

Abstract
Background and Aims:
Effect of serum 25-hydroxy vitamin D (25[OH] D) levels on the recovery of critically ill mechanically ventilated patients is unclear. Hence, this study assessed 25(OH)D levels of critically ill patients on mechanical ventilation at the time of admission to the Intensive Care Unit (ICU) and its relationship with clinical outcome.
Methods:
In this prospective observational pilot study, forty adult patients receiving mechanical ventilation in the ICU were included. Serum 25(OH)D was assessed within 24 h of admission. Primary outcome was 30-day mortality and secondary outcomes were days on mechanical ventilation, ICU-length of stay (ICU-LOS), days to reach spontaneous breathing trial (SBT), requirement of advanced care modality and complications.
Results:
Seventy-five percent patients had low serum 25(OH)D (65% deficient and 10% insufficient). Between patients with low and normal vitamin D, there was no significant difference in 30-day mortality (10% vs. 16.7%; P = 0.81), days on mechanical ventilation (16.2 ± 8.9 vs. 19.9 ± 8.4; P = 0.23), ICU-length of stay (18.7 ± 8.5 vs. 23.3 ± 11.4; P = 0.28), days to reach SBT (11.5 (0–20) vs. 21 (8–30); P = 0.78), complications developed during ICU stay (P = 0.60) and need for advanced care modalities (P = 0.72).
Conclusion:
Low Vitamin D level at admission did not affect 30-day mortality of critically ill patients on mechanical ventilation.
Key words: Intensive Care Units, mechanical ventilation, Vitamin D
INTRODUCTION
Vitamin D is a fat-soluble vitamin synthesized in the skin with exposure to ultraviolet B radiation, converted to 25-hydroxyvitamin D 25(OH)D in the liver and then to its active form 1, 25(OH)D, by 1-alpha-hydroxylase, in the kidneys.[1] Vitamin D deficiency can result from inadequate sunlight exposure, limited dietary intake, impaired gastrointestinal absorption and renal dysfunction. Vitamin D plays important role in calcium and phosphate homeostasis and also has several pleiotropic actions. Adequacy of Vitamin D has been associated with lower levels of inflammatory mediators, C-reactive proteins and erythrocyte sedimentation rate,[2] whereas its deficiency is associated with organ dysfunction and increased susceptibility to hospital-acquired infections in critically ill patients.[3]
Patients receiving mechanical ventilation are at increased risk of Vitamin D deficiency due to prolonged confinement to bed with decreased exposure to sunlight, poor dietary intake, abnormal gastrointestinal functions and drug interactions. Vitamin D deficiency or insufficiency is prevalent in up to 50% of the critically ill patients, 17% of whom have undetectable serum Vitamin D levels.[4] Moraes et al. have shown higher mortality rates among patients with insufficient Vitamin D levels (32.2%) in comparison to patients with adequate Vitamin D levels (13.2%), with no significant difference in other secondary outcomes such as length of stay in Intensive Care Unit (ICU-LOS), need for mechanical ventilation, culture positivity or rate of hospital-acquired infections in the patients.[5] However, the effect of therapeutic administration of Vitamin-D in critically ill patients did not consistently result in a better outcome, rather generated conflicting inferences.[6,7]
The present study was conducted to assess the serum Vitamin D status of the mechanically ventilated critically ill patients at the time of admission to the ICU and its effect on their clinical outcome.
METHODS
The present study was a prospective observational pilot project where 40 adult patients on mechanical ventilation admitted in the ICUs of a tertiary care institute were included after clearance from the Institute Ethics Committee. Informed consent was taken from the legally acceptable representatives of the patients on mechanical ventilation. The inclusion criteria were (i) patients on mechanical ventilation, (ii) >18 years of age, (iii) expected to be on mechanical ventilation for >72 h. Patients with chronic kidney disease, pregnancy, untreated hypothyroidism, thyroidectomy/parathyroidectomy/neck surgery and readmissions in ICUs were excluded from the study.
