

Abstract
Objective
Using prospectively gathered data across a 35-year follow-up interval, we assessed the association of educational achievement and school behaviors with risk for the development of an alcohol-use disorder in adulthood.
Method
The baseline population consisted of 1,242 first-grade students in 1966–1967 residing in the Woodlawn community of Chicago, Illinois. Follow-up interviews were completed for adolescents and their mothers (1975–1976), during young adulthood (1992–1993), and midlife (2002–2003). A total of 1,052 individuals completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder. Logistic regression with multiple imputation to account for missing information was used to assess the relationships between early-educational and school-behavior characteristics with onset of a DSM-III-R/DSM-IV alcohol-use disorder (defined using the Composite International Diagnostic Interview).
Results
Relatively few of the hypothesized educational predictors were associated with risk for alcohol-use disorders in adulthood. The measures found to be predictive of a subsequent alcohol-use disorder included the following: (1) math achievement among first-grade boys, (2) mothers’ report of skipping school among adolescent males, (3) self-report of skipping school among adolescent girls, and (4) school dropout. Early shyness among first-grade boys was protective for later alcohol-use disorders.
Conclusions
The current report supplies data on the association of educational characteristics and school behaviors with the development of an alcohol-use disorder in a population-based sample with an extended interval of follow-up. Gender-specific differences are discussed.
Educational level, scholastic achievement, and school behaviors are linked to alcohol consumption and alcohol-use disorders in a number of ways. We know, for example, that students who drink heavily tend to do less well in classes and are more likely to leave school prematurely. This may be due to interference with school bonding (Hawkins et al., 1999; Guo et al., 2001; McBride et al., 1995) and reduction or cessation of age-appropriate prosocial activities (Costa et al., 1999; Prinstein et al., 2001; Spoth et al., 1996) as well as to direct ethanol toxicity on cerebral functioning (e.g., Ratti et al., 1999, 2002; Zeigler et al., 2005). On the other hand, there is evidence supporting the reciprocal relationships that specific behaviors during school and the failure to achieve educational goals may predict the subsequent development of maladaptive drinking behavior and alcohol-use disorders (Crum et al., 1992, 1998; Riala et al., 2003; Schulenberg et al., 1994). These relationships also may differ by race or ethnicity (Crum and Anthony, 2000).
During grade school and adolescence, successfully completing school is considered one of the principal social role expectations for this stage of life. Whether failure in this area has a lasting impact on future risk for alcohol-use disorders has largely been unexplored. For these types of explorations, data that provide information across extended periods and that access differential life stages are needed. Some prior literature links the failure to meet social role expectations with subsequent development of problem behavior (Jessor and Jessor, 1977; Jones, 1968, 1971; Kellam and Ensminger, 1980; Loper et al., 1973; McCord and McCord, 1962; Robins et al., 1962). For example, in the classic longitudinal study conducted by Jessor and colleagues (Donovan et al., 1983; Jessor and Jessor, 1977), a low value placed on academic achievement and low expectations for academic recognition in adolescence correlated with problem drinking in adulthood. Based on this type of developmental research, we inferred a relationship between poor performance of social roles at one stage in life (early childhood and adolescence) with the development of problem behavior at a later stage (young adulthood and midlife). Being successful in school could be viewed as a social role expectation at one stage in life, and the inability to achieve this goal (e.g., poor grades, skipping classes) may be associated with the subsequent development of heavy drinking and ultimately alcohol abuse and/or dependence.
Using data from the Woodlawn Study in a prior examination of early school behaviors with risk of alcohol-use disorders in young adulthood, we found that specific predictors could be identified as early as first grade (Crum et al., 1998). In the current study, we aimed to extend these analyses to examine educational achievement and school behaviors as potential risk factors for alcohol abuse and/or dependence across a 35-year follow-up interval, into midlife. Hypothesizing that poor academic performance and maladaptive school behaviors in grade school and adolescence would be associated with an increased risk of alcohol disorders in midlife, we examined a variety of characteristics that represent a range of school involvement and educational achievement factors. These included academic performance (school grades, standardized test scores), maladaptive school behaviors (being suspended, skipping school), educational level and school dropout (highest grade completed), scholastic aspirations, and assessments from multiple raters (teachers and mothers).
Method
Data collection and sample population
The original study population (n = 1,242) consisted of nearly all children (13 families did not participate) from the first-grade classrooms in the Woodlawn community, a relatively poor black community on the south side of Chicago, IL. First-grade students at nine public and three parochial schools were included in the study. Because nearly all first-grade students in this community were assessed, potential selection biases related to study inclusion were virtually eliminated. Beginning in 1966–1967, the study participants were followed longitudinally for 35 years. They were assessed in first grade, at age 16–17 (1975–1976), in young adulthood (ages 32–33), and in midlife (ages 42–43). Data were also obtained through public records (school records, police arrest records, and motor vehicle records).
In 1992–1993, a total of 952 young adult participants were re-interviewed. Most recently, in 2002–2003, 72.2% of those who survived and were not incapacitated participated in the midlife interview (n = 833, see Figure 1). Written informed consent was obtained for study participation. A total of 135 refused or otherwise could not be interviewed. The remainder (n = 185) could not be located. Since the study began, 91 individuals have died or have become incapacitated. Relative to study participants who reported moderate or light use of distilled spirits during adolescence, participants who reported heavy use of distilled spirits were less likely to be located and interviewed and had a greater probability of death prior to the follow-up interview. In addition, high-school dropouts were less likely to be located and interviewed compared with those with a General Educational Development or general equivalency diploma (GED) or regular high-school diploma. However, attrition was not associated with beer, wine, or marijuana use during adolescence. In addition, there were no differences in the proportion interviewed as measured by first-grade reports of shy and aggressive behavior, mother’s educational level, and time spent in poverty or receiving welfare assistance.
Figure 1.
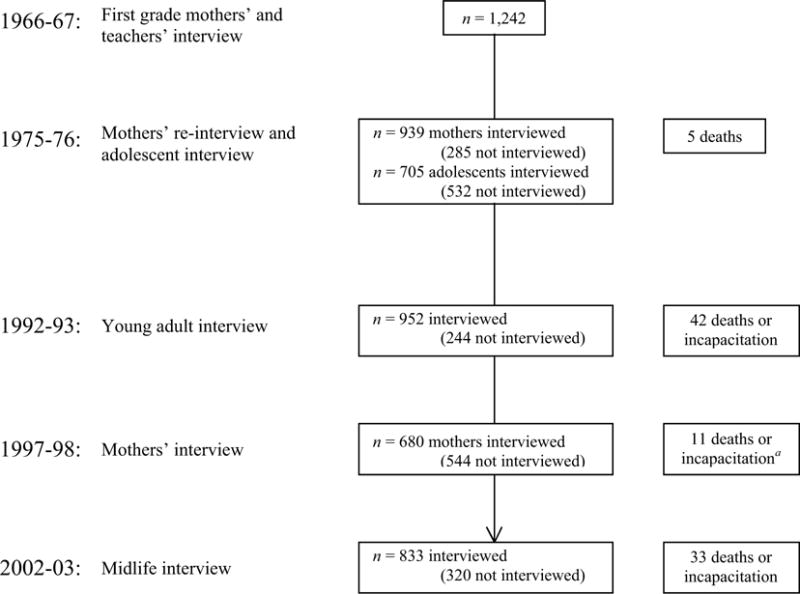
Diagram of the data collection for the Woodlawn Study. The analyses presented in this article are based on an overall sample size of 1,052, using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder. “Not interviewed” represents those who could not be located as well as those who refused to be interviewed. A total of 18 mothers had more than one child enrolled in the study. aThe mothers’ interview provided additional information on participants’ death or incapacitation.
