

Abstract
We report a rare presentation of an anterior inferior cerebellar artery (AICA) infarct in a 74-year-old woman with acute-onset nausea, vomiting, vertigo and gait instability long before the full onset of symptoms and a negative MRI on admission. Over the next several days the patient developed left facial weakness, numbness, hypoacusis, and limb and gait ataxia, and was found to have acute infarcts of the left pons and cerebellar peduncle consistent with an AICA syndrome. We discuss this rare stepwise presentation in AICA syndrome and possible underlying pathophysiology. Such patients at risk for cerebrovascular disease should undergo a careful history, exam and follow-up, even with negative MRI findings, as their symptoms may precede a serious vascular event.
Keywords: brain stem/cerebellum, cranial nerves, neuroimaging, neurootology, stroke
Background
We report a rare stepwise presentation of an anterior inferior cerebellar artery (AICA) infarct, which can guide management in patients with this presentation.
Case presentation
A 74-year-old woman, of Ghanese origin, presented with acute-onset vertigo associated with nausea, vomiting, left ear tinnitus and gait instability. Her medical history was notable only for diabetes, for which she was not taking any medications. Her social and family history were non-contributory.
Investigations
On physical examination, she had gait ataxia and left limb dysmetria, but no ophthalmoplegia, nystagmus, dysarthria, facial numbness, weakness or Horner’s syndrome.
The patient had stable vital signs and unremarkable laboratory data and viral serology. MRI showed no diffusion restriction, with only some scattered punctate subcortical white matter signal changes.
Differential diagnosis
With ataxia and dysmetria on exam, there was concern for a cerebellar lesion. However, with no acute infarcts or structural lesions on MRI, she was considered to have a peripheral vestibular disorder, supported by the vertigo and tinnitus.
Treatment
The patient was treated with intravenous steroids for presumed vestibular neuritis, with some improvement in her dizziness and nausea over several days.
Outcome and follow-up
Five days into the hospitalisation, she developed left facial weakness in a lower motor neuron pattern and left facial numbness. A repeat MRI showed an acute left AICA distribution infarct involving the pons and the middle cerebellar peduncle (figure 1). The patient underwent a thorough cardiovascular work-up and was started on dual antiplatelet therapy for basilar atherosclerosis. With supportive management, she had improvement in her symptoms over the next few days. The ataxia took several weeks to fully resolve.
Figure 1.
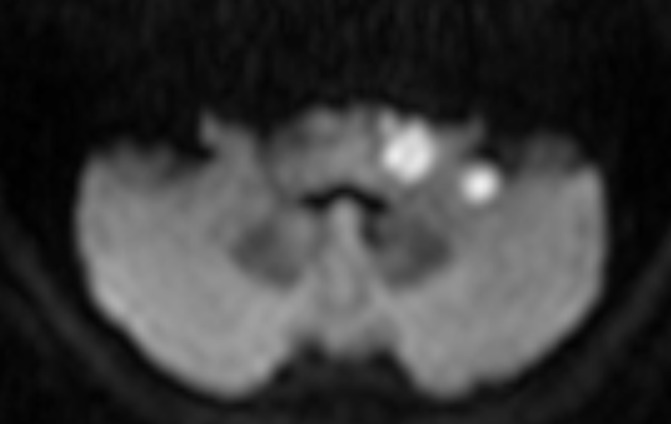
Repeat MRI with foci of diffusion restriction in the left pons and the middle cerebellar peduncle consistent with an acute infarct.
Discussion
Adams1 was first to describe the clinical syndrome associated with an AICA infarction. Patients present with acute-onset nausea, vertigo, ataxia, tinnitus and hypoacusia, which can be mistaken for an inner ear disorder. The inner ear is supplied by the internal auditory artery (IAA), and in most people arises from the AICA and to a lesser degree from the basilar artery or the posterior inferior communicating artery (PICA). The AICA, in turn, is a branch of the basilar artery, additionally vascularising the dorsolateral inferior pons, anteroinferior cerebellum and the eighth nerve. Commonly affected structures involve the nuclei and/or roots of the trigeminal, facial and vestibulocochlear nerve, acoustic structures, and the anterolateral spinothalamic tract, and explain the characteristic cranial nerve and crossed sensory findings.2 The cerebellar signs stem from lesions of the middle cerebellar peduncle, restiform body, ventral spinocerebellar tract or the cerebellar hemispheres.
The IAA has little collateral blood supply and is particularly susceptible to ischaemia. In contrast, the vestibulocochlear nerves have a rich network of anastomotic vessels from arteries supplying the adjacent dura mater, petrous bone, as well as branches of the AICA and PICA. As such, their involvement depends on the integrity of the collateral arterial supply.3 Most stroke syndromes start suddenly and are worst at onset. A minority of patients, however, have a more stepwise course. Per a recent review, somewhere between 8% and 31% of patients with an AICA infarct have a prodrome of audiovestibular disturbance before the onset of other central symptoms.4 A smaller percentage have normal MRIs on presentation. In a study of 54 consecutive patients who were diagnosed with AICA territory strokes, 4 had normal MRIs on presentation.5 This suggests that rarely patients have transient ischaemia to the inner ear preceding a complete infarct and syndrome. An MRI during this time may show no restricted diffusion, which can delay diagnosis.
Learning points.
At-risk patients with vertigo, without typical complaints of common inner ear disorders, should have a thorough evaluation and close follow-up.
In select cases, there may be an indication for audiometry to detect subclinical hearing loss, as well as primary prevention with antiplatelet and cholesterol-reducing medications.
Footnotes
Contributors: SHS: design, draft and revision. FN: draft, critical revision of content. DL: critical revision of content.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Adams RD. Occlusion of the anterior inferior cerebellar artery. Arch Neurol Psychiatry 1943;49:765–70. 10.1001/archneurpsyc.1943.02290170135010 [DOI] [Google Scholar]
- 2. Amarenco P, Hauw JJ. Cerebellar infarction in the territory of the anterior and inferior cerebellar artery. A clinicopathological study of 20 cases. Brain 1990;113:139–55. [DOI] [PubMed] [Google Scholar]
- 3. Martin RG, Grant JL, Peace D, et al. Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve complex. Neurosurgery 1980;6:483–507. 10.1227/00006123-198005000-00001 [DOI] [PubMed] [Google Scholar]
- 4. Kim HA, Lee H. Recent advances in understanding audiovestibular loss of a vascular cause. J Stroke 2017;19:61–6. 10.5853/jos.2016.00857 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kim JS, Cho KH, Lee H. Isolated labyrinthine infarction as a harbinger of anterior inferior cerebellar artery territory infarction with normal diffusion-weighted brain MRI. J Neurol Sci 2009;278(1-2):82–4. 10.1016/j.jns.2008.12.002 [DOI] [PubMed] [Google Scholar]