

Abstract
Objectives:
To measure the prevalence of antenatal depression among pregnant women attending the primary health care (PHC) antenatal care clinics in Jeddah, Saudi Arabia and to determine associated factors.
Methods:
Following a cross-sectional study design, 320 pregnant women attending the antenatal care clinics in the Ministry of Health PHC Centers in Jeddah, Saudi Arabia between January 1st 2017 and February 15th 2017 were interviewed. A self-administered questionnaire used for data collection asked about socio-demographic variables and included the Edinburgh Postnatal Depression Scale.
Results:
The most common contributor was the harming herself (mean±SD, 2.7±0.60). Factors significantly associated with depression among participants were the number of daughters, previous diagnosis of depression, and financial problems.
Conclusions:
The prevalence of antepartum depression among pregnant women in Jeddah is 57.5%, and the greatest contributor is the thought of harming herself.
Antenatal depression is a depressive episode that begins during pregnancy, and if untreated, it is a significant predictor of postpartum depression. Research conducted in the U.S. showed that one-third of postnatal depression cases begin during pregnancy. Evidence indicates that symptoms of depression during pregnancy are more prevalent than during the postnatal period.1 Depressed mothers cannot function properly, and they are prone to adverse effects including noncompliance with prenatal care clinic attendance, being less concerned with her health in general, decreasing the quantity of their nutrition, getting irregular or reduced sleep, and pre-eclampsia. They might also have increased uterine irritability, preterm delivery, and postpartum bleeding, and symptoms could be so severe that they commit suicide.2,3 Negative consequences associated with babies of mothers with antenatal depression include increased risk of low birth weight or small-for-gestational age, smaller head circumference, stillbirth, and birth asphyxia. Maternal depressive symptoms and stress during the second and third trimesters were shown to be inversely related to poorer mother-infant bonding during the postnatal period. Antenatal depression also has negative outcomes on the mother’s social and personal adjustments and marital relationships.2-5 Almost 10% of pregnant women worldwide experience depression, and the rate is higher (15%) in developing countries. It has been estimated that depressive disorders will be the leading cause of global disease burden in women by the year 2020.6,7 The prevalence of antenatal depression was 33.8% in Tanzania.5 Al-Azri et al8 showed that the prevalence of antenatal depression among Omani women was 24.3%. In Egypt, Abdelhai et al9 showed that 63% of women expressed simultaneous anxiety and depression. The literature on depression during pregnancy in Saudi Arabia is scarce. A study performed in Riyadh City reported that the prevalence was around 18.6%.3 Diagnosing antenatal depression is difficult because the physiological signs of normal pregnancy overlap the symptoms of antenatal depression.2 A recent systematic review in Tanzania recommended administering a screening tool to identify women with antenatal depression, and it should be a universal practice to promote the long-term well-being of mothers and babies.5
Antenatal depression has not been sufficiently studied because most studies of maternal depression focus on postpartum depression.2,10 Moreover, antenatal depression has increased worldwide, and early detection and proper management are cornerstones to preventing serious complications such as postpartum depression and psychosis. Therefore, this study aimed to measure the prevalence of antenatal depression and to determine the associated risk factors associated among pregnant women attending prenatal care clinics at Ministry of Health primary care centers in Jeddah, Saudi Arabia.
Methods
Following a cross-sectional design, this study included 320 women who attended the antenatal clinics at 8 primary health care (PHC) centers from the northern part, and 6 PHC centers from the southern part of Jeddah City, Saudi Arabia, between January 1st 2017 and February 15th 2017. Using the Raosoft website,11 the sample size (n=320) was calculated to detect an expected 20% prevalence of antenatal depression with a 4% margin of error and 80% statistical power using a total population of 2,000 and a confidence level of 95%.
The inclusion criteria were pregnant women living in Jeddah, with a gestational age greater than 8 weeks attending an antenatal clinic in the selected PHC centers and any pregnant women not fulfilling these inclusion criteria were excluded.