The current analyses are based on an overall sample size of 1,052, using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder. Because our principal goal was to assess educational achievement and school behaviors as potential predictors of subsequent alcohol-use disorders, in the analyses of educational information gathered from the adolescent and adult interviews, we excluded the 46 participants who reported that the age of alcohol-use disorder onset was prior to age 18 (n = 1,006). Age of onset was defined as the age at which the first symptom of an alcohol-use disorder occurred. Our concern was that early drinking problems may have led to school dropout rather than the reverse.
Instrument and measures
Interviews in first grade (1966–1967)
The rating of children’s behavior in first grade was based on reports from mothers and teachers. Teachers were interviewed on three separate occasions: (1) early, (2) middle, and (3) late in the first-grade year. We used the third teacher interview for these analyses. Teachers identified five types of maladaptive behavior by reporting the excessive presence of the following: (1) lacking in involvement with classmates (e.g., shy, timid, alone too much, daydreamer, friendless, aloof); (2) aggressive behavior (e.g., fights too much, steals, lies, resists authority, is destructive to others or property, obstinate, disobedient, uncooperative); (3) immature behavior (e.g., acts too young physically and/or emotionally, cries too much, has tantrums, sucks thumb, is physically poorly coordinated, masturbates, urinates in class, seeks too much attention); (4) not working up to ability (e.g., does not learn as well as assessment of ability indicates); and (5) restlessness (e.g., fidgets, is unable to sit still in classroom). In the teachers’ interview, children were ranked on a 4-point scale that used “0” to indicate that the student was within minimal limits of acceptable behavior, “1” to indicate mildly excessive, “2” to indicate moderately excessive, and “3” to indicate severely excessive. The mothers’ interview included similar descriptions of these five maladaptive types of behavior, and mothers were asked to indicate whether their child was not at all that way (0), just a little that way (1), quite a bit that way (2), or very much that way (3). Responses were categorized separately for mothers and teachers.
Interviews during adolescence (1975–1976)
Items from the adolescent interview included self-reports of skipping school, being suspended, and educational expectations and included (1) “Please tell me how many times you’ve (skipped a day at school without a real excuse/been suspended from school) in the last 3 years?” (answer choices were the following: [1] never, [2] once, [3] twice, [4] three or four times, and [5] five or more times); and (2) “How far do you think you really will go the way it looks now?” (answer choices were the following: [1] some high school, [2] finish high school, [3] some college, [4] finish college, and [5] beyond college). Mothers were asked similar questions. The items were included as continuous variables in the analyses. Log transformations of these variables yielded comparable findings (data not shown).
Math and reading achievement (first, seventh, and eighth grades)
Reports of scores on the Metropolitan Readiness Test, math, and reading grades in first grade as well as standardized math and reading scores in seventh and eighth grades were assessed. Because correlations of seventh and eighth grade scores were high (for math scores: r = .61, p < .001; for reading scores: r = .69, p < .001), we used a mean of the scores from the two grades to represent scores during adolescence. Results from each of the tests had a normal distribution, such that continuous measures of the test scores were included in the regression models.
Educational level and school dropout
Information on the highest level of schooling achieved was based on self-report information gathered in the adult interviews. In addition, these data were supplemented by assessments of school records and mothers’ reports (1997–1998 interview).
Alcohol-use disorder diagnoses
The presence of an alcohol-use disorder (alcohol abuse or dependence) in the young adult and midlife interviews was assessed based on computer algorithms of data gathered with the Michigan version of the Composite International Diagnostic Interview (CIDI; Kessler et al., 1994; Robins et al., 1988). In the young adult interview (1992–1993), the diagnoses were based on criteria from the DSM-III-R (American Psychiatric Association, 1987). By the time of the midlife interview (2002–2003), the DSM-IV (American Psychiatric Association, 1994) had been adopted, and survey questions reflected the new DSM-IV criteria. Concordance between DSM-III-R and DSM-IV diagnoses of current and lifetime alcohol abuse and dependence is reported to be good to excellent among population-based samples of adults and adolescents (e.g., Grant, 1996; Hasin et al., 1996a,b; Pollock et al., 2000), particularly when classifications for alcohol abuse and dependence are combined (any alcohol-use disorder; Grant, 1993, 1992; Hasin et al., 1996a,b; Pollock et al., 2000). In the current study, a lifetime diagnosis of DSM-III-R (from the young adult interview) and/or DSM-IV (midlife interview) alcohol-use disorder was used as the dependent variable.
Statistical analysis
After initial descriptive analyses were completed, logistic regression models were used to estimate degree of association between measures of schooling and educational achievement with the occurrence of an alcohol-use disorder in adulthood at the time of the young adult or midlife interview. All study participants are of similar age and racial or ethnic background, and all were residents of the same community as children. Because of the association of maternal drinking history with development of alcohol-use disorders in this population (odds ratio [OR] = 1.57, 95% confidence interval [CI]: 1.01–2.44, p = .047), the multiple logistic regression analyses were completed while holding constant report of maternal history of regular drinking. In a departure from our prior assessment of educational characteristics with alcohol-use disorders with this sample (Crum et al., 1998), we chose to stratify all the analyses by sex instead of simply including this covariate in the multivariate regression models. This was done to explore potential sex-specific differences in the relationships of educational characteristics with alcohol-use disorders. Prevalence and incidence of alcohol abuse and dependence is well documented to be higher among males as compared with females (Eaton et al., 1989; Grant et al., 2004; Helzer et al., 1991; Kessler et al., 1997). In addition, high-school dropout rates (Ensminger and Slusarcick, 1992; Kominski, 1990) and risk trajectories also may differ by sex (Blume, 1986; Lex, 1991; Schmidt et al., 1990; Wilsnack and Wilsnack, 1993).
