

ABSTRACT
Cefiderocol, a novel parenteral siderophore cephalosporin, exhibits potent efficacy against most Gram-negative bacteria, including carbapenem-resistant strains. The aim of this study was to perform a population pharmacokinetic (PK) analysis based on plasma cefiderocol concentrations in healthy subjects, subjects with various degrees of renal function, and patients with complicated urinary tract infection (cUTI) or acute uncomplicated pyelonephritis (AUP) caused by Gram-negative pathogens and to calculate the fraction of the time during the dosing interval where the free drug concentration in plasma exceeds the MIC (fTMIC). Population PK models were developed with three renal function markers, body surface area-adjusted estimated glomerular filtration rate (eGFR), absolute eGFR, and creatinine clearance, on the basis of 2,571 plasma concentrations from 91 subjects without infection and 238 patients with infection. The population PK models with each renal function marker adequately described the plasma cefiderocol concentrations. Clear relationships of total clearance (CL) to all renal function markers were observed. Body weight and disease status (with or without infection) were also significant covariates. The CL in patients with infection was 26% higher than that in subjects without infection. The fTMIC values were more than 75% in all patients (and were 100% in most patients), suggesting that a sufficient exposure to cefiderocol was provided by the tested dose regimens (2 g every 8 h as the standard dose regimen) for the treatment of cUTI or AUP caused by Gram-negative pathogens.
KEYWORDS: acute uncomplicated pyelonephritis, augmented renal function, cefiderocol, cephalosporin, complicated urinary tract infection, pharmacokinetics, population pharmacokinetics, renal function, siderophore
INTRODUCTION
Cefiderocol (product code S-649266) is a new injectable cephalosporin with a catechol group on the side chain at the C-3 position of the cephalosporin core that was initially identified by Shionogi & Co., Ltd., Osaka, Japan, and that exerts its antibacterial activity by inhibiting the synthesis of bacterial cell walls. Cefiderocol exhibits potent efficacy in vitro and in vivo against most Gram-negative bacteria, including carbapenem-resistant strains of Enterobacteriaceae, Pseudomonas aeruginosa, and Acinetobacter baumannii (1–4). Cefiderocol is being developed for the treatment of carbapenem-resistant Gram-negative bacterial infections, including nosocomial pneumonia, bloodstream infections, and complicated urinary tract infection (cUTI).
For cefiderocol, which exhibits bactericidal activity dependent on the duration of action, the pharmacokinetic (PK)/pharmacodynamic (PD) index most closely correlated with efficacy is the fraction of the time during the dosing interval where the free drug concentration in plasma exceeds the MIC (fTMIC) (5–7), as has been described with other cephalosporins (8, 9). In vivo animal infection models demonstrated a bacteriostatic effect at an fTMIC of 40% to 70% and a bactericidal effect (≥1-log reduction) at an fTMIC of 55% to 80% against carbapenem-resistant strains of Enterobacteriaceae, P. aeruginosa, and A. baumannii (5–7). Cefiderocol PK are linear over the range of 100 to 2,000 mg (10). Cefiderocol is mainly excreted unchanged via the kidneys (as 60% to 70% of the dose in subjects with normal renal function), and thus, the clearance of cefiderocol is dependent on renal function (11). The in vitro plasma protein binding of cefiderocol was 57.8%. The population PK model was previously developed on the basis of the concentration data of cefiderocol in healthy subjects and subjects with various degrees of renal function (12). The developed model well described the plasma concentration data.
The aim of this study was to perform a population PK analysis based on the plasma cefiderocol concentrations in healthy subjects, subjects with various degrees of renal function, and patients with cUTI or acute uncomplicated pyelonephritis (AUP) caused by Gram-negative pathogens in a phase 2 study of cefiderocol for the treatment of cUTI (13) and to calculate the fTMIC. A summary of the study designs is shown in Table S1 in the supplemental material. The population PK models were developed using three renal function markers: (i) the estimated glomerular filtration rate (eGFR), which was calculated by the modification of diet in renal disease (MDRD) equation (14) or an equation reported by Matsuo et al. for Japanese subjects (15) (the body surface area-adjusted eGFR [eGFRadj]); (ii) the eGFR converted by multiplying by the individual's body surface area and dividing by 1.73 m2 (absolute eGFR [eGFRabs]); and (iii) creatinine clearance (CLCR), which was calculated by the Cockcroft-Gault equation (16). These three renal function markers were assessed separately in the population PK analysis because they have been used as renal function markers (14, 17–19) and the selection of renal function markers might affect the prediction of cefiderocol PK. fTMIC was calculated on the basis of simulated steady-state plasma cefiderocol concentrations and the MICs of Gram-negative uropathogens detected in the cUTI study.
RESULTS
A total of 2,571 plasma cefiderocol concentrations obtained from 329 subjects were used for developing the population PK models. Data for samples stored under unstable conditions, samples with anomalous concentrations, or samples with concentrations below the limit of quantification (BLQ) (n = 264 concentrations) (see Materials and Methods) were excluded from the analysis.
The subject characteristics are shown in Table 1. The parameter estimates are provided in Table 2.
TABLE 1.
