

Abstract
Objectives:
To determine the optimal cutoff value for neck circumference (NC) that define overweight/obesity and assess its predictive potential for cardiometabolic risks (CMR) among Saudi subjects.
Methods:
A cross sectional study of 785 adults recruited from a public health awareness campaign in Medina, Saudi Arabia during June 2015. Waist circumference (WC), NC, body mass index (BMI), blood pressure (BP), and random blood glucose (RBG) were assessed, and the presence of CMR were collected by a questionnaire. Pearson’s correlation coefficients were used to evaluate the associations of NC with other anthropometric indices and CMR. The optimal cutoff value for NC to identify overweight/obesity was determined by receiver operating characteristic (ROC) curves.
Results:
There were significant correlations between NC and BMI, weight, WC, age, RBG, and BP. The area under the curve for NC and WC in the ROC analysis was 0.86 for men and 0.77 for women, and NC ≥39.25 cm for men and ≥34.75 cm for women were the best cutoff levels for identifying subjects with central obesity with an 89% sensitivity and a 71% specificity for men and an 80% sensitivity and a 65% specificity for women. These cutoff levels for NC were associated with a significantly increased risk for diabetes, dyslipidemia, and hypertension.
Conclusion:
Neck circumference is positively correlated with BMI and WC, and can be used to identify overweight/obesity and predict CMR in Saudi individuals.
Obesity is widely correlated with cardiometabolic risk and is strongly associated with diabetes, dyslipidemia, and hypertension. There are many approaches for assessing obesity. Some measurements, such as weight, waist circumference (WC), waist: hip ratio, and body mass index (BMI) are commonly used at primary care centers, while other measurements, such as ultrasound, CT scan, and MRI, are costly and largely used for research purposes.1 While BMI is frequently used to assess for overweight and obesity, it does not differentiate between fat and other tissues, such as muscles, and does not account for regional fat distribution. Waist circumference, as an index of central obesity, may be better for predicting obesity-related health risks than BMI. Nevertheless, WC measurements may be inconvenient or difficult to obtain in some situations, such as with severely obese subjects. In addition, WC measurements are affected by fullness of the abdomen after a meal or due to abdominal gases or pregnancy. Moreover, respiratory movement and thick clothing can also affect the accuracy of WC measurements.2 Recent studies have revealed that neck circumference (NC), as an index of upper-body subcutaneous adipose tissue distribution, is a good tool to identify overweight and obesity1,3-6 and it is associated with cardiometabolic risks (CMR) beyond that of BMI and WC.7-10 Neck circumference measurement is easy to perform, quick, reliable, and inexpensive. In addition, its measurement is convenient and not affected by the aforementioned factors that influence WC measurement. Because there is heterogeneity in body size among different ethnic populations, the cut-off values for the classic anthropometric indices such as BMI and WC and their predictive potential for CMR are varied.11 The aim of the current study was to determine the optimal cutoff value for NC to identify overweight/obesity and assess its predictive potential for CMR among Saudi subjects.
Methods
The study was a cross-sectional study involving adult Saudi subjects 18 years of age and older of both genders. The subjects were recruited during a public health awareness campaign in Medina, Kingdom of Saudi Arabia, during June 2015. Subjects with goiters or thyroid nodules and pregnant women were excluded. The study was approved by the research and human ethics committee of Taibah University, Medina. The study was carried out according to principles of Helsinki Declaration.