To include information from participants with missing data, we used multiple imputations in the logistic regression analyses. Missing data refer to various types of data incompleteness arising from nonresponse to certain questions or longitudinal panel dropouts. In general, the Woodlawn Study suffered little from nonresponse to specific questions: If respondents agreed to participate, they generally did not refuse to answer specific questions. However, all longitudinal studies suffer from some degree of attrition, which may reflect any one or more of the following: (1) an inability to locate participants, (2) the refusal of panel members to participate, (3) mortality, or (4) the physical or mental incapacity to participate. Modern software programs for handling unbalanced longitudinal data improve on methods that discard the incomplete cases by including all the data, but also may yield biased inferences under plausible models for the dropout process, specifically when dropout is nonrandom. A number of methods that provide for nonrandom dropout processes have been proposed (Allison, 2001; Diggle and Kenward, 1994; Little, 1993, 1994; Little and Rubin, 1987; Schafer, 1997). Little (1995) reviewed these methods and suggested that different types of missing data have different solutions for analysis. One type of missing data is that which does not seem to depend on the outcome but does depend on the covariates (covariate-dependent dropout or missing at random [MAR]). In our sample, we found that the most common missing data classification was data that were missing at random or for which the dropout mechanism did not depend on the outcome values (e.g., alcohol-use disorder) but did vary with the value of fixed covariates measured at baseline (e.g., school performance). Based on the assumption of MAR, we incorporated multiple imputations in our regression analyses using SAS PROC MI (version 9.1; SAS Institute Inc., Cary, NC). An expectation-maximization (EM) algorithm (Dempster et al., 1977) for maximum likelihood (ML) estimation of an unstructured covariance matrix is available in SAS (Yuan, 2000). Because approximately 40% of the data were missing when all four waves of the data were included, we used 10 multiple imputed datasets. We compared the results of listwise deletion (n = 634) and multiple imputed data (n = 1,052). We found that the coefficients from the imputed data were not markedly different from those found when using listwise deletion. However, the reported standard errors are much lower, leading to higher test statistics and lower p values.
Results
In our sample, we identified a total of 246 cases of an alcohol-use disorder from data gathered at the young adult and midlife interviews (Table 1). Because the sample was originally identified from first-grade students living in the Woodlawn community, there are no age and race differences between the alcohol-use disorder cases and noncases. As would be expected based on prior epidemiological studies of alcohol abuse and dependence (Crum et al., 1992; Grant et al., 2004; Helzer et al., 1991; Kessler et al., 1997), cases were more likely to be male and to have dropped out of school before getting a high-school diploma. Maternal educational level was not associated with case status. However, mothers of cases were more likely to self-report regular alcohol use.
Table 1.
Frequency distribution of characteristics for cases and noncases of DSM-III-R or DSM-IV alcohol abuse and/or dependence; data are from the Woodlawn Studya
| Characteristics | Cases (n = 246, 23.4%) |
Noncases (n = 806, 76.6%) |
t or χ2, df, pb |
|---|---|---|---|
| Age, mean (SD) years | 42.7 (0.49) | 42.8 (0.53) | t = 0.24, 1,047 df, p = .807 |
| Sex, n (%) | |||
| Men | 172 (69.9%) | 332 (41.2%) | χ2 = 62.33, 1 df, |
| Women | 74 (30.1%) | 474 (58.8%) | p < .001 |
| Race/ethnicity, n (%)c | |||
| Black | 244 (99.2%) | 795 (99.3%) | χ2 = 0.01, 1 df, |
| Other | 2 (0.8%) | 6 (0.7%) | p = .920 |
| Educational level of study participant, n (%)d | |||
| No diploma | 67 (27.2%) | 133 (16.6%) | χ2 = 28.28, 4 df, |
| General Equivalency Diploma (GED) | 25 (10.2%) | 49 (6.1%) | p < .001 |
| Regular high-school diploma | 81 (32.9%) | 259 (32.3%) | |
| College, no degree | 57 (23.2%) | 248 (30.9%) | |
| College degreee | 16 (6.5%) | 113 (14.1%) | |
| Mother’s educational level, mean (SD) years | 10.5 (2.27) | 10.7 (2.34) | t = 1.06, 1,037 df, p = .289 |
| Mother’s drinking history, n (%) | |||
| Self-reported regular use of alcohol | 32 (15.9%) | 60 (9.6%) | χ2 = 6.18, 1 df, |
| No regular alcohol use | 169 (84.1%) | 566 (90.4%) | p = .013 |
Notes: DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; DSM-IV = DSM, Fourth Edition.
The data are based on our overall sample of 1,052 participants (using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder). Information on mother’s regular use of alcohol was obtained from the mother’s interview when the child was an adolescent (827 mothers of the 1,052 sample provided this information);
chi-square, degrees of freedom, p value: for analyses that include a cell with less than 10, the p value for Fisher’s exact test is reported; for analyses involving mean years the t test p value is reported;
a total of five noncases (0.6% of noncases) did not provide information on race/ethnicity and were not included in the analyses involving race/ethnicity;
for four noncases (0.5% of noncases), we did not have information on educational level, and these participants were not included in the analyses involving that educational level;
associate of arts degree and higher.
Only a few of the hypothesized educational characteristics were associated with a subsequent risk for alcohol-use disorders. Among male participants, higher achievement in first-grade math was associated with a decreased risk of developing alcohol abuse or dependence in adulthood (Table 2). However, achievement in math and reading in either first grade or during adolescence was not associated with the onset of an alcohol-use disorder among female participants. Relative to first-grade boys who were neither shy nor aggressive, boys who were shy were less likely to develop an alcohol-use disorder in adulthood (Table 3). However, these teacher ratings did not predict the occurrence of alcohol abuse or dependence for girls. In addition, teachers’ and mothers’ assessment of first-grade achievement (Table 3) and mothers’ and adolescents’ report of educational expectations (Table 4) were not associated with risk for an alcohol-use disorder among either male or female participants. Yet some school behaviors during adolescence did predict adult-onset alcoholism, including self-reports of higher frequency of skipping school among girls and the mothers’ report of skipping school among boys (Table 5). Relative to those with a college degree or higher education, risk of developing an alcohol-use disorder was greatest for males who had dropped out of school before getting their diploma (OR = 3.37, 95% CI: 1.36–8.34; Table 6). Interestingly, risk was also associated with having a regular high-school diploma among males (OR = 2.38, 95% CI: 1.01–5.68) but not among those who dropped out but then got a GED. Among females, the pattern differed. Relative to females with a college degree, the risk of developing an alcohol-use disorder was appreciably elevated for those who dropped out of school and then obtained a GED (OR = 3.85, 95% CI: 1.07–13.85).
Table 2.
Association of developing a DSM-III-R/DSM-IV alcohol-use disorder by school performance using scores from the Metropolitan Readiness Test and standardized tests as well as first-grade math and reading grades, based on logistic regression analyses with imputation, stratified by gender; data are from the Woodlawn Study (n = 1,052)a
| School performance: Grades and test scoresb |
Unadjusted OR (95% CI), p |
Adjusted ORc (95% CI), p |
|---|---|---|
| Men (n = 504) | ||
| Metropolitan Readiness Testd | 0.99 (0.98–1.01), p = .55 | 0.99 (0.98–1.01), p = .55 |
| Math, first grade | 0.78 (0.62–0.99), p = .04 | 0.78 (0.62–0.98), p = .04 |
| Reading, first grade | 0.86 (0.67–1.11), p = .24 | 0.87 (0.68–1.12), p = .27 |
| Standardized math scores, seventh/eighth graded,e | 0.99 (0.98–1.02), p = .93 | 0.99 (0.98–1.02), p = .92 |
| Standardized reading scores, seventh/eighth graded,e | 0.99 (0.98–1.01), p = .61 | 0.99 (0.98–1.01), p = .62 |
| Women (n = 548) | ||
| Metropolitan Readiness Testd | 0.99 (0.98–1.01), p = .97 | 1.00 (0.98–1.01), p = .89 |
| Math, first grade | 1.04 (0.76–1.41), p = .82 | 1.04 (0.76–1.42), p = .79 |
| Reading, first grade | 0.87 (0.63–1.21), p = .42 | 0.89 (0.64–1.25), p = .50 |
| Standardized math scores, seventh/eighth graded,e | 0.99 (0.97–1.01), p = .49 | 0.99 (0.97–1.01), p = .52 |
| Standardized reading scores, seventh/eighth graded,e | 1.01 (0.98–1.02), p = .78 | 1.00 (0.98–1.02), p = .71 |
Notes: DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; DSM-IV = DSM, Fourth Edition; OR = odds ratio; CI = confidence interval.