Subject characteristicsa
| Characteristic | Value |
||
|---|---|---|---|
| Subjects without infectionb (n = 91) | Patients with cUTI or AUP (n = 238) | Overall | |
| Body wt (kg) | |||
| Mean (SD) | 73.4 (17.3) | 77.8 (16.1) | 76.6 (16.5) |
| Median (range) | 68.4 (45.1–124.1) | 76.4 (46.3–138.0) | 74.1 (45.1–138.0) |
| Age (yr) | |||
| Mean (SD) | 40.6 (15.7) | 60.5 (16.3) | 55.0 (18.4) |
| Median (range) | 36.0 (20–74) | 65.0 (18–93) | 59.0 (18–93) |
| eGFRadj (ml/min/1.73 m2) | |||
| Mean (SD) | 86.3 (38.9) | 70.8 (24.5) | 75.1 (29.9) |
| Median (range) | 99.0 (4–146) | 72.0 (14–142) | 77.0 (4–146) |
| eGFRabs (ml/min) | |||
| Mean (SD) | 89.8 (38.6) | 77.2 (27.2) | 80.6 (31.2) |
| Median (range) | 99.0 (5–144) | 78.0 (16–148) | 83.0 (5–148) |
| CLCR (ml/min) | |||
| Mean (SD) | 108.3 (48.2) | 83.0 (31.9) | 90.0 (38.7) |
| Median (range) | 121.0 (7–185) | 83.0 (25–186) | 90.0 (7–186) |
| CLCR (ml/min) for patients with cUTI (n = 175) | |||
| Mean (SD) | 81.3 (32.8) | ||
| Median (range) | 80.0 (25–186) | ||
| CLCR (ml/min) for patients with AUP (n = 63) | |||
| Mean (SD) | 87.6 (29.0) | ||
| Median (range) | 93.0 (32–159) | ||
| Albumin concn (g/dl) | |||
| Mean (SD) | 4.2 (0.3) | 4.1 (0.5) | 4.1 (0.5) |
| Median (range) | 4.2 (3.1–4.8) | 4.2 (2.5–5.3) | 4.2 (2.5–5.3) |
| Aspartate aminotransferase concn (U/liter) | |||
| Mean (SD) | 20.7 (8.1) | 19.7 (11.5) | 20.0 (10.7) |
| Median (range) | 18.0 (10–45) | 18.0 (6–101) | 18.0 (6–101) |
| Alanine aminotransferase concn (U/liter) | |||
| Mean (SD) | 20.6 (10.4) | 20.1 (16.6) | 20.2 (15.1) |
| Median (range) | 18.0 (5–51) | 15.0 (4–111) | 16.0 (4–111) |
| Total bilirubin concn (mg/dl) | |||
| Mean (SD) | 0.78 (0.38) | 0.60 (0.30) | 0.65 (0.34) |
| Median (range) | 0.78 (0.20–2.00) | 0.53 (0.19–2.88) | 0.57 (0.19–2.88) |
| No. (%) of subjects by sex | |||
| Male | 75 (82.4) | 108 (45.4) | 183 (55.6) |
| Female | 16 (17.6) | 130 (54.6) | 146 (44.4) |
| No. (%) of subjects by race | |||
| White | 23 (25.3) | 230 (96.6) | 253 (76.9) |
| Nonwhite | 68 (74.7) | 8 (3.4) | 76 (23.1) |
| Asian | 49 (53.9) | 7 (2.9) | 56 (17.0) |
| Black or African American | 17 (18.7) | 0 (0.0) | 17 (5.2) |
| Native American or Alaska Native | 1 (1.1) | 0 (0.0) | 1 (0.3) |
| Other | 1 (1.1) | 1 (0.4) | 2 (0.6) |
CLCR, creatinine clearance calculated by the Cockcroft-Gault equation; eGFRadj, body surface area-adjusted estimated glomerular filtration rate; eGFRabs, absolute estimated glomerular filtration rate; cUTI, complicated urinary tract infection; AUP, acute uncomplicated pyelonephritis.
Subjects without infection included healthy subjects and subjects with various degrees of renal function.
TABLE 2.
Population PK parameter estimates for base model and final modelse
| Parameter | Units | Base model |
Final model with eGFRadja |
Final model with eGFRabsb |
Final model with CLCRc |
||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | % RSE | Estimate | % RSE | Estimate | % RSE | Estimate | % RSE | ||
| OBJ | 9,697.817 | 9,386.181 | 9,377.486 | 9,363.552 | |||||
| PK parameters | |||||||||
| CL | liters/h | 4.60 | 2.8 | 5.02 | 2.8 | 4.56 | 1.8 | 4.23 | 1.5 |
| V1 | liters | 9.91 | 3.6 | 7.93 | 6.5 | 7.92 | 3.2 | 7.93 | 3.1 |
| Q2 | liters/h | 5.81 | 7.2 | 5.81 | 22.0 | 5.78 | 5.6 | 5.75 | 5.3 |
| V2 | liters | 5.37 | 3.8 | 5.41 | 4.4 | 5.41 | 3.4 | 5.41 | 3.3 |
| Q3 | liters/h | 0.106 | 19.2 | 0.109 | 98.2 | 0.109 | 17.2 | 0.109 | 14.4 |
| V3 | liters | 0.729 | 9.3 | 0.736 | 48.4 | 0.735 | 8.6 | 0.734 | 7.3 |
| Effect of renal function markerd on CL | 0.631 | 12.4 | 0.621 | 3.5 | 0.653 | 3.9 | |||
| Effect of body wt on CL | 0.531 | 18.6 | |||||||
| Effect of body wt on V1 | 0.800 | 72.8 | 0.789 | 12.8 | 0.798 | 12.2 | |||
| Effect of body wt on V2 | 0.689 | 26.4 | 0.673 | 10.8 | 0.698 | 17.3 | |||
| Effect of disease status on CL | 1.15 | 3.2 | 1.26 | 3.1 | |||||
| Effect of disease status on V1 | 1.35 | 5.1 | 1.36 | 5.1 | 1.36 | 4.9 | |||
| % CV for IIV for CL (sh_ηp) | 48.8 (1.4) | 11.4 | 33.0 (2.9) | 14.3 | 32.6 (2.9) | 14.4 | 31.8 (3.1) | 15.8 | |
| % CV for IIV for V1 (sh_ηp) | 56.1 (8.8) | 21.7 | 46.3 (11.1) | 28.8 | 46.3 (11.0) | 27.7 | 45.8 (11.1) | 28.2 | |
| % CV for IIV for V2 (sh_ηp) | 42.8 (32.2) | 29.9 | 37.9 (34.2) | 35.8 | 38.3 (34.2) | 35.6 | 38.2 (34.2) | 35.5 | |
| % CV for proportional residual error (sh_ε) | 14.8 (14.9) | 12.1 | 15.1 (14.2) | 12.7 | 15.1 (14.2) | 12.6 | 15.1 (14.1) | 12.8 | |
CL = 5.02 · (eGFRadj/77.0)0.631 · (body weight/74.1)0.531; V1 = 7.93 · (body weight/74.1)0.800 · 1.35disease status (disease status = 0 for subjects without infection and disease status = 1 for patients with infection; disease status is treated in the same way for the disease status superscripts in footnotes b and c); V2 = 5.41 · (body weight/74.1)0.689.