After receiving informed consent from the participants, assessments of the demographic data and the presence of atherosclerotic cardiovascular diseases such as ischemic heart disease, diabetes, hypertension, and dyslipidemia were collected by a questionnaire through face-to-face interviews. Height, weight, WC, NC, and BP were measured in all participants and the random blood glucose (RBG) level was obtained using a finger stick. The WC was measured midway between the lower costal margin and the upper iliac crest. The NC was measured in the middle of the neck between the mid-cervical spine and mid-anterior neck. In subjects with a laryngeal prominence, NC was taken below the prominence. All circumferences were measured while the subjects were standing upright with their faces kept straight and their shoulders relaxed. The BMI was calculated as weight (kg)/height (m)2. Central obesity was defined according to the National Cholesterol Education Program-Third Adult Treatment Panel as WC ≥102 cm for men and ≥88 cm for women.11
Statistical analyses were performed using Statistical Package for the Social Sciences software (version 20.0; SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as the mean±standard deviation (SD), and categorical variables were expressed as numbers (percentages). An independent t-test was used for continuous variables, and a Chi-square analysis was used for categorical variables. Receiver operating characteristic (ROC) curves were used to determine the optimal cutoff value for NC to identify overweight/obesity. Pearson’s correlation coefficients were used to evaluate the associations of NC with other anthropometric indices and CMR. A p<0.05 was used as the cut-off value for significance.
Results
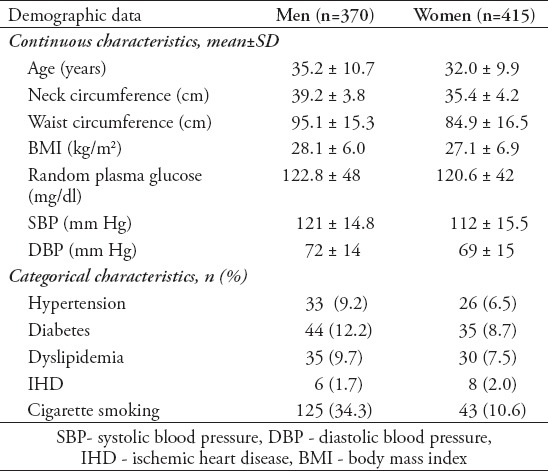
This study involved 785 adults, including 415 (52.4%) women and 370 (46.6%) men, with a mean age of 33.31 (range 18-65). The demographic data for the participants are presented in Table 1. The mean NC was 39.19±3.9 cm for men and 35.32± 4.2 cm for women. Sixty-two percent of the participants were overweight or obese, 68% of the men and 55.3% of the women. The mean NC of the subjects with normal weights was 36.74±2.8 cm for the men and 33.5±3.4 cm for the women.
Table 1.
Demographic data of 785 participants.
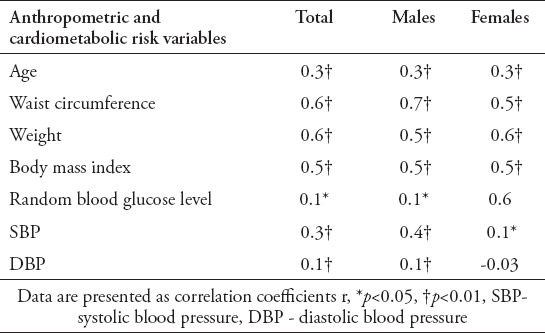
Pearson’s correlation coefficients revealed significant positive associations between NC and WC, BMI, weight, age, RBG, systolic blood pressure (SBP) and diastolic blood pressure (DBP). All of these associations were observed in both genders except for RBG and DBP, which were not associated with NC in female subjects (Table 2).
Table 2.
Pearson correlation coefficients for neck circumference with anthropometric measurements and cardiometabolic risks
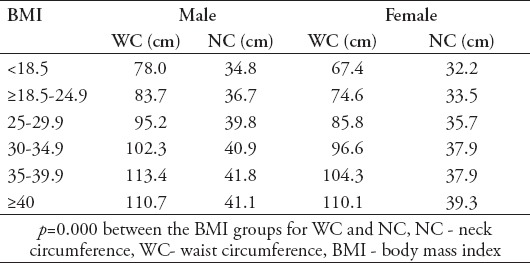
The mean NCs for the subjects with central obesity, defined as a WC ≥102 cm for men and ≥88 cm for women, were 39.4 cm for men and 37.6 cm for women. The mean NC and WC of the subjects according to the BMI categories are presented in Table 3.
Table 3.
Waist circumference and NC according to the BMI groups in both genders.