Written official approval was obtained from the Joint Program of Family and Community Medicine before conducting the research. Approval by a higher authority (Ministry of Health) was also received. The study was conducted according to the principles of the revised Declaration of Helsinki. Written anonymous consents were received from all participants on the first page of the questionnaire, where a direct question asked for the participant to check a box signifying consent before answering any other sections of the questionnaire. No names, file numbers, or any identifying information was obtained, and all collected data were kept confidential, giving access only to the researcher and statistician. All women who were approached were given a full explanation of the study and were informed of their rights to refuse to participate. However, those women diagnosed with antenatal depression were referred immediately to their primary doctor.
The data collection tool comprised a self-administered questionnaire that consisted of the sociodemographic characteristic questionnaire and the translated Arabic version of the Edinburgh Postnatal Depression Scale (EPDS) questionnaire, validated by the Department of Health, Government of Western Australia, copyrighted in 2006. It is a widely-used first step for identifying antenatal depression and was successfully used in the current study. It had been proven valid and reliable for identifying women at risk for depression during and after pregnancy. Its reliability and validity in psychiatric and epidemiologic studies have been extensively demonstrated.5,12 Scores of at least 13 were considered to indicate probable antenatal depression and the need for further evaluation.
The IBM SPSS Statistics for Windows (IBM Corp, Armonk, NY, USA) version 21 package was used for statistical analysis. All categorical data were defined in terms of number (%), and numerical data were defined in terms of means and standard deviations (SDs). Binary logistic regression was performed to assess the association between antenatal depression and factors potentiating depression in pregnant women. Statistical significance was recognized when p-value was less than 0.05.
Results
Half the interviewed pregnant women (51.2%) were aged between 28 and 37 years; only 6 (1.9%) were aged less than 17 years. Most (83.4%) of the women, as well as their husbands (80.9%), had high education levels. Nevertheless, more than half the women (57.5%) were jobless, and the most common job was teacher (17.5%). Most (97.1%) were currently married. One-third of the women (33.1%) reported monthly incomes of more than 10,000 SR, and 41.6% reported monthly incomes ranging between 5,000 and 10,000 SR (Table 1).
Table 1.
Characteristics of the interviewed pregnant women (N=320).
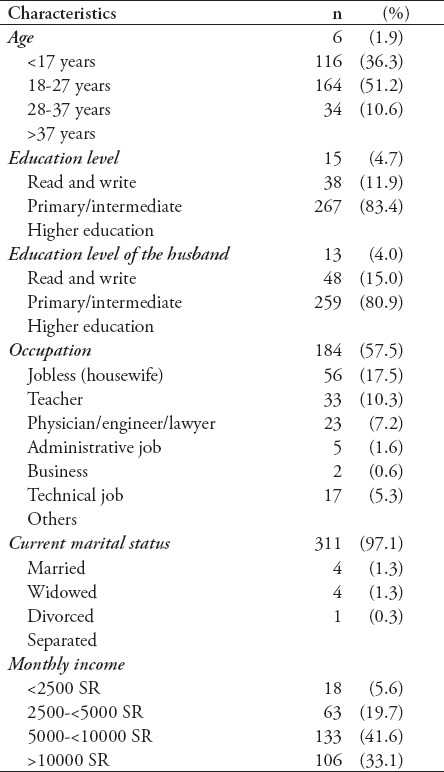
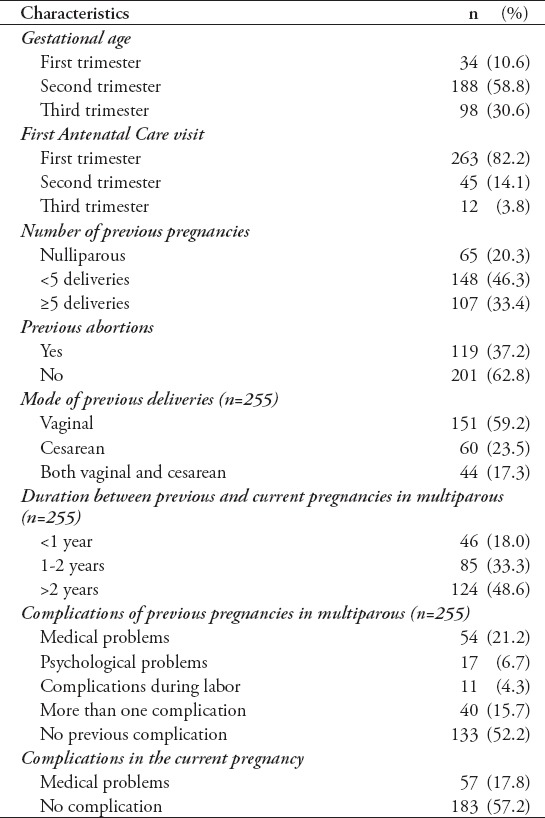