The data are based on our overall sample of 1,052 participants (using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder);
grades and test scores were included as continuous variables in each logistic regression model;
each logistic regression model includes a covariate for mothers’ self-report of regular alcohol use; separate logistic regression models were completed for each school-performance outcome measure;
for the math scores, mean (SD) = 87.55 (12.15), range: 45–131; for the reading scores, mean = 84.98 (14.24), range: 24–136.50; and for the Metropolitan Readiness Test, mean = 58.07 (18.53), range: 2–98;
the mean of the seventh- and eighth-grade standardized scores was included in the model as a continuous variable.
Table 3.
Association of developing a DSM-III-R/DSM-IV alcohol-use disorder by ratings from the child’s mother and teacher of their classroom behavior and achievement level in first grade, based on logistic regression analyses using multiple imputations, stratified by gender; data are from the Woodlawn Study (n = 1,052)a
| First-grade classroom behavior and achievement level | Unadjusted OR (95% CI), p |
Adjusted ORb (95% CI), p |
|---|---|---|
| Men (n = 504) | ||
| Teachers’ rating of classroom behavior | ||
| Shy only | 0.58 (0.33–0.98), p = .03 | 0.62 (0.32–0.97), p = .02 |
| Aggressive only | 1.06 (0.65–1.74), p = .40 | 1.17 (0.31–1.35), p = .37 |
| Both shy and aggressive | 1.11 (0.68–1.83), p = .27 | 1.23 (0.52–1.98), p = .25 |
| Neither shy or aggressivec | 1.00 | 1.00 |
| Teachers’ ratings of underachievement | ||
| Any | 1.40 (0.97–2.03), p = .07 | 1.36 (0.94–1.98), p = .09 |
| Nonec | 1.00 | 1.00 |
| Mothers’ rating of underachievement | ||
| Any | 0.86 (0.60–1.25), p = .43 | 0.87 (0.60–1.26), p = .46 |
| Nonec | 1.00 | 1.00 |
| Women (n = 548) | ||
| Teachers’ rating of classroom behavior | ||
| Shy only | 0.84 (0.40–1.75), p = .43 | 0.80 (0.46–1.96), p = .43 |
| Aggressive only | 1.38 (0.70–2.71), p = .31 | 1.30 (0.67–2.81), p = .33 |
| Both shy and aggressive | 1.05 (0.47–2.36), p = .99 | 1.03 (0.41–2.89), p = .91 |
| Neither shy or aggressivec | 1.00 | 1.00 |
| Teachers’ ratings of underachievement | ||
| Any | 1.46 (0.89–2.39), p = .14 | 1.49 (0.90–2.46), p = .12 |
| Nonec | 1.00 | 1.00 |
| Mothers’ rating of underachievement | ||
| Any | 1.55 (0.95–2.54), p = .08 | 1.54 (0.94–2.53), p = .08 |
| Nonec | 1.00 | 1.00 |
Notes: DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; DSM-IV = DSM, Fourth Edition; OR = odds ratio; CI = confidence interval.
The data are based on our overall sample of 1,052 participants (using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder);
each logistic regression model includes a covariate for mothers’ self-report of regular alcohol use; separate logistic regression models were completed for each school-behavior and achievement-outcome measure;
reference category.
Table 4.
Association of developing a DSM-III-R/DSM-IV alcohol-use disorder by the mothers’ and adolescents’ report of educational expectations, based on logistic regression analyses using multiple imputations, stratified by gender; data are from the Woodlawn Study (n = 1,006)a
| Educational expectationsb | Uadjusted OR (95% CI), p |
Adjusted ORc (95% CI), p |
|---|---|---|
| Men (n = 467) | ||
| Mothers’ expectations reported in first graded | 0.89 (0.75–1.07), p = .22 | 0.90 (0.75–1.07), p = .24 |
| Mothers’ expectations reported during adolescence | 0.95 (0.78–1.17), p = .64 | 0.95 (0.77–1.17), p = .63 |
| Adolescents’ expectations | 0.90 (0.71–1.15), p = .39 | 0.90 (0.71–1.15), p = .40 |
| Women (n = 539) | ||
| Mothers’ expectations reported in first gradee | 0.82 (0.64–1.06), p = .12 | 0.83 (0.65–1.07), p = .15 |
| Mothers’ expectations reported during adolescence | 0.92 (0.71–1.19), p = .53 | 0.92 (0.71–1.19), p = .54 |
| Adolescents’ expectations | 1.04 (0.79–1.37), p = .76 | 1.08 (0.81–1.42), p = .61 |
Notes: DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; DSM-IV = DSM, Fourth Edition; OR = odds ratio; CI = confidence interval.
The analyses are based on an overall sample size of 1,052, using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder; in the analyses of educational information gathered from the adolescent and adult interviews, we excluded the 46 participants who reported that the age of alcohol-use disorder onset was prior to age 18 (n = 1,006); age of onset was defined as the age for which the first alcohol-use disorder symptom occurred;
education expectations are included as continuous variables with increasing score indicative of higher expectation for level of schooling to be completed; log transformation yielded comparable findings;
each logistic regression model includes a covariate for mothers’ self-report of regular alcohol use; separate logistic regression models were completed for each educational-expectation outcome;
analyses of the reports by mothers of first-grade boys are based on an imputed sample size of 504;
analyses of the reports by mothers of first-grade girls are based on an imputed sample size of 548.
Table 5.
Association of developing a DSM-III-R/DSM-IV alcohol-use disorder by school behaviors during adolescence as reported by the mother and adolescent, based on logistic regression analyses using multiple imputations, stratified by gender; data are from the Woodlawn Study (n = 1,006)a
| School behaviors during adolescenceb | Unadjusted OR (95% CI), p |
Adjusted ORc (95% CI), p |
|---|---|---|
| Men (n = 467) | ||
| Mothers’ report | ||
| Suspension from school | 1.00 (0.80–1.25), p = .97 | 1.01 (0.80–1.26), p = .98 |
| Skipping school | 1.22 (1.02–1.46), p = .03 | 1.22 (1.02–1.46), p = .03 |
| Adolescents’ report | ||
| Suspension from school | 1.13 (0.94–1.35), p = .18 | 1.13 (0.94–1.35), p = .18 |
| Skipping school | 1.06 (0.89–1.26), p = .52 | 1.06 (0.89–1.25), p = .52 |
| Women (n = 539) | ||
| Mothers’ report | ||
| Suspension from school | 1.28 (0.92–1.77), p = .14 | 1.20 (0.85–1.68), p = .29 |
| Skipping school | 1.02 (0.80–1.30), p = .90 | 0.99 (0.78–1.28), p = .91 |
| Adolescents’ report | ||
| Suspension from school | 1.21 (0.95–1.55), p = .12 | 1.20 (0.94–1.54), p = .14 |
| Skipping school | 1.25 (1.01–1.54), p = .04 | 1.24 (1.01–1.53), p = .05 |
Notes: DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; DSM-IV = DSM, Fourth Edition; OR= odds ratio; CI = confidence interval.