The ROC analysis showed that the area under the curve (AUC) for NC and central obesity was 0.86 for men (p=0.000) and 0.77 for women (p=0.000) (Figures 1 & 2). Neck circumferences that were ≥39.25 cm for men and ≥34.75 cm for women were the best cutoff levels for identifying the subjects with central obesity, with a sensitivity of 89% and a specificity of 71% for men and a sensitivity of 80% and a specificity of 65% for women. These cutoff levels of NC were associated with a significant increase in the risk of type 2 diabetes (p=0.000), dyslipidemia (p=0.001), and hypertension (p=0.005) with odds ratio of 2.6 (95% CI 1.6-4.3), 2.6 (95% CI 1.2-3.9), and 1.9 (95% CI 1.2-3), respectively.
Figure 1.
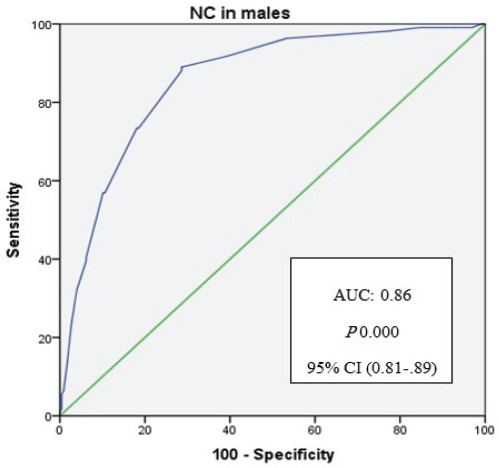
Receiver operating characteristic curves related to neck circumference and central obesity (waist circumference >102 cm) in males. Diagonal segments are produced by ties. NC - neck circumference
Figure 2.
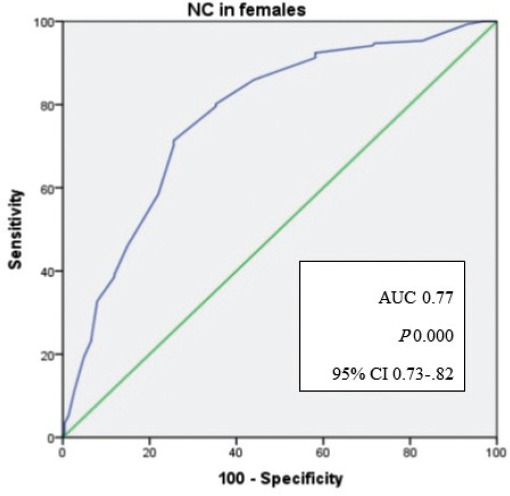
Receiver operating characteristic curves related to neck circumference and central obesity (waist circumference >88 cm) in females. Diagonal segments are produced by ties. NC - neck circumference
Discussion
Upper-body subcutaneous fat accumulation in the neck appears to be associated with CMR beyond generalized adiposity. To elucidate the application of NC as an indicator of overweight/obesity among Saudi subjects and to investigate its importance as a predictor for CMR, we performed this cross-sectional survey of 785 adult participants in Madinah, Saudi Arabia.
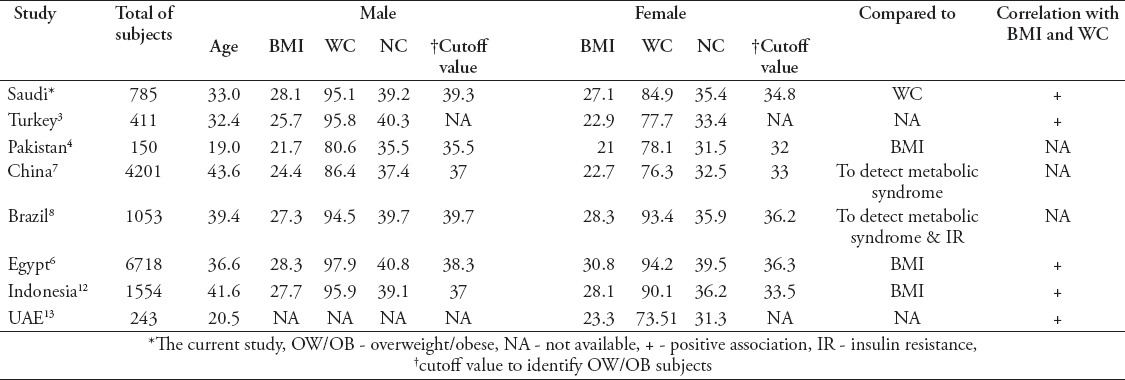
The mean NC for the participants in the current study was 39.2±3.8 in men and 35.4±4.2 in women, which was comparable to those figures reported for Brazilians,8 and Indonesians12 but lower than those reported for Egyptians6 and higher than those for Pakistani,4 Chinese,7 and United Arab of Emirate (UAE)13 subjects. The lower mean NC reported in the Pakistani and UAE studies was due to the inclusion of only young college students aged 18 to 20 years with a mean BMI 21.3.4,13 On the other hand, a study from Turkey reported a higher mean NC for men and a lower mean NC for women compared to our figures (Table 4).3
Table 4.