Table 2 shows that most participants were either in their second (58.8%), or third (30.6%) trimester, and that most (82.2%) indicated they started their antenatal care visits in the first trimester. Most were multiparous, and almost half (46.3%) had been pregnant fewer than 5 times. One-third (33.4%) reported more than 5 deliveries. More than one-third (37.2%) stated they had previous abortions. Almost one-quarter (23.5%) of the multiparous women had previous cesarean sections, and 17.3% previously had both vaginal and cesarean section births. It had been more than 2 years since the previous pregnancy for 48.6% of the multiparous participants. A total of 47.8% of the women experienced complications in previous pregnancies, and most were medical (21.2%) and psychological (6.7%) problems. Additionally, 15.7% had more than one complication. In the current pregnancy, 17.8% stated they experienced a medical problem, 12.8% stated they experienced a psychological problem, and 12.2% stated they experienced more than one complication (Table 2). We found that 48.1% of the participants planned for the current pregnancy, but 36.3% did not. Furthermore, 10% expressed that “it is not welcomed from their own side,” and 5.6% said, “it is not welcomed by the husband.” Results show that half (43.9%) of the multiparous pregnant women had 3 or more previous live births, and most (92.9%) had less than 3 male children. Fewer (78%) had less than 3 female children. Slightly less than half (46.7%) of the multiparous women indicated they had previous low birth weight babies. More women indicated that their current fetus was female versus male (39.4% versus 29.4%). However, 46.8% wished that the current baby would be male, whereas 26.6% wished it were female.
Table 2.
Obstetric history of 320 women who attended the antenatal clinics.
Results show that almost half (45%) of the participants complained of a lack of support at home, and almost one-third (32.2%) were employed while 28.1% had financial difficulties. Additionally, 17 (5.3%) of the women claimed they had been exposed to violence. The majority (87.5%) reported that one or more family members were suffering from psychological problems, and of those, 10.9% were their mothers, and 33.4% were in more than one family member. One in five (21.6%) expressed they were diagnosed with depression, 12.1% looked for medical consultation, and 14 (4.4%) received treatment. About two-thirds (62.2%) stated they had sleep disorders.
Of those who had previous abortions (n=119), most (110, 92.4%) reported they suffered from one or more psychological problems following abortion, mostly grief (46.2%), depressed mood and disappointment (16.8%), and anxiety (12.6%). Additionally, 16.8% suffered from a combination of these. Based on the overall sum of scores for the items on the EPDS, results illustrate that more than half of the participants had depression (57.5%).
Table 3 shows the contribution of each item of the EPDS on the overall score. The ones that contributed the most were the thought of harming herself (mean ± SD, 2.7 ± 0.60), being anxious without reason (1.7 ± 0.88), unhappiness to the extent of crying (1.7 ± 0.94), and feeling sad, or miserable (1.6 ± 0.60; Table 3).
Table 3.