The analyses are based on an overall sample size of 1,052, using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder; in the analyses of educational information gathered from the adolescent and adult interviews, we excluded the 46 participants who reported that the age of alcohol-use disorder onset was prior to age 18 (n = 1,006); age of onset was defined as the age for which the first alcohol-use disorder symptom occurred;
school behaviors are included as continuous variables with increasing score indicative of greater frequency of suspension or skipping school; log transformation yielded comparable findings;
each logistic regression model includes a covariate for mothers’ self-report of regular alcohol use; separate logistic regression models were completed for each school-behavior outcome measure.
Table 6.
Association of developing a DSM-III-R/DSM-IV alcohol-use disorder by educational level, based on logistic regression analyses, using multiple imputation, stratified by gender; data are from the Woodlawn Study (n = 1,006)a
| Educational level | Unadjusted OR (95% CI), p |
Adjusted ORb (95% CI), p |
|---|---|---|
| Men (n = 467) | ||
| Grade or high school, no diploma | 3.44 (1.39–8.47), p < .001 | 3.37 (1.36–8.34), p = .01 |
| General Equivalency Diploma (GED) | 1.71 (0.55–5.30), p = .35 | 1.68 (0.54–5.22), p = .40 |
| Regular high-school diplomac | 2.41 (1.01–5.75), p = .05 | 2.38 (1.01–5.68), p = .05 |
| Some colleged | 2.01 (0.81–4.96), p = .13 | 2.00 (0.81–4.93), p = .20 |
| College degree or highere | 1.00 | 1.00 |
| Women (n = 539) | ||
| Grade or high school, no diploma | 2.43 (0.82–7.25), p = .11 | 2.37 (0.79–7.10), p = .19 |
| General Equivalency Diploma (GED) | 3.86 (1.08–13.83), p = .04 | 3.85 (1.07–13.85), p = .04 |
| Regular high-school diplomac | 2.02 (0.73–5.64), p = .18 | 2.03 (0.73–5.67), p = .24 |
| Some colleged | 2.10 (0.77–5.74), p = .15 | 2.14 (0.78–5.86), p = .20 |
| College degree or highere | 1.00 | 1.00 |
Notes: DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; DSM-IV = DSM, Fourth Edition; OR= odds ratio; CI = confidence interval.
The analyses are based on an overall sample size of 1,052, using multiple imputations to account for missing information among the nonincapacitated survivors who completed the young adult and/or midlife interviews and provided information to assess the presence of a lifetime alcohol-use disorder; in the analyses of educational information gathered from the adolescent and adult interviews, we excluded the 46 participants who reported that the age of alcohol-use disorder onset was prior to age 18 (n = 1,006); age of onset was defined as the age for which the first alcohol-use disorder symptom occurred;
the adjusted logistic regression model includes a covariate for mothers’ self-report of regular alcohol use; all educational level categories are included in both the unadjusted and adjusted models referenced to those with a college degree or higher;
this category also includes individuals who may have completed additional noncollege training (such as vocational training);
this category also includes individuals who may have completed a 2-year college degree, such as the associate of arts degree;
reference category.
Discussion
In this study, we found that relatively few of the hypothesized educational characteristics were associated with subsequent risk for alcohol-use disorders. However, some measures of educational underachievement and maladaptive school behaviors early in life are associated with an increased risk for alcohol-use disorders in adulthood. Early predictors of alcohol-use disorders in this population included first-grade math achievement among boys and reports of skipping school (by mothers for boys and by self-report for girls). Dropping out of school was strongly predictive for male participants but less so for female participants. These results converge with evidence from prior prospective studies of educational level and school behaviors in this and other samples (Crum et al., 1992, 1998; Riala et al., 2003). However, these findings provide evidence that a few early predictors may be associated with risk that extends through midlife, 35 years after the initial assessments. These findings also highlight potential gender differences in the predictive probability of these early measures of educational achievement and school behaviors.
Although findings from this study are generally consistent with prior analyses, there are some differences. For example, in these analyses, which are stratified by gender, male (but not female) participants with a high-school diploma have an increased risk for an alcohol-use disorder relative to those with a college degree or higher. In prior analyses with the Woodlawn and the Epidemiologic Catchment Area samples, having a high-school diploma was not associated with an increased risk of alcohol abuse or dependence (Crum et al., 1992, 1998). Furthermore, in our current analyses of female participants, those who had dropped out of school and then subsequently obtained a GED had the highest probability of developing an alcohol-use disorder. This finding also differs from previous studies. Because prior analyses were not stratified by gender, the current findings highlight potentially significant differences in the relationship between education and alcohol-use disorder that may exist for males as compared with females. It is plausible that educational achievement is more important regarding risk for alcohol-use disorders among males. Failure to meet social role expectations (e.g., underachievement, dropping out of school) may result in low self-esteem, anxiety, and mood disturbance. The social role expectations for educational achievement are likely to differ by gender. Failure to meet these expectations and the probability of using alcohol as a method to cope with these failures are also likely to be different for males than for females. Maladaptive drinking may be used as a way of coping with negative affect for males whereas females may respond to these failures with internalizing disorders such as depression, as others have suggested (Aneshensel, 1992; Horwitz et al., 1996). Further exploration of gender differences with respect to the degree of school bonding (Ensminger and Slusarcick, 1992; Ensminger et al., 1982), other concurrent deviant behaviors (e.g., Jessor and Jessor, 1977), peer drinking, and symptoms of depression or anxiety will aid in providing additional potential etiologic explanations for the current findings. One of the findings differing by sex in these analyses was the potential role of early math achievement. Prior cross-sectional analyses of black populations have shown that academic achievement is associated with lower alcohol consumption (Wright and Fitzpatrick, 2004); however, how early math achievement, especially within gender subgroups, may relate to subsequent alcohol-use disorders has not been examined. It could be a marker for later achievement; or, alternatively, there may be something specific about math skills that relates to later alcohol problems.