CL = 4.56 · (eGFRabs/83.0)0.621 · 1.15disease status; V1 = 7.92 · (body weight/74.1)0.789 · 1.36disease status; V2 = 5.41 · (body weight/74.1)0.673.
CL = 4.23 · (CLCR/90.0)0.653 · 1.26disease status; V1 = 7.93 · (body weight/74.1)0.798 · 1.36disease status; V2 = 5.41 · (body weight/74.1)0.698.
eGFRadj, eGFRabs, or CLCR for each model.
CI, confidence interval; CLCR, creatinine clearance calculated by the Cockcroft-Gault equation; eGFRabs, absolute estimated glomerular filtration rate; eGFRadj, body surface area-adjusted estimated glomerular filtration rate; IIV, interindividual variability; sh_ηp, shrinkage in the standard deviation of interindividual variability parameters η; sh_ε, shrinkage in the standard deviation of intraindividual variability parameters ε; RSE, relative standard error.
A 3-compartment model was used as a structural PK model since the population mean parameters were estimated appropriately and were similar to those estimated in the previous population PK analyses (12). The proportional error model was selected, since the relative standard error (RSE; in percent) of the PK parameter estimates obtained using the combination error model were large (4.1% to 1,721%), which suggested that the model was not robust.
The correlations of the renal function markers are presented in Fig. S1. The correlations for eGFRadj and eGFRabs were comparable, while they were slightly lower than the correlation for CLCR. Clear relationships of CL to eGFRadj, eGFRabs, and CLCR were observed using the base model and are shown in Fig. 1 for CLCR and Fig. S2 for eGFRadj and eGFRabs. Each renal function marker was a significant covariate for CL, and each was incorporated using the power model, which provided an objective function value (OBJ) similar to or less than that from the piecewise linear model and which had a smaller number of estimable parameters than the other model. The effects of body weight on CL and the volume of distribution in the central and peripheral compartments (V1 and V2, respectively) and the effect of disease status on V1 were significant in the final model with eGFRadj. The effects of body weight on V1 and V2 and the effect of disease status on CL and V1 were significant in the final models with eGFRabs and CLCR. The final model with CLCR demonstrated that CL and V1 in patients with infection were 26% and 36% higher, respectively, than those in subjects without infection. The incorporation of significant covariates in each final model reduced the interindividual variability (IIV) for CL, V1, and V2 from that in the base model. In comparison with the IIV in the base model, in the final model with CLCR, IIV was reduced from 48.8% to 31.8% for CL, 56.1% to 45.8% for V1, and 42.8% to 38.2% for V2.
FIG 1.
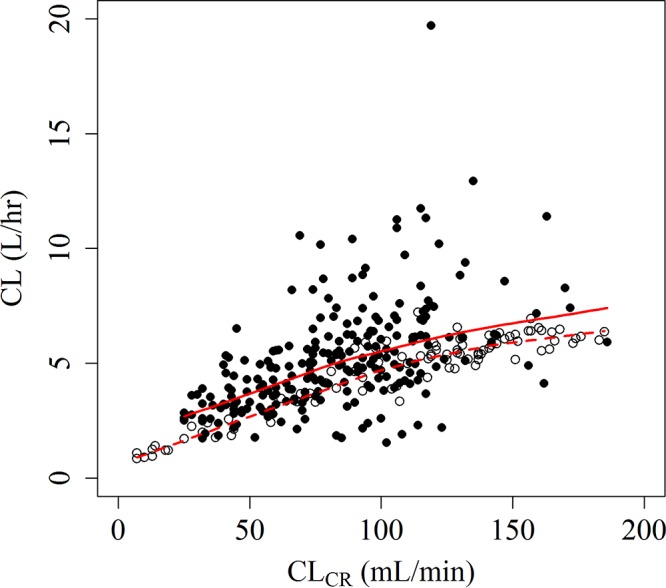
Relationship between CL and CLCR. Filled circles, patients with infection; open circles, subjects without infection; solid line, LOWESS (locally weighted scatterplot smoothing) line for patients with infection; dashed line, LOWESS line for subjects without infection.