The clinical and biochemical profile of the patients were recorded using a pre-designed proforma. Blood samples for serum 25 hydroxy vitamin D [25(OH)D] estimation were collected within 24 h of admission to the ICU. The blood samples were centrifuged within 30 min of collection to separate the serum and stored at a temperature of −70°C, until tested. DiaSorin Inc., LIAISON 25(OH)D total assay (REF 310600), a direct competitive chemiluminescence immunoassay with interassay precision (functional sensitivity) of 20%, was used for quantitative determination of total 25(OH)D in serum. In the absence of special guidelines regarding serum 25(OH)D levels in critically ill or patients on mechanical ventilation, we assumed values >30 ng/ml sufficient, 20–30 ng/ml as insufficient and <20 ng/ml as deficient for the patients on mechanical ventilation.[8] Treating clinicians were not informed about the Vitamin-D levels of all patients. However, if the treating clinician was specifically suspecting Vitamin-D deficiency and ordered Vitamin-D level in any patient, that patient was excluded from the statistical analysis.
Subsequent management of the patient was as per ICU protocol. Daily sedation breaks, use of Ventilator Associated Pneumonia (VAP) bundle, daily assessment for readiness to spontaneous breathing trial (SBT) and extubation, deep vein thrombosis prophylaxis, use of lung protective ventilation strategy, use of muscle relaxant in case of severe acute respiratory distress syndrome (ARDS) with PaO2/FiO2 <150 and plateau pressure above 30 cmH2O, blood glucose target 140–180 mg/dl were part of the general ICU management protocol. The outcome predictability of the patients was measured using 'Acute Physiology and Chronic Health Evaluation' (APACHE II) and 'sequential organ failure assessment' (SOFA) scores within first 24 h of admission to ICU.
The primary outcome was 30-day mortality and secondary outcomes were days on mechanical ventilation, ICU-LOS, days to reach SBT, other complications and need for advanced care modalities. All the outcomes were noted by the critical care nurse till 30-days.
The data were coded, entered into Excel sheet and analysed using SPSS 23.0 and STATA 12.1 (IBM Corporation, SPSS version 23.0, Chicago; STATA 12.1, m/s Systech Technocraft Services Pvt. Ltd., Mumbai, Maharashtra). Descriptive statistics including frequency, percentage, mean and standard deviation were used. Inferential statistics included Pearson Chi-square test, Bonferroni test, Wilcoxon Rank (Mann–Whitney) test, Spearman's rank correlation coefficient and one-way ANOVA. The level of significance was considered at 0.05.
RESULTS
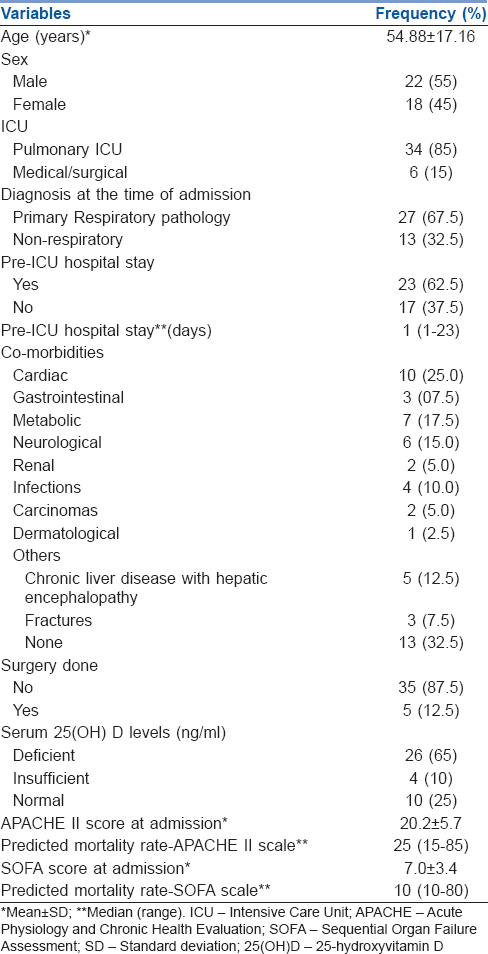
Majority of the patients (87.5%) were non-operative and had the mean age of 54.8 ± 17.16 years (range - 21–85). Fifty-five percent of them were male. The most common cause of ICU admission was pulmonary conditions (67.5%); however, most frequent co-morbidities were cardiac (25%) followed by metabolic (17.5%) and neurological (15%). Low levels of 25(OH)D were present in 75% (30/40) of the patients (65% deficient and 10% insufficient) [Table 1]. Twenty-five percent of them were Vitamin D sufficient with serum 25(OH)D values >30 ng/ml.