In prior analyses of the Woodlawn data, poor grades in school along with aggressive behavior were associated with increased risk for school dropout (Ensminger and Slusarcick, 1992), and first-grade shyness was associated with less alcohol use during adolescence (Kellam and Ensminger, 1980) and a tendency to initiate drinking at an older age (Fleming et al., 1982). These are some possible explanations for the findings in the current report. Bush and Iannotti (1992) also found that shyness was negatively associated with alcohol use among grade school children. In our current study, shyness alone was associated with a decreased risk for an alcohol-use disorder. Specifically, shy boys were less likely than boys who were neither shy nor aggressive to develop alcohol abuse or dependence in adulthood. These individuals may be less likely to engage in deviant behavior related to social inhibitory traits or be more likely to gravitate to activities involving less aggressive peers. Shyness may cause delays in initiation of alcohol use. Later age of drinking onset has been shown to be associated with reduced risk for alcohol dependence (Grant and Dawson, 1997), independent of other strong predictors such as family history (Grant, 1998). Shyness also may relate strongly to specific school behaviors, school bonding, and socialization in ways that delay or reduce the probability of maladaptive drinking patterns. Some theorize that shyness may facilitate a suppressor effect on drinking behavior based on the self-representational model and negative expectancies related to alcohol use (Bruch et al., 1992, 1997; Meade Eggleston et al., 2004). These findings also raise important questions regarding potential mediators in these relationships among black youth that will need to be explored further in future analyses. For example, questions remain as to whether shy individuals may be more receptive to religious prohibitions on drinking. In addition, spirituality and religious involvement may have important protective effects in this population. Zimmerman and Maton (1992) found that black adolescents who dropped out of high school but were involved in church activities reported less use of alcohol and other drugs. Decreases in religious activity during high school are associated with increases in drinking (Steinman and Zimmerman, 2004), but the relationship of religiosity with alcohol use among adolescents varies by race and ethnicity (Brown et al., 2001; Heath et al., 1999). In addition, religious involvement may interact with mood symptoms. For example, in recent analyses of the Woodlawn data, the relationship of religiosity and drinking behavior was moderated by negative affect: Depression was associated with problem drinking only for those with infrequent church attendance (Bowie et al., 2006).
Several limitations in the present study merit attention. First, the extensive longitudinal follow-up of the sample must be balanced with study attrition and missing information inherent in any prospective study. As a consequence, we completed multiple imputations to take into account information from participants who did not complete all four waves of the data collection. Findings from the multiple imputed analyses were comparable to those using listwise deletion. These statistical strategies improve the standard errors, but the possibility exists that biased estimates are also generated. Second, because of the screening protocol used with the CIDI, as well as the limits in power for these gender-stratified analyses, it was not possible to assess alcohol abuse separately from alcohol dependence. It is plausible that educational predictors may differ for alcohol abuse compared with the more severe symptomatology and clinical course associated with alcohol dependence. In fact, some predictors may only be associated with the more severe diagnostic category. Third, consistent with our a priori hypotheses, multiple analyses were completed to assess the associations of the various educational characteristics with risk for alcohol-use disorders. It is always possible in such instances that some associations were due to random error (chance) or to Type I error. Fourth, other potential predictors of alcohol-use disorders were not included in these analyses because the data were not available. For example, although we held constant maternal drinking history, further assessments of familial alcohol dependence, as well as other risk factors such as peer drinking, would help broaden our understanding of potential explanations for the associations included in this report. Finally, we were not able to assess the precise temporal relationship between school dropout and the development of the alcohol-use disorder for some study participants. For example, some individuals with early problem drinking may have subsequently done poorly in school as a result of the maladaptive alcohol use rather than the reverse, as we specifically hypothesized. In order to help ensure that the onset of the disorder temporally occurred after our education measures, we removed those who indicated that the onset of the first alcohol-use disorder symptom was prior to age 18 for analyses that involved educational and school behavior data gathered after the first-grade interview.
Notwithstanding these considerations, the current report supplies information that may be useful in furthering our understanding of the association of educational achievement and school behaviors with the development of alcohol-use disorders in the community. Specific assessments of potential etiologic mechanisms for these associations will be important to assess in future analyses. The potential role for other deviant behaviors, peer drinking, cognitive functioning, genetic factors, and concurrent psychopathology need to be further explored. The findings emphasize the need for continued efforts to provide this type of prospective data for alcohol and other substance use disorders, particularly in subgroups of the population in which development of alcohol abuse and dependence has been understudied, such as racial and ethnic subgroups. Community-based prospectively gathered epidemiological data provide one of the best sources for understanding patterns of development of alcohol-use disorders, which may not be possible without selection biases in cross-sectional surveys and treatment samples. With additional assessments of longitudinal data available from community sources, our understanding of etiologic factors for alcohol abuse and dependence and potential avenues for prevention will continue to improve.
Footnotes
This work was supported by National Institute of Child Health and Human Development grant HD046103 and National Institute on Drug Abuse grant DA006630.
Contributor Information
ROSA M. CRUM, Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland; Department of Mental Health, Johns Hopkins University Bloomberg School of Public Health, and the Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, Baltimore, MD.
HEE-SOON JUON, Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland; Department of Health, Behavior and Society, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD.
KERRY M. GREEN, Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland; Department of Mental Health, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD.