Mean scores for the response of the pregnant women on the EPDS items assessing depression (Score 0-3 for each item).
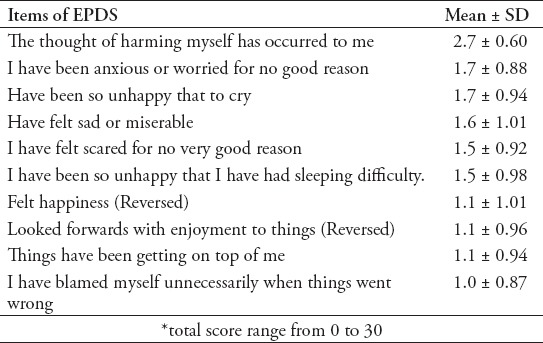
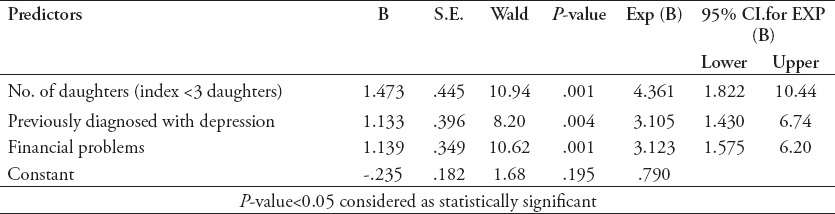
Table 4 shows the logistic regression model for predictors of antenatal depression based on our participant group. The number of daughters, previous diagnosis of depression, and financial problems were significant predictors. Controlling for other factors, having more than 3 daughters increases the likelihood for depression by almost four-fold (odds ratio, 4.361, 95% confidence interval [CI]: 1.822-10.436), previous diagnosis with depression increases it by almost three-fold (odds ratio, 3.105, 95% CI: 1.430-6.741), and financial problems increase it by around 3-fold (odds ratio, 3.123, 95% CI: 1.575-6.195; p<0.05; Table 4).
Table 4.
Logistic regression for predictors of antenatal depression.
Discussion
This current study shows that more than half (57.5%) the participants had antenatal depression, a prevalence which is slightly higher than that reported by Moawed et al,3 who found the prevalence was 44.2% among pregnant women in Riyadh, Saudi Arabia. These dissimilarities could be attributed to the assessment tools used. We used the EPDS, which has proven validity and reliability,11 rather than the Beck Depression Inventory. In addition, our study setting was PHC centers rather than a hospital.
Our detected prevalence was lower than that found in Egypt, where 63% of pregnant women expressed simultaneous anxiety and depressive manifestations.9 This difference might be due to the inclusion of anxiety with depression. On the other hand, much lower figures were found in Finland (0.8%),14 Spain (14.8%),15 Turkey (16.8%),16 Cote d’Ivoire (32.9%),17 and Tanzania (33.8%).5
Fisher et al18 found that depression in pregnancy is at least as prevalent in high- as in low-income countries, if not more so. Wide variations in reported prevalence rates could stem from differences in study setting, sampled population, or measurement and assessment tools.
Several researchers found factors that are either associated with or potentiate antenatal depression. The greatest risk factor for major depression during pregnancy is a history of depression before pregnancy, which was associated with a 22.4-fold increase in the prevalence of major depression during pregnancy.13 This strong association was evident in our study: a significantly higher prevalence of antenatal depression was found among those who reported depression diagnoses, who needed medical consultations, and who were treated for depression (odds ratio, 3.123, 95% CI; 1.575-6.195).
Shidhaye et al19 assessed the association between gender preference for a male child with antenatal depression in rural Maharashtra and demonstrated that the desire to deliver a male child was strongly associated with the outcome of antenatal depression. Moreover, Escriba-Aguir et al20 attributed this response to disappointed spouses in addition to negative reactions of family members toward the birth of a female, thus initiating or exacerbating depression. This notion supports our findings that antenatal depression is significantly more likely to occur in mothers who have three or more daughters.