The number of estimable parameters was the same among the final models developed with eGFRadj, eGFRabs, and CLCR; and the typical parameter values, the IIV for each parameter, and the intraindividual variability were comparable among the final models (Table 2). Of the three final models, the OBJ of the model with CLCR was the lowest, and thus, the calculation of post hoc PK parameters and fTMIC was performed by using the final model with CLCR. The goodness-of-fit (GOF) plot for the final model with CLCR is presented in Fig. S3. As shown in Fig. 2, the visual predictive check (VPC) indicated that the median predicted concentration profiles by disease status and renal function group well captured the observed data with a lack of bias. The prediction intervals in subjects without infection were relatively wide compared to the distribution of the observed data.
FIG 2.

Visual predictive check for the final model with CLCR by disease status and renal function group. The results for 200 simulations are shown, and data are presented on a semilogarithmic scale. Renal function groups defined by CLCR were as follows: augmented renal function, CLCR ≥ 120 ml/min; normal renal function or mild renal impairment, CLCR = 60 to <120 ml/min; moderate or severe renal impairment or end-stage renal disease (ESRD), CLCR = 5 to <60 ml/min. Noninfected, subjects without infection; Infected, patients with infection; Time, time after the previous dose; solid lines, observed median; dashed lines, observed 2.5th and 97.5th percentiles; dark gray shaded areas, model-predicted 95% confidence interval of the median; light gray shaded areas, model-predicted 95% confidence intervals of the 2.5th and 97.5th percentiles.
Figure 3 shows box plots for individual post hoc CL values with empirical Bayesian estimation by renal function group (augmented and normal renal function; mild, moderate, and severe renal impairment; and end-stage renal disease [ESRD]). The CL of cefiderocol decreased with decreasing renal function. Figure 4 shows box plots for individual post hoc V1 values for patients with infection by body weight group (<55, 55 to <70, 70 to <90, or 90 to 138 kg). V1 was slightly dependent on body weight, which is consistent with the fact that body weight was a significant covariate on V1 in the population PK analysis. The maximum concentration (Cmax) and daily area under the concentration-time curve (AUC) for patients with infection, calculated using individual post hoc PK parameters, are summarized by dose regimen in Table 3. The daily AUC was similar among the dose groups.
FIG 3.

Box plots for individual post hoc CL values by renal function group defined by CLCR. (a) All subjects; (b) subjects without infection; (c) patients with infection. The final model with CLCR was used to estimate individual parameters. Renal function groups defined by CLCR were as follows: augmented renal function: CLCR ≥ 120 ml/min; normal renal function, CLCR = 90 to <120 ml/min; mild renal impairment, CLCR = 60 to <90 ml/min; moderate renal impairment, CLCR = 30 to <60 ml/min; severe renal impairment, CLCR = 15 to <30 ml/min; end-stage renal disease (ESRD), CLCR = 5 to <15 ml/min. Thick center lines, medians; top and bottom lines of the boxes, first and third quartiles (interquartile range), respectively; whiskers, the most extreme data within 1.5× the interquartile range; circles, outliers beyond 1.5× the interquartile range.
FIG 4.
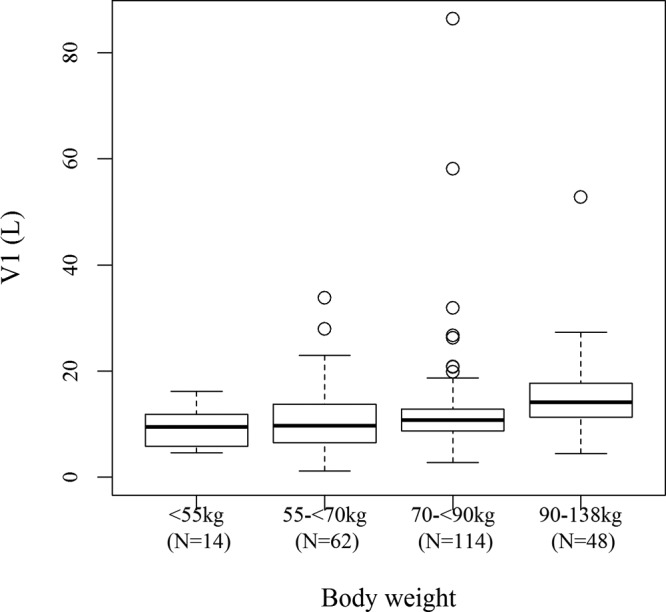
Box plot for individual post hoc V1 for patients with infection by body weight group defined by CLCR. The final model with CLCR was used to estimate individual parameters. Thick center lines, medians; top and bottom lines of the boxes, first and third quartiles (interquartile range), respectively; whiskers, the most extreme data within 1.5× the interquartile range; circles, outliers beyond 1.5× the interquartile range.
TABLE 3.