JUDITH ROBERTSON, Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland Department of Health, Behavior and Society, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD.
KATE FOTHERGILL, Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland Department of Health, Behavior and Society, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD.
MARGARET ENSMINGER, Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, the Department of Health, Behavior and Society, Johns Hopkins University Bloomberg School of Public Health, and the Department of Sociology, Johns Hopkins University, Baltimore, MD.
References
- Allison PD. Missing Data, Quantitative Application in the Social Sciences, No. 07-136. Thousand Oaks, CA: Sage; 2001. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R) Washington, DC: 1987. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) Washington, DC: 1994. [Google Scholar]
- Aneshensel CS. Social stress: Theory and research. Annual Rev Sociology. 1992;18:15–38. [Google Scholar]
- Blume SB. Women and alcohol: A review. JAMA. 1986;256:1467–1470. [PubMed] [Google Scholar]
- Bowie J, Ensminger M, Robertson J. Alcohol-use problems in black young adults: Effects of religiosity, social resources, and mental health. J Stud Alcohol. 2006;67:44–53. doi: 10.15288/jsa.2006.67.44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown TL, Parks GS, Zimmerman RS, Phillips CM. The role of religion in predicting adolescent alcohol use and problem drinking. J Stud Alcohol. 2001;62:696–705. doi: 10.15288/jsa.2001.62.696. [DOI] [PubMed] [Google Scholar]
- Bruch MA, Heimberg RG, Harvey C, Mccann M, Mahone M, Slavkin SL. Shyness, alcohol expectancies, and alcohol use: Discovery of a suppressor effect. J Res Pers. 1992;26:137–149. [Google Scholar]
- Bruch MA, Rivet KM, Heimberg RG, Levin MA. Shyness, alcohol expectancies, and drinking behavior: Replication and extension of a suppressor effect. Pers Indiv Diff. 1997;22:193–200. [Google Scholar]
- Bush PJ, Iannotti RJ. Elementary school children’s use of alcohol, cigarettes and marijuana and classmates’ attribution of socialization. Drug Alcohol Depend. 1992;30:275–287. doi: 10.1016/0376-8716(92)90062-h. [DOI] [PubMed] [Google Scholar]
- Costa FM, Jessor R, Turbin MS. Transition into adolescent problem drinking: The role of psychosocial risk and protective factors. J Stud Alcohol. 1999;60:480–490. doi: 10.15288/jsa.1999.60.480. [DOI] [PubMed] [Google Scholar]
- Crum RM, Anthony JC. Educational level and risk for alcohol abuse and dependence: Differences by race-ethnicity. Ethnic Dis. 2000;10:39–52. [PubMed] [Google Scholar]
- Crum RM, Bucholz KK, Helzer JE, Anthony JC. The risk of alcohol abuse and dependence in adulthood: The association with educational level. Amer J Epidemiol. 1992;135:989–999. doi: 10.1093/oxfordjournals.aje.a116411. [DOI] [PubMed] [Google Scholar]
- Crum RM, Ensminger ME, Ro MJ, McCord J. The association of educational achievement and school dropout with risk of alcoholism: A twenty-five-year prospective study of inner city children. J Stud Alcohol. 1998;59:318–326. doi: 10.15288/jsa.1998.59.318. [DOI] [PubMed] [Google Scholar]
- Dempster AP, Laird NM, Rubin DB. Maximum likelihood from incomplete data via the EM algorithm (with discussion) J Royal Stat Soc. 1977;39:1–38. Series B. [Google Scholar]
- Diggle P, Kenward MG. Informative dropout in longitudinal data analysis. Appl Stat. 1994;43:49–94. [Google Scholar]
- Donovan JE, Jessor R, Jessor L. Problem drinking in adolescence and young adulthood: A follow-up study. J Stud Alcohol. 1983;44:109–137. doi: 10.15288/jsa.1983.44.109. [DOI] [PubMed] [Google Scholar]
- Eaton WW, Kramer M, Anthony JC, Dryman A, Shapiro S, Locke BZ. The incidence of specific DIS/DSM-III mental disorders: Data from the NIMH Epidemiologic Catchment Area Program. Acta Psychiat Scand. 1989;79:163–178. doi: 10.1111/j.1600-0447.1989.tb08584.x. [DOI] [PubMed] [Google Scholar]
- Ensminger ME, Brown CH, Kellam SG. Sex differences in antecedents of substance use among adolescents. J Social Issues. 1982;38(2):25–42. [Google Scholar]
- Ensminger ME, Slusarcick AL. Paths to high school graduation or dropout: A longitudinal study of a first-grade cohort. Sociol Educ. 1992;65:95–113. [Google Scholar]
- Fleming JP, Kellam SG, Brown CH. Early predictors of age at first use of alcohol, marijuana, and cigarettes. Drug Alcohol Depend. 1982;9:285–303. doi: 10.1016/0376-8716(82)90068-0. [DOI] [PubMed] [Google Scholar]
- Grant BF. DSM-III-R and proposed DSM-IV alcohol abuse and dependence, United States 1988: A nosological comparison. Alcsm Clin Exp Res. 1992;16:1068–1077. doi: 10.1111/j.1530-0277.1992.tb00701.x. [DOI] [PubMed] [Google Scholar]
- Grant BF. Comparison of DSM-III-R and draft DSM-IV alcohol abuse and dependence in a general population sample. Addiction. 1993;88:1709–1716. doi: 10.1111/j.1360-0443.1993.tb02047.x. [DOI] [PubMed] [Google Scholar]
- Grant BF. DSM-IV, DSM-III-R, and ICD-10 alcohol and drug abuse/ harmful use and dependence, United States, 1992: A nosological comparison. Alcsm Clin Exp Res. 1996;20:1481–1488. doi: 10.1111/j.1530-0277.1996.tb01152.x. [DOI] [PubMed] [Google Scholar]
- Grant BF. The impact of a family history of alcoholism on the relationship between age at onset of alcohol use and DSM-IV alcohol dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. Alcohol Hlth Res World. 1998;22:144–147. [PMC free article] [PubMed] [Google Scholar]
- Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. J Subst Abuse. 1997;9:103–110. doi: 10.1016/s0899-3289(97)90009-2. [DOI] [PubMed] [Google Scholar]
- Grant BF, Dawson DA, Stinson FS, Chou SP, Dufour MC, Pickering RP. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991-1992 and 2001-2002. Drug Alcohol Depend. 2004;74:223–234. doi: 10.1016/j.drugalcdep.2004.02.004. [DOI] [PubMed] [Google Scholar]
- Guo J, Hawkins JD, Hill KG, Abbot RD. Childhood and adolescent predictors of alcohol abuse and dependence in young adulthood. J Stud Alcohol. 2001;62:754–762. doi: 10.15288/jsa.2001.62.754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasin D, Li Q, McCloud S, Endicott J. Agreement between DSM-III, DSM-III-R, DSM-IV and ICD-10 alcohol diagnoses in US community-sample heavy drinkers. Addiction. 1996a;91:1517–1527. doi: 10.1046/j.1360-0443.1996.9110151710.x. [DOI] [PubMed] [Google Scholar]
- Hasin D, McCloud S, Li Q, Endicott J. Cross-system agreement among demographic subgroups: DSM-III, DSM-III-R, DSM-IV and ICD-10 diagnoses of alcohol use disorders. Drug Alcohol Depend. 1996b;41:127–135. doi: 10.1016/0376-8716(96)01232-x. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Graham JW, Maguin E, Abbott R, Hill KG, Catalano RF. Preventing adolescent health-risk behaviors by strengthening protection during childhood. Arch Pediat Adolesc Med. 1999;153:226–234. doi: 10.1001/archpedi.153.3.226. [DOI] [PubMed] [Google Scholar]
- Heath AC, Madden PA, Grant JD, McLaughlin TL, Todorov AA, Bucholz KK. Resiliency factors protecting against teenage alcohol use and smoking: Influences of religion, religious involvement and values, and ethnicity in the Missouri Adolescent Female Twin Study. Twin Res. 1999;2:145–155. doi: 10.1375/136905299320566013. [DOI] [PubMed] [Google Scholar]