El-Behadli et al21 noted that family financial resources might not be directly related to antenatal depression, but it could mediate the influence of social support and fears of not meeting the demands of the coming child. This is consistent with our findings, where a significantly higher proportion of those with antenatal depression reported family financial problems.
The limitations of this study are the sample size of 320, which was calculated for a one-month duration, but it takes 2 weeks more to reach this target sample size because of the limited number of ANC clinics in PHC centers and the lack of participation. Also, there are fewer pregnant women attending PHC centers for ANC compared to specialized obstetrics and gynecology clinics in hospitals. Intensive research and clinical attainment must be directed toward early detection and understanding antenatal depression to develop powerful interventions that are suitable for integration into the PHC system in Saudi Arabia.
In conclusion, the prevalence of antepartum depression is high among pregnant women in Jeddah. The greatest contributors are for the though of self-harming being anxious without reason, being unhappy to the extent of crying, and feeling sad or miserable. Several risk factors are associated with antepartum depression and include delivery of female babies, having past or a family history of depression, and exposure to financial problems.
We therefore recommended that pregnant women be routinely screened for depression during antenatal care. The necessary psychological care for pregnant women, especially those with risk factors for antenatal depression, should be provided by PCH centers. Moreover, pregnant women and their family members should receive health education about measures they can take to avoid antenatal depression.
Footnotes
References.
*References should be primary source and numbered in the order in which they appear in the text. At the end of the article the full list of references should follow the Vancouver style.
*Unpublished data and personal communications should be cited only in the text, not as a formal reference.
*The author is responsible for the accuracy and completeness of references and for their correct textual citation.
*When a citation is referred to in the text by name, the accompanying reference must be from the original source.
*Upon acceptance of a paper all authors must be able to provide the full paper for each reference cited upon request at any time up to publication.
*Only 1-2 up to date references should be used for each particular point in the text.
Sample references are available from: http://www.nlm.nih.gov/bsd/uniform_requirements.html
References
- 1.Ashley JM, Harper BD, Arms-Chavez CJ, LoBello SG. Estimated prevalence of antenatal depression in the US population. Arch Womens Ment Health. 2016;19:395–400. doi: 10.1007/s00737-015-0593-1. [DOI] [PubMed] [Google Scholar]
- 2.Zeng Y, Cui Y, Li L. Prevalence and predictors of antenatal depressive symptoms among Chinese women in their third trimester: a cross-sectional survey. BMC Psychiatry. 2015;15:66. doi: 10.1186/s12888-015-0452-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Moawed SA, Gemaey EM, Al-Mutairi HA. Prevalence of Depression among Saudi Pregnant Women. IOSR Journal of Nursing and Health Science. 2015;4:61–68. [Google Scholar]
- 4.Rossen L, Hutchinson D, Wilson J, Burns LA, Olsson C, Allsop S, et al. Predictors of postnatal mother-infant bonding: the role of antenatal bonding, maternal substance use and mental health. Arch Womens Ment Health. 2016;19:609–622. doi: 10.1007/s00737-016-0602-z. [DOI] [PubMed] [Google Scholar]
- 5.Rwakarema M, Premji SS, Nyanza EC, Riziki P, Palacios-Derflingher L. Antenatal depression is associated with pregnancy-related anxiety, partner relations, and wealth in women in Northern Tanzania: a cross-sectional study. BMC Womens Health. 2015;15:68. doi: 10.1186/s12905-015-0225-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World Health Organization. Maternal Mental Health. Available from URL: www.who.int/reproductivehealth/publications/general/9789241563567/en/
- 7.Bohra N, Srivastava S, Bhatia MS. Depression in women in Indian context. Indian J Psychiatry. 2015;57:S239–S245. doi: 10.4103/0019-5545.161485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Al-Azri M, Al-Lawati I, Al-Kamyani R, Al-Kiyumi M, Al-Rawahi A, Davidson R, et al. Prevalence and Risk Factors of Antenatal Depression among Omani Women in a Primary Care Setting: Cross-sectional study. Sultan Qaboos Univ Med J. 2016;16:e35–e41. doi: 10.18295/squmj.2016.16.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Abdelhai R, Mosleh H. Screening for antepartum anxiety and depression and their association with domestic violence among Egyptian pregnant women. J Egypt Public Health Assoc. 2015;90:101–108. doi: 10.1097/01.EPX.0000471670.64665.8f. [DOI] [PubMed] [Google Scholar]
- 10.O'Connor E, Rossom RC, Henninger M, Groom HC, Burda BU. Primary Care Screening for and Treatment of Depression in Pregnant and Postpartum Women Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2016;315:388–406. doi: 10.1001/jama.2015.18948. [DOI] [PubMed] [Google Scholar]
- 11.Raosoft. Database web survey software for gathering information. [[Update 2011]]. Available from URL: http://www.raosoft.com/
- 12.Friesen K, Peterson WE, Squires J, Fortier C. Validation of the Edinburgh Postnatal Depression Scale for Use With Young Childbearing Women. J Nurs Meas. 2017;25:1–16. doi: 10.1891/1061-3749.25.1.E1. [DOI] [PubMed] [Google Scholar]
- 13.Räisänen S, Lehto SM, Nielsen HS, Gissler M, Kramer MR, Heinonen S. Risk factors for and perinatal outcomes of major depression during pregnancy: a population-based analysis during 2002-2010 in Finland. BMJ Open. 2014;4:e004883. doi: 10.1136/bmjopen-2014-004883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.de la Fe Rodríguez-Muñoz M, Le HN, de la Cruz IV, Crespo MEO, Méndez NI. Feasibility of screening and prevalence of prenatal depression in an obstetric setting in Spain. Eur J Obstet Gynecol Reprod Biol. 2017;215:101–105. doi: 10.1016/j.ejogrb.2017.06.009. [DOI] [PubMed] [Google Scholar]
- 15.AkçalıAslan P, Aydın N, Yazıcı E, Aksoy AN, Kirkan TS, Daloglu GA. Prevalence of depressive disorders and related factors in women in the first trimester of their pregnancies in Erzurum, Turkey. Int J Soc Psychiatry. 2014;60:809–817. doi: 10.1177/0020764014524738. [DOI] [PubMed] [Google Scholar]
- 16.Bindt C, Appiah-Poku J, Te Bonle M, Schoppen S, Feldt T, Barkmann C, et al. Antepartum Depression and Anxiety Associated with Disability in African Women: Cross-Sectional Results from the CDS Study in Ghana and Cote d'Ivoire. PLOS One. 2012;7:e48396. doi: 10.1371/journal.pone.0048396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fisher J, Cabral de Mello M, Patel V, Rahman A, Tran T, Holton S, et al. Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: a systematic review. Bull World Health Organ. 2012;90:139G–149G. doi: 10.2471/BLT.11.091850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shidhaye P, Shidhaye R, Phalke V. Association of gender disadvantage factors and gender preference with antenatal depression in women: a cross-sectional study from rural Maharashtra. Soc Psychiatry Psychiatr Epidemiol. 2017;52:737–748. doi: 10.1007/s00127-017-1380-2. [DOI] [PubMed] [Google Scholar]
- 19.Escribà-Agüir V, Artazcoz L. Gender differences in postpartum depression: a longitudinal cohort study. J Epidemiol Community Health. 2011;65:320–326. doi: 10.1136/jech.2008.085894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.El-Behadli AF, Sharp C, Hughes SO, Obasi EM, Nicklas TA. Maternal depression, stress and feeding styles: towards a framework for theory and research in child obesity. Br J Nutr. 2015;113:S55–S71. doi: 10.1017/S000711451400333X. [DOI] [PubMed] [Google Scholar]