Cutoff value for neck circumferences (NC) among different populatio
In the present study, there was a high prevalence of overweight/obesity in 62% of the participants; 68% men and 55.3% women. These results are similar to those reported by the World Health Organization for Saudi men aged 18 years and older, but lower than those reported for Saudi women (71.9%).14 Consistent with the results of previous studies,3,4,6,7 our study revealed significant positive correlations between NC and the conventional anthropometric measures of obesity (weight, BMI, and waist circumference). In previous study that evaluated neck adipose tissue and abdominal visceral adipose tissue using computer tomography, NC was positively associated with abdominal visceral fat.15
Furthermore, we observed a significant positive correlation between NC and SBP in both genders and between NC and DBP in men but not women. Similarly, we identified a positive correlation between NC and RBG in men but found no correlation in women. These differences could be attributed to the sample size of the study. Several previous studies have shown positive correlations between NC and SBP, DBP,5,7 and glucose level in both genders.10
A NC of ≥39.25 cm for men and ≥34.75 cm for women might be considered the cutoff value for the identification of overweight/obesity of the Saudi population. Comparable cutoff values were suggested for Brazilian8 and Egyptian men,6 while lower cutoff values were suggested for Chinese,7 Indonesian,12 and Pakistani4 men. In women, lower cutoff values were suggested for Chinese,7 Indonesian,12 and Pakistani4 and higher cutoff values for Brazilian8 and Egyptian women6 (Table 4). Differences in body size among different populations might clarify the heterogeneity of the cut-off values for NC, which is the case for other standard anthropometric measures such as BMI and WC. The lower cut-off values for NC in the Chinese and Indonesian population could be explained by the smaller body size of populations from the Far East. Differences in the mean age of the studies’ participants, sample size of the study, and the differences in the parameter to which NC was compared to define the cut off value for overweight/obesity, could be other factors contributing to the differences in the cut-off values for NC between different populations.
The cutoff level for NC in the current study was associated with significant increases in the risks of type 2 diabetes, dyslipidemia, and hypertension with odds ratios of 2.6, 2.6 and 1.9, respectively. These results are in agreement with many studies that have revealed this association even after adjustment for the levels of visceral adiposity.2,7-9 Moreover, the results of a recent study suggest that NC performs better than WC in the assessment of metabolic health in individuals with severe obesity.2
Study limitation
This stud was conducted only in one region of Saudi Arabia; therefore, selection bias cannot be excluded. However, the study was conducted during the summer in a public mall where there were many visitors from different regions of Saudi Arabia. The study design was also cross-sectional, which may limit its interpretation of the causality of associations. Finally, we did not measure lipid levels and examined their correlation with NC to obtain a complete profile of the metabolic syndrome. Further longitudinal studies from different regions of Saudi Arabia are required to confirm our results.
Acknowledgment
The authors gratefully acknowledge the Taibah Medical Club (TMC), Taibah University, Medina, Kingdom of Saudi Arabia, for arranging the campaign and our appreciation to the TMC members for their crucial role in collecting the data.