- Helzer JE, Burnam A, McEvoy LT. Alcohol abuse and dependence. In: Robins LN, Regier DA, editors. Psychiatric Disorders in America: The Epidemiologic Catchment Area Study. New York: Free Press; 1991. pp. 81–115. [Google Scholar]
- Horwitz AV, White HR, Howell-White S. The use of multiple outcomes in stress research: A case study of gender differences in responses to marital dissolution. J Hlth Social Behav. 1996;37:278–291. [PubMed] [Google Scholar]
- Jessor R, Jessor SL. Problem Behavior and Psychosocial Development: A Longitudinal Study of Youth. San Diego: Academic Press; 1977. [Google Scholar]
- Jones MC. Personality correlates and antecedents of drinking patterns in adult males. J Cons Clin Psychol. 1968;32:2–12. doi: 10.1037/h0025447. [DOI] [PubMed] [Google Scholar]
- Jones MC. Personality antecedents and correlates of drinking patterns in women. J Cons Clin Psychol. 1971;36:61–69. doi: 10.1037/h0030474. [DOI] [PubMed] [Google Scholar]
- Kellam SG, Ensminger ME. Theory and method in child psychiatric epidemiology. In: Earls F, editor. Studies of Children. New Brunswick, NJ: Rutgers University Press; 1980. pp. 145–180. [Google Scholar]
- Kessler RC, Crum RM, Warner LA, Nelson CB, Schulenberg J, Anthony JC. Lifetime co-occurrence of DSM-III-R alcohol abuse and dependence with other psychiatric disorders in the National Comorbidity Survey. Arch Gen Psychiat. 1997;54:313–321. doi: 10.1001/archpsyc.1997.01830160031005. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Mcgonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Arch Gen Psychiat. 1994;51:8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- Kominski R. Estimating the national high school dropout rate. Demography. 1990;27:303–311. [PubMed] [Google Scholar]
- Lex BW. Some gender differences in alcohol and polysubstance users. Hlth Psychol. 1991;10:121–132. doi: 10.1037//0278-6133.10.2.121. [DOI] [PubMed] [Google Scholar]
- Little RJA. Pattern-mixture models for multivariate incomplete data. J Amer Stat Assoc. 1993;88:125–134. [Google Scholar]
- Little RJA. A class of pattern-mixture models for normal missing data. Biometrika. 1994;81:471–483. [Google Scholar]
- Little RJA. Modeling the drop-out mechanism in repeated-measure studies. J Amer Stat Assoc. 1995;90:1112–1121. [Google Scholar]
- Little RJA, Rubin DB. Statistical Analysis with Missing Data. New York: John Wiley & Sons; 1987. [Google Scholar]
- Loper RG, Kammeier ML, Hoffmann H. MMPI characteristics of college freshman males who later became alcoholics. J Abnorm Psychol. 1973;82:159–162. doi: 10.1037/h0034959. [DOI] [PubMed] [Google Scholar]
- Mcbride CM, Curry SJ, Cheadle A, Anderman C, Wagner EH, Diehr P, Psaty B. School-level application of a social bonding model to adolescent risk-taking behavior. J School Hlth. 1995;65:63–68. doi: 10.1111/j.1746-1561.1995.tb03347.x. [DOI] [PubMed] [Google Scholar]
- McCord W, McCord J. A longitudinal study of the personality of alcoholics. In: Pittman DJ, Snyder CR, editors. Society, Culture, and Drinking Patterns. New York: John Wiley & Sons; 1962. pp. 413–430. [Google Scholar]
- Meade Eggleston A, Woolaway-Bickel K, Schmidt NB. Social anxiety and alcohol use: Evaluation of the moderating and mediating effects of alcohol expectancies. J Anxiety Disord. 2004;18:33–49. doi: 10.1016/j.janxdis.2003.07.005. [DOI] [PubMed] [Google Scholar]
- Pollock NK, Martin CS, Langenbucher JW. Diagnostic concordance of DSM-III, DSM-III-R, DSM-IV and ICD-10 alcohol diagnoses in adolescents. J Stud Alcohol. 2000;61:439–446. doi: 10.15288/jsa.2000.61.439. [DOI] [PubMed] [Google Scholar]
- Prinstein MJ, Boergers J, Spirito A. Adolescents’ and their friends’ health-risk behavior: Factors that alter or add to peer influence. J Pediat Psychol. 2001;26:287–298. doi: 10.1093/jpepsy/26.5.287. [DOI] [PubMed] [Google Scholar]
- Ratti MT, Bo P, Giardini A, Soragna D. Chronic alcoholism and the frontal lobe: Which executive functions are imparied? Acta Neurol Scand. 2002;105:276–281. doi: 10.1034/j.1600-0404.2002.0o315.x. [DOI] [PubMed] [Google Scholar]
- Ratti MT, Soragna D, Sibilla L, Giardini A, Albergati A, Savoldi F, Bo P. Cognitive impairment and cerebral atrophy in “heavy drinkers”. Prog Neuropsychopharmacol Biol Psychiat. 1999;23:243–258. doi: 10.1016/s0278-5846(98)00103-1. [DOI] [PubMed] [Google Scholar]
- Riala K, Isohanni I, Jokelainen J, Taanila A, Isohanni M, Rasanen P. Low educational performance is associated with drunk driving: A 31-year follow-up of the northern Finland 1966 birth cohort. Alcohol Alcsm. 2003;38:219–223. doi: 10.1093/alcalc/agg079. [DOI] [PubMed] [Google Scholar]
- Robins LN, Bates WM, O’neal P. Adult drinking patterns of former problem children. In: Pittman DJ, Snyder CR, editors. Society, Culture, and Drinking Patterns. New York: John Wiley & Sons; 1962. pp. 395–412. [Google Scholar]
- Robins LN, Wing J, Wittchen HU, Helzer JE, Babor TF, Barke J, Farmer A, Jablenski R, Regier DA, Et AL. The Composite International Diagnostic Interview: An epidemiologic instrument suit able for use in conjunction with different diagnostic systems and in different cultures. Arch Gen Psychiat. 1988;45:1069–1077. doi: 10.1001/archpsyc.1988.01800360017003. [DOI] [PubMed] [Google Scholar]
- Schafer JL. Analysis of Incomplete Multivariate Data. New York: Chapman & Hall; 1997. [Google Scholar]
- Schmidt C, Klee L, Ames G. Review and analysis of literature on indicators of women’s drinking problems. Brit J Addict. 1990;85:179–192. doi: 10.1111/j.1360-0443.1990.tb03069.x. [DOI] [PubMed] [Google Scholar]
- Schulenberg J, Bachman JG, O’malley PM, Johnston LD. High school educational success and subsequent substance use: A panel analysis following adolescents into young adulthood. J Hlth Social Behav. 1994;35:45–62. [PubMed] [Google Scholar]
- Spoth R, Redmond C, Hockaday C, Yoo S. Protective factors and young adolescent tendency to abstain from alcohol use: A model using two waves of intervention study data. Amer J Commun Psychol. 1996;24:749–770. doi: 10.1007/BF02511033. [DOI] [PubMed] [Google Scholar]
- Steinman KJ, Zimmerman MA. Religious activity and risk behavior among African American adolescents: Concurrent and developmental effects. Amer J Commun Psychol. 2004;33:151–161. doi: 10.1023/b:ajcp.0000027002.93526.bb. [DOI] [PubMed] [Google Scholar]
- Wilsnack SC, Wilsnack RW. Epidemiology research in women’s drinking: Recent progress and directions for the 1990s. In: Lisansky Gomberg ES, Nirenberg TD, editors. Women and Substance Abuse, Norwood. NJ: Ablex; 1993. pp. 62–99. [Google Scholar]
- Wright DR, Fitzpatrick KM. Psychosocial correlates of substance use behaviors among African American youth. Adolescence. 2004;39:653–667. [PubMed] [Google Scholar]
- Yuan Y. Proceedings of the Twenty-Fifth Annual SAS Users Group International Conference. Cary, NC: SAS Institute; 2000. Multiple imputation for missing data: Concepts and new development. (Paper No. 267). [Google Scholar]
- Zeigler DW, Wang CC, Yoast RA, Dickinson BD, Mccaffree MA, Robinowitz CB, Sterling ML. The neurocognitive effects of alcohol on adolescents and college students. Prev Med. 2005;40:23–32. doi: 10.1016/j.ypmed.2004.04.044. [DOI] [PubMed] [Google Scholar]
- Zimmerman MA, Maton KI. Life-style and substance use among male African-American urban adolescents: A cluster analytic approach. Amer J Commun Psychol. 1992;20:121–138. doi: 10.1007/BF00942184. [DOI] [PubMed] [Google Scholar]