cancer; 1994. [PubMed] [Google Scholar]
- 18.Tsugane S. Salt, salted food intake, and risk of gastric cancer: epidemiologic evidence. Cancer Sci. 2005;96:1–6. doi: 10.1111/j.1349-7006.2005.00006.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tsugane S, Sasazuki S, Kobayashi M, Sasaki S. Salt and salted food intake and subsequent risk of gastric cancer among middle-aged Japanese men and women. Br J Cancer. 2004;90:128–34. doi: 10.1038/sj.bjc.6601511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chakraborty S, Tarantolo SR, Batra SK, Hauke RJ. Incidence and prognostic significance of second primary cancers in renal cell carcinoma. Am J Clin Oncol. 2013;36:132–42. doi: 10.1097/COC.0b013e3182438ddf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Beisland C, Talleraas O, Bakke A, Norstein J. Multiple primary malignancies in patients with renal cell carcinoma: a national population-based cohort study. BJU Int. 2006;97:698–702. doi: 10.1111/j.1464-410X.2006.06004.x. [DOI] [PubMed] [Google Scholar]
- 22.Rabbani F, Reuter VE, Katz J, Russo P. Second primary malignancies associated with renal cell carcinoma: influence of histologic type. Urology. 2000;56:399–403. doi: 10.1016/s0090-4295(00)00682-8. [DOI] [PubMed] [Google Scholar]
- 23.Thompson RH, Leibovich BC, Cheville JC, Webster WS, Lohse CM, Kwon ED, et al. Second primary malignancies associated with renal cell carcinoma histological subtypes. J Urol. 2006;176:900–3. doi: 10.1016/j.juro.2006.04.080. [DOI] [PubMed] [Google Scholar]
- 24.Sun M, Lughezzani G, Perrotte P, Karakiewicz PI. Treatment of metastatic renal cell carcinoma. Nat Rev Urol. 2010;7:327–38. doi: 10.1038/nrurol.2010.57. [DOI] [PubMed] [Google Scholar]
- 25.Mataraza JM, Gotwals P. Recent advances in immuno-oncology and its application to urological cancers. BJU Int. 2016;118:506–14. doi: 10.1111/bju.13518. [DOI] [PubMed] [Google Scholar]
- 26.Davey RJ, van der Westhuizen A, Bowden NA. Metastatic melanoma treatment: combining old and new therapies. Crit Rev Oncol Hematol. 2016;98:242–53. doi: 10.1016/j.critrevonc.2015.11.011. [DOI] [PubMed] [Google Scholar]
- 27.Hu-Lieskovan S, Mok S, Homet Moreno B, Tsoi J, Robert L, Goedert L, et al. Improved antitumor activity of immunotherapy with BRAF and MEK inhibitors in BRAF(V600E) melanoma. Sci Transl Med. 2015;7:279ra41. doi: 10.1126/scitranslmed.aaa4691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Massari F, Santoni M, Ciccarese C, Santini D, Alfieri S, Martignoni G, et al. PD-1 blockade therapy in renal cell carcinoma: current studies and future promises. Cancer Treat Rev. 2015;41:114–21. doi: 10.1016/j.ctrv.2014.12.013. [DOI] [PubMed] [Google Scholar]
- 29.Mahoney KM, Freeman GJ, McDermott DF. The next immune-checkpoint inhibitors: PD-1/PD-L1 blockade in melanoma. Clin Ther. 2015;37:764–82. doi: 10.1016/j.clinthera.2015.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Carosella ED, Ploussard G, LeMaoult J, Desgrandchamps F. A systematic review of immunotherapy in urologic cancer: evolving roles for targeting of CTLA-4, PD-1/PD-L1, and HLA-G. Eur Urol. 2015;68:267–79. doi: 10.1016/j.eururo.2015.02.032. [DOI] [PubMed] [Google Scholar]
- 31.Rubino C, de Vathaire F, Dottorini ME, Hall P, Schvartz C, Couette JE, et al. Second primary malignancies in thyroid cancer patients. Br J Cancer. 2003;89:1638–44. doi: 10.1038/sj.bjc.6601319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ronckers CM, McCarron P, Ron E. Thyroid cancer and multiple primary tumors in the SEER cancer registries. Int J Cancer. 2005;117:281–8. doi: 10.1002/ijc.21064. [DOI] [PubMed] [Google Scholar]
- 33.Berthe E, Henry-Amar M, Michels JJ, Rame JP, Berthet P, Babin E, et al. Risk of second primary cancer following differentiated thyroid cancer. Eur J Nucl Med Mol Imaging. 2004;31:685–91. doi: 10.1007/s00259-003-1448-y. [DOI] [PubMed] [Google Scholar]
- 34.Edmonds CJ, Smith T. The long-term hazards of the treatment of thyroid cancer with radioiodine. Br J Radiol. 1986;59:45–51. doi: 10.1259/0007-1285-59-697-45. [DOI] [PubMed] [Google Scholar]
- 35.Akslen LA, Glattre E. Second malignancies in thyroid cancer patients: a population-based survey of 3658 cases from Norway. Eur J Cancer. 1992;28:491–5. doi: 10.1016/s0959-8049(05)80085-1. [DOI] [PubMed] [Google Scholar]
- 36.Malchoff CD, Sarfarazi M, Tendler B, Forouhar F, Whalen G, Joshi V, et al. Papillary thyroid carcinoma associated with papillary renal neoplasia: genetic linkage analysis of a distinct heritable tumor syndrome. J Clin Endocrinol Metab. 2000;85:1758–64. doi: 10.1210/jcem.85.5.6557. [DOI] [PubMed] [Google Scholar]
- 37.Cohen HT, McGovern FJ. Renal-cell carcinoma. N Engl J Med. 2005;353:2477–90. doi: 10.1056/NEJMra043172. [DOI] [PubMed] [Google Scholar]
- 38.Fioroni I, Dell'Aquila E, Pantano F, Intagliata S, Caricato M, Vincenzi B, et al. Role of c-mesenchymal-epithelial transition pathway in gastric cancer. Expert Opin Pharmacother. 2015;16:1195–207. doi: 10.1517/14656566.2015.1037739. [DOI] [PubMed] [Google Scholar]
- 39.Peng Z, Zhu Y, Wang Q, Gao J, Li Y, Li Y, et al. Prognostic significance of MET amplification and expression in gastric cancer: a systematic review with meta-analysis. PLoS One. 2014;9:e84502. doi: 10.1371/journal.pone.0084502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Miettinen M, Lasota J. Succinate dehydrogenase deficient gastrointestinal stromal tumors (GISTs): a review. Int J Biochem Cell Biol. 2014;53:514–9. doi: 10.1016/j.biocel.2014.05.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Niemeijer ND, Papathomas TG, Korpershoek E, de Krijger RR, Oudijk L, Morreau H, et al. Succinate dehydrogenase (SDH)-deficient pancreatic neuroendocrine tumor expands the SDH-related tumor spectrum. J Clin Endocrinol Metab. 2015;100:E1386–93. doi: 10.1210/jc.2015-2689. [DOI] [PubMed] [Google Scholar]
- 42.Doyle LA, Nelson D, Heinrich MC, Corless CL, Hornick JL. Loss of succinate dehydrogenase subunit B (SDHB) expression is limited to a distinctive subset of gastric wild-type gastrointestinal stromal tumours: a comprehensive genotype-phenotype correlation study. Histopathology. 2012;61:801–9. doi: 10.1111/j.1365-2559.2012.04300.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.