Table 1.
Demographic profile of mechanically ventilated patients admitted in selected Intensive Care Units (n=40)
The biochemical and clinical profile of patients on mechanical ventilation with normal and low serum 25(OH)D levels were comparable [Table 2]. The mean APACHE II and SOFA scores and the median predicted mortality rates at the time of admission were similar in patients with normal and low serum 25(OH)D levels [Table 2]. A statistically insignificant trend was seen towards increased ICU-LOS (23.3 ± 11.4 vs. 18.7 ± 8.5), increased mechanical ventilation days (19.9 ± 8.4 vs. 16.2 ± 8.9) and days to reach SBT (21 vs. 11.5 days) in the patients with low serum 25(OH)D levels as compared to patients with normal levels. Similarly, patients with low serum 25(OH)D levels had higher 30-day mortality (16.7%) in comparison to patients with normal levels (10%); although it did not reach statistical significance (P = 0.81) [Table 3].
Table 2.
Demographic, biochemical and physiological characteristics of mechanically ventilated patients along with their serum 25-hydroxyvitamin D levels, admitted in selected Intensive Care Units (n=40)
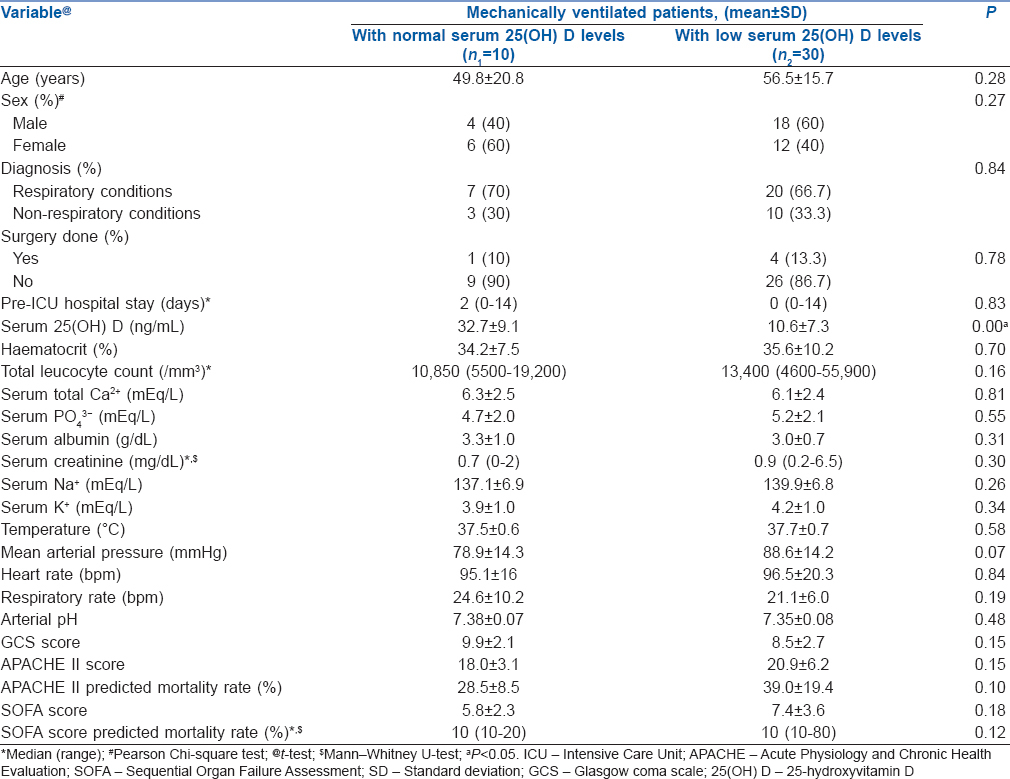
Table 3.
