

Abstract
Background:
District level determinants of total fertility rate in Empowered Action Group states of India can help in ongoing population stabilization programs in India.
Objective:
Present study intends to assess the role of district level determinants in predicting total fertility rate among districts of the Empowered Action Group states of India.
Material and Methods:
Data from Annual Health Survey (2011-12) was analysed using STATA and R software packages. Multiple linear regression models were built and evaluated using Akaike Information Criterion. For further understanding, recursive partitioning was used to prepare a regression tree.
Results:
Female married illiteracy positively associated with total fertility rate and explained more than half (53%) of variance. Under multiple linear regression model, married illiteracy, infant mortality rate, Ante natal care registration, household size, median age of live birth and sex ratio explained 70% of total variance in total fertility rate. In regression tree, female married illiteracy was the root node and splits at 42% determined TFR <= 2.7. The next left side branch was again married illiteracy with splits at 23% to determine TFR <= 2.1.
Conclusion:
We conclude that female married illiteracy is one of the most important determinants explaining total fertility rate among the districts of an Empowered Action Group states. Focus on female literacy is required to stabilize the population growth in long run.
Keywords: Married illiteracy, regression tree, total fertility rate
Introduction
Total fertility rate (TFR) is one of the key health indicators for understanding the population growth and stability.[1] The fertility rate directly influences maternal health, and eventually socioeconomic status of the people, family, society, and at large the economy of a nation.[2,3,4] Recent London Summit on Family Planning 2020 is a step to revamp the activities of population stabilization including TFR.
In India, many states achieved replacement level fertility yet TFR is high among others. The Government of India emphasized on states with poor health indicators (classified as Empowered Action Group [EAG] and Assam) contributing highest in the fertility pool. This is also evident in Registrar General of India's series of Annual Health Surveys (AHSs) conducted to track and accelerate health outcomes in these EAG states.[5,6,7]
The previous studies highlighted age at marriage, female literacy, and socioeconomic status as important determinants affecting TFR but none has focused on district-level determinants in EAG states.[5,8,9] This study produces a comprehensive detail of demographic profile and key health indicators of 284 districts in EAG states. Our analysis aims to find the role of female illiteracy and other district level determinants affecting TFR among the EAG states where AHS was conducted during the year 2011-12.
Subject and Methods
Data sources
We analyzed secondary data from AHS (2011–12) captured for nine EAG states. AHS survey covered a total of 284 districts, with sample population of 18.2 million and 3.6 million households. Data analysis was done in June 2016.
Variables
We identified TFR as the dependent variable. Selected independent variables were household size, sex ratio, work participation rate, female married illiteracy, age of marriage, and age at first live birth. Other important covariates were infant mortality rate (IMR), antenatal care (ANC) registration, ANC utilization, and institutional delivery, and reach of family planning services to target population, i.e., unmet need for spacing, unmet need for limiting, and total unmet need.
Data analysis
Data for dependent and independent variables obtained from AHS was organized in Excel file and imported to STATA version 13.1 (StataCorp LP)[10] and R software (The R foundation) for further statistical analysis.[12]
Univariate analysis was done using the linear regression model. Multicollinearity was reviewed using Pearson's correlation coefficients. Multiple linear regression model was manually built using forward stepwise method where the Akaike information criterion (AIC) value was reviewed on every change in explanatory variables. Smaller AIC value was considered as an indicator for improved model. Simultaneously, coefficient of determination was also reviewed for improvement in explained variance in the model. Regression coefficients and 95% confidence intervals were tabulated to present the findings. Statistical significance was considered at 5% (0.05) in the study.
Regression tree
All statistically significant explanatory variables from multiple regression model were used in building regression tree. It was done in “R”[11] using “rpart”-package.[12] Tree pruning was done at 0.020 complexity parameter value after reviewing the x-error (estimates of cross-validated prediction error). However, as number of districts under analysis were smaller (n=284), we did not attempted in-depth interpretation of the regression tree.