Summary of individual post hoc PK parameters for Cmax and daily AUC for patients with infectiona
| Dose regimen | No. of patients | Cmax (μg/ml) | Daily AUC (μg · h/ml) |
|---|---|---|---|
| 2 g q8h | 139 | 138 (29.5–460) | 1,184 (270.0–3,562) |
| 1.5 g q8h | 26 | 134 (79.0–292) | 1,186 (588.2–2,505) |
| 1 g q8h | 22 | 87.5 (57.0–161) | 1,108 (588.4–1,719) |
| 1.5 g q6h | 8 | 102 (73.8–138) | 862.0 (525.2–1,227) |
| 1 g q6h | 40 | 79.9 (30.7–122) | 1,026 (316.4–1,686) |
| 0.75 g q6h | 3 | 69.3 (67.3–72.6) | 1,003 (872.9–1,181) |
The values represent the mean (range). The final model with CLCR was used to calculate the individual parameters for patients with infection. The dose regimen was tested in the phase 2 study of cefiderocol for the treatment of cUTI or AUP. q8h, every 8 h; q6h, every 6 h.
A summary of the MIC distribution for each pathogen is shown in Table S3. The calculated fTMIC values based on the simulated steady-state plasma cefiderocol concentrations and the MIC of Gram-negative uropathogens detected in the cUTI study were more than 75% in all patients (and were 100% in most patients).
DISCUSSION
We separately developed three population PK models based on plasma cefiderocol concentration data for subjects with or without infection by using different renal function markers (eGFRadj, eGFRabs, and CLCR). All models developed with the different renal function markers adequately described the plasma cefiderocol concentration data. These results suggest that any renal function marker could be used to adjust the cefiderocol dose.
eGFRadj and eGFRabs were similar, while they were slightly lower than that of CLCR (see Fig. S1 in the supplemental material), which is consistent with well-known findings (14, 17). The MDRD equation is recognized as providing estimates of the GFR more accurate than those provided by the Cockcroft-Gault equation (18). On the other hand, there have been reports that the CLCR estimated by the Cockcroft-Gault equation is closer to the measured creatinine clearance than the estimated GFR calculated with other equations, including the MDRD equation, for estimation of an augmented renal function (measured CLCR > 130 ml/min) in critically ill patients (19). CLCR was the best predictor of cefiderocol PK on the basis of the OBJ by the use of NONMEM software. However, the difference in the predictive performance among the models with each renal function marker would not be clinically significant. Therefore, it was suggested that any of these renal function markers can be used for dose adjustment and simulations based on renal function markers.
Body weight was a statistically significant covariate on CL, V1, and V2 in the final model with eGFRadj and V1 and V2 in the final models with eGFRabs and CLCR. Body weight was selected as a covariate on CL for the model with eGFRadj but not the models with eGFRabs and CLCR. This is probably because eGFRabs and CLCR could accommodate the effect of body scale for describing the cefiderocol PK but eGFRadj could not. The post hoc analyses suggested that V1 was slightly dependent on body weight. However, the individual V1 values overlapped among the body weight groups, as shown in Fig. 4, and ratios of the median values of V1 relative to the typical value of V1 for infected patients (11.1 liters) were close to 1, with the values of the ratios being 0.85 for individuals weighing <55 kg, 0.87 for individuals weighing 55 to <70 kg, 0.96 for individuals weighing 70 to <90 kg, and 1.27 for individuals weighing ≥90 kg, suggesting that the effect of body weight on cefiderocol PK would not be clinically significant.
The disease status (with or without infection) was a significant covariate on V1 in the final model with eGFRadj and CL and V1 in the final models with eGFRabs and CLCR. The final model with CLCR suggested that the values of CL and V1 in patients with infection were 26% and 36% higher, respectively, than those in subjects without infection. These results were consistent with the report for ceftolozane, a parenteral cephalosporin, in patients with cUTI (in which the values of both clearance and the volume of distribution were 21% higher in subjects with infection than subjects without infection) (20). The IIV for patients with infection was higher than that for subjects without infection, as shown in Fig. 2, which is probably because the plasma concentrations from the patients were limited (3 points per patient) and the IIV could not be calculated adequately.
The fTMIC values were more than 75% in all patients (and were 100% in most patients), suggesting that the level of cefiderocol exposure obtained with the dose regimen used in the cUTI study (Table S2) would be sufficient for the treatment of cUTI and AUP caused by Gram-negative uropathogens (median MIC, 0.06 μg/ml; MIC range, 0.004 to 8 μg/ml; MIC90, 1 μg/ml). This sufficient exposure was expected from the results of Monte Carlo simulations, which indicated, using the PK model for healthy subjects, that a dose of 2 g every 8 h (q8h) with a 1-h infusion provided a high probability of attainment of a target of an fTMIC of 75% against organisms with MICs up to 4 μg/ml (12). In addition, the mean urine cefiderocol concentrations for 8 patients in the cUTI study were 2,710 μg/ml (range, 953 to 5,520 μg/ml) at 2 h after the start of infusion and 1,520 μg/ml (range, 336 to 4,220 μg/ml) at 6 h after the start of infusion. Urine cefiderocol concentrations were also high relative to the MIC values detected in the cUTI study. As the protein-unbound fraction was not obtained in the phase 2 study of cefiderocol for the treatment of cUTI, individual fTMIC values were calculated on the basis of the free concentrations in plasma using a fixed value for the unbound fraction of 0.422. The effect of the fixed unbound fraction would be minimal for the calculation of fTMIC because the plasma unbound fraction was similar between the various renal function groups (11).