Outcomes of mechanically ventilated patients, with normal and low serum 25-hydroxyvitamin D levels, admitted in selected Intensive Care Units (n=40)
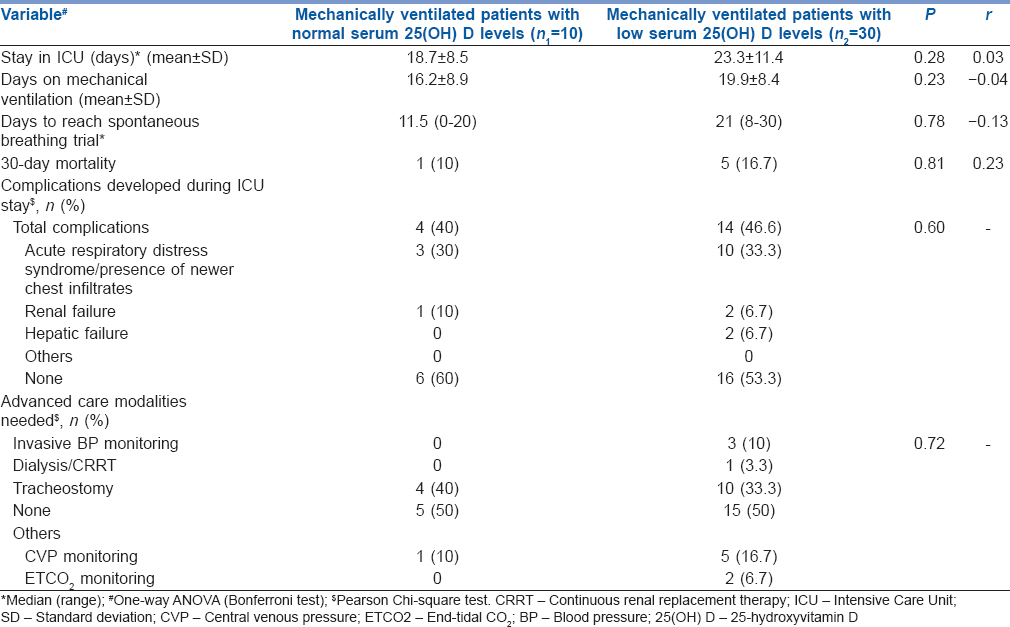
The total number and type of complications developed and requirement for advanced care modalities were similar in patients with normal or low 25(OH)D level [Table 3].
DISCUSSION
The present study revealed that the majority of the patients receiving mechanical ventilation had low serum 25(OH)D levels. In the present study, the most common co-morbidity observed in patients on mechanical ventilation was cardiac in nature. Patients receiving mechanical ventilation with normal and low serum 25(OH)D had comparable biochemical and clinical profile. The outcome of patients in terms of days on mechanical ventilation, LOS in ICU, days to reach SBT, predicted mortality, complications developed and requirement for advanced care modalities in both the groups were also similar. These findings were contradictory to some of the previous studies. This might be because different studies defined the cut off for serum 25(OH)D differently, as well as the co-morbidities, and the primary diagnoses of patients were different in the various studies.
This observation of high prevalence of low serum Vitamin D among patients on mechanical ventilation is similar to that reported earlier in critically ill patients by other investigators.[9,10,11] In the present study, the clinical profile of the patients with normal and low levels of serum 25(OH)D levels were similar. However, other studies[12,13] suggested significant differences among the patients with normal and low serum 25(OH)D levels in terms of mean total leucocyte count,[12] serum calcium,[12,13,14] albumin,[12,13] creatinine[12] and APACHE II and SOFA score.[12] These findings might be due to the type of patients enrolled, as the studies[12,13] mentioned above were conducted in critically ill surgical patients, whereas in the present study, majority (87.5%) of the patients were non-operative.
Vitamin D helps in modulating immunity; hence, its deficiency may predispose critically ill patients to acquire nosocomial infections. In fact, a previous study[15] suggested prolonged ICU stay of the critically ill patients with low serum 25(OH)D levels due to nosocomial infections, complications such as metabolic derangement and immune dysfunctions. On the contrary, another study[9] found that there was no difference among patients on mechanical ventilation with normal and low serum Vitamin D levels in terms of the development of complications. We observed no significant difference in ICU-LOS and development of complications.