Footnotes
References
- 1.Ben-Noun L, Sohar E, Laor A. Neck circumference as a simple screening measure for identifying overweight and obese patients. Obes Res. 2001;9:470–477. doi: 10.1038/oby.2001.61. [DOI] [PubMed] [Google Scholar]
- 2.Joshipura K, Mu-oz-Torres F, Vergara J, Palacios C, Pérez CM. Neck Circumference May Be a Better Alternative to Standard Anthropometric Measures. J Diabetes Res. 2016;2016:6058916. doi: 10.1155/2016/6058916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Saka M, Türker P, Ercan A, Kiziltan G, Baş M. Is neck circumference measurement an indicator for abdominal obesity? A pilot study on Turkish Adults. Afr Health Sci. 2014;14:570–575. doi: 10.4314/ahs.v14i3.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hingorjo MR, Qureshi MA, Mehdi A. Neck circumference as a useful marker of obesity: a comparison with body mass index and waist circumference. J Pak Med Assoc. 2012;62:36–40. [PubMed] [Google Scholar]
- 5.Hatipoglu N, Mazicioglu MM, Kurtoglu S, Kendirci M. Neck circumference: an additional tool of screening overweight and obesity in childhood. Eur J Pediatr. 2010;169:733–739. doi: 10.1007/s00431-009-1104-z. [DOI] [PubMed] [Google Scholar]
- 6.Sarry El Din A, Hassan N, El-Masry S, Al-Tohamy M. Neck circumference as a simple screening measure for identifying Egyptian overweight and obese adults. Maced J Med Sci. 2013;6:232–237. [Google Scholar]
- 7.Zhou JY, Ge H, Zhu MF, Wang LJ, Chen L, Tan YZ, et al. Neck circumference as an independent predictive contributor to cardio-metabolic syndrome. Cardiovasc Diabetol. 2013;12:76. doi: 10.1186/1475-2840-12-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stabe C, Vasques AC, Lima MM, Tambascia MA, Pareja JC, Yamanaka A, et al. Neck circumference as a simple tool for identifying the metabolic syndrome and insulin resistance: results from the Brazilian Metabolic Syndrome Study. Clin Endocrinol (Oxf) 2013;78:874–881. doi: 10.1111/j.1365-2265.2012.04487.x. [DOI] [PubMed] [Google Scholar]
- 9.Preis SR, Massaro JM, Hoffmann U, D'Agostino RB, Sr, Levy D, Robins SJ, et al. Neck circumference as a novel measure of cardiometabolic risk: the Framingham Heart study. J Clin Endocrinol Metab. 2010;95:3701–3710. doi: 10.1210/jc.2009-1779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ben-Noun L, Laor A. Relationship of neck circumference to cardiovascular risk factors. Obes Res. 2003;11:226–231. doi: 10.1038/oby.2003.35. [DOI] [PubMed] [Google Scholar]
- 11.Alberti KG, Zimmet P, Shaw J. Metabolic syndrome--a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006;23:469–480. doi: 10.1111/j.1464-5491.2006.01858.x. [DOI] [PubMed] [Google Scholar]
- 12.Lindarto D, Shierly Syafril S. Neck circumference in overweight/obese subjects who visited the binjai supermall in Indonesia. Open Access Maced J Med Sci. 2016;4:319–323. doi: 10.3889/oamjms.2016.072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Papandreou D, Noor ZT, Rashed M, Jaberi HA. Association of neck circumference with obesity in female college students. Open Access Maced J Med Sci. 2015;3:578–581. doi: 10.3889/oamjms.2015.118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.World Health Organization. Global Health Observatory (GHO) Global and regional trends by WHO Regions 1990-2013. Overweight. [Internet] Geneva (CH): WHO; 2014. Available from http://www.who.int/gho/en/ [Google Scholar]
- 15.Li HX, Zhang F, Zhao D, Xin Z, Guo SQ, Wang SM, et al. Neck circumference as a measure of neck fat and abdominal visceral fat in Chinese adults. BMC Public Health. 2014;14:311. doi: 10.1186/1471-2458-14-311. [DOI] [PMC free article] [PubMed] [Google Scholar]