As shown in Fig. 3c, the clearance of cefiderocol in the 23 cUTI or AUP patients with augmented renal function (CLCR ≥ 120 ml/min) was higher than that in the patients with normal renal function (CLCR = 90 to <120 ml/min). Creatinine clearance was not measured in this study. Although the use of a measured creatinine clearance may be more appropriate to define augmented renal function, the use of an equation-derived value, such as CLCR estimated by the Cockcroft-Gault equation, would be clinically practical. Monte Carlo simulations suggested that a more frequent dose (every 6 h) had a benefit for subjects with augmented renal function to attain a sufficient fTMIC (12). The target patient population for cefiderocol includes critically ill patients infected with multidrug-resistant strains, which would be less susceptible than the uropathogens collected from the cUTI study. Augmented renal function is often observed in critically ill patients. Therefore, shortening of the cefiderocol dosing interval would be recommended for patients with augmented renal function to obtain enough exposure against organisms for which the MIC is higher.
In summary, our models developed with eGFRadj, eGFRabs, or CLCR described well the PK of cefiderocol. Clear relationships of CL to renal function markers were observed, as expected. It was revealed that the exposure to cefiderocol in patients with infection would be modestly lower than that in subjects without infection. A cefiderocol exposure sufficient for the treatment of cUTI and AUP caused by Gram-negative uropathogens was provided by the tested dose regimens (2 g q8h as the standard dose regimen).
MATERIALS AND METHODS
Data.
Plasma cefiderocol concentration data from two phase 1 studies (10–12) and one phase 2 cUTI study (13) were used for the modeling (see Table S1 in the supplemental material). The population PK models were previously developed on the basis of plasma and urine cefiderocol concentration data for 54 healthy subjects and plasma concentration data for 37 subjects with various degrees of renal function (12).
In this study, the plasma concentration data for cUTI and AUP patients in the cUTI study (13) were included to develop the population PK models. The cUTI study was a multinational, double-blind, randomized study to assess the efficacy and safety of cefiderocol in hospitalized adults with cUTI with or without pyelonephritis or AUP caused by Gram-negative pathogens in comparison with intravenous imipenem-cilastatin (IMP-CS). The patients received 2 g as a 1-h intravenous infusion three times daily at 8-h intervals (q8h) for 7 or 14 days. The dose of cefiderocol was reduced on the basis of renal function and body weight, as shown in Table S2, consistent with the dosing instructions for IMP-CS, in order to maintain the blinding to the 2 treatments.
Blood samples for PK testing were not collected from 7 patients mainly due to patient withdrawal from the study. Blood samples for PK testing from 1 patient were not analyzed because the conditions used to store the sample did not meet the criteria required to maintain stability. Three concentrations from 1 patient were not used for analysis because the sampling times were unidentified. A total of 264 samples obtained after cefiderocol administration, which were mainly from healthy subjects, had concentrations that were BLQ and were excluded from the analyses. Plasma concentrations from 1 patient were entirely excluded from the analysis because they were all BLQ. A total of 156 blood samples from 52 patients were delayed in their delivery to the laboratory where the buffer was added to the samples for stabilization and had been stored at −20°C for more than 7 days after the samples were drawn but prior to the addition of the buffer; therefore, they were excluded from the analyses since cefiderocol is not thought to be stable in blood samples on the basis of stability data. Eight plasma concentrations obtained in the renal impairment study and the cUTI study were excluded from the analysis because they were considered anomalous, as the concentrations were much higher than the typical plasma concentrations, with the Cmax being 153 μg/ml following a 2-g dose. After exclusion of these data, a total of 2,571 plasma cefiderocol concentrations from 329 subjects were used for the development of the population PK models. MIC data for 195 pathogens from 189 patients were used for calculation of the fTMIC. Subject characteristics obtained at the baseline were used (Table 1).
Bioanalytical method.
The composite samples were prepared by treating plasma with a buffer (0.2 mol/liter ammonium acetate, pH 5) in a 1:1 ratio by volume and used for measurement of cefiderocol concentrations. The cefiderocol concentrations were determined using a validated high-performance liquid chromatography-tandem mass spectrometry (LC-MS/MS) assay. The assay was linear from 0.1 to 100 μg/ml for plasma. The precision and accuracy of the assay were 1.2% to 6.2% and −5.3% to 2.1%, respectively, for plasma. The lower limit of quantification of cefiderocol in plasma was 0.1 μg/ml.
Population pharmacokinetic analyses.
A 3-compartment model was tested for describing the plasma concentration profiles of cefiderocol since the 3-compartment model well described the plasma cefiderocol concentration data for healthy subjects and subjects with various degrees of renal function (12). The 3-compartment model included the following parameters: CL, the volume of distribution in the central and peripheral compartments (V1, V2, and V3), and intercompartmental clearance (Q2 and Q3). The IIV for the PK parameters was assumed to follow a log-normal distribution and an exponential error model, defined as Pi = TVP × exp(ηP,i), where Pi represents the value of the PK parameter for the ith individual, TVP represents the typical value of the population PK parameter, and ηP,i denotes the difference between the value of the PK parameter for the ith individual and the typical value of the PK parameter. IIV was considered for CL, V1, Q2, and V2. The proportional error model and the combination error model (an additive error model plus a proportional error model) were used to test for intraindividual (residual) variability.
After a base model was built, the influence of subject characteristics was assessed to build a covariate model. Renal function markers, body weight, age, sex, albumin (ALB) concentration, aspartate aminotransferase concentration, alanine aminotransferase concentration, bilirubin concentration, race, and disease status (subjects without infection or patients with infection) were tested as covariates on CL; and age, body weight, sex, race, ALB concentration, and disease status were tested as covariates on V1. Body weight was also tested as a covariate on V2, for which the IIV was estimable.