Results
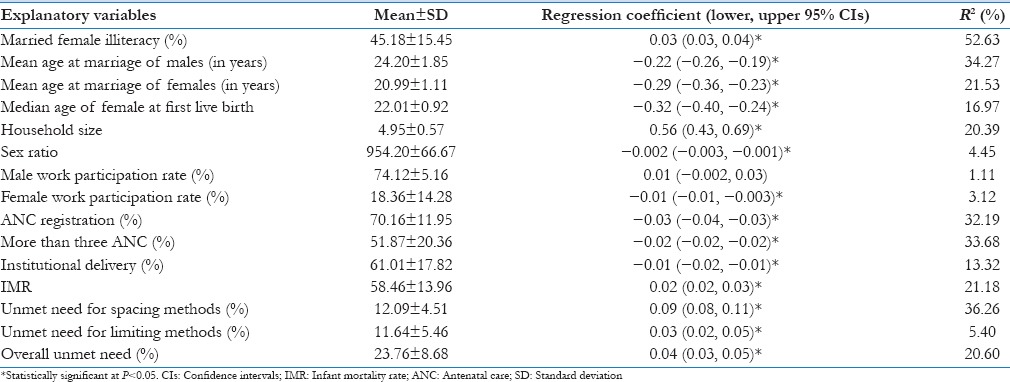
The estimated parameters were TFR (mean, 3.09 ± 0.71); illiteracy among married females (mean, 45.18 ± 15.45%); age at first live birth (median, 22.01 ± 0.92 years); IMR (mean, 58.46 ± 13.96 per 1000 live births); ANC registration (rate, 70.16 ± 11.95%); and total unmet need (mean, 23.76 ± 8.68%). Under univariate linear regression married illiteracy, IMR, unmet need for spacing, unmet need for limiting, total unmet need, and household size were significantly associated with fertility rate of the districts whereas age of marriage (male and female), age of first live birth, work participation rate of females, ANC registration, more than three antenatal check-up, and institutional deliveries showed significant protective effect on TFR. Married illiteracy explained maximum variance (53%) for predicting the TFR. The characteristics of predictors and their corresponding regression coefficient with 95% confidence interval under univariate analysis are given in Table 1.
Table 1.
Summary of explanatory variables and result of univariate analysis
Multiple regression analysis
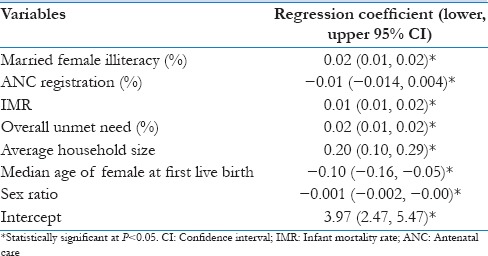
Under multiple linear regression, married female illiteracy, ANC registration, IMR, unmet need, household size, age of first live birth, and sex ratio were found to be statistically significant. This model produced least AIC value among different hierarchical models. And the model explained 70% of variance of TFR. The details of regression coefficients and corresponding 95% confidence interval are given in Table 2.
Table 2.
Regression coefficients for multiple linear model to explain total fertility rate of the districts
Classification and regression tree
Using statistically significant explanatory variables under final multiple linear regression model, the regression tree revealed married illiteracy as most important variables (root node) which later interacted with ANC registration, IMR, and unmet need to decide the extent of TFR. The explanatory variables of the pruned tree explained 66% of variance while full model with all seven explanatory variables explained 70% of variance. Female married illiteracy was found to be a root node and split was at 42% to determine the TFR ≤2.7. In the next left split of married illiteracy at 23%, it further determined the TFR ≤2.1.
Discussion
Our study found married female (15–49 years) illiteracy explaining maximum variance in TFR at district level among EAG states. The most pronounced effect of illiteracy was visualized under Classification and Regression Trees (CART) where married illiteracy is appeared as root node and found to be foremost correlates of higher TFR in the districts. In the same regression tree, in next branch at 23% of married illiteracy, it further reduced the TFR. This decline in TFR with improved literacy was in agreement with various previous publications in India.[13,14,15,16,17] This signifies that literacy is still an important factor in determining TFR among EAG states. Female education usually helps in improving female autonomy[18] which makes them aware of birth control methods, accessibility of maternal services, and better survival of their infant and children,[19,20,21] and make them understand the importance of smaller family.[22] However, in contrary to that another publication revealed that reduction in TFR is more due to increased contraception and alterations in reproductive behavior and not due to increased literacy among females.[23] Higher ANC registration rate is one of the indicators of better accessibility of maternal health services, which shows improved contact between health system/health workers and beneficiaries and thus indication of improved availability of health services to females at various health institutions. ANC in India is an incentivized program through villages’ level community health volunteers, Accredited Social Health Activists. This also facilitates awareness, consultancy, and access services of family planning at various levels of health services, this higher ANC registration may translate into the reduction of TFR of the districts. In the regression tree, ANC registration was the second most important variable to decide the TFR of the district interacting with central node - married female illiteracy.