Vitamin D is considered important in the prevention of alveolar inflammation and maintenance of respiratory epithelial and mucosal integrity.[16] Optimal serum Vitamin D levels might facilitate an early SBT and shortened duration of mechanical ventilation. However, in the present study, day to reach SBT and duration of mechanical ventilation were similar among the patients with normal and low serum Vitamin D levels. These findings were similar to that of a previous study[14] but in contrast to the observations of another study[17]
Low serum 25(OH)D levels along with the co-morbidities, immune and metabolic dysfunctions might also contribute to the prolonged stay in ICU, increased mortality, complications developed and need for advanced care modalities among patients on mechanical ventilation. In the present study, we observed no significant association of serum 25(OH)D levels with 30-day mortality. This is contrary to the observation by other investigators[9,17] where 28-day mortality was significantly higher in critically ill participants with low serum 25(OH)D levels as compared to participants with normal serum 25(OH)D levels.
In the present study, patients with low and normal serum 25(OH)D levels had comparable requirement for advanced care modalities such as tracheostomy, invasive blood pressure, central venous pressure monitoring and renal replacement therapy. These findings are similar to that reported earlier.[12,13,17,18,19] However, another study,[9] on the contrary, reported Vitamin D sufficient patients required lesser number of invasive monitoring techniques (invasive blood pressure and central venous pressure monitoring) and renal replacement therapy.
Major limitation of the study was observational design and small sample size. Vitamin D level was measured only once, and there was no provision in the protocol to supplement Vitamin D in those with low 25(OH)D levels. This study revealed no significant effect of admission Vitamin D level on the 30-day mortality of critically ill mechanically ventilated patients. However, a trend was observed towards increasing ICU-LOS, increased number of mechanical ventilation days and days to reach SBT. But none of them reached statistical significance possibly because of small sample size. Hence, our observations need confirmation by larger study including bigger sample size and the effect of Vitamin D supplementation in critically ill patients with low 25(OH)D levels also need to be studied in randomized control trials, as previous studies generated controversial results.[6,7,20] Moreover, due to observational nature of the study, we could not strictly control other confounding factors which could affect the duration of mechanical ventilation such as mode of ventilation, specific sedative used, specific fluid management strategy, and diuretic use to name a few.
CONCLUSION
Vitamin D deficiency is prevalent in as high as 75% of critically ill patients on mechanical ventilation. However, this deficiency does not affect the outcome of patients in terms of 30-day mortality, LOS in ICU, number of days on mechanical ventilation, number of days to reach first SBT, complications developed and advanced care modalities required during ICU stay.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We are grateful to Mr. Kulwant Singh, statistician, AIIMS, for helping with the analysis of the data.
REFERENCES
- 1.Tortora JG, Derrickson HB, editors. Function of Skin: Synthesis of Vitamin D. 12th ed. Asia: John Wiley and Sons Pvt., Ltd; 2009. Principles of anatomy and physiology; p. 161. [Google Scholar]
- 2.Shapira Y, Agmon-Levin N, Shoenfeld Y. Mycobacterium tuberculosis, autoimmunity, and Vitamin D. Clin Rev Allergy Immunol. 2010;38:169–77. doi: 10.1007/s12016-009-8150-1. [DOI] [PubMed] [Google Scholar]
- 3.Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of Vitamin D deficiency: An endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30. doi: 10.1210/jc.2011-0385. [DOI] [PubMed] [Google Scholar]
- 4.Lee P, Eisman JA, Center JR. Vitamin D deficiency in critically ill patients. N Engl J Med. 2009;360:1912–4. doi: 10.1056/NEJMc0809996. [DOI] [PubMed] [Google Scholar]
- 5.Moraes RB, Friedman G, Wawrzeniak IC, Marques LS, Nagel FM, Lisboa TC, et al. Vitamin D deficiency is independently associated with mortality among critically ill patients. Clinics (Sao Paulo) 2015;70:326–32. doi: 10.6061/clinics/2015(05)04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Amrein K, Schnedl C, Holl A, Riedl R, Christopher KB, Pachler C, et al. Effect of high-dose Vitamin D3 on hospital length of stay in critically ill patients with Vitamin D deficiency: The VITdAL-ICU randomized clinical trial. JAMA. 2014;312:1520–30. doi: 10.1001/jama.2014.13204. [DOI] [PubMed] [Google Scholar]
- 7.Han JE, Jones JL, Tangpricha V, Brown MA, Brown LAS, Hao L, et al. High dose Vitamin D administration in ventilated Intensive Care Unit patients: A Pilot double blind randomized controlled trial. J Clin Transl Endocrinol. 2016;4:59–65. doi: 10.1016/j.jcte.2016.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Henry HL, Bouillon R, Norman AW, Gallagher JC, Lips P, Heaney RP, et al. 14th Vitamin D workshop consensus on Vitamin D nutritional guidelines. J Steroid Biochem Mol Biol. 2010;121:4–6. doi: 10.1016/j.jsbmb.2010.05.008. [DOI] [PubMed] [Google Scholar]
- 9.Aygencel G, Turkoglu M, Tuncel AF, Candır BA, Bildacı YD, Pasaoglu H, et al. Is Vitamin D insufficiency associated with mortality of critically ill patients? Crit Care Res Pract. 2013;2013:856747. doi: 10.1155/2013/856747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Arnson Y, Gringauz I, Itzhaky D, Amital H. Vitamin D deficiency is associated with poor outcomes and increased mortality in severely ill patients. QJM. 2012;105:633–9. doi: 10.1093/qjmed/hcs014. [DOI] [PubMed] [Google Scholar]
- 11.Higgins DM, Wischmeyer PE, Queensland KM, Sillau SH, Sufit AJ, Heyland DK, et al. Relationship of Vitamin D deficiency to clinical outcomes in critically ill patients. JPEN J Parenter Enteral Nutr. 2012;36:713–20. doi: 10.1177/0148607112444449. [DOI] [PubMed] [Google Scholar]
- 12.Quraishi SA, Bittner EA, Blum L, McCarthy CM, Bhan I, Camargo CA, Jr, et al. Prospective study of Vitamin D status at initiation of care in critically ill surgical patients and risk of 90-day mortality. Crit Care Med. 2014;42:1365–71. doi: 10.1097/CCM.0000000000000210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lucidarme O, Messai E, Mazzoni T, Arcade M, du Cheyron D. Incidence and risk factors of Vitamin D deficiency in critically ill patients: Results from a prospective observational study. Intensive Care Med. 2010;36:1609–11. doi: 10.1007/s00134-010-1875-8. [DOI] [PubMed] [Google Scholar]
- 14.Quraishi SA, McCarthy C, Blum L, Cobb JP, Camargo CA., Jr Plasma 25-hydroxyvitamin D levels at initiation of care and duration of mechanical ventilation in critically ill surgical patients. JPEN J Parenter Enteral Nutr. 2016;40:273–8. doi: 10.1177/0148607114566276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Matthews LR, Ahmed Y, Wilson KL, Griggs DD, Danner OK. Worsening severity of Vitamin D deficiency is associated with increased length of stay, surgical Intensive Care Unit cost, and mortality rate in surgical Intensive Care Unit patients. Am J Surg. 2012;204:37–43. doi: 10.1016/j.amjsurg.2011.07.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dancer RC, Parekh D, Lax S, D'Souza V, Zheng S, Bassford CR, et al. Vitamin D deficiency contributes directly to the acute respiratory distress syndrome (ARDS) BMC Anesthesiol. 2015;15:617, 24. doi: 10.1136/thoraxjnl-2014-206680. Doi: 101186/s12871-015-0063-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Venkatram S, Chilimuri S, Adrish M, Salako A, Patel M, Diaz-Fuentes G, et al. Vitamin D deficiency is associated with mortality in the medical Intensive Care Unit. Crit Care. 2011;15:R292. doi: 10.1186/cc10585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.McKinney JD, Bailey BA, Garrett LH, Peiris P, Manning T, Peiris AN, et al. Relationship between Vitamin D status and ICU outcomes in veterans. J Am Med Dir Assoc. 2011;12:208–11. doi: 10.1016/j.jamda.2010.04.004. [DOI] [PubMed] [Google Scholar]
- 19.Flynn L, Zimmerman LH, McNorton K, Dolman M, Tyburski J, Baylor A, et al. Effects of Vitamin D deficiency in critically ill surgical patients. Am J Surg. 2012;203:379–82. doi: 10.1016/j.amjsurg.2011.09.012. [DOI] [PubMed] [Google Scholar]
- 20.Amrein K, Sourij H, Wagner G, Holl A, Pieber TR, Smolle KH, et al. Short-term effects of high-dose oral Vitamin D3 in critically ill Vitamin D deficient patients: A randomized, double-blind, placebo-controlled pilot study. Crit Care. 2011;15:R104. doi: 10.1186/cc10120. [DOI] [PMC free article] [PubMed] [Google Scholar]