The effects of eGFRadj, eGFRabs, and CLCR on CL were initially tested because clear relationships of CL to renal function markers were observed (Fig. 1 and S2), and the effects of the other covariates in the models with each renal function marker were tested. On the basis of visual inspection of the data (Fig. 1), the effect of the renal function markers on CL was tested by using a piecewise linear model and a power model. The cutoff value for the piecewise linear model was determined to be 100 ml/min/1.73 m2 or 100 ml/min for each renal function marker on the basis of data from a previous report (12).
Next, the effect of body weight on CL, V1, Q2, and V2 was tested by using the power model since body weight is generally a physiological factor that influences PK.
After incorporation of renal function markers and body weight, which showed significant effects, into the base model, the effects of the other covariates were tested using a screening with univariate addition. The continuous covariates were tested by using the power model, and the categorical covariates were tested by using a multiplicative model.
Covariates with a P value of <0.01 by the χ2 test and a change in the OBJ (ΔOBJ) of <−6.64 for 1 degree of freedom were included in the base model.
The covariates found to be significant as a result of the screening were included in the base model to construct a full model. To construct the final model, stepwise backward deletion was performed to delete from the full model the insignificant covariates, that is, those with a P value of <0.001 by the χ2 test and an ΔOBJ of <10.83 for 1 degree of freedom.
All population PK models were evaluated on the basis of GOF plots. A prediction-corrected VPC (21) was performed. In the binning for time, each bin was determined to correspond to each nominal sampling time.
Calculation of post hoc PK parameters and fTMIC.
The calculation of post hoc PK parameters and fTMIC was performed by using the final model with CLCR, which had the lowest OBJ of three final models with different renal function markers. Cmax and the daily AUC for patients with infections were calculated by use of the final model with individual post hoc PK parameters with empirical Bayesian estimation and are summarized by dose regimen. The daily AUC was calculated as the daily dose divided by CL, whereas fTMIC and Cmax were calculated on the basis of steady-state plasma concentrations simulated every 0.25 h. The dose regimens of cefiderocol tested in the cUTI study, where the dose was adjusted on the basis of the patients' renal function and body weight (Table S2), were used in the summary (Table 3). Individual fTMIC values were calculated on the basis of the free concentrations in plasma using a fixed value for the unbound fraction of 0.422 and the MIC of the Gram-negative uropathogen detected at the baseline.
Software.
NONMEM (version 7.3.0) software (22) was used to estimate population PK parameters by the first-order conditional estimation with interaction and to execute simulations. Perl-speaks NONMEM (version 4.2.0) software (23) was used to execute the NONMEM run. R (version 3.0.3) software (24) was used to calculate individual fTMIC, Cmax, and AUC values on the basis of post hoc PK parameters and to create graphics.
Supplementary Material
ACKNOWLEDGMENTS
This study was supported by Shionogi.
N.K., T.K., and T.W. are employees of Shionogi & Co., Ltd. R.E. is a consultant to Shionogi.
Footnotes
Supplemental material for this article may be found at https://doi.org/10.1128/AAC.01391-17.
REFERENCES
- 1.Ito A, Kohira N, Bouchillon SK, West J, Rittenhouse S, Sader HS, Rhomberg PR, Jones RN, Yoshizawa H, Nakamura R, Tsuji M, Yamano Y. 2016. In vitro antimicrobial activity of S-649266, a catechol substituted siderophore cephalosporin, when tested against non-fermenting gram-negative bacteria. J Antimicrob Chemother 71:670–677. doi: 10.1093/jac/dkv402. [DOI] [PubMed] [Google Scholar]
- 2.Kohira N, West J, Ito A, Ito-Horiyama T, Nakamura R, Sato T, Rittenhouse S, Tsuji M, Yamano Y. 2015. In vitro antimicrobial activity of a siderophore cephalosporin, S-649266, against Enterobacteriaceae clinical isolates, including carbapenem-resistant strains. Antimicrob Agents Chemother 60:729–734. doi: 10.1128/AAC.01695-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ito A, Toba S, Nishikawa T, Oota M, Kanazawa S, Fukuhara N, Yamaguchi T, Nakamura R, Tsuji M, Yamano Y. 2015. S-649266, a novel siderophore cephalosporin: binding affinity to PBP and in vitro bactericidal activity, abstr ECCMID-1871. Abstr 25th Eur Congr Clin Microbiol Infect Dis (ECCMID). [Google Scholar]
- 4.Nakamura R, Toba S, Tsuji M, Yamano Y, Shimada J. 2014. A novel siderophore cephalosporin. IV. In vivo efficacy in various murine infection models, abstr F-1558. Abstr 54th Intersci Conf Antimicrob Agents Chemother. American Society for Microbiology, Washington, DC. [Google Scholar]
- 5.Nakamura R, Toba S, Ito A, Tsuji M, Yamano Y, Shimada J. 2014. A novel siderophore cephalosporin. V. Pharmacodynamic assessment in murine thigh infection models, abstr F-1559. Abstr 54th Intersci Conf Antimicrob Agents Chemother. American Society for Microbiology, Washington, DC. [Google Scholar]