Improved (lower) IMR indicates better survival of infants which may also help the mother to feel more comfortable in achieving convincing family size quickly with lower fertility.[24] Higher infant mortality, as determinants of higher fertility rates, is reported by some of the earlier publications.[25,26,27,28] CART show IMR as the third important determinants to decide the TFR in interaction with ANC registration rate and female married illiteracy. The IMR of the district later interacted with unmet need to decide the TFR of the respective districts. We also found, unmet need for family planning is significant determinant for higher TFR, which is in agreement with the study conducted by Stover and Ross confirming reduced TFR with higher contraceptives use.[29] Higher unmet need for family planning is an indicator of poor family planning services for spacing and limiting methods. Thus, higher unmet need might be reflected in the same way to keep TFR higher in the districts.
We found that increased age of live birth reducing TFR significantly alone after adjusting other variables. A similar finding was reported by National Family Health Survey-III (NFHS-III) which explained the age of live birth as an important indicator for fertility rate.[30] Our finding is also supported by other studies documenting inverse association of age of the first live birth and fertility rate.[31,32] Usually, age of the first live birth and age of marriage reduce the reproductive span and thus help in the decline of TFR.
Sex ratio is also positively associated with TFR in this study. The sex ratio is believed to be a proxy indicator of son preferences.[30] Findings of this study are consistent with the findings of other publications where effect of son preferences on TFR are well established.[15,28,33,34,35] Son preference and respective change in the fertility rate are also described by NFHS-III which supports the findings of this study.
Finally, we conclude that female married illiteracy plays an important role in determining the TFR of EAG states of India. Along with female married illiteracy, ANC registration, IMR, total unmet needs, household size, and age of the first live birth are some of the other important predictors of TFR. We recommend focusing on these covariates to improve TFR among EAG states at the district level.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Bongaarts J. Human population growth and the demographic transition. Philos Trans R Soc Lond B Biol Sci. 2009;364:2985–90. doi: 10.1098/rstb.2009.0137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Payne J. The impact of a reduced fertility rate on women's health. BMC Womens Health. 2004;4(Suppl 1):S11. doi: 10.1186/1472-6874-4-S1-S11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ashraf QH, Weil DN, Wilde J. The effect of fertility reduction on economic growth. Popul Dev Rev. 2013;39:97–130. doi: 10.1111/j.1728-4457.2013.00575.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tung SL. An econometric analysis of the effects of population change on economic growth: A study of Taiwan. Appl Econ. 1984;16:523–38. doi: 10.1080/00036848400000067. [DOI] [PubMed] [Google Scholar]
- 5.Murugesan P, Srinivasan S. Fertility transition in Empowered Action Group (EAG) states of India. International Contemporary Research Journal in Management and Social Science. 2016;2:63–71. [Google Scholar]
- 6.New Delhi: 2013. [Last accessed on 2015 Mar 05]. Registrar General and Census Commissioner. SRS Statistical Report 2013. Available from: http://www.censusindia.gov.in/vital_statistics/SRS_Reports_2013.html . [Google Scholar]
- 7.Spoorenberg T, Dommaraju P, Spoorenberg T, Dommaraju P. Regional fertility transition in India: An analysis using synthetic parity progression ratios. Int J Popul Res 2012. 2012. [Last cited on 2016 Jul 10]. pp. 1–20. Hindawi Publishing Corporation. Available from: http://www.hindawi.com/journals/ijpr/2012/358409/
- 8.Dreze J, Murthi M. Popul Dev Rev. Vol. 27. Blackwell Publishing Ltd; 2001. [Last cited on 2016 Jul 10]. Fertility, education, and development: Evidence from India; pp. 33–63. Available from: http://doi.wiley.com/10.1111/j.1728-4457.2001.00033.x . [Google Scholar]
- 9.Jalagar VB, Srinivasamurthy K. Fertility decline in India: 1961-70. Rural Demogr. 1980;7:15–23. [PubMed] [Google Scholar]
- 10.StataCorp. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP; 2013. [Google Scholar]
- 11.R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2014. [Google Scholar]
- 12.Therneau T, Atkinson B, Ripley B. rpart: Recursive Partitioning and Regression Trees. R package version 4. 2014:1–8. [Google Scholar]
- 13.Asha Jindal, Pandey NN. Statistical Study of Female Literacy and Selected SocioEconomic and Demographic Variables in Uttar Pradesh, InImran Saleemand Ashraf Imam (Ed), Education in Emerging Indian Society, APH Publishing Corporation. 2013:213–21. [Google Scholar]
- 14.Chaudhuri S. The desire for sons and excess fertility: A household-level analysis of parity progression in India. Int Perspect Sex Reprod Health. 2012;38:178–86. doi: 10.1363/3817812. [DOI] [PubMed] [Google Scholar]
- 15.Vikram K. College Park: University of Maryland; 2012. The Role of Social and Cultural Capital in Fertility Preference and Contraceptive Use. Population Association of America, 2012. [Google Scholar]
- 16.Saurabh S, Sarkar S, Pandey DK. Female literacy rate is a better predictor of birth rate and infant mortality rate in India. J Family Med Prim Care. 2013;2:349–53. doi: 10.4103/2249-4863.123889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mohanty SK, Fink G, Chauhan R, Canning D. Distal determinants of fertility decline: Evidence from 640 Indian districts. Demogr Res. 2016;34:373–406. [Google Scholar]
- 18.Alfano M, Arulampalam W, Kambhampati U. Female autonomy and education of the subsequent generation: Evidence from India. Cape Town: 5th IZA/World Bank Conference on Employment and Development, Capetown. 2010 [Google Scholar]
- 19.Abadian S. Women's autonomy and its impact on fertility. World Dev. 1996;24:1793–809. [Google Scholar]
- 20.Mistry R, Galal O, Lu M. “Women's autonomy and pregnancy care in rural India: A contextual analysis”. Soc Sci Med. 2009;69:926–33. doi: 10.1016/j.socscimed.2009.07.008. [DOI] [PubMed] [Google Scholar]
- 21.Shroff MR, Griffiths PL, Suchindran C, Nagalla B, Vazir S, Bentley ME. Does maternal autonomy influence feeding practices and infant growth in rural India? Soc Sci Med. 2011;73:447–55. doi: 10.1016/j.socscimed.2011.05.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Singh K, Singh K, Singh B, Pathak A. Impact of education and autonomy on fertility of women in Eastern Uttar Pradesh. Demogr India. 2002;31:223–33. [Google Scholar]
- 23.Mari Bhat PN. Returning a favor: Reciprocity between female education and fertility in India. World Dev. 2002;30:1791–803. [Google Scholar]
- 24.Hossain MB, Phillips JF, Legrand TK. The impact of childhood mortality on fertility in six rural thanas of Bangladesh. Demography. 2007;44:771–84. doi: 10.1353/dem.2007.0047. [DOI] [PubMed] [Google Scholar]
- 25.Agrawal R. Influence of infant and child mortality on fertility in India. Seminar on Infant Mortality in Relation to the Level of Fertility. Bangkok: Committee for International Coordination of National Research in Demography, Bangkok. 1975:163–83. [Google Scholar]
- 26.Syamala TS. Relationship between infant and child mortality and fertility – An enquiry into goan women. Indian J Pediatr. 2001;68:1111–5. doi: 10.1007/BF02722920. [DOI] [PubMed] [Google Scholar]
- 27.Rezaei S, Jamshidi K, Moradi K. Impact of socioeconomic and health system factors on infant mortality rate in Organization of the Petroleum Exporting Countries (OPEC): Evidence from 2004 to 2013. Int J Pediatr. 2015;3:493–9. [Google Scholar]
- 28.Singh P, Mishra A, Mishra OP. Predictors of third and higher order births in India. Indian J Community Health. 2015;27:443–7. [Google Scholar]
- 29.Stover J, Ross J. Changes in the distribution of high-risk births associated with changes in contraceptive prevalence. BMC Public Health. 2013;13(Suppl 3):S4. doi: 10.1186/1471-2458-13-S3-S4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.I. Mumbai: IIPS; 2007. International Institute for Population Sciences (IIPS) and Macro International. Fertility and Fertility Preferences, National Family Health Survey (NFHS-3), 2005–06: India. [Google Scholar]
- 31.Majuro, Marshall Islands: Economic Policy, Planning and Statistics Office; August; 2008. Demographic and Health Survey 2007. [Google Scholar]
- 32.Tripathy P, Sarangi P. Proximate determinants of fertility in India. J Fam Welf. 2004;50:22–9. [Google Scholar]
- 33.Bhandari GP, Premarajan KC, Jha N, Yadav BK, Paudel IS, Nagesh S. Prevalence and determinants of unmet need for family planning in a district of Eastern region of Nepal. Kathmandu Univ Med J (KUMJ) 2006;4:203–10. [PubMed] [Google Scholar]
- 34.Calhoun LM, Nanda P, Speizer IS, Jain M. The effect of family sex composition on fertility desires and family planning behaviors in urban Uttar Pradesh, India. Reprod Health. 2013;10:48. doi: 10.1186/1742-4755-10-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Rele JR. Some aspects of family and fertility in India. Popul Stud (NY) 1962;15:267. [Google Scholar]