- 6.Horiyama T, Toba S, Nakamura R, Tsuji M, Yamano Y, Shimada J. 2014. A novel siderophore cephalosporin. VI. Magnitude of PK/PD parameter required for efficacy in murine lung infection model, abstr F-1560. Abstr 54th Intersci Conf Antimicrob Agents Chemother. American Society for Microbiology, Washington, DC. [Google Scholar]
- 7.Horiyama T, Toba S, Nakamura R, Tsuji M, Yamano Y, Shimada J. 2014. A novel siderophore cephalosporin. VII. Magnitude of PK/PD parameter required for efficacy in murine thigh infection model, abstr F-1561. Abstr 54th Intersci Conf Antimicrob Agents Chemother. American Society for Microbiology, Washington, DC. [Google Scholar]
- 8.Craig WA. 1995. Interrelationship between pharmacokinetics and pharmacodynamics in determining dosage regimens for broad-spectrum cephalosporins. Diagn Microbiol Infect Dis 22:89–96. doi: 10.1016/0732-8893(95)00053-D. [DOI] [PubMed] [Google Scholar]
- 9.Craig WA. 1998. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis 26:1–12. doi: 10.1086/516284. [DOI] [PubMed] [Google Scholar]
- 10.Shimada J, Saisho Y, Katsube T, White S, Fukase H. 2014. S-649266, a novel siderophore cephalosporin for Gram negative bacterial infections: pharmacokinetics, safety and tolerability in healthy subjects, abstr F-1564. Abstr 54th Intersci Conf Antimicrob Agents Chemother. American Society for Microbiology, Washington, DC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Katsube T, Echols R, Arjona Ferreira JC, Krenz HK, Berg JK, Galloway C. 2017. Cefiderocol, a siderophore cephalosporin for Gram-negative bacterial infections: pharmacokinetics and safety in subjects with renal impairment. J Clin Pharmacol 57:584–591. doi: 10.1002/jcph.841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Katsube T, Wajima T, Ishibashi T, Arjona Ferreira JC, Echols R. 2017. Pharmacokinetic/pharmacodynamic modeling and simulation of cefiderocol, a parenteral siderophore cephalosporin, for dose adjustment based on renal function. Antimicrob Agents Chemother 61:e01381-16. doi: 10.1128/AAC.01381-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Portsmouth S, Veenhuyzen D, Echols R, Machida M, Arjona Ferreira JC, Ariyasu M, Nagata T. 2017. Cefiderocol compared with imipenem/cilastatin in the treatment of adults with complicated urinary tract infections with or without pyelonephritis or acute uncomplicated pyelonephritis: results from a multicenter, double-blind, randomized study (APEKS-cUTI), abstr ECCMD-7582. Abstr 27th Eur Congr Clin Microbiol Infect Dis (ECCMID). [Google Scholar]
- 14.Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, Kusek JW, Van Lente F, Chronic Kidney Disease Epidemiology Collaboration. 2006. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med 145:247–254. doi: 10.7326/0003-4819-145-4-200608150-00004. [DOI] [PubMed] [Google Scholar]
- 15.Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, Tomino Y, Yokoyama H, Hishida A. 2009. Collaborators Developing the Japanese Equation for Estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 53:982–992. doi: 10.1053/j.ajkd.2008.12.034. [DOI] [PubMed] [Google Scholar]
- 16.Cockcroft DW, Gault MH. 1976. Prediction of creatinine clearance from serum creatinine. Nephron 16:31–41. doi: 10.1159/000180580. [DOI] [PubMed] [Google Scholar]
- 17.Lin J, Knight EL, Hogan ML, Singh AK. 2003. A comparison of prediction equations for estimating glomerular filtration rate in adults without kidney disease. J Am Soc Nephrol 14:2573–2580. doi: 10.1097/01.ASN.0000088721.98173.4B. [DOI] [PubMed] [Google Scholar]
- 18.Stevens LA, Nolin TD, Richardson MM, Feldman HI, Lewis JB, Rodby R, Townsend R, Okparavero A, Zhang YL, Schmid CH, Levey AS, Chronic Kidney Disease Epidemiology Collaboration. 2009. Comparison of drug dosing recommendations based on measured GFR and kidney function estimating equations. Am J Kidney Dis 54:33–42. doi: 10.1053/j.ajkd.2009.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Baptista JP, Udy AA, Sousa E, Pimentel J, Wang L, Roberts JA, Lipman J. 2011. A comparison of estimates of glomerular filtration in critically ill patients with augmented renal clearance. Crit Care 15:R139. doi: 10.1186/cc10262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chandorkar G, Xiao A, Mouksassi MS, Hershberger E, Krishna G. 2015. Population pharmacokinetics of ceftolozane/tazobactam in healthy volunteers, subjects with varying degrees of renal function and patients with bacterial infections. J Clin Pharmacol 55:230–239. doi: 10.1002/jcph.395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bergstrand M, Hooker AC, Wallin JE, Karlsson MO. 2011. Prediction-corrected visual predictive checks for diagnosing nonlinear mixed-effects models. AAPS J 13:143–151. doi: 10.1208/s12248-011-9255-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Beal SL, Sheiner LB, Boeckmann AJ. 1989-2006. NONMEM users guide. Icon Development Solutions, Ellicott City, MD. [Google Scholar]
- 23.Lindbom L, Pihlgren P, Jonsson EN. 2005. PsN-Toolkit—a collection of computer intensive statistical methods for non-linear mixed effect modeling using NONMEM. Comput Methods Programs Biomed 79:241–257. doi: 10.1016/j.cmpb.2005.04.005. [DOI] [PubMed] [Google Scholar]
- 24.R Core Team. 